
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
NRI College of Pharmacy, Pothavarappadu, Agiripalli, Eluru
The escalating burden of non-communicable diseases (NCDs), aging populations, and rising healthcare costs have placed immense pressure on healthcare systems worldwide. Traditional treatment-focused models are increasingly unsustainable, necessitating a strategic pivot toward preventive medicine and the application of pharmacoeconomic principles. This review explores how the integration of these two disciplines can shape more equitable, efficient, and sustainable healthcare systems globally. Preventive medicine emphasizes proactive health promotion, risk reduction, and early detection of disease, reducing the need for high-cost interventions and improving population health outcomes. Pharmacoeconomics provides tools to evaluate the value of medical interventions in terms of both cost and effectiveness, guiding policymakers in making evidence-based decisions that ensure the optimal use of limited resources. The article outlines key concepts, tools, and methodologies within both fields, including cost-effectiveness analysis, quality-adjusted life years (QALYs), and return on investment (ROI). It also discusses the integration of preventive strategies into health policy, the role of Pharmacoeconomics in public health decision-making, and real-world applications from countries such as Thailand, the United Kingdom, Brazil, and India. Challenges such as delayed economic returns, underfunding, data limitations, and political resistance are also critically examined. Looking ahead, the article highlights the potential of digital health, genomics, and global health technology assessments in enhancing preventive care delivery. It concludes that the convergence of preventive medicine and Pharmacoeconomics is not merely desirable but essential for the future of global healthcare. This integrated approach has the potential to transform health systems into more resilient, cost-effective, and patient-centred models, ensuring long-term health security and sustainability
Healthcare systems across the globe are undergoing a profound transformation. This shift is driven by a complex interplay of factors demographic transitions characterized by aging populations, rapid urbanization, epidemiological shifts toward non-communicable diseases (NCDs), increasing life expectancy, and growing public awareness of health and wellness. According to the United Nations, by 2050, one in six people globally will be over the age of 65, leading to a dramatic rise in age-related diseases and chronic conditions [1]. As these changes unfold, they exert mounting pressure on healthcare infrastructures, many of which are already financially strained.
Healthcare expenditures continue to rise globally, reaching over 10% of global GDP in recent years, with even higher rates in high-income countries [2]. This increasing financial burden, driven largely by the cost of treating chronic conditions, expensive pharmaceutical innovations, and hospital-based care, has rendered many traditional curative healthcare models unsustainable. In particular, the high costs of long-term treatments for diseases such as diabetes, cardiovascular conditions, and cancer are proving overwhelming for both governments and individuals, especially in low- and middle-income countries (LMICs). These challenges underscore the urgent need to reimagine healthcare delivery models in ways that emphasize prevention, health promotion, and efficient resource utilization.
Preventive Medicine: Proactive Healthcare for Population Well-being
Preventive medicine is a proactive approach to health that focuses on averting disease before it occurs or progresses. It encompasses a spectrum of strategies including immunizations, health education, screening programs, environmental safety, behavioural interventions, and public health legislation. The discipline is typically categorized into three hierarchical levels:
Numerous studies support the effectiveness of preventive medicine. For example, early detection of colorectal cancer through faecal occult blood testing has been shown to reduce mortality by up to 33% [3]. Similarly, tobacco taxation and public smoking bans have significantly reduced smoking rates and associated morbidity [4]. Such interventions demonstrate not only health benefits but also economic savings by reducing hospitalizations and costly treatments.
Despite the clear advantages, preventive medicine remains underutilized in many healthcare systems, often due to fragmented policies, insufficient funding, and lack of political commitment. In resource-limited settings, where the burden of disease is highest, prevention remains a neglected pillar due to competing priorities and budgetary constraints.
Figure 1: Importance Of Preventive Medicine.
Pharmacoeconomics: Value-Based Decision-Making in Healthcare
Pharmacoeconomics is a vital subfield of health economics that evaluates the comparative value of pharmaceutical products and healthcare interventions by analysing their cost-effectiveness, utility, and benefit relative to their outcomes. In an era where drug prices are rapidly escalating and budgets are limited, pharmacoeconomic evaluations help determine which treatments provide the best value for money.
Pharmacoeconomic analyses include:
These methodologies are instrumental in health policy formulation, particularly in determining drug reimbursement schemes and public funding allocations. Countries such as the UK, Canada, and Australia have institutionalized Pharmacoeconomics through agencies like NICE (National Institute for Health and Care Excellence), which mandates that only interventions meeting specific cost-effectiveness thresholds are reimbursed under public health systems [5].
Pharmacoeconomics is also gaining relevance in LMICs where resources are particularly scarce. For instance, in Thailand, the Health Intervention and Technology Assessment Program (HITAP) has been pivotal in guiding decisions for the Universal Coverage Scheme (UCS), ensuring that publicly funded services are both effective and affordable [6].
Figure 2: Importance Of Pharmacoeconomics
Converging Disciplines: A Framework for Sustainable Healthcare
The integration of preventive medicine with Pharmacoeconomics offers a promising framework for sustainable healthcare reform. Preventive strategies are often more cost-effective than curative approaches, but their value can be difficult to quantify without robust economic evaluation. When pharmacoeconomic tools are applied to preventive interventions, policymakers are better equipped to allocate resources toward programs that offer the greatest health benefits per unit of cost.
For example, pharmacoeconomic studies have confirmed the long-term cost-effectiveness of:
These findings highlight how the convergence of prevention and economic evaluation not only improves individual and population health but also safeguards public health budgets from long-term inflationary pressures.
Table 1: Economic Return on Preventive Health Interventions.
|
Intervention |
Estimated ROI |
Source/Country |
|
Childhood immunization |
$16–$44 per $1 invested |
Global (The Lancet) |
|
Workplace wellness programs |
$3.27 (medical) and $2.73 (productivity) per $1 invested |
United States |
|
Tobacco control policies |
High long-term returns |
WHO Global Estimates |
|
Diabetes prevention (lifestyle change) |
High ROI through delayed onset |
United States |
|
HPV vaccination |
Cost-effective and life-saving |
Thailand, UK |
Lessons from the COVID-19 Pandemic
The COVID-19 pandemic underscored the fragility of global healthcare systems and the consequences of underinvesting in preventive infrastructure. Countries that had robust surveillance systems, stockpiles of critical supplies, strong public health communication, and universal health coverage were far better positioned to respond rapidly and effectively. In contrast, others faced overwhelming demand on hospitals, shortages of essential supplies, and soaring mortality rates.
Moreover, the pandemic highlighted the critical role of economic modelling in public health decision-making. Forecasts based on pharmacoeconomic models influenced decisions about vaccine rollout strategies, lockdowns, and allocation of critical care resources. It became abundantly clear that prevention and preparedness are not optional they are essential pillars of health security.
Global Burden of Disease and Healthcare Spending:
The global health landscape has witnessed a dramatic shift over recent decades from a predominance of infectious diseases to the rising tide of non-communicable diseases (NCDs). Conditions such as cardiovascular diseases, diabetes, cancer, and chronic respiratory illnesses now account for over 70% of all global deaths, according to the Global Burden of Disease Study 2020 [11]. This epidemiological transition, although reflective of medical progress and rising life expectancy, has placed enormous and often unsustainable financial demands on health systems worldwide.
The Economic Toll of NCDs:
Managing chronic diseases is inherently resource-intensive. It requires long-term medication, frequent monitoring, specialist consultations, and often expensive interventions such as surgeries or dialysis. These direct medical costs are compounded by indirect costs, which include:
The World Economic Forum and Harvard School of Public Health have projected that the global economic burden of NCDs could exceed $30 trillion by 2030, equivalent to nearly half of global GDP in 2010 [12]. For low- and middle-income countries (LMICs), this growing burden threatens to derail economic development, overwhelm public health budgets, and exacerbate health inequities.
In high-income countries, the scenario is similarly concerning. For instance, in the United States, it is estimated that 90% of the nation’s $4.1 trillion annual healthcare spending is attributable to people with chronic and mental health conditions [13]. These unsustainable cost trajectories underscore the need for a strategic pivot from curative to preventive health systems.
Reactive Systems vs. Proactive Investment:
Countries with fragmented, hospital-centric, and reactive healthcare delivery models often face runaway expenditures. These systems prioritize treatment over prevention and frequently lack integration across public health, primary care, and insurance systems.
Preventive interventions such as routine screenings, immunizations, early diagnosis programs, and community health education have been shown to be cost-effective or even cost-saving. A landmark study by the Trust for America's Health found that an investment of just $10 per person per year in proven community-based prevention programs could save the United States over $16 billion annually within five years [14].
Moreover, health promotion campaigns, such as anti-smoking efforts or public nutrition education, are among the most cost-effective tools in the public health arsenal. For every dollar spent on tobacco control, it is estimated that governments can save up to $55 in healthcare costs and productivity gains [15].
Preventive Medicine and Universal Health Coverage:
Global momentum is building toward Universal Health Coverage (UHC) a commitment to ensuring all people receive needed health services without financial hardship. However, achieving UHC is not feasible without strong preventive strategies. Preventive care improves population health and reduces overall healthcare costs, making it a critical component of sustainable UHC implementation.
International organizations such as the World Health Organization (WHO), World Bank, and United Nations increasingly advocate for integrating preventive services into essential health benefit packages. The WHO’s “Best Buys” initiative identifies interventions such as salt reduction, tobacco taxation, and cervical cancer screening that are highly cost-effective and feasible for low-resource settings [16].
The Dual Burden in LMICs:
While NCDs dominate global mortality, many LMICs continue to face a dual burden grappling with infectious diseases like tuberculosis, malaria, and HIV alongside rising NCD prevalence. This scenario leads to compounded strain on healthcare resources, requiring versatile and integrated public health approaches.
Cost-effective solutions in these regions may include:
For example, India’s national health mission has adopted multipronged strategies, including Health and Wellness Centres (HWCs), which provide screenings for diabetes, hypertension, and certain cancers while continuing infectious disease control [17]. These integrated approaches ensure better resource utilization and long-term cost containment.
Lessons from Global Success Stories:
Several countries provide empirical evidence that strategic investment in prevention reduces costs and improves outcomes:
These programs share common features: government commitment, data-driven planning, multi-sectoral collaboration, and long-term investment horizons. They serve as reproducible models for countries seeking to balance cost containment with health equity.
Economic Modelling and Policy Design:
The inclusion of pharmacoeconomic evaluation in healthcare policy design is accelerating. Governments, insurers, and international donors increasingly demand that health interventions be assessed not only for clinical efficacy but also for economic value. This approach enables:
Tools like Incremental Cost-Effectiveness Ratios (ICERs) and Quality-Adjusted Life Years (QALYs) are now commonly used in decisions ranging from national formulary inclusion to benefit package design.
Global Collaboration and Funding for Prevention:
Preventive care often requires upfront investment, making external funding and technical assistance critical especially in low-resource settings. Agencies such as:
These collaborative efforts, backed by rigorous economic evaluations, have reshaped global health financing priorities, shifting more funds toward long-term prevention rather than short-term cure.[18]
Concepts of Preventive Medicine:
Preventive medicine is a cornerstone of public health that aims to protect, promote, and maintain health and well-being while preventing disease, disability, and premature death. It operates on the principle that preventing health problems before they occur or detecting them early when they are most treatable is far more effective and economical than managing full-blown illnesses. The discipline combines epidemiology, environmental health, behavioural sciences, biostatistics, and health services management to inform evidence-based public health strategies [19].
The practice of preventive medicine is typically stratified into three primary levels, each targeting different phases of disease progression, and now increasingly includes a fourth quaternary prevention in response to modern challenges.
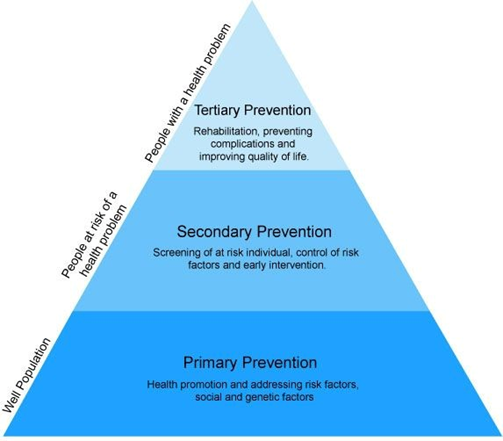
Figure 3: Levels of Prevention in Preventive Medicine.
Primary Prevention: Stopping Disease Before It Starts
Primary prevention seeks to eliminate or mitigate risk factors before a disease or injury occurs. It encompasses a range of public health and clinical interventions designed to build population resilience and remove triggers of illness. Examples include:
The economic and social benefits of primary prevention are well-documented. According to the WHO, every dollar invested in tobacco control yields an average return of $7 in healthcare savings and productivity gains [14]. Immunizations are among the most cost-effective health interventions, with childhood vaccines alone preventing over 2 million deaths globally each year [20].
Secondary Prevention: Early Detection and Timely Intervention
Secondary prevention focuses on the early identification and treatment of asymptomatic diseases or risk factors. It aims to halt or slow the progression of disease through routine screening and early intervention.
Examples include:
Secondary prevention is critical for NCDs, which often develop silently. Early detection can lead to timely treatment, improved outcomes, and reduced healthcare costs. For instance, the U.S. Preventive Services Task Force (USPSTF) found that regular screening for colorectal cancer can reduce mortality by up to 68% [21].
In low- and middle-income countries, task-shifting strategies such as training community health workers to perform screenings can improve access and cost-effectiveness.
Tertiary Prevention: Managing Chronic Conditions
Tertiary prevention deals with the management of established disease to prevent complications, reduce disability, and improve quality of life. It includes:
The objective is to reduce disease impact and help individuals maintain function. For example, structured cardiac rehabilitation programs have been shown to reduce the risk of secondary cardiac events and improve life expectancy in patients with coronary artery disease [22].
Quaternary Prevention: Avoiding Overmedicalization
Quaternary prevention is a more recent concept, introduced to address the growing concern of unnecessary medical interventions, overdiagnosis, and overtreatment. In today’s consumer-driven and defensive medical environment, patients are often exposed to redundant tests, surgeries, or medications that do not improve outcomes and may cause harm.
This level of prevention involves:
For instance, routine PSA screening for prostate cancer in asymptomatic men has been questioned due to high rates of false positives and unnecessary procedures. A quaternary prevention approach promotes careful assessment and restraint in such cases[23].
Table 2: Levels of Preventive Medicine and Their Applications.
|
Level of Prevention |
Definition |
Examples |
Economic Impact |
|
Primary Prevention |
Prevents onset of disease |
Vaccinations, tobacco control, health education |
Reduces incidence and future treatment costs |
|
Secondary Prevention |
Early disease detection |
Cancer screenings, hypertension/diabetes screening |
Limits progression, lowers hospitalization costs |
|
Tertiary Prevention |
Reduces impact of disease |
Rehabilitation, chronic disease management |
Improves quality of life, prevents complications |
|
Quaternary Prevention |
Avoids over-medicalization |
Avoiding unnecessary treatments |
Minimizes waste and adverse effects |
Vehicles for Preventive Medicine Implementation
Several public health programs serve as operational platforms for preventive medicine across society:
Immunization Campaigns:
Programs such as GAVI’s vaccination efforts in LMICs and routine childhood immunizations in developed countries have substantially reduced morbidity and mortality from vaccine-preventable diseases.
Health Promotion and Education:
Mass media campaigns, community outreach, and school-based programs encourage healthy behaviours. Examples include anti-smoking ads, sexual health education, and digital platforms promoting mental wellness.
Environmental Health Initiatives:
Ensuring access to clean air, water, and sanitation is vital. Poor environmental conditions remain a major contributor to preventable disease burden, especially in urban slums and rural areas.
Nutritional Interventions:
Programs addressing malnutrition, obesity, and micronutrient deficiencies are particularly important in populations facing food insecurity. Strategies include food fortification, school meal programs, and public awareness initiatives.
Surveillance and Early Warning Systems:
A vital aspect of preventive medicine is disease surveillance collecting, analysing, and disseminating data to detect outbreaks or shifts in health trends. Real-time surveillance was key to identifying COVID-19 hotspots, guiding public health interventions, and deploying resources efficiently.
Systems like Integrated Disease Surveillance Program (IDSP) in India and ECDC surveillance systems in the EU inform national health policies and emergency responses [24].
Preventive Medicine Across Sectors
Workplace Health Programs:
Employers play a key role in promoting preventive care. Workplace wellness initiatives such as annual health checks, ergonomic assessments, and mental health counselling help reduce absenteeism and improve employee morale and productivity.
School Health Programs:
Preventive interventions targeted at youth lay the foundation for lifelong health. These include:
Studies show that school-based interventions can reduce adolescent obesity and improve mental well-being [25].
Integration into Primary Care:
Family physicians are increasingly being trained to incorporate prevention into regular consultations. Tools like the ABCDE approach (Assess risk, Behaviour change, Clinical interventions, Diet/exercise counselling, Education) provide a structured method for preventive care delivery at the primary care level.
Future Outlook and Challenges
Preventive medicine has tremendous potential to reshape global health outcomes, but its full integration into healthcare systems remains a work in progress. Barriers include:
To overcome these, a whole-of-society approach involving healthcare providers, governments, educators, civil society, and private industry is needed. Policies must prioritize long-term public health investments over short-term curative gains.
Principles and Tools of Pharmacoeconomics:
Pharmacoeconomics is a specialized area within health economics that provides a systematic framework for analysing the value of pharmaceutical products, medical devices, and healthcare interventions. As healthcare systems worldwide contend with escalating costs, resource constraints, and growing demands, Pharmacoeconomics offers vital tools for prioritizing interventions that deliver the greatest health benefit per unit of expenditure [26].
At its core, Pharmacoeconomics seeks to maximize value for money in health care by balancing costs with outcomes such as extended survival, improved quality of life, and disease prevention. It is indispensable in guiding decisions related to drug formularies, insurance reimbursement, national health policy, and clinical practice guidelines [27].
Objectives of Pharmacoeconomic Evaluation
The primary goal is to inform healthcare decisions by comparing the cost and consequences of alternative treatments. Pharmacoeconomic studies help answer key questions such as:
This economic insight is especially important in low- and middle-income countries, where finite resources require precise allocation to maximize population health gains [28].
Key Methodologies in Pharmacoeconomics
Pharmacoeconomics employs several core analytical methods, each tailored to different decision-making contexts:
1. Cost-Minimization Analysis (CMA)
Used when two or more interventions demonstrate equivalent clinical outcomes, CMA compares their total costs and identifies the less expensive option. For example, if two antibiotics are equally effective for pneumonia, the cheaper one would be preferred [29].
2. Cost-Effectiveness Analysis (CEA)
CEA evaluates the cost per unit of health outcome, such as cost per life year gained or per case of disease prevented. This method is widely used in public health programs to assess interventions like hypertension screening or smoking cessation [30].
3. Cost-Utility Analysis (CUA)
CUA refines CEA by incorporating patient preferences and quality of life, typically using Quality-Adjusted Life Years (QALYs) or Disability-Adjusted Life Years (DALYs). Interventions are ranked based on their cost per QALY gained. This approach is heavily relied upon by health technology assessment (HTA) bodies like NICE in the UK or PBAC in Australia [31].
4. Cost-Benefit Analysis (CBA)
CBA translates both costs and outcomes into monetary values, allowing a straightforward comparison. If the monetary benefits outweigh the costs, the intervention is considered economically justified. Although less commonly used due to ethical challenges in valuing life and health, CBA is helpful in environmental health and workplace safety programs [32].
Table 3: Key Pharmacoeconomic Evaluation Methods.
|
Evaluation Method |
Description |
Outcome Measure |
Application |
|
CMA (Cost-Minimization Analysis) |
Compares costs of equally effective options |
Cost only |
Generic substitution |
|
CEA (Cost-Effectiveness Analysis) |
Compares costs per natural health unit gained |
Life-years saved, cases prevented |
Vaccine programs |
|
CUA (Cost-Utility Analysis) |
Incorporates quality of life |
QALYs or DALYs |
Chronic disease treatment |
|
CBA (Cost-Benefit Analysis) |
Monetizes both costs and outcomes |
Net monetary benefit |
Workplace wellness programs |
|
BIA (Budget Impact Analysis) |
Projects financial impact over time |
Total cost to system |
Drug reimbursement planning |
Types of Costs Considered
A comprehensive pharmacoeconomic study includes multiple types of costs:
Sensitivity and Uncertainty Analysis
Healthcare decisions often involve uncertainty regarding future events, costs, or treatment outcomes. Sensitivity analysis is used to test how results change when input variables are varied. For example, it assesses how the cost-effectiveness of a drug may change if drug prices increase or patient adherence declines.
There are several types:
These tools improve the robustness of pharmacoeconomic conclusions and inform more confident policy decisions.
Budget Impact Analysis (BIA)
While cost-effectiveness focuses on value, BIA estimates the actual financial impact of adopting a new intervention within a specific budget or payer context. BIAs answer questions such as:
BIA is critical for short-term fiscal planning, especially for public health authorities and insurance companies [35].
Applications in Health Systems and Policy
Pharmacoeconomic principles are increasingly embedded into healthcare policy and clinical decision-making:
Role of Real-World Evidence (RWE)
Traditionally, pharmacoeconomic studies relied on clinical trial data. However, randomized controlled trials (RCTs) often do not reflect real-life patient populations or health system dynamics. Real-World Evidence (RWE) derived from electronic health records, patient registries, or insurance claims enhances the relevance and applicability of pharmacoeconomic analyses.
For instance:
Global Adoption and Frameworks
The use of Pharmacoeconomics is growing globally:
These frameworks empower governments to negotiate drug prices, select essential medicines, and design benefit packages based on economic evidence rather than market forces alone.
Economic Evaluation of Preventive Strategies:
The economic evaluation of preventive strategies plays a pivotal role in shaping evidence-based health policy, ensuring that interventions not only improve population health but also deliver good value for the resources invested. As healthcare systems strive to manage rising expenditures and meet the demands of diverse populations, preventive strategies—ranging from immunizations to lifestyle interventions have emerged as cost-saving and life-enhancing options.
Unlike curative treatments that often address conditions after they have progressed, preventive strategies intervene early, thereby averting the onset or worsening of disease. This proactive approach leads to lower healthcare utilization, reduced hospital admissions, improved productivity, and better long-term health outcomes [39].
Types of Economic Evaluations in Prevention
Several types of economic analyses are commonly applied to evaluate preventive interventions:
Cost-Effectiveness Analysis (CEA)
CEA measures the cost required to achieve a specific health outcome, such as the cost per life-year saved or per case of disease prevented. Preventive strategies such as mammography screening, colorectal cancer screening, and hypertension control have consistently shown strong cost-effectiveness profiles. For instance, cervical cancer screening programs paired with HPV vaccination are not only clinically effective but also offer significant cost savings by reducing the incidence of advanced cancer [40].
Cost-Utility Analysis (CUA)
CUA incorporates quality of life into the analysis, reporting results in cost per QALY (Quality-Adjusted Life Year). Smoking cessation programs, cardiovascular risk screenings, and diabetes prevention initiatives are examples of interventions with favourable cost-utility ratios. According to a study in Health Affairs, every $1 invested in childhood immunization yields up to $44 in benefits when factoring in productivity gains and treatment cost avoidance [41].
Cost-Benefit Analysis (CBA)
CBA expresses both costs and outcomes in monetary terms, facilitating straightforward comparisons. An example is tobacco control: WHO estimates that effective tobacco control policies implemented globally from 2007 to 2017 saved more than 15 million lives and avoided billions in treatment costs [42]. Workplace productivity gains further amplify the value of such interventions.
Return on Investment (ROI)
ROI calculates the financial return generated per dollar invested. Preventive programs, especially in chronic disease management and workplace wellness, often yield high ROIs. A U.S.-based Diabetes Prevention Program showed that lifestyle changes (e.g., diet and exercise) delayed or prevented type 2 diabetes, reducing future treatment costs and generating net economic gains [43].
Real-World Applications and Case Examples
Preventive strategies are particularly impactful when implemented on a population-wide scale:
Preventive Health in Workplaces and Schools
Preventive care also extends into occupational and educational settings, where early interventions can yield large returns.
Barriers to Economic Evaluation in Prevention
Despite strong evidence, preventive strategies often face underinvestment due to several structural and policy challenges:
To address these challenges, organizations such as the World Health Organization (WHO) and the World Bank advocate integrating Health Technology Assessments (HTAs) into national planning. HTAs systematically evaluate the clinical, economic, social, and ethical impacts of preventive interventions [51].
Moving Toward Prevention-Focused Budgets
Several high-performing health systems are allocating a fixed percentage of their healthcare budgets to preventive care:
Such examples highlight the growing global consensus that prevention is not only clinically justified but also fiscally responsible.
Integration of Preventive Medicine into Health Policy:
Integrating preventive medicine into health policy represents a transformative shift from reactive, treatment-based healthcare models to proactive, wellness-oriented systems. This approach aligns health systems with the broader goals of sustainability, equity, and cost-efficiency. As the global burden of disease increasingly leans toward non-communicable diseases (NCDs) and pandemics, the imperative for robust preventive frameworks becomes more pressing than ever [53].
Policy Instruments and Legal Frameworks
Governments worldwide are leveraging legislative and regulatory tools to embed prevention in national health systems. Measures such as mandatory vaccination laws, sin taxes (on tobacco, alcohol, sugary beverages), front-of-pack food labelling, and occupational health standards directly support preventive goals. For instance, the Framework Convention on Tobacco Control (FCTC) has facilitated coordinated global efforts in reducing tobacco use, leading to improved respiratory and cardiovascular health in ratifying countries [54].
In Mexico, the implementation of a soda tax in 2014 led to a 12% decline in sugary beverage consumption in the first year, with a greater effect seen in low-income households. These types of fiscal policies not only influence consumer behaviour but also generate revenue for other public health initiatives [55].
Urban planning and transportation policy can also be designed with health promotion in mind. Examples include city master plans that prioritize green spaces, bike paths, and pedestrian-friendly zones, thereby encouraging physical activity and reducing pollution-related diseases [56].
Preventive Services in Universal Health Coverage (UHC)
Preventive care is increasingly recognized as a core component of Universal Health Coverage (UHC), which aims to provide equitable health services without causing financial hardship. Countries like Thailand, Brazil, and Rwanda have shown that integrating preventive services such as routine immunization, maternal and child care, and chronic disease screening into national health insurance schemes yields better outcomes and reduces long-term costs [57].
In Thailand, the National Health Security Office (NHSO) allocates specific budgets for prevention and health promotion within its UHC framework. This includes funding for school health programs, sexual health education, and vaccinations, demonstrating how UHC can be a vehicle for equitable access to preventive services [58].
Brazil’s Unified Health System (SUS) includes preventive outreach through Family Health Strategy (FHS) teams that visit communities to provide vaccinations, screen for hypertension, and conduct health education sessions. This model significantly reduced avoidable hospitalizations and infant mortality in underprivileged areas [59].
Primary Care as the Foundation for Prevention
A strong primary healthcare (PHC) system serves as the bedrock for the effective integration of preventive medicine. The Alma-Ata Declaration and the WHO's “Health for All” strategy underscore the centrality of PHC in delivering preventive services such as vaccinations, lifestyle counselling, and early disease detection [60].
Countries with robust PHC networks, such as Finland, Cuba, and Sri Lanka, consistently achieve better health outcomes despite limited spending. In Finland, for example, the integration of cardiovascular risk screening into primary care has contributed to a 65% reduction in coronary mortality over four decades [61].
Incorporating prevention into routine medical encounters allows for early risk identification and timely intervention. General practitioners (GPs) play a pivotal role in guiding patients toward healthy behaviours and appropriate screenings, especially for conditions like cervical cancer, hypertension, and diabetes [62].
Financial Incentives and Performance-Based Models
Reimbursement structures are also shifting to encourage preventive care delivery. Pay-for-performance (P4P) models, wherein healthcare providers are rewarded for achieving preventive health targets, have gained traction in countries like the United Kingdom, United States, and Germany.
The UK's Quality and Outcomes Framework (QOF) incentivize general practices to meet vaccination targets, manage chronic conditions proactively, and conduct regular health checks. Evaluations have shown modest improvements in preventive service delivery, although results vary by region and practice size [63].
In the U.S., Medicare’s Shared Savings Program Rewards Accountable Care Organizations (ACOs) that achieve cost savings through improved preventive care, thereby aligning clinical and financial incentives [64].
Multisectoral Collaboration and Community Involvement
Integrating prevention into health policy requires multisectoral cooperation across health, education, agriculture, housing, and transportation. For instance:
Community engagement is equally crucial. In Rwanda, community health workers (CHWs) are instrumental in delivering health education, distributing preventive materials, and monitoring at-risk populations. This model, supported by both government policy and community trust, has dramatically improved maternal and child health indicators [66].
Data, Surveillance, and Policy Adaptation
Reliable health information systems and surveillance infrastructures are essential for tailoring preventive policies to evolving needs. Countries like Singapore and South Korea leverage real-time data to track disease patterns, evaluate interventions, and adjust national strategies accordingly. Digital tools, including electronic health records, mHealth apps, and data dashboards, are enabling personalized prevention strategies and improving coordination between care providers and policymakers [67].
Evidence-informed policymaking also depends on economic evaluations. Tools such as Health Technology Assessments (HTAs) and Budget Impact Analyses (BIAs) guide decision-makers in identifying which preventive services offer the greatest value for money [68].
Challenges to Integration
Despite its benefits, integrating prevention into policy faces significant barriers:
The Way Forward
To strengthen the integration of preventive medicine into health policy, the following steps are recommended:
When effectively integrated into policy, preventive medicine has the potential to transform population health, reduce health disparities, and build financially sustainable health systems [70].
Pharmacoeconomics in Public Health Decision-Making:
Pharmacoeconomics has emerged as a central component of evidence-based public health decision-making, particularly as health systems worldwide confront rising costs, limited budgets, and increasing demands for transparency and efficiency. It provides a structured framework to evaluate not only the clinical effectiveness but also the economic value of health interventions, particularly pharmaceuticals. This analytical approach enables policymakers to prioritize healthcare investments that maximize population health while minimizing financial burdens [71].
Role in Formulary Management and Reimbursement
One of the most widespread applications of pharmacoeconomic data is in formulary decision-making. By comparing the cost-effectiveness and budget impact of medications, national and regional health authorities can determine which drugs should be included in essential medicine lists and public health insurance formularies. Agencies such as the National Institute for Health and Care Excellence (NICE) in the UK use pharmacoeconomic evaluations, specifically Quality-Adjusted Life Years (QALYs) and Incremental Cost-Effectiveness Ratios (ICERs), to make reimbursement decisions that ensure value for money [72].
The QALY allows policymakers to compare a wide range of interventions on a common scale that integrates both length and quality of life. Interventions that fall below a predetermined cost-per-QALY threshold are considered cost-effective and may be funded through public systems [73].
Application in Low- and Middle-Income Countries (LMICs)
In resource-constrained settings, pharmacoeconomic analysis helps governments prioritize limited health budgets by focusing on interventions that offer the greatest benefit at the lowest cost. The WHO Model List of Essential Medicines is a prominent example of Pharmacoeconomics in action. This list guides national procurement decisions by highlighting essential drugs that provide significant public health benefits and are cost-effective across diverse economic settings [74].
For example, antimalarial therapies, ARVs for HIV, and oral rehydration solutions have all been promoted based on favourable cost-effectiveness profiles in LMICs. These decisions have saved millions of lives while optimizing donor and public funds [75].
Informing Immunization Policy and Disease Prevention
Pharmacoeconomics plays an increasingly pivotal role in vaccine policy. Economic evaluations support decisions on vaccine introduction, schedule optimization, and target population selection. The adoption of HPV vaccines, pneumococcal conjugate vaccines (PCV), and rotavirus vaccines in national immunization programs was often backed by studies demonstrating high health impact and favourable cost-utility ratios [76].
In the United States, the Advisory Committee on Immunization Practices (ACIP) considers cost-effectiveness data in recommending new vaccines. Similarly, Gavi, the Vaccine Alliance, uses economic modelling to determine which countries qualify for vaccine subsidies, ensuring high-value vaccines reach the most vulnerable populations [77].
Role in Chronic Disease and Mental Health Management
Chronic diseases, such as hypertension, diabetes, asthma, and mental illnesses, require sustained treatment over the lifetime of the patient. Pharmacoeconomic evaluations ensure that therapies selected for these conditions are both clinically effective and financially justifiable over the long term. For instance, multiple cost-effectiveness studies have shown that antihypertensive medications significantly reduce the risk of stroke, heart failure, and mortality, resulting in positive net economic benefits even in older populations [78].
In mental health, pharmacoeconomic analyses have supported the integration of antidepressants, cognitive behavioural therapy, and community-based psychosocial interventions into public programs. These interventions, though initially costly, have been shown to reduce hospitalization, increase workforce participation, and improve long-term patient outcomes [79].
Broader Applications in Health Technology Assessment (HTA)
Beyond pharmaceuticals, Pharmacoeconomics forms a core component of Health Technology Assessment (HTA). HTA evaluates medical devices, diagnostic tests, surgical techniques, and digital health tools in terms of their safety, efficacy, cost-effectiveness, and social impact. Countries such as Canada (CADTH), Australia (PBAC), and South Korea (NECA) routinely use HTA to inform nationwide health decisions [80].
For example, pharmacoeconomic modelling has supported the adoption of telemedicine platforms, especially in rural regions, by demonstrating their cost savings related to travel, hospital admissions, and lost productivity. Similarly, point-of-care diagnostics for tuberculosis or HIV have been widely adopted in LMICs due to their favourable cost-benefit profiles [81].
Integration into Universal Health Coverage (UHC) Frameworks
Pharmacoeconomic principles have been integral to the design of health benefits packages in universal health coverage schemes. Countries such as Thailand, Mexico, and Colombia use cost-effectiveness data to decide which services to include in publicly funded insurance schemes. This ensures financial protection, health equity, and efficient allocation of resources [82].
For example, Thailand’s National Health Security Office (NHSO) uses pharmacoeconomic analysis to evaluate new interventions before inclusion in the UHC benefit package. Only services that meet both clinical and economic thresholds are added, ensuring the sustainability of the system [83].
Role in Global Health Funding and Price Negotiation
Global health donors and procurement agencies also rely on pharmacoeconomic data to inform funding decisions and price negotiations. Organizations like The Global Fund, Gavi, and Unit aid use cost-effectiveness analyses to allocate funding to the most impactful interventions and to negotiate tiered pricing with pharmaceutical companies [84].
For example, pharmacoeconomic studies enabled Gavi to secure low prices for pentavalent vaccines, resulting in expanded access for children in low-income countries. These price reductions, supported by data on disease burden and intervention impact, allow for greater health return on investment [85].
Challenges and Opportunities in Implementation
Despite its increasing importance, the implementation of Pharmacoeconomics faces several challenges:
To address these issues, international organizations such as the World Bank, ISPOR, and WHO are investing in capacity-building programs, including technical training, toolkits, and regional centres of excellence in Pharmacoeconomics [87].
Moreover, the use of real-world evidence (RWE), big data, and machine learning algorithms is improving the robustness and applicability of pharmacoeconomic models, especially in fast-evolving areas such as oncology and rare diseases [88].
Challenges in Implementing Preventive Strategies and Economic Evaluations:
Despite robust evidence supporting the value of preventive medicine and Pharmacoeconomics, the practical implementation of these approaches remains fraught with numerous obstacles. These challenges span economic, institutional, political, technical, and sociocultural domains, and they vary significantly between high-income and low- and middle-income countries (LMICs). Recognizing and addressing these barriers is essential for optimizing the health and economic benefits of prevention-centred healthcare systems [89].
Delayed Return on Investment
A key barrier to widespread adoption of preventive strategies is the delayed return on investment (ROI). Many preventive interventions, such as childhood vaccinations, chronic disease screenings, and lifestyle modification programs, require substantial upfront investments but yield benefits that manifest over years or even decades. This long-time horizon poses a challenge for governments and institutions that operate on short-term fiscal or electoral cycles, making prevention a less attractive investment despite its cost-effectiveness in the long run [90].
For instance, anti-obesity initiatives or diabetes prevention programs may reduce long-term morbidity and healthcare costs, but the immediate fiscal outlay and delayed benefits often deter adequate funding and policy attention [91].
Underfunding of Preventive Health Services
Preventive services remain underfunded globally, despite clear evidence of their effectiveness. The World Health Organization (WHO) reports that many countries allocate less than 5% of their total health budgets to prevention and public health, with the vast majority directed toward curative and hospital-based services [92]. This imbalance persists even though preventive care often yields greater cost savings per unit investment than treatment, particularly for chronic diseases and infectious disease control.
Political and public pressure to increase investment in high-profile curative services (e.g., cancer care, advanced surgeries) exacerbates the neglect of prevention. Moreover, budgeting structures that separate public health from clinical care often silo funding streams and reduce opportunities for integrated planning [93].
Limitations in Data and Economic Evaluation Capacity
Robust pharmacoeconomic evaluations require reliable, comprehensive data on costs, health outcomes, disease burden, and resource use. Unfortunately, many LMICs lack the health information infrastructure and trained personnel to generate such data. This deficiency undermines the ability to conduct local economic evaluations or adapt global models to country-specific contexts [94].
Additionally, there is a shortage of trained health economists, particularly in the public sector. Without local expertise in economic modelling and cost-effectiveness analysis, governments may rely heavily on foreign consultants or generic models that fail to capture local healthcare realities [95].
Health Inequities and Access Gaps
Preventive services often fail to reach marginalized and underserved populations, exacerbating health disparities. Structural barriers including geographic isolation, poverty, low health literacy, and cultural stigma limit access to screenings, immunizations, and health promotion services [96].
For example, rural communities may lack transportation or healthcare facilities, while urban slums may face infrastructural deficiencies. In many cases, preventive strategies are designed with a “one-size-fits-all” approach, which does not account for diverse population needs, resulting in inequitable outcomes [97].
Ensuring equity in preventive care requires targeted outreach, community involvement, and culturally sensitive service delivery models.
Resistance to Systemic Change
Another significant barrier is the resistance to change from within the healthcare system itself. Providers often receive incentives for curative services, such as fee-for-service payments, rather than for delivering preventive care. Additionally, medical training curricula have traditionally emphasized diagnosis and treatment over prevention and public health, leading to a skills and mindset gap among clinicians [98].
Institutions entrenched in reactive, treatment-focused care are slow to adopt proactive strategies. Without structural reforms such as outcome-based reimbursement, continuing education in preventive medicine, and integration of public health principles into practice prevention will remain secondary to treatment [99].
Ethical and Political Considerations
Pharmacoeconomic evaluations, while grounded in data, sometimes generate ethical dilemmas. Assigning monetary value to human life or comparing interventions purely based on cost-effectiveness can provoke public and political resistance. For example, denying access to a costly cancer drug due to low cost-effectiveness ratios may be interpreted as prioritizing economics over compassion [100].
Moreover, preventive strategies involving behavioural change (e.g., smoking bans, sugar taxes) often face opposition on grounds of individual liberty, cultural norms, or industry lobbying. Politicians may avoid supporting such measures for fear of alienating voters or stakeholders, even when supported by economic evidence [101].
Commercial Influence and Misaligned Incentives
The pharmaceutical industry’s influence on healthcare priorities can create tensions between commercial interests and public health goals. High-revenue treatments often receive more advocacy, research funding, and promotional efforts compared to low-cost preventive interventions. As a result, pharmaceutical innovation is disproportionately focused on curative rather than preventive therapies [102].
In some cases, industry lobbying can skew national formularies or insurance coverage decisions toward expensive medications with marginal benefits. This undermines efforts to implement cost-effective, preventive measures grounded in pharmacoeconomic evaluations [103].
Contextual Misalignment of Economic Models
Many pharmacoeconomic models are developed in high-income countries with different cost structures, healthcare systems, and population health profiles compared to LMICs. Applying these models directly to LMIC contexts can lead to misleading conclusions, poor policy choices, and wasted resources [104].
Factors such as labour costs, availability of infrastructure, disease prevalence, and cultural preferences must be incorporated into local pharmacoeconomic assessments. This requires context-specific data, stakeholder involvement, and sensitivity analyses to adapt global models appropriately [105].
Strategies to Overcome Implementation Barriers
To overcome these challenges, a multi-pronged strategy is essential:
Future Directions and Global Implications:
The future of sustainable healthcare systems depends heavily on advancing preventive medicine and integrating pharmacoeconomic principles at every level of health planning and implementation. As countries face increasing burdens of chronic diseases, aging populations, and economic constraints, a strategic shift from treatment to prevention becomes not just a choice but a necessity [107].
One of the most important future directions is the adoption of digital health technologies. Mobile health (mHealth), telemedicine, wearable devices, and electronic health records (EHRs) offer powerful platforms for delivering preventive care, monitoring health behaviours, and conducting real-time pharmacoeconomic assessments. For example, AI-driven predictive analytics can identify at-risk individuals and allow for timely interventions, reducing hospitalizations and treatment costs [108].
Personalized medicine and genomics are also expected to revolutionize prevention by enabling more precise risk stratification and targeted preventive strategies. Pharmacogenomics can help tailor drug therapies that prevent adverse events and improve cost-effectiveness. Soon, integrating genomic screening into preventive health packages may become routine, especially in high-income countries [109].
Another major trend is the global harmonization of health technology assessment (HTA) processes. By sharing data, methodologies, and best practices, countries can streamline evaluation and avoid duplication of work. This would enhance decision-making efficiency and ensure consistency in resource allocation globally. Organizations like the International Network of Agencies for HTA (INAHTA) and the Global Health Technology Assessment Network (GHTAN) are leading this effort [110].
Table 4 : Examples of Countries Implementing Preventive Strategies with Pharmacoeconomic Support.
|
Country |
Program/Agency |
Focus Area |
Key Outcome |
Reference |
|
Thailand |
HITAP/UCS |
HPV screening, cost-effectiveness |
Improved screening cost-efficiency |
[103] |
|
UK |
NICE |
HTA, QALY-based decisions |
Rational and equitable resource use |
[104] |
|
Brazil |
FHS + Bolsa Família |
Community-based primary care |
Reduced infant mortality, equity gains |
[105] |
|
Rwanda |
CHWs + Insurance |
Immunization, maternal health |
$21 return per $1 spent |
[106] |
|
Canada |
Cost-utility evaluations |
Zoster vaccine, chronic disease |
Lower hospitalizations, better outcomes |
[107] |
|
India |
Ayushman Bharat + HWCs |
NCD prevention, screenings |
Early disease detection |
[108] |
|
South Korea |
NHIS Screening |
Biennial checkups |
Decline in NCD-related mortality |
[109] |
|
Vietnam |
WHO PEN |
Cost-effective NCD management |
Reduced premature CVD mortality |
[110] |
Investment in preventive infrastructure including community health workers, vaccination centres, and early screening facilities is projected to grow. Countries are realizing the need for long-term funding models, including public-private partnerships, sin taxes, and insurance schemes dedicated to prevention. Innovative financing mechanisms such as social impact bonds and results-based financing are being explored to scale up preventive interventions [111].
In low- and middle-income countries, expanding universal health coverage (UHC) to include preventive services is crucial. International organizations such as WHO, Gavi, and the World Bank are working with governments to integrate cost-effective prevention into health benefit packages. A growing body of evidence suggests that even minimal investments in preventive services can yield significant economic and health returns in these regions [112].
On a global scale, climate change and urbanization are emerging as key drivers influencing health systems. Environmental hazards, air pollution, and unhealthy urban lifestyles are contributing to the growing burden of NCDs. Future preventive strategies must adopt a “Health in All Policies” (HiAP) approach that links public health with urban planning, environmental protection, and transportation policies [113].
Equity-focused prevention will also be central to sustainable health. Targeting social determinants of health such as education, housing, nutrition, and employment through cross-sector collaborations will be key to reducing disparities and achieving inclusive healthcare outcomes. Programs like Brazil’s Bolsa Família and India’s Ayushman Bharat demonstrate the value of integrating health with social welfare strategies [114].
Academic institutions and think tanks will play a pivotal role in training the next generation of health economists, public health leaders, and data scientists. Interdisciplinary education that merges clinical knowledge with economics, ethics, and technology will prepare future professionals to design and implement prevention-oriented health systems [115].
Finally, global political commitment is essential. High-level advocacy, such as the United Nations Sustainable Development Goals (especially SDG 3: Good Health and Well-being), provides a framework for collaborative action. Countries must align national policies with global commitments and ensure accountability in implementing preventive and economic health reforms [116].
In summary, the integration of preventive medicine and Pharmacoeconomics into health systems is not merely an option it is an imperative for long-term health security and fiscal sustainability. With coordinated efforts, innovative solutions, and equitable policies, the global community can transform health systems to be proactive, efficient, and resilient in the face of future challenges [117].
Case Studies and Real-World Applications:
Case studies across the globe offer compelling evidence of the effectiveness of preventive medicine and Pharmacoeconomics in action. These real-world applications help demonstrate how strategic health interventions can lead to substantial cost savings, improved health outcomes, and more resilient health systems.
Thailand’s Universal Coverage Scheme (UCS) is a widely recognized example of how Pharmacoeconomics informs national health decisions. The Health Intervention and Technology Assessment Program (HITAP) has integrated cost-effectiveness analyses into the country’s decision-making process, resulting in the adoption of essential and affordable health interventions. Through this system, Thailand introduced cervical cancer screening using HPV DNA testing, demonstrating that it was more cost-effective and lifesaving than older methods [118].
In the United Kingdom, the National Institute for Health, and Care Excellence (NICE) has applied pharmacoeconomic principles for decades. NICE recommendations determine which technologies and drugs are available under the National Health Service (NHS), ensuring that only interventions offering sufficient value per QALY (Quality-Adjusted Life Year) are funded. This has made the UK’s healthcare system one of the most economically rational and equitable in the world [119].
Rwanda’s health system reform serves as a model for low-income countries. Despite limited resources, Rwanda dramatically improved vaccination coverage, maternal health, and access to essential services through community health workers and results-based financing. A study showed that every dollar spent on immunization generated $21 in economic returns, highlighting the power of preventive investment [120].
Brazil’s Family Health Strategy (FHS), integrated with the Bolsa Família program, significantly reduced hospitalizations due to conditions sensitive to primary care. By deploying multidisciplinary teams to underserved communities and linking social support with health services, Brazil created a model where preventive health and social welfare intersect [121].
In Canada, cost-utility analyses are used to assess vaccination programs and preventive medications for chronic diseases. For instance, introducing the zoster vaccine for older adults was shown to be cost-effective in reducing the burden of herpes zoster and post-herpetic neuralgia, resulting in fewer hospital visits and better quality of life [122].
India’s Ayushman Bharat program, launched in 2018, aims to strengthen primary health care through Health and Wellness Centres (HWCs) and provide financial protection via the Pradhan Mantri Jan Arogya Yojana (PM-JAY). HWCs deliver a broad range of preventive and promotive services, including screenings for hypertension, diabetes, and certain cancers. Studies have already shown early detection leading to reduced costs and better outcomes [123].
The U.S. Affordable Care Act (ACA) also mandated coverage of preventive services without cost-sharing. This led to increased uptake of screenings, vaccines, and wellness visits. The Centres for Medicare & Medicaid Services (CMS) estimated that such provisions could save billions over the long term by reducing emergency care and hospitalizations [124].
Vietnam’s public health strategy, emphasizing early detection and cost-effective treatment of NCDs, has shown strong results. Supported by international donors and guided by WHO’s Package of Essential Noncommunicable (PEN) Disease Interventions, the country reduced premature deaths from cardiovascular diseases while maintaining a low-cost, scalable model [125].
In South Korea, the National Health Insurance Service (NHIS) implements a mandatory biennial health check-up program. These check-ups, combined with health counselling and lifestyle modification support, have been credited with lowering national rates of obesity and diabetes-related complications, making South Korea one of the few high-income nations to effectively curb NCD growth [126].
These diverse examples underscore the versatility and necessity of preventive medicine and Pharmacoeconomics. From high-income nations to low-resource settings, applying these disciplines improves cost-efficiency, promotes equitable access, and creates systems resilient to future health crises.
Policy Recommendations and Actionable Insights:
Translating the principles of preventive medicine and Pharmacoeconomics into concrete policy requires actionable, scalable, and evidence-informed strategies. The following recommendations aim to guide governments, public health authorities, and global institutions in shaping more resilient and economically sustainable healthcare systems.
1. Increase Investment in Preventive Health Services
Governments should earmark a larger portion of healthcare budgets specifically for prevention. This includes funding vaccination programs, screening services, nutrition initiatives, mental health outreach, and health education. Evidence suggests that even modest increases in preventive health funding can yield large economic returns by reducing disease burden and treatment costs [127].
2. Institutionalize Pharmacoeconomic Evaluation in Policy-Making
Health Technology Assessment (HTA) bodies should be established or strengthened to ensure that cost-effectiveness analyses guide decisions about which interventions are funded. Policymakers should require pharmacoeconomic justifications for the inclusion of treatments, drugs, and technologies into national health benefit packages [128].
3. Integrate Preventive Care into Universal Health Coverage (UHC)
Preventive services should be embedded within primary healthcare and guaranteed as part of national UHC schemes. Early diagnosis and risk mitigation must be treated as essential services to ensure that financial protection extends to long-term health maintenance and disease prevention [129].
4. Incentivize Providers for Delivering Preventive Care
Payment models must evolve to reward outcomes rather than volume. Value-based healthcare systems can offer financial incentives to providers for preventive activities such as immunization coverage, screening participation, and chronic disease management, aligning clinician behaviour with public health goals [130].
5. Develop National and Subnational Data Systems
High-quality health and economic data are essential to monitor the impact of preventive measures and evaluate their cost-effectiveness. Governments should invest in interoperable electronic health records, national health surveys, and cost databases to support evidence-based planning [140].
6. Build Capacity in Health Economics and Public Health
Countries should establish academic programs, fellowships, and technical training in Pharmacoeconomics and preventive medicine. Strengthening local expertise ensures that interventions are context-specific and sustainable in the long run [141].
7. Promote Multisectoral Collaboration
Health outcomes are shaped by non-health sectors such as education, environment, agriculture, and finance. A “Health in All Policies” approach should be adopted where health impact assessments become a standard part of cross-sector decision-making [142].
8. Encourage International Partnerships and Knowledge Sharing
Global agencies such as WHO, the World Bank, and Gavi should support country-led efforts through technical guidance, financial assistance, and the dissemination of best practices. Regional collaborations can facilitate capacity building and promote policy convergence on prevention and Pharmacoeconomics [143].
9. Ensure Equity in Prevention Efforts
Targeted programs should address the needs of marginalized populations including rural communities, informal workers, and ethnic minorities to avoid widening health disparities. Social determinants must be incorporated into both health strategy and economic evaluation frameworks [144].
10. Institutionalize Monitoring, Evaluation, and Accountability
Performance indicators should be tied to the uptake and effectiveness of preventive services, and pharmacoeconomic evaluation should be embedded into routine policy review. Transparent reporting fosters trust and promotes accountability across all stakeholders [145].
Preventive medicine and Pharmacoeconomics are not theoretical constructs they are pragmatic tools that can guide countries toward achieving the Sustainable Development Goals (SDGs), particularly Goal 3 on health and well-being. Policymakers must act decisively, using these tools to create health systems that are proactive, patient-centred, and financially viable.
CONCLUSION:
As global healthcare systems contend with the dual challenges of rising non-communicable diseases and constrained economic resources, the integration of preventive medicine and Pharmacoeconomics emerges as an essential strategy for achieving long-term sustainability. Preventive medicine emphasizes proactive health promotion, early detection, and risk reduction, thereby reducing disease incidence and severity. Pharmacoeconomics, on the other hand, ensures that healthcare investments yield maximum value by identifying cost-effective interventions and guiding equitable resource allocation.
Together, these disciplines offer a transformative approach to healthcare shifting the focus from reactive, high-cost treatment to proactive, value-based care. Case studies from diverse global contexts including Thailand, the UK, Rwanda, and India demonstrate that investing in preventive strategies not only improves population health outcomes but also delivers significant economic returns. These real-world successes underline the practicality and efficacy of aligning preventive care with economic evaluation.
However, widespread implementation faces numerous challenges, including delayed return on investment, political inertia, data limitations, and health inequities. Overcoming these barriers requires strong political will, multisectoral collaboration, capacity-building in health economics, and a commitment to equity and inclusivity in health service delivery.
Looking forward, innovations in digital health, personalized medicine, and global health technology assessment offer promising avenues for enhancing the reach and impact of preventive Pharmacoeconomics. By embedding prevention and economic evaluation into health policies, funding mechanisms, and clinical practice, nations can build resilient healthcare systems capable of withstanding future health and financial crises.
In conclusion, the convergence of preventive medicine and Pharmacoeconomics represents a paradigm shift necessary for global health sustainability. It is not merely an academic ideal it is a practical, evidence-based imperative to ensure healthier populations, smarter spending, and stronger health systems for generations to come.
REFERENCES




Galla Naga Deepika, Bandi Aasritha, Dasari Cherishma Sri, Dr. Adusumalli Surendra, Preventive Medicine and Pharmacoeconomics: Shaping Sustainable Healthcare Systems Worldwide, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 947-981. https://doi.org/10.5281/zenodo.17078136
 10.5281/zenodo.17078136
10.5281/zenodo.17078136