Department of Pharmacognosy, K.B. Raval College of Pharmacy, Shertha, Gandhinagar, Gujarat 382423, India
Drug induced liver injury is a leading cause of acute liver failure and a major reason for drug withdrawal, treatment discontinuation, and hospitalization worldwide. DILI results from complex mechanisms involving reactive metabolite formation, oxidative stress, mitochondrial dysfunction, bile acid dysregulation, and immune mediated hepatotoxicity. Despite advances in pharmacovigilance and causality assessment tools, effective preventive or therapeutic options remain limited, with N-acetylcysteine being mainly useful in acetaminophen toxicity and liver transplantation reserved for severe cases. In this context, plant-derived hepatoprotective compounds have gained attention due to their antioxidant, anti inflammatory, anti-apoptotic, antifibrotic, and detoxification enhancing effects. Several medicinal plants such as Silybum marianum (silymarin), Phyllanthus spp., Picrorhiza kurroa, Glycyrrhiza glabra, Curcuma longa, and Andrographis paniculata contain bioactive phytoconstituents (flavonoids, phenolics, terpenoids, lignans, and alkaloids) that modulate critical pathways like Nrf2/ARE, NF-kB, CYP450 enzymes, mitochondrial integrity, and inflammatory cytokine signaling. This review summarizes the pathophysiology of DILI, discusses key hepatoprotective phytoconstituents and medicinal plants, evaluates preclinical and clinical evidence, highlights safety concerns including herb-drug interactions, and outlines regulatory challenges and future perspectives for translating plant based hepatoprotectives into evidence based preventive strategies for DILI.
Drug induced liver injury refers to liver damage caused by prescription drugs, OTC medications, herbal products, and dietary supplements. It represents one of the most frequent causes of acute hepatitis and acute liver failure in clinical practice, and it remains a key obstacle in drug development and post marketing safety surveillance.1,2 DILI may manifest as asymptomatic elevations in liver enzymes or as severe hepatocellular necrosis, cholestasis, mixed injury patterns, or even acute liver failure requiring transplantation.1,3 The incidence of drug induced liver injury varies across populations due to genetic factors, prescribing patterns, and reporting systems, but it is consistently recognized as a major contributor to morbidity and mortality.2,4
A unique challenge of drug induced liver injury is its unpredictability. While some reactions are dose dependent (intrinsic hepatotoxicity such as acetaminophen overdose), many cases are idiosyncratic, occurring in susceptible individuals with variable latency and clinical presentation.1,5 Current management primarily involves early recognition, prompt discontinuation of the offending drug, supportive care, and specific antidotes only in select scenarios (e.g., N-acetylcysteine for acetaminophen toxicity).6,7 This therapeutic gap motivates exploration of hepatoprotective strategies that can prevent or mitigate injury.
Plant-derived hepatoprotective agents are attractive because they often contain multiple bioactive compounds that target diverse pathogenic mechanisms including oxidative stress, inflammation, mitochondrial damage, and impaired detoxification.8,9 Many medicinal plants have long standing use in traditional systems such as Ayurveda, Traditional Chinese Medicine, and Unani (or Yunani) medicine for jaundice, hepatitis, and liver disorders. Modern pharmacological studies increasingly support the potential of plant derived compounds as adjuncts or preventive agents in drug-induced liver injury.8-10
This review aims to: summarize the mechanistic basis of DILI, highlight key antihepatotoxicity medicinal plants and phytoconstituents, discuss preclinical and clinical evidence, evaluate safety and herb drug interactions and propose future directions for clinical translation.
Drug exposure
↓
Phase I metabolism (CYP450) → Reactive metabolites
↓
Oxidative stress (ROS) + GSH depletion
↓
Mitochondrial dysfunction → ATP depletion → Cell death
↓
Inflammation (NF-kB, cytokines) + Immune activation
↓
Hepatocyte injury (ALT/AST) → Cholestasis / Necrosis / ALF
Fig.1 Overview of DILI and sites of Hepatoprotective Intervention
Plant-derived hepatoprotectives act by:
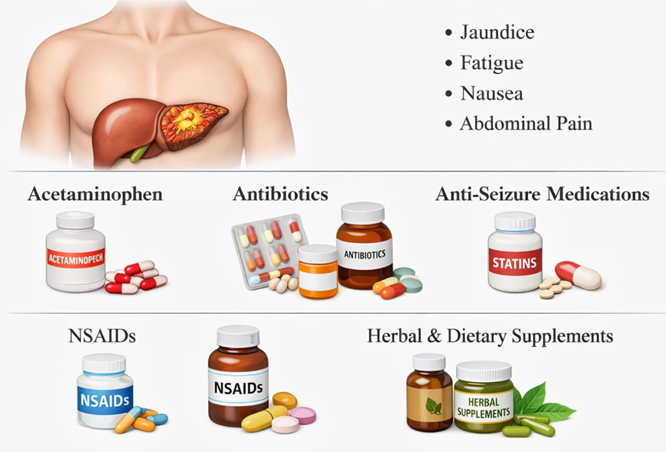
Fig.2 Liver injury caused by commonly used medications.11
PATHOPHYSIOLOGY OF DRUG INDUCED LIVER INJURY
Drug-induced liver injury is not a single mechanism phenomenon, it involves complex interactions between drug metabolism, immune response, genetic susceptibility, and environmental factors. Key pathophysiological processes include oxidative stress, mitochondrial injury, immune activation, and bile acid transport disruption.1,2
Classification and Patterns of injury
Drug induced liver injury is broadly categorized into intrinsic (predictable, dose related) and idiosyncratic (unpredictable, not clearly dose related) forms.1,5 Clinical injury patterns include hepatocellular, cholestatic, and mixed injury types, often assessed using the R ratio (ALT/ALP relative to upper limits of normal).1,3 Severity ranges from mild enzyme elevation to acute liver failure (ALF).2,6
Examples:
Acetaminophen is metabolized into the NAPQI metabolite, which leads to GSH depletion and hepatocyte necrosis.12 Isoniazid froms reactive intermediates that cause oxidative stress & mitochondrial dysfunction.13
Oxidative stress and Relative metabolites
A central mechanism in drug induced liver injury is oxidative stress, resulting from excessive reactive oxygen species generation and depletion of antioxidant defenses such as glutathione. Many drugs undergo Phase I metabolism via CYP450 enzymes to form reactive intermediates that can covalently bind proteins, lipids, and DNA, triggering cellular dysfunction.14,15 For example, acetaminophen is metabolized to NAPQI, which depletes GSH and induces oxidative injury when detoxification capacity is overwhelmed.6,14
Mitochondrial dysfunction
Mitochondrial damage is strongly implicated in both intrinsic and idiosyncratic drug-induced liver injury. Reactive metabolites may impair electron transport chain activity, induce mitochondrial permeability transition (MPT), reduce ATP production, and activate apoptosis or necrosis.17,18 Mitochondrial dysfunction also amplifies oxidative stress, forming a self perpetuating injury cycle.16,18
Immune-mediated hepatotoxicity
Some DILI cases involve immune mechanisms, where drug-protein adducts (haptens also known as incomplete antigen) trigger adaptive immune responses. Danger associated molecular patterns (DAMPs) released from injured liver cell can activate Kupffer cells and recruit inflammatory cells, leading to cytokine storms and hepatocyte death.21,22 This immune involvement is particularly relevant in idiosyncratic DILI and explains variability among patients.5,21
Cholestasis and Bile acid dysregulation
Drug-induced cholestasis may occur through inhibition of bile transporters such as BSEP (bile salt export pump), leading to intracellular bile acid accumulation and liver cell injury.21 Cholestatic DILI often presents with skin sensation, jaundice, and elevated alkaline phosphatase.3,21
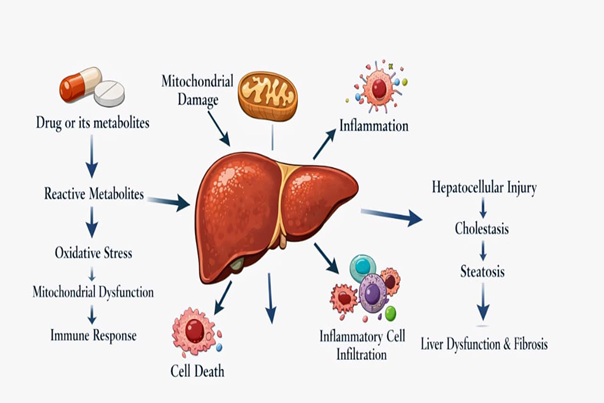
Fig.3 Pathogenesis of drug- induced liver injury.22
HEPATOPROTECTIVE MEDICINAL PLANTS
The liver, a central organ for metabolism, detoxification, and homeostasis, is highly susceptible to injury caused by drugs, toxins, alcohol, and viral infections. Drug-induced liver injury is a significant clinical problem worldwide, representing a major cause of acute liver failure and drug withdrawal from the market.23,24 Conventional pharmacological treatments for liver disorders are often limited, and some synthetic hepatoprotective agents can have side effects or insufficient efficacy.25
Medicinal plants have been traditionally employed for the management of liver disorders in various systems of medicine, including Ayurveda, Unani, and Traditional Chinese Medicine. These plants often contain bioactive phytochemicals such as flavonoids, polyphenols, lignans, terpenoids, and alkaloids that exhibit hepatoprotective, antioxidant, anti-inflammatory, and anti-fibrotic properties.26,27
Scientific studies have validated the hepatoprotective potential of several medicinal plants. For example, Silybum marianum (milk thistle) seeds contain silymarin, which stabilizes hepatocyte membranes, enhances antioxidant defense, and reduces lipid peroxidation.28,29 Curcuma longa (turmeric) rhizome contains curcumin, which modulates inflammatory pathways (NF-kB, TNFα) and activates the Nrf2 mediated antioxidant response.30,31 Other notable hepatoprotective plants include Glycyrrhiza glabra (licorice), Andrographis paniculata, Phyllanthus amarus, Picrorhiza kurroa, and Tinospora cordifolia, which have shown efficacy in both preclinical and clinical studies of drug or toxin induced liver injury.32-37
The hepatoprotective effects of medicinal plants are largely attributed to their ability to:
Scavenge reactive oxygen species (ROS) and enhance endogenous antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT), and glutathione (GSH), Suppress inflammatory mediators, including NF-kB, TNF-α, IL-6, and COX-2, Stabilize hepatocyte membranes and maintain mitochondrial integrity, thereby reducing apoptosis and necrosis.
Modulate drug metabolizing enzymes such as cytochrome P450 (CYP) isoforms to prevent formation of toxic metabolites.38-40
Given their multi-targeted mechanisms and favorable safety profiles, hepatoprotective medicinal plants continue to be an important resource for the development of novel therapeutic agents against DILI and other liver disorders. Their integration into modern medicine requires systematic pharmacological, phytochemical, and clinical evaluation to ensure efficacy and safety.41-43
Table 1. Hepatoprotective Medicinal Plants: Botanical Details, Part Used, Traditional and Modern Uses 1-27
|
Plant Name (Common) |
Botanical Name |
Family |
Plant Used |
Traditional Uses |
Modern/ Scientific Uses |
|
Milk Thistle
|
Silybum marianum
|
Asteraceae |
Seeds |
Treatment of jaundice, liver disorders, gallbladder complaints
|
Antioxidant, Nrf2 activation, ↑GSH, SOD, CAT, hepatocyte membrane stabilization, anti-fibrotic |
|
Turmeric |
Curcuma longa |
Zingiberaceae |
Rhizome |
Liver tonic, anti-inflammatory, wound healing |
Anti-inflammatory (NF-kB inhibition), antioxidant, mitochondrial protection, CYP450 modulation |
|
Licorice
|
Glycyrrhiza glabra |
Fabaceae
|
Root
|
Hepatitis, jaundice, cough remedy |
Anti-inflammatory (↓HMGB1, NF-kB), membrane stabilization, immune modulation |
|
Andrographis
|
Andrographis paniculata
|
Acanthaceae
|
Whole plant, leaves |
Fever, liver disorders, dysentery |
Antioxidant, anti-inflammatory, ↑GST/SOD, hepatocyte protection |
|
Picrorhiza
|
Picrorhiza kurroa
|
Plantaginaceae
|
Rhizome |
Liver disorders, jaundice, chronic hepatitis |
↑ GSH, ↓lipid peroxidation, immune modulatory, protects against anti TB drug induced liver injury |
|
Phyllanthus
|
Phyllanthus amarus
|
Phyllanthaceae
|
Whole plant |
Jaundice, hepatitis, kidney tonic |
CYP2E1 inhibition, antioxidant, hepatocyte regeneration |
|
Green Tea
|
Camellia sinensis
|
Theaceae
|
Leaves |
General health tonic, digestive aid |
Catechins (EGCG): antioxidant, mitochondrial protection, ↓CYP mediated toxic metabolites |
|
Resveratrol source (Grapes)
|
Vitis vinifera |
Vitaceae
|
Fruit/skin |
Blood purifier, liver tonic |
SIRT1/AMPK activation, mitochondrial protection, anti-apoptotic, antioxidant |
|
Ginger
|
Zingiber officinale
|
Zingiberaceae
|
Rhizome |
Stomachic, liver disorders, anti-inflammatory |
Antioxidant, anti-inflammatory, ↓ROS, hepatocyte protection |
|
Aloe vera
|
Aloe barbadensis
|
Asphodelaceae
|
Leaves |
Liver tonic, skin healing |
Anti-inflammatory, antioxidant, hepatocyte regeneration, protects against drug induced liver injury |
|
Berberis
|
Berberis aristata
|
Berberidaceae
|
Root, bark |
Jaundice, liver tonic |
Activates AMPK, antioxidant, anti-inflammatory, mitochondrial protection |
|
Guduchi
|
Tinospora cordifolia
|
Menispermaceae
|
Stem, leaves |
Jaundice, fever, liver disorders |
↑ Antioxidant enzymes, immune modulatory, hepatoprotective |
|
Black Cumin
|
Nigella sativa |
Ranunculaceae
|
Seeds |
Liver tonic, jaundice, digestive aid |
Thymoquinone: antioxidant, anti-inflammatory, protects against Hepatotoxicity |
BIOACTIVE PHYTOCONSTITUENTS
The hepatoprotective efficacy of medicinal plants is primarily attributed to their diverse bioactive phytoconstituents, which act on multiple molecular targets involved in drug induced liver injury (DILI).Among these, flavonoids, phenolics (polyphenols), and terpenoids are the most extensively studied classes and have demonstrated consistent protective effects in experimental and clinical models of liver injury. Their pleiotropic actions enable modulation of oxidative stress, inflammation, mitochondrial dysfunction, and impaired detoxification pathways that collectively contribute to DILI.14,25
Flavonoids:
Flavonoids constitute one of the largest classes of plant secondary metabolites and are ubiquitously present in hepatoprotective medicinal plants such as Silybum marianum, Phyllanthus amarus, Camellia sinensis, and Curcuma longa. Structurally, flavonoids possess a C6-C3-C6 skeleton, consisting of two aromatic rings connected by a heterocyclic pyran ring, with variations in hydroxylation, methylation, and glycosylation patterns influencing biological activity.40
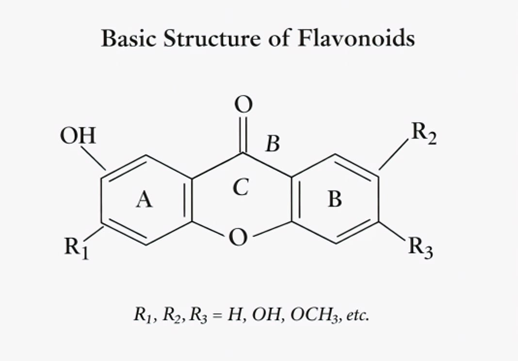
Fig.4 Basic Structure of Flavonoids.44
Mechanisms of Hepatoprotection
Flavonoids exert hepatoprotective effects mainly through:
Direct scavenging of reactive oxygen species (ROS) and reactive nitrogen species, Up regulation of endogenous antioxidant defenses via activation of the Nrf2-ARE signaling pathway, leading to increased expression of superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), and glutathione (GSH), Inhibition of inflammatory signaling pathways, particularly NF-kB, resulting in reduced expression of TNF-α, IL-1β, IL-6, and COX-2, Stabilization of hepatocyte membranes and prevention of lipid peroxidation.29,42,45
Examples:
Quercetin and kaempferol have demonstrated protective effects against acetaminophen (paracetamol) and anti tubercular drug-induced hepatotoxicity by reducing oxidative stress and suppressing inflammatory mediators.42 Silybin, the major flavonolignan component of silymarin, enhances hepatocyte regeneration and inhibits fibrogenesis, making it one of the most clinically relevant flavonoids in liver therapy.28,29
Phenolics and Polyphenols:
Phenolic compounds are characterized by one or more hydroxyl groups attached to aromatic rings, enabling efficient electron donation and free radical neutralization. Polyphenols such as curcumin, resveratrol, gallic acid, and ellagic acid are abundant in hepatoprotective plants and exhibit broad spectrum liver protective activity.31
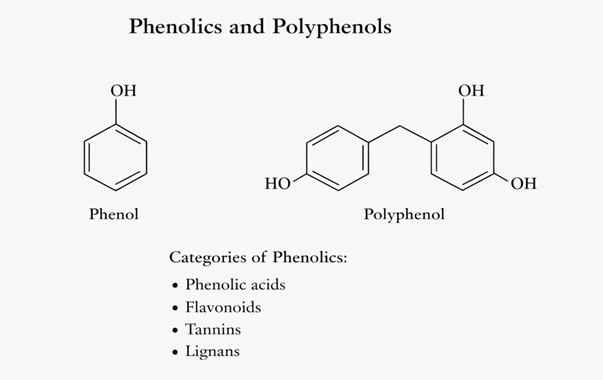
Fig.5 Phenol group & Polyphenol.46
Mechanisms of Hepatoprotection
Phenolics protect the liver through:
Inhibition of lipid peroxidation and oxidative membrane damage, Chelation of transition metals, reducing Fenton reaction mediated ROS generation, Modulation of inflammatory and apoptotic pathways, including NF-kB, MAPK, and caspase cascades, Preservation of mitochondrial membrane potential, thereby preventing hepatocyte apoptosis and necrosis.30,47
Examples:
Curcumin from Curcuma longa has been extensively studied for its ability to suppress NF-kB activation, reduce pro-inflammatory cytokine production, and activate Nrf2 mediated antioxidant defenses in models of DILI.31 Resveratrol from Vitis vinifera protects against mitochondrial dysfunction and enhances cellular energy homeostasis through activation of SIRT1 and AMPK signaling pathways.36
Terpenoids:
Terpenoids are a structurally diverse class of compounds derived from isoprene units and include mono-, di-, tri-, and tetraterpenes. Hepatoprotective terpenoids such as andrographolide, glycyrrhizin, oleanolic acid, and ursolic acid are widely distributed in medicinal plants used for liver disorders.48
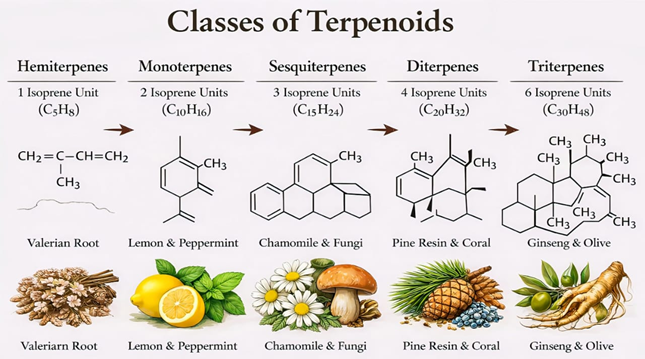
Fig.6 Schematic draw of terpenoid classes.48
Mechanisms of Hepatoprotection
Terpenoids exert hepatoprotective actions by:
Inducing phase II detoxification enzymes such as glutathione S-transferase (GST) and UDP-glucuronosyl transferase (UGT), Suppressing inflammatory mediators and immune mediated liver injury, Protecting mitochondrial integrity and inhibiting hepatocyte apoptosis, Reducing fibrosis through modulation of hepatic stellate cell activation.37,49
Examples:
Andrographolide from Andrographis paniculata has shown efficacy against drug-induced hepatotoxicity by enhancing antioxidant defenses and suppressing inflammatory cytokines.50 Glycyrrhizin from Glycyrrhiza glabra exhibits membrane-stabilizing and immunomodulatory effects, contributing to its clinical use in chronic liver diseases.32
Structure-Activity Relationship (SAR) Considerations
The hepatoprotective potential of phytoconstituents is strongly influenced by their chemical structure. Hydroxyl groups, conjugated double bonds, and α,β-unsaturated carbonyl moieties enhance antioxidant and anti-inflammatory activity, while glycosylation affects solubility and bioavailability. Understanding SAR relationships aids in identifying lead compounds and optimizing phytochemical based hepatoprotective therapies.27,43
MECHANISMS OF HEPATOPROTECTIVE BY PLANT-DERIVED COMPOUNDS
Antioxidant defense enhancement
A major protective mechanism is reduction of oxidative stress through scavenging ROS and enhancing endogenous antioxidant defenses. Activation of the Nrf2 pathway leads to up regulation of antioxidant enzymes such as SOD, catalase, glutathione peroxidase, and HO-1.51,52 Many phytochemicals (curcumin, silymarin, resveratrol) have been shown to stimulate this pathway.51,53,54
Anti-inflammatory effects
Inflammation is central to progression of liver injury. Phytoconstituents can inhibit NF-kB activation, suppress pro-inflammatory cytokines (TNF-α, IL-6), and reduce COX-2 and iNOS expression, limiting immune mediated damage.39,47,54
Modulation of CYP450 enzyme
CYP450 enzymes can generate reactive metabolites. Certain plant compounds modulate CYP activity, reducing formation of toxic intermediates. However, this also raises herb-drug interaction risks.15,55 For example, silymarin and curcumin may influence CYP3A4 and other isoforms.55,56
Enhancement of detoxification enzymes
Phase II conjugation enzymes like GST and UGT detoxify reactive metabolites. Many plant extracts enhance these enzymes, improving clearance and reducing cellular damage.52,57
Mitochondrial protection and Anti-apoptotic action
Plant compounds can preserve mitochondrial membrane potential, reduce lipid peroxidation, prevent cytochrome release, and suppress caspase activation, thereby reducing apoptosis and necrosis.16,18,58
Table 2. Phytochemicals and Their Hepatoprotective Mechanisms
|
Phyto- Chemical |
Plant Source |
Chemical Class |
Structural Feature (SAR) |
Mechanisms of hepatoprotection |
DILI model |
Clinical relevance |
|
Silibinin (Silymarin) |
Silybum marianum |
Flavono-lignan |
Phenolic rings, dioxane structure |
Activates Nrf2/ARE pathway → ↑ GSH, SOD, CAT, ↓ lipid peroxidation, anti-fibrotic, membrane stabilization. |
APAP, CCl?, anti-TB drugs
|
Widely used hepato-protective, clinical evidence available |
|
Curcumin |
Curcuma longa |
Poly-phenol |
β-diketone moiety, phenolic OH groups |
Antioxidant & anti-inflammatory → Inhibits NF-kB, TNF-α,activates Nrf2, mitochondrial protection, anti-fibrotic |
APAP, MTX, INH RIF |
Bioavailability limits clinical use |
|
Glycyrrhizin |
Glycyrrhiza glabra |
Tri-terpenoid saponin |
Glycosidic triterpene backbone |
HMGB1 inhibition → Modulates cytokines, membrane stabilization, immune modulatory action. |
Viral hepatitis drug induced injury
|
Approved injectable in some countries |
|
Andrograph-olide |
Andrographis paniculata |
Di- terpenoid lactone |
Lactone ring, hydroxyl groups |
Enhances antioxidant enzymes → ↑GST,SOD, ↓RO, suppresses inflammation, hepatoprotection. |
APAP, ethanol |
Traditional use, preclinical evidence |
|
Resveratrol |
Grapes, berries |
Stilbene |
Multiple hydroxyl groups |
Activates SIRT1/AMPK mitochondrial biogenesis, ↓oxidative stress and apoptosis |
APAP, ethanol |
Nutraceutical potential |
|
Quercetin |
Fruits, vegetables |
Flavonoid |
Catechol structure in B-ring |
ROS scavenging, inhibits lipid peroxidation, ↓ TNF-α, IL1β |
APAP, CCl? |
Dietary flavonoid |
|
EGCG |
Camellia sinensis |
Flavan-3-ol |
Gallate ester |
Antioxidant, ↓CYP mediated bioactivation, mitochondrial stabilization |
APAP |
Dose-dependent hepatoprotection |
|
Picroside I & II
|
Picrorhiza kurroa
|
Iridoid glycosides
|
Glycosidic iridoid nucleus
|
↑ GSH, ↓lipid peroxidation, immune modulation |
INH-RIF
|
Used in Ayurveda |
|
Phyllanthin
|
Phyllanthus amarus
|
Lignan
|
Methylenedioxy phenyl rings
|
↓ CYP2E1, antioxidant defense, hepatocyte regeneration |
APAP ethanol
|
Traditional hepatoprotective |
|
Berberine
|
Berberis spp.
|
Isoquinoline alkaloid
|
Quaternary ammonium structure
|
Activates AMPK, ↓oxidative stress, anti-inflammatory |
MTX, APAP
|
Emerging clinical interest |
|
Luteolin
|
Medicinal plants |
Flavone
|
Hydroxylated flavone
|
Inhibits NF-kB/MAPK, antioxidant and anti-inflammatory |
APAP
|
Preclinical evidence |
|
Kaempferol
|
Fruits, vegetables
|
Flavonol
|
Hydroxy-lated flavonol
|
↓ apoptosis, ↑antioxidant enzymes, hepatocyte protection |
APAP
|
Dietary relevance |
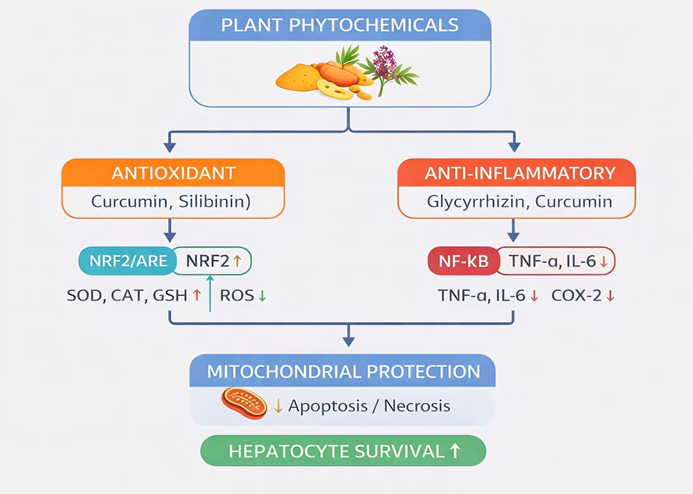
Fig.7 Mechanism of hepatoprotection by Plant- Derived Compounds.59
PRECLINICAL AND CLINICAL EVIDENCE
Overview: What Is DILI & How Plant Compounds Help
Drug?Induced Liver Injury (DILI):
DILI occurs when medications (e.g., acetaminophen/paracetamol, isoniazid, rifampicin, methotrexate, chemotherapeutic agents) cause liver damage by increasing oxidative stress, inflammation, apoptosis, or mitochondrial dysfunction. There are currently no fully approved, highly effective pharmacologic therapies for DILI, which has encouraged research into natural, plant?derived hepatoprotective agents.11
Plant?derived hepatoprotective agents work through multiple mechanisms including:
Antioxidant activity (scavenging free radicals), Anti?inflammatory effects, Restoration of mitochondrial function, Modulation of cellular stress signaling (e.g., Nrf2, NF?kB), Anti?apoptotic and cell?protective effects.11
Preclinical Evidence (Animal & Cell Models)
Silymarin (from Silybum marianum):
In animal models (rats, mice, pigs), silymarin reduces biochemical markers of liver damage (ALT, AST), limits oxidative stress, and improves histopathological outcomes in hepatotoxicity models (e.g., acetaminophen, anti?tuberculosis drugs).60
Mechanistic evidence shows silymarin scavenges free radicals, stabilizes hepatocyte cell membranes, and supports hepatocyte regeneration.11
In a recent pig model, silymarin reduced liver dysfunction markers and supported structural liver protection, highlighting relevance beyond rodent models.45
Mechanistic pathways observed in preclinical studies include:
Activation of Nrf2/ARE antioxidant pathways, Down regulation of NF-kB mediated inflammation, Enhanced glutathione and other detoxifying enzymes.60
Flavonoids & Phenolic compounds:
Plant flavonoids like quercetin, baicalin, naringin, ferulic acid, gastrodin, ursolic acid, and catalpol have shown protective effects in animal models of drug-induced liver damage.
Table 3. Selected Plant-Derived Compounds and Their Preclinical Mechanisms in Drug-Induced Liver Injury (DILI) 11
|
Compound |
Source |
Mechanism (Preclinical) |
|
Quercetin |
vegetables, fruits |
Antioxidant, modulation of Nrf2/HO?1, mitigates oxidative injury. |
|
Baicalin |
Scutellaria baicalensis |
Promotes hepatocyte regeneration, influences Nrf2 & mTOR pathways. |
|
Naringin |
citrus fruits |
Up regulates SIRT1, inhibits apoptosis & inflammation. |
|
Ferulic acid |
grains & plants |
Reduces oxidative stress & inflammatory cytokines. |
|
Gastrodin |
Gastrodia elata |
Limits cytokines & oxidative stress via ERK/JNK/MAPK, Nrf2. |
|
Ursolic acid |
many plant families |
Modulates detoxifying enzymes, reduces oxidative stress. |
|
Catalpol |
Rehmannia species |
Suppresses autophagy, activates detox pathways. |
These compounds consistently reduce serum liver enzymes, limit histological damage, and boost antioxidant defenses in DILI animal models.11
Clinical Evidence (Human Studies)
Silymarin: Most Extensively Studied
Prevention of Anti Tuberculosis DILI (Anti TB DILI) :
A meta analysis of randomized clinical trials in TB patients taking hepatotoxic anti TB medications (e.g., isoniazid, rifampicin):
Silymarin significantly reduced the incidence of anti?TB DILI at 4?weeks compared to placebo, It also decreased ALT, AST, and ALP levels, reflecting improved liver function, The protective effect was observed early (week 4), though long?term prevention beyond 8?weeks was less clear, Silymarin was well tolerated with no significant increase in adverse events vs. placebo.11
General DILI & Hepatoprotective support:
Clinical studies indicate that in patients with drug induced liver injuries (including non TB contexts and metabolic liver conditions), silymarin was associated with improvements in liver enzyme profiles and liver related outcomes.11
Some clinical trials have shown lower ALT, AST, and GGT in Silymarin treated patients vs. control, suggesting hepatic enzyme normalization during toxin exposure.11
Summary of clinical silymarin evidence:
Beneficial in short term DILI prevention (anti TB drugs)
Improves liver biochemical markers
Generally safe with few adverse effects.11
Clinical caveats: Evidence strength varies. While meta analyses support protective effects in anti TB DILI, more large scale, well controlled clinical trials are needed for broader DILI contexts.
Other plant compounds: Clinical data limited:
Most non-silymarin compounds (e.g., quercetin, naringin, baicalin) have strong preclinical support but limited clinical trial evidence specifically in DILI patients. This highlights the need for translational studies bridging preclinical promise to human efficacy.11
Molecular mechanisms underlying hepatoprotection
Plant derived compounds exert hepatoprotective effects via multiple molecular pathways:
Oxidative stress & Antioxidant defence:
Activation of Nrf2/ARE pathway increases detox enzymes (e.g., HO?1), Direct free radical scavenging reduces lipid peroxidation & Increased glutathione and superoxide dismutase levels.60
Inflammation modulation:
Down regulation of NF-kB reduces pro?inflammatory cytokines (TNF-α, IL-1β). Many phytochemicals also suppress MAPK and JNK signaling pathways.11
Apoptosis & Cellular protection:
Prevention of apoptosis via modulation of Bcl?2 family proteins and caspase cascades, Preserves mitochondrial membrane integrity and function.60
Detoxification & Metabolism:
Up regulation of phase?II detoxifying enzymes, Potential stabilization of cell membranes against Xenobiotic insults.60
Clinical considerations & Future directions
Safety:
Most plant compounds (especially silymarin) are well tolerated at studied doses. However, not all herbal products are safe-quality, contamination, and adulteration can affect outcomes. Rigorous product standardization is crucial.11
Evidence Gaps:
Numerous preclinical studies show efficacy in animal models. Human clinical evidence beyond silymarin remains limited and needs robust RCTs.
Research Needs:
Standardized clinical trials with clear definitions of DILI, Dose optimization studies for phytochemicals like quercetin, naringin, baicalin, Investigations into combinations of compounds that may synergize mechanisms.
SAFETY, TOXICITY & HERB-DRUG INTERACTIONS
Plant derived hepatoprotective agents are widely perceived as safe due to their natural origin and traditional use. However, “natural = safe” is a misconception, several herbal extracts can cause toxicity, especially at high doses, with chronic use, or when co administered with conventional drugs. This section critically evaluates toxicity profiles, safety considerations, mechanisms of adverse effects, and clinically relevant herb-drug interactions of major phytoconstituents reviewed earlier (flavonoids, phenolics, terpenoids) in the context of DILI prevention.
Although medicinal plants and their bioactive phytoconstituents are widely perceived as safe due to their natural origin, increasing evidence indicates that herbal products can cause hepatotoxicity or interact with conventional drugs, particularly when used indiscriminately or concomitantly with hepatotoxic medications. Therefore, evaluation of safety, toxicity, and herb-drug interactions is essential before integrating hepatoprotective medicinal plants into modern therapeutic regimens.25,61
Safety profile of Hepatoprotective medicinal plants
Most hepatoprotective medicinal plants demonstrate a favorable safety margin at therapeutic doses, supported by long-term traditional use and experimental studies. For example, Silybum marianum (milk thistle) and its active constituent silymarin have been extensively evaluated in clinical trials and are generally well tolerated, even with prolonged administration.29,41 Mild adverse effects such as gastrointestinal discomfort, headache, and allergic reactions have occasionally been reported but are usually self limiting.
Similarly, Curcuma longa (turmeric) and curcumin exhibit high safety, with human studies reporting no serious toxicity even at doses up to 8–12 g/day. However, poor bioavailability often necessitates high doses or formulation strategies, which may influence safety profiles.54 Other plants such as Andrographis paniculata, Phyllanthus amarus, Picrorhiza kurroa, and Tinospora cordifolia are also considered relatively safe when used within recommended dose ranges.35,45,50,62
Toxicity concerns associated with herbal hepatoprotective
Despite their benefits, herb-induced liver injury has emerged as an important clinical concern. Certain medicinal plants or their formulations may cause hepatotoxicity due to: Overdose or prolonged use, Poor quality control or contamination (heavy metals, pesticides, adulterants), Misidentification of plant species and Individual susceptibility or genetic polymorphisms.
Green tea (Camellia sinensis) extracts rich in epigallocatechin gallate have been associated with rare cases of hepatotoxicity, particularly at high doses used in weight loss supplements. The toxicity is thought to be related to mitochondrial dysfunction and oxidative stress at supra-physiological concentrations.63,64
Likewise, excessive intake of glycyrrhizin from Glycyrrhiza glabra may lead to pseudoaldosteronism, characterized by hypertension, hypokalemia, and fluid retention, indirectly affecting hepatic and systemic homeostasis.65
Herb-drug interactions in drug-induced liver injury
Herb-drug interactions are of particular concern in patients receiving potentially hepatotoxic drugs such as anti tubercular agents, anti-epileptics, anticancer drugs, and anti- retrovirals. Many phytochemicals influence drug metabolizing enzymes and transporters, thereby altering pharmacokinetics and toxicity profiles.66
Interaction with cytochrome P450 enzymes
Several hepatoprotective phytoconstituents modulate CYP450 enzymes:
Silymarin inhibits CYP3A4 and CYP2C9, potentially increasing plasma levels of drugs such as warfarin, phenytoin, and statins.67 Curcumin inhibits CYP1A2, CYP2C9, and CYP3A4, which may alter the metabolism of acetaminophen, NSAIDs, and chemotherapeutic agents.68 Quercetin and resveratrol can inhibit CYP3A4 and CYP2C8, leading to altered drug clearance.36 These interactions may be beneficial in reducing toxic metabolite formation but may also increase the risk of adverse drug reactions if not monitored.
Interaction with drug transporters
Phytochemicals may also affect hepatic transporters such as P-glycoprotein and organic anion transporting polypeptides. For instance, silymarin and glycyrrhizin have been shown to modulate P-gp activity, influencing drug absorption and biliary excretion.69
Clinical implications and Regulatory considerations
From a clinical perspective, hepatoprotective medicinal plants should be:
Used at standardized doses, Prescribed with caution in patients on poly pharmacy, Avoided in individuals with pre-existing severe liver disease unless supported by clinical evidence, Regulatory agencies increasingly emphasize pharmacovigilance of herbal medicines, including mandatory reporting of adverse events and herb- induced liver injury. Rigorous toxicological evaluation, standardization, and clinical trials are essential to ensure the safe integration of medicinal plants into evidence based medicine.70-72
REGULATORY CLINICAL CHALLENGES
Regulatory frameworks for herbal medicines differ across countries. Many plant-based hepatoprotectives are marketed as dietary supplements rather than medicines, limiting requirements for rigorous clinical trials.73,74 Challenges include: Lack of standardized formulations and dose optimization, Inadequate long-term toxicity data,Variable endpoints in clinical trials, Difficulty distinguishing protective effects from spontaneous recovery after drug discontinuation.5,74 Integration into clinical practice requires evidence based guidelines, validated biomarkers, and robust pharmacovigilance systems.2,75
CONCLUSION
Plant-derived hepatoprotective compounds offer promising multi target strategies for preventing and mitigating drug induced liver injury. Through antioxidant, anti-inflammatory, mitochondrial protective, and detoxification enhancing mechanisms, phytochemicals such as silymarin, curcumin, glycyrrhizin, and picrosides may reduce susceptibility to DILI. However, limitations in clinical evidence, product standardization, and safety concerns such as herb-induced liver injury and herb-drug interactions must be addressed. With rigorous clinical trials, quality controlled formulations, and mechanistic validation, plant-based hepatoprotectives may emerge as valuable adjuncts in preventing DILI in high-risk patients.
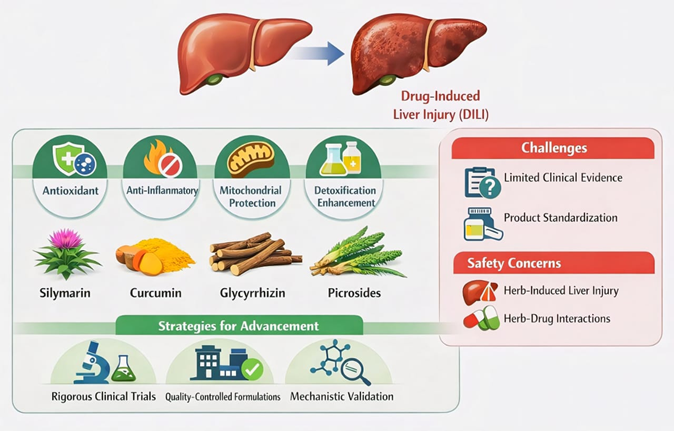
Fig.8 Plant-Based Hepatoprotectives for DILI Prevention.76
ABBREVATION
REFERENCES

Krishna Patel, Bagga Nirvair Kaur, Khushbu Tapodhan, Dr. Kinjal Patel, Plant-Derived Hepatoprotective Compounds in the Prevention of Drug Induced Liver Injury: Mechanisms, Evidence, Safety, and Future Directions, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 2425-2444. https://doi.org/10.5281/zenodo.19142868
 10.5281/zenodo.19142868
10.5281/zenodo.19142868
