Sri Raghavendra College of Pharmacy, Chitradurga, Karnataka, India 577501
Conjoined twin separation surgery is among the most complex and rare procedures in paediatric surgery, demanding careful pharmacological planning. Cross-circulation, shared organs, and altered drug metabolism make anesthetic and perioperative drug management highly challenging. This review highlights preoperative assessment, intraoperative anesthetic strategies, and postoperative dosing adjustments, with emphasis on the critical role of clinical pharmacists in minimizing medication errors and optimizing patient safety. Published experiences remain limited, yet they provide essential guidance for developing evidence-based pharmacological protocols in future cases.
Epidemiology and Classification
Conjoined twins are an extremely rare congenital anomaly, with an estimated incidence of 1 in 50,000 to 200,000 live births worldwide.[1,2] The condition occurs more frequently in females and is reported more often in developing countries.[3,4] Conjoined twins arise from incomplete embryonic division between the 13th and 15th day of gestation, resulting in varying degrees of anatomical fusion and shared organs.[5,6] They are classified according to the site of union—thoracopagus, omphalopagus, craniopagus, and pygopagus being the most commonly reported types.[7,8] Thoraco-omphalopagus twins, in particular, present major challenges due to frequent sharing of hepatic and cardiovascular systems.[9,10]
Although rare, conjoined twins have fascinated physicians for centuries, with some of the earliest recorded cases dating back to the 10th century. [11,12] The survival of conjoined twins has historically been poor, with most cases ending in stillbirth or neonatal death. Advances in prenatal imaging such as ultrasound, MRI, and 3D reconstruction now allow earlier detection, often as early as the first trimester. [13] This enables better counseling of families and facilitates planning for delivery in tertiary centers with surgical capability. [14]
Epidemiologically, nearly 75% of conjoined twins are female, a ratio consistently observed across multiple studies, though the exact mechanism remains unknown. [15,16] Some researchers suggest a greater in utero survival advantage in female fetuses, while others propose reporting bias as a contributing factor. [17]
Geographic clustering has also been observed, with a higher number of reported cases in India, Pakistan, Nigeria, and Southeast Asia. [18,19] Socioeconomic factors, lack of access to prenatal screening, and cultural considerations often influence whether such cases are documented, carried to term, or surgically managed. [20]
Classification remains clinically important because prognosis and surgical feasibility vary with type. Thoracopagus twins, accounting for almost 40% of all cases, carry the worst prognosis, particularly if a single fused heart is present.[21] Omphalopagus twins, on the other hand, generally have a more favorable outcome, especially when only hepatic tissue is shared. [22] Craniopagus twins represent one of the most technically demanding surgical challenges due to shared cerebral venous sinuses. [23] Pygopagus and ischiopagus twins can often be separated successfully, though postoperative complications like spinal instability or urinary dysfunction may persist. [24]
Rare variants such as cephalopagus (fusion of face and thorax) and rachipagus (dorsal fusion along the spine) are almost universally fatal. [25]
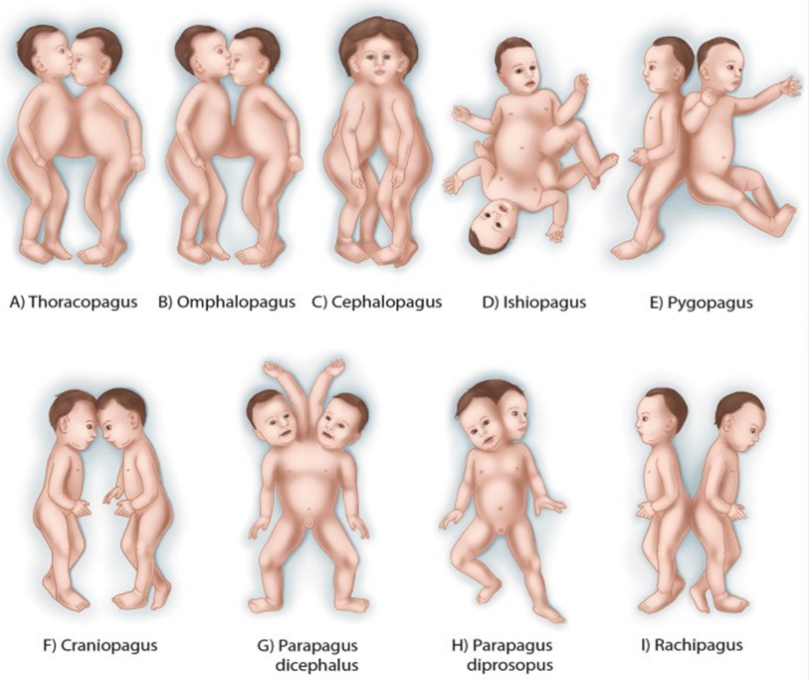
Fig.01 Types of Conjoined Twins
Pathophysiology and Embryology
Conjoined twinning arises from incomplete embryonic division between the 13th–15th day post-fertilization.[9,10] The degree of fusion varies from shared skin and musculature to common vital organs such as the heart, liver, or gastrointestinal tract.[11,12] During normal development, the embryo begins to split into two distinct organisms around the second week of gestation. In conjoined twins, this division halts prematurely, leaving the embryos partially fused. The exact mechanism remains debated, with two primary hypotheses proposed: the fission theory and the fusion theory.[9] The fission theory suggests that incomplete splitting of the embryonic disc results in physically joined twins, whereas the fusion theory proposes that initially separate embryos may secondarily fuse due to proximity and adhesive properties of early embryonic tissues. [10,11]
The specific timing of developmental arrest influences the anatomical presentation. For example, early incomplete division may result in thoracopagus or omphalopagus twins, while later disruptions may produce pygopagus or craniopagus forms. [12,13] The degree of vascular connection also varies widely. Some pairs share only superficial tissue bridges, while others demonstrate common livers, gastrointestinal tracts, or even a single functional heart, significantly complicating survival and surgical separation.[14]
From a physiological perspective, conjoined twins often face imbalanced circulation and organ function. Cross-circulation can result in unequal oxygen delivery, altered drug metabolism, and discrepancies in growth between the two twins. [15] In extreme cases, one twin may function as a hemodynamic or metabolic “support twin”, bearing the majority of physiological burden, while the co-twin may remain underdeveloped (a condition termed parasitic twinning). [16]
Advances in imaging, including fatal MRI, ultrasonography, and angiographic studies, now provide detailed insights into the shared anatomy and physiology of conjoined twins before birth. [17,18] Such diagnostic clarity has proven invaluable in counselling families, planning surgical strategies, and anticipating pharmacological challenges.
Despite these technological advancements, the rarity and heterogeneity of cases mean that no universal model of pathophysiology exists. Each set of conjoined twins presents with unique structural and physiological challenges, underscoring the importance of individualized, multidisciplinary management. [19,20] This variability not only determines surgical feasibility but also has a profound effect on drug distribution and metabolism. [13,14]
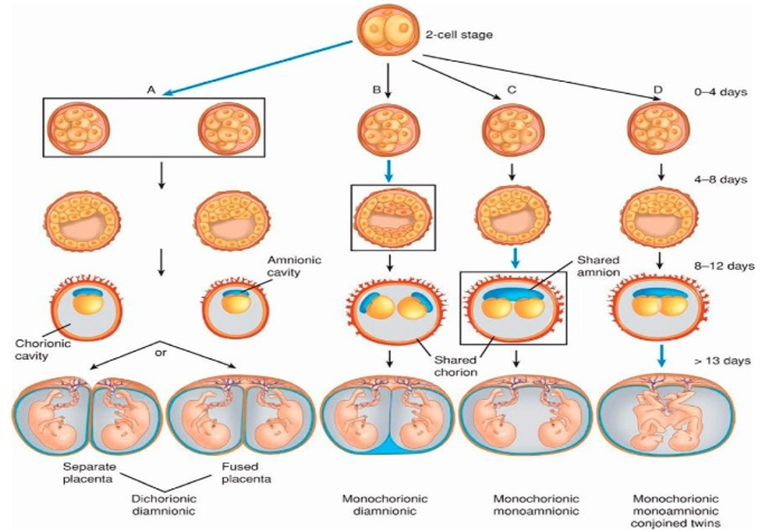
Fig.02 embryological stages showing incomplete division leading to conjoined twins
Pharmacological Challenges in Conjoined Twins
Pharmacological management is uniquely complicated by the phenomenon of cross-circulation, in which drugs administered to one twin can enter the circulation of the other.[11,12] This alters pharmacokinetics and pharmacodynamics, leading to unpredictable drug effects such as unexpected sedation, respiratory depression, or neuromuscular blockade in the non-dosed twin.[13,14] The presence of cross-circulation is perhaps the single most important determinant of pharmacological safety in conjoined twins. The unpredictable transfer of medications between twins can result in double dosing or inadequate exposure, both of which have life-threatening implications. [17] In some cases, one twin may receive nearly the full intended drug dose while the other experiences unintended but significant pharmacological effects. [18] This variability complicates every aspect of perioperative care, including anaesthesia, analgesia, antibiotic therapy, and critical care pharmacology.
Several case reports illustrate the seriousness of this issue. In one instance, a neuromuscular blocking agent administered to one thoracopagus twin resulted in complete respiratory paralysis in the sibling due to extensive vascular shunting. [19] In another, sedative medication caused one twin to enter deep anaesthesia while the other displayed only mild sedation, making balanced induction nearly impossible. [20]
Because of such risks, preoperative evaluation of cross-circulation is mandatory. Radionuclide scanning provides quantitative data on the degree of vascular sharing, while atropine challenge tests remain a quick bedside tool: if an injected dose of atropine in one twin produces tachycardia in both, significant cross-circulation exists. [21,22] Similarly, dye dilution studies with indigo carmine or methylene blue are simple but effective for mapping circulation patterns. [23] Advanced echocardiographic and angiographic studies further help clarify shared cardiovascular structures that influence drug kinetics. [24]
The impact of shared organs adds another layer of pharmacological complexity. A fused liver, common in thoraco-omphalopagus twins, means that hepatic metabolism is altered, sometimes functioning as a “shared metabolic factory” for both twins. [25] This can prolong drug half-lives, reduce clearance, and increase toxicity risks, particularly with hepatically metabolized drugs such as opioids, benzodiazepines, and certain antibiotics. [26] Similarly, shared renal structures alter excretion of renally cleared drugs like aminoglycosides, leading to heightened nephrotoxic potential. [27]
To mitigate these risks, drug administration in conjoined twins is often guided by the principle of “titrate to effect” rather than standard weight-based dosing. [28] Continuous monitoring of cardiorespiratory responses, depth of anesthesia, and neuromuscular function is essential to adjust dosages in real time. [29] Moreover, whenever possible, short-acting agents with predictable clearance (e.g., remifentanil, propofol) are favored over long-acting medications that may accumulate unpredictably. [30]
Finally, the role of the clinical pharmacist in the perioperative team cannot be overstated. Pharmacists assist in verifying doses, anticipating cross-effects, checking drug compatibility, and preventing inadvertent double dosing — risks that are magnified when two nearly identical patients are treated simultaneously in a high-stakes surgical setting. [29,30] Their presence significantly enhances patient safety in these rare and complex procedures.Preoperative testing with radionuclide imaging, echocardiography, or atropine challenge remains essential for identifying the degree of cross-circulation and planning individualized anaesthetic strategies.[15,16]
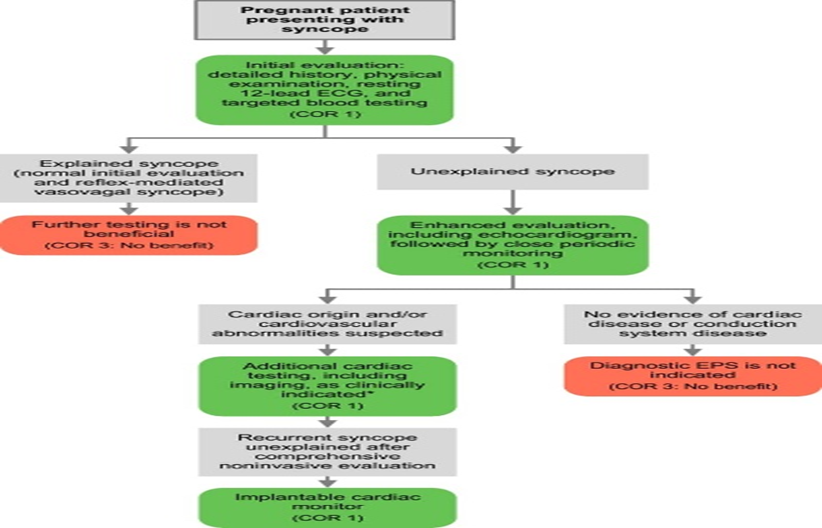
Fig. 03 Flowchart showing cross-circulation evaluation tests — atropine test, radionuclide imaging, dye dilution
Intraoperative Anaesthetic Strategies
Intraoperative management demands coordinated teamwork between two anaesthesia teams, each assigned to one twin with color-coded circuits, monitors, and drug syringes to prevent errors.[17,18] Balanced anaesthesia using volatile agents, opioids, and neuromuscular blocking drugs has been the most commonly described approach.[19,20] However, the presence of shared liver or renal structures complicates drug metabolism and clearance, requiring titration to clinical effect.[21,22] Massive haemorrhage is a frequent complication, especially during separation of hepatic vasculature, making early activation of massive transfusion protocols and coagulation monitoring essential.[23,24]
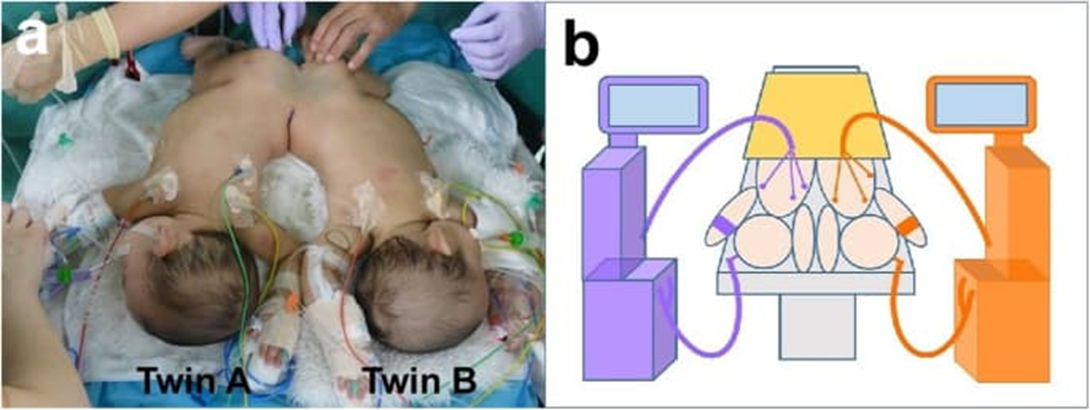
Fig 04 Operating room setup with dual anaesthesia teams and color-coded equipment
Hemodynamic and Surgical Considerations
Separation surgery often induces abrupt hemodynamic changes due to sudden alterations in shared circulatory physiology. [25,26] Vasopressor infusions and fluid therapy must be carefully titrated to maintain stability for both twins during critical phases of surgery. [27,28] Team communication, use of BI spectral index (BIS) monitoring, and staged induction techniques have been reported to optimize intraoperative safety. [29,30]

Fig 05 Graphical representation of hemodynamic changes before, during, and after separation
Postoperative Pharmacological Care
Following successful separation, each twin transitions to independent physiology, making postoperative drug dosing critically important. Sedation, analgesia, antibiotics, and anticoagulants must be recalculated for each individual twin, considering differences in weight, organ function, and hemodynamic status. [25,26] Clinical pharmacists play a vital role by verifying doses, checking drug compatibilities, and preventing infusion errors in the intensive care unit. [27,28] Evidence suggests that active pharmacist participation significantly reduces medication-related complications in these highly complex cases. [29,30]
Fig 06 Medication safety workflow chart showing pharmacist role in postoperative management
Need for Evidence-Based Protocols
Despite significant advances, separation surgeries remain high-risk procedures with mortality rates influenced by shared anatomy and surgical complexity. [5,7] Current literature is largely limited to case reports and small series, underscoring the need for systematic data collection. Each published experience contributes critical insights into drug management, perioperative protocols, and the role of multidisciplinary collaboration. Establishing evidence-based guidelines is essential to improve outcomes and provide future teams with structured pharmacological strategies. [11,19]
METHODS
This review was developed by systematically collecting and analyzing published literature related to the pharmacological aspects of separation surgery in conjoined twins.
Search Strategy
Electronic databases including PubMed, Google Scholar, and Scopus were searched using the terms: “conjoined twins,” “separation surgery,” “pharmacological management,” “cross-circulation,” “perioperative drugs,” and “anesthesia.” Boolean operators (AND/OR) were applied to broaden the search. Additional articles were identified by screening the references of selected papers.
Eligibility Criteria
Articles were included if they:
Articles were excluded if they:
Data Extraction
From each included study, the following information was extracted: type of conjoining, extent of shared anatomy, perioperative pharmacological interventions, intraoperative anesthetic strategies, postoperative drug management, complications, and outcomes. Priority was given to case reports and reviews that provided detailed pharmacological insights.
Synthesis of Evidence
The collected information was categorized into thematic areas:
In total, 30 articles were identified that met the eligibility criteria and were included in the present review.
RESULTS
Pharmacological management in conjoined twin separation is highly complex due to shared organ systems and the possibility of cross-circulation. Preoperative assessment is crucial, including evaluation of cross-circulation and cardiac function, which guides the choice and dosing of anesthetic agents (4, 2, 12). Drug administration strategies, such as sequential or simultaneous induction, are tailored according to the extent of circulatory sharing to avoid under- or overdosing (9, 10). Maintenance of anesthesia commonly involves a combination of inhalational and intravenous agents, with careful monitoring using techniques like BIS to ensure adequate depth while minimizing systemic effects (7, 12, 13). Regional anesthesia may be used in combination with general anesthesia to reduce drug requirements in certain cases (6, 17). Intraoperative pharmacological management requires meticulous planning, including color-coded lines and predefined dosing protocols, as medications given to one twin can affect the other (11, 20). Hemodynamic stability is maintained with careful titration of vasoactive drugs, while ventilatory support is individualized due to anatomical differences (3, 5, 7). Postoperatively, drug dosing is adjusted considering altered pharmacokinetics after separation, and continuous monitoring for organ function and analgesia needs is essential for optimal recovery (9, 10, 24). Overall, successful pharmacological management relies on careful preoperative evaluation, individualized anesthetic plans, and coordinated multidisciplinary care (1, 2, 11)
DISCUSSION
1) What the case-based literature really tells us
Most evidence on pharmacological management in conjoined-twin separation comes from single cases or small series. That makes randomized comparisons impossible, but the reports consistently converge on a few load-bearing themes:
2) Quantifying cross-circulation and using it to drive dosing
Reports use atropine challenges, dye studies, radionuclide techniques, and hemodynamic/EEG responses to estimate shunting between twins. [13,14,16,18,21–23] Yet the field lacks a shared vocabulary for “how much” cross-flow matters. A useful operational scheme is to stratify into:
Minimal (no physiologic response in co-twin): proceed with near-standard, independent dosing, but still split teams and label lines. [12,19]
Moderate (subtle HR/BIS change): reduce initial boluses 25–50%, avoid long-acting agents, and titrate to effect with continuous monitors in both twins. [13,16,18]
High (clear mirror response or radionuclide transfer): sequential induction, prioritize infusions over boluses, and anticipate delayed offset from shared metabolism. [9,11,14]
This moves cross-circulation testing from a diagnostic curiosity to a dose-calibration tool.
3) Induction and maintenance: why “short and steerable” wins
Across cases, anesthetic plans that favor short-context agents and infusion-based control consistently reduce surprises. [19,20,24] Volatile anesthesia is feasible but less “steerable” when cross-circulation exists, because redistribution can blur depth asymmetrically; dual BIS and frequent clinical checks help detect this. [12,18]
Practical implications:
Prefer titrated propofol/remifentanil infusions over large boluses when cross-flow is non-trivial. [19,20]
Keep neuromuscular blockade short and monitor each twin independently with TOF; avoid long-acting relaxants that could trap one twin paralyzed while the other is awake if flows diverge. [11,15]
Use sequential induction in high cross-flow states so the “second” twin’s baseline isn’t distorted by the “first” twin’s drugs. [9,14]
4) Drug class–specific insights from the literature
Opioids: Remifentanil’s esterase metabolism makes effect more predictable when hepatic sharing exists; large fentanyl boluses are over-represented in reports of unexpected co-twin depression. [19,20,24]
Hypnotics: Propofol works well with infusion-first strategies; slow titration prevents co-twin overshoot when cross-circulation is present. [19]
Neuromuscular blockers: Case reports link unintended co-twin apnea to rocuronium/vecuronium boluses in high shunting; TOF-guided micro-titration mitigates this. [11,15]
Vasoactives: Phenylephrine/norepinephrine responses can “telegraph” cross-flow; dose the minimum effective and re-assess both twins after every change. [21,22]
Antimicrobials: When livers are joined, first-dose peaks may equalize across twins, but clearance can delay; aminoglycosides/vancomycin call for early TDM after separation to re-set dosing. [24,30]
Antifibrinolytics & coagulation products: During hepatic division, TXA and goal-directed coagulation therapy (e.g., fibrinogen concentrate/cryoprecipitate guided by viscoelastic testing) align with lower product exposure in reports, though data are sparse and center-specific. [23,24]
5) Hemorrhage and coagulopathy: pharmacology is a team sport
Hepatic transection is the inflection point for blood loss and coagulopathy. [23,24] Teams that pre-define massive transfusion triggers, pre-prime warming/rapid infusers, and use point-of-care coagulation (TEG/ROTEM where available) can convert empiric transfusion into targeted pharmacotherapy (fibrinogen first when low, platelets for poor MA, PCC/FFP for prolonged times). [23,24,] Pharmacists are pivotal here—tracking cumulative calcium, antifibrinolytics, and compatibility to avoid precipitation or line clogging during high-throughput transfusion. [20]
6) Monitoring as a pharmacology tool (not just “monitoring”)
Dual BIS helps detect covert co-twin hypnotic effects; TOF on both twins spots unintended NMB spread; arterial lines provide beat-to-beat readouts to titrate vasoactives independently. [12,18,39,40] Treat these signals as dose feedback loops rather than passive displays.
7) Human factors and error-proofing are pharmacological safeguards
Wrong-syringe and wrong-patient errors are the unique, ever-present threats when two nearly identical patients lie side-by-side. [17,20] Reliable strategies in the literature—two completely separate anesthesia carts, color-coded circuits/syringes, duplicated pumps, mirrored room layout, and a do-not-cross line for lines and staff—directly reduce drug error risk.[17,18,20] Embedding a medication time-out before every dose change sounds simple but is repeatedly associated with fewer near-misses.[17,20]
8) Transition pharmacology after separation: a new baseline overnight
Immediately after division, each twin’s physiology “reboots.” Doses based on pre-separation dynamics often over- or under-shoot. The most successful teams treat the first 6–12 hours as a dose-finding phase: re-calculate all continuous infusions per actual post-separation weight and organ function, re-assess analgesia/sedation targets, and order early labs (liver panel, creatinine, coagulation) to re-anchor antimicrobial and anticoagulant regimens. [24–26,30] Pharmacist-led reconciliation—purging duplicated orders, fixing rate units, and checking compatibilities—has tangible safety impact. [27–30]
9) Regional techniques: useful adjuncts if the risk ledger allows
Reports describe combined caudal/epidural plus general anesthesia for lower-body joins, reducing systemic opioid needs and smoothing emergence. [6,17] The trade-off is coagulopathy risk during long hepatic phases; thus, neuraxial plans should be pre-authorized with a stop rule—if coagulation derails, defer or remove catheters early. [6,23,24]
10) Practical, evidence-informed framework (actionable “how-to”)
Based on converging case experience: [9–12,15–20,23–30]
During surgery
After separation
11) Limitations of the current evidence
The literature base is small and heterogeneous; outcome signals can be confounded by anatomy, timing (elective vs emergency), and resource variability. [5,7,9,14,28] Many reports lack pharmacokinetic sampling, standard definitions of cross-flow, or consistent outcome metrics, which limits meta-analysis and formal guideline development.[11,19]
12) Research priorities
A pragmatic research agenda emerges from gaps highlighted across cases: [9,11,16,19,24]
13) Bottom line
The strongest lesson from decades of case experience is that measurement-guided, process-reliable pharmacology outperforms any fixed drug recipe. When cross-circulation is quantified, doses are titrated to real-time signals, and the medication system is engineered for zero mix-ups, teams report safer anesthetics and smoother post-separation courses—even in the most complex anatomical variants. [9–12,15–20,23–30]
DECLARATIONS
REFERENCES



Azra Banu Gokak, Ismail Zabiulla, Kruthik N., Pharmacological Management in Conjoined Twin Separation Therapy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1186-1197. https://doi.org/10.5281/zenodo.17099291
 10.5281/zenodo.17099291
10.5281/zenodo.17099291
