1Shri Ram Murti Smarak, College of Engineering and Technology (Pharmacy), Bareilly, 243407, India.
2Anjali College of Pharmacy and Science, Agra, 283202, India.
3Sainik Pharmacy College, Hanumanganj, Prayagraj,221505, India.
Quercetin, a flavanol abundant in fruits and vegetables, exhibits potent antioxidant, anti-inflammatory, immunomodulatory, and neuroprotective properties, making it a promising therapeutic candidate for chronic diseases characterized by oxidative stress and inflammation. This review evaluates quercetin’s therapeutic potential in asthma, hypertension, allergic rhinitis, and neurodegenerative disorders, which share common pathological mechanisms. An in-depth analysis of preclinical and clinical studies highlights its ability to scavenge free radicals, modulate cytokine release, stabilize mast cells, improve endothelial function, and protect neuronal integrity. In asthma and allergic rhinitis, quercetin reduces eosinophilic inflammation, Th2 cytokines, and histamine release. In hypertensive models and clinical trials, it improves vascular function and lowers blood pressure. In neurodegenerative diseases, it mitigates oxidative neuronal injury and amyloid toxicity. However, its clinical applicability is limited by poor bioavailability and a lack of robust human trials. Advancements in formulation strategies and further clinical validation are essential to harness quercetin’s therapeutic potential fully.
Quercetin is a naturally occurring polyphenolic flavonol, classified within the broader group of flavonoids—plant-derived secondary metabolites involved in pigmentation and defense mechanisms. It is ubiquitously present in a wide range of edible plant sources, including fruits, vegetables, seeds, grains, and beverages such as green tea and red wine[1–3]. Among these, onions, apples, grapes, capers, kale, broccoli, and various berries are particularly rich in quercetin, making it one of the most frequently consumed flavonoids in the human diet[4,5]. Structurally, quercetin is a flavonol characterized by the typical C6–C3–C6 backbone, comprising two aromatic rings (A and B) linked via a heterocyclic pyrone ring (C). The molecule features five hydroxyl groups at positions 3, 5, 7, 3′, and 4′, which are primarily responsible for its potent antioxidant activity. These hydroxyl moieties enable quercetin to effectively scavenge reactive oxygen species (ROS), chelate transition metal ions, and inhibit lipid peroxidation [6–8]. Notably, the catechol group on the B-ring plays a pivotal role in neutralizing free radicals, contributing significantly to its redox-modulating capacity. Quercetin, in its aglycone form, is a lipophilic compound with poor aqueous solubility, which substantially limits its oral bioavailability. Its absorption in the gastrointestinal tract is minimal, and it undergoes extensive first-pass metabolism through glucuronidation, sulfation, and methylation in both the intestinal epithelium and liver [9–11].
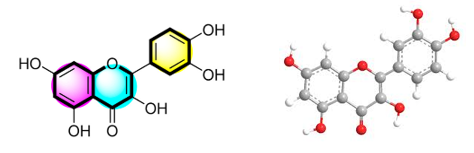
Figure 1: Chemical structure and 3D conformer of quercetin.
In nature, quercetin predominantly exists in glycosylated forms—such as quercetin-3-O-glucoside, quercetin-3-O-galactoside, and quercetin-3-O-rutinoside (rutin)—which exhibit distinct absorption kinetics and metabolic stability. These glycosides are subject to differential hydrolysis by intestinal enzymes and gut microbiota, influencing their systemic bioactivity [10–12]. Pharmacologically, quercetin exhibits a broad spectrum of biological activities, including antioxidant, anti-inflammatory, antiviral, antimicrobial, anti-allergic, cardioprotective, neuroprotective, and anticancer effects [13–15]. Its antioxidant efficacy stems not only from direct free radical scavenging but also from the upregulation of endogenous antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) [16].
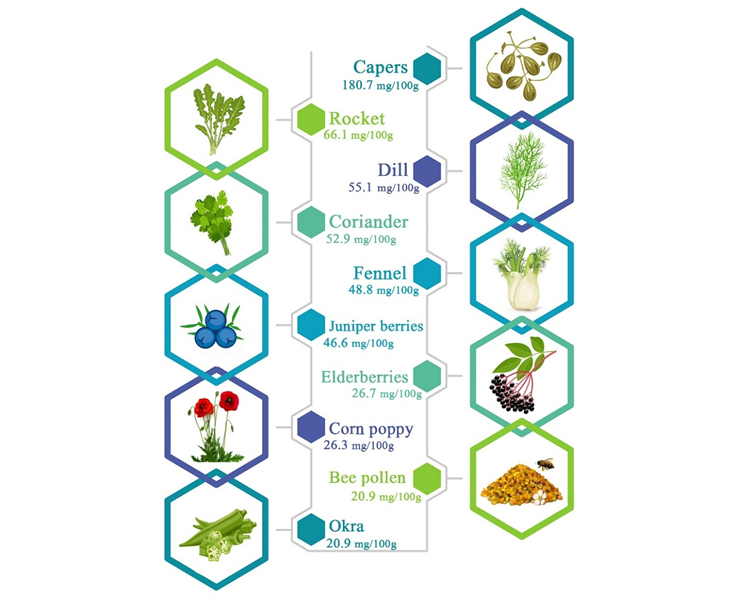
Figure 2. The main sources of quercetin
Moreover, quercetin modulates several key signalling pathways—namely NF-κB, MAPKs, PI3K/Akt, and Nrf2—that are central to inflammation, apoptosis, and cellular stress responses [17–19]. Given its pleiotropic pharmacological profile and dietary abundance, quercetin has been extensively investigated for its therapeutic potential in managing chronic conditions such as cardiovascular diseases, metabolic syndrome, allergic disorders, respiratory ailments, and neurodegenerative diseases. However, its clinical utility remains constrained by poor bioavailability, prompting the development of advanced delivery systems, including nanoparticles, liposomes, and phytosome-based formulations, to enhance its pharmacokinetic and therapeutic performance [20–22]. Quercetin exerts its pharmacological effects primarily through free radical scavenging, modulation of intracellular signalling pathways, and regulation of gene expression. As a potent antioxidant, it neutralizes reactive oxygen species (ROS), inhibits lipid peroxidation, and protects cellular macromolecules from oxidative damage. Additionally, quercetin chelates redox-active transition metals such as iron and copper, thereby limiting metal-catalyzed ROS generation [21]. Its anti-inflammatory activity is mediated by the suppression of pro-inflammatory cytokines, including TNF-α, IL-1β, and IL-6. Quercetin also inhibits key transcription factors such as nuclear factor-kappa B (NF-κB) and activator protein-1 (AP-1) [22–24]. These are central to the expression of inflammatory genes. Furthermore, it downregulates the expression of inflammatory enzymes like cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS), contributing to its molecular anti-inflammatory profile. [25–27].
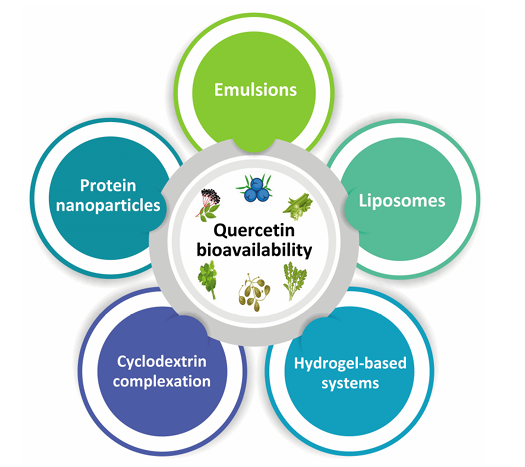
Figure 3. Recent strategies on the enhancement of quercetin bioavailability.
In allergic conditions, quercetin acts as a mast cell stabilizer, effectively preventing degranulation and the subsequent release of histamine, prostaglandins, and leukotrienes [28–30]. This action mitigates the acute phase of allergic responses and reduces tissue inflammation. Beyond mast cell stabilization, quercetin exhibits immuomodulatory properties by shifting the Th1/Th2 balance toward a Th1-dominant response and enhancing the production of interferon-γ (IFN-γ) [31–32], thereby promoting a more regulated immune profile. Furthermore, quercetin influences multiple intracellular signaling pathways, including PI3K/Akt, MAPK, and Nrf2, which are integral to cellular stress responses, inflammation, and redox homeostasis [33–35].
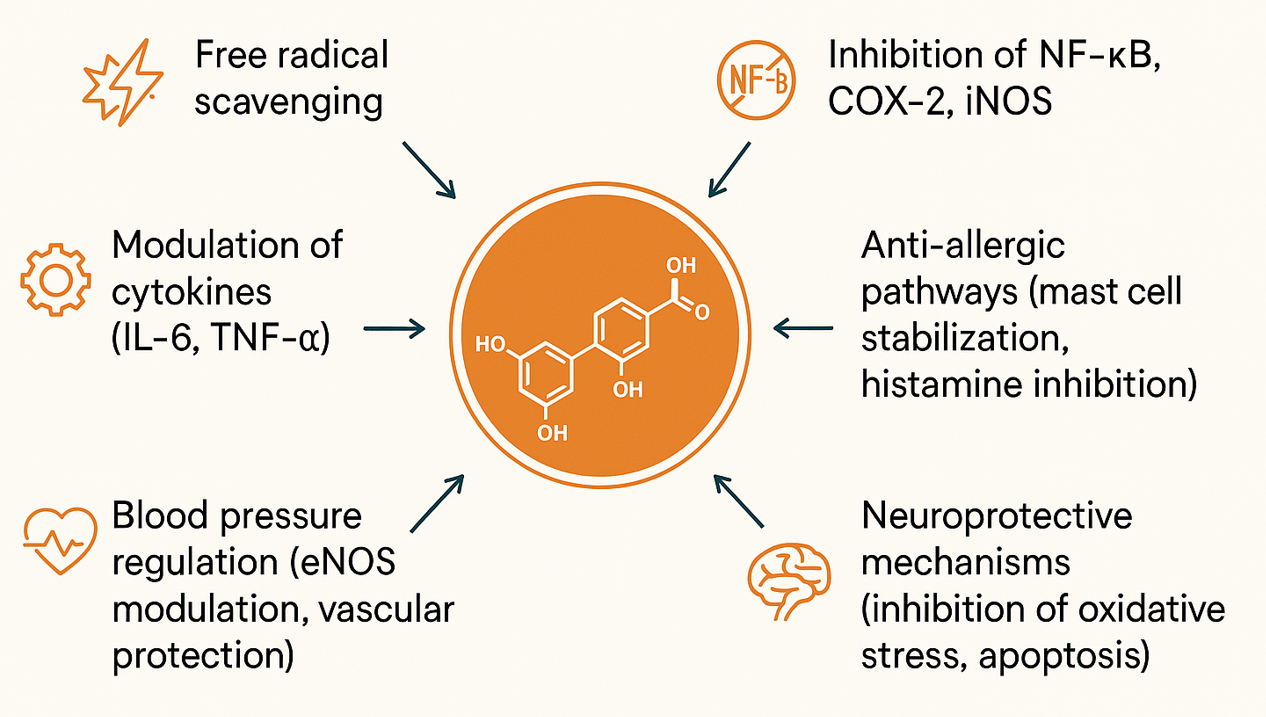
Figure 4. Diagram illustrating quercetin’s multifunctional therapeutic roles—antioxidant, anti-inflammatory, antihypertensive, antiallergic, and neuroprotective—via cytokine modulation, NF-κB/COX-2 inhibition, eNOS activation, and mast cell stabilization.
The rationale for selecting asthma, hypertension, allergic rhinitis, and neurodegenerative disorders as focal points in this review lies in their high global prevalence, escalating healthcare burden, and convergence of underlying pathophysiological mechanisms. Despite their clinical heterogeneity, these conditions share common molecular hallmarks, including oxidative stress, chronic inflammation, and immune dysregulation [37–39]. Central to their pathogenesis is the persistent activation of signaling pathways such as NF-κB, MAPKs, and pro-inflammatory cytokine networks—all of which are known targets of quercetin’s modulatory activity. Therefore, investigating quercetin’s therapeutic potential across this disease spectrum offers a coherent and mechanistically grounded framework for evaluating its role as a broad-spectrum bioactive agent. Asthma is a chronic inflammatory airway disorder characterized by airway hyperresponsiveness, mucus overproduction, and infiltration of eosinophils and mast cells, leading to bronchial obstruction and episodic exacerbations. Quercetin has demonstrated efficacy in preclinical models by suppressing Th2-mediated immune responses, downregulating cytokines such as IL-4, IL-5, and IL-13, and reducing eosinophilic infiltration in airway tissues. Additionally, its ability to stabilize mast cells, reinforce epithelial barrier integrity, and attenuate oxidative stress in bronchial smooth muscle highlights its potential as an adjunctive therapeutic agent in asthma management [40,41]. Hypertension, a major risk factor for cardiovascular disease, is closely associated with endothelial dysfunction, diminished nitric oxide (NO) bioavailability, and vascular oxidative stress. Quercetin exerts vasoprotective effects by enhancing endothelial nitric oxide synthase (eNOS) activity, inhibiting NADPH oxidase-mediated ROS generation, and restoring vascular redox balance [42–44]. Both preclinical and clinical studies have reported modest yet significant reductions in systolic and diastolic blood pressure following quercetin supplementation, particularly in hypertensive individuals, supporting its role as a natural antihypertensive compound. Allergic rhinitis is an IgE-mediated inflammatory condition of the nasal mucosa, clinically manifested by nasal congestion, sneezing, rhinorrhea, and pruritus. It is primarily driven by allergen-induced mast cell degranulation, which triggers the release of histamine, prostaglandins, leukotrienes, and pro-inflammatory interleukins. Quercetin exerts therapeutic potential in allergic rhinitis through its mast cell-stabilizing activity, achieved by inhibiting intracellular calcium influx and downregulating histidine decarboxylase expression—thereby reducing histamine synthesis and release [45–47]. Moreover, quercetin modulates the Th2-skewed immune response by attenuating cytokines such as IL-4, IL-5, and IL-13, and alleviates mucosal edema, collectively contributing to symptomatic relief and improved nasal airflow. Neurodegenerative disorders such as Alzheimer’s disease (AD) and Parkinson’s disease (PD) are characterized by progressive neuronal degeneration, accumulation of misfolded protein aggregates, mitochondrial dysfunction, and chronic neuroinflammation. Central to their pathogenesis is oxidative stress, which induces DNA fragmentation, protein oxidation, and lipid peroxidation within neuronal membranes. Quercetin exhibits significant neuroprotective potential by scavenging reactive oxygen species (ROS), attenuating microglial activation, and inhibiting the aggregation of β-amyloid peptides. Additionally, it modulates apoptotic signalling pathways, thereby preserving neuronal viability [48,49]. Notably, quercetin can cross the blood–brain barrier (BBB) and interact with key neuroenzymes such as acetylcholinesterase and monoamine oxidase, further supporting its therapeutic relevance in the management of neurodegenerative conditions. Collectively, these four conditions—namely, asthma, hypertension, allergic rhinitis, and neurodegenerative disorders—serve as a representative framework for assessing the multifaceted therapeutic potential of quercetin. Common pathological mechanisms, including chronic inflammation, oxidative stress, and immune dysregulation, underpin each. Quercetin’s ability to modulate these interconnected pathways underscores its promise as a broad-spectrum bioactive agent with relevance across diverse chronic disease states. The present review aims to critically evaluate quercetin's therapeutic potential in managing asthma, hypertension, allergic rhinitis, and neurodegenerative disorders—diseases that, despite their clinical differences, share underlying mechanisms such as oxidative stress, inflammation, and immune dysregulation. Quercetin, a bioactive flavonoid found abundantly in fruits and vegetables, exhibits a broad spectrum of pharmacological activities, including antioxidant, anti-inflammatory, and immunomodulatory effects, making it a promising candidate for targeting these conditions. This review synthesizes current preclinical and clinical evidence on quercetin, emphasizing its molecular mechanisms, pharmacodynamic actions, and therapeutic potential across diverse pathological conditions. Special focus is placed on its limited oral bioavailability and the emergence of advanced nanoformulation strategies—such as nanoparticles, liposomes, and phytosomes—that aim to enhance systemic absorption and pharmacokinetic performance. The review also delineates quercetin’s chemical structure, dietary sources, and biological activities, highlighting its regulatory effects on cytokine expression, mast cell stabilization, and endothelial function. Furthermore, the potential of combination therapies and condition-specific dosing regimens is explored. Looking ahead, future research should prioritize well-designed clinical trials, precision-targeted delivery systems, and pharmacokinetic optimization to facilitate the clinical translation of quercetin’s pleiotropic benefits into effective therapeutic interventions.
Quercetin mediates its therapeutic effects through a constellation of interconnected biological pathways. As a potent antioxidant, it neutralizes free radicals and reactive oxygen species (ROS), thereby attenuating oxidative stress and preventing lipid peroxidation and cellular injury [50]. It also modulates key inflammatory signaling cascades by inhibiting nuclear factor-kappa B (NF-κB), cyclooxygenase-2 (COX-2), and inducible nitric oxide synthase (iNOS), resulting in the downregulation of pro-inflammatory mediators [51]. In the context of immune regulation, quercetin suppresses cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), contributing to its immunomodulatory profile [52]. In allergic conditions, quercetin stabilizes mast cells and inhibits the release of histamine and other allergic mediators, thereby exerting anti-allergic effects [53]. Cardiovascular benefits are mediated through the activation of endothelial nitric oxide synthase (eNOS), enhancement of nitric oxide (NO) bioavailability, and preservation of vascular integrity—mechanisms that support blood pressure regulation [54,55]. Within the nervous system, quercetin confers neuroprotection by mitigating oxidative neuronal damage, inhibiting apoptotic pathways, and suppressing neuroinflammation, underscoring its relevance in neurodegenerative disease management [56,57].
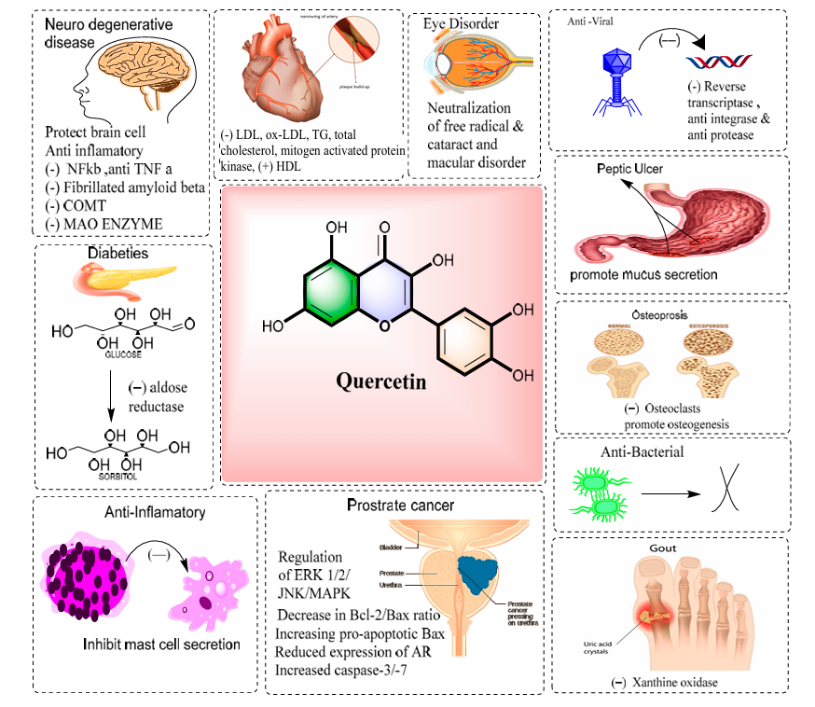
Figure 5. A schematic diagram represents the pharmacological efficacy of quercetin
2. Quercetin in Asthma
Quercetin exhibits considerable promise in attenuating the pathophysiological hallmarks of asthma, particularly by mitigating airway inflammation and immune hypersensitivity [58]. Its anti-asthmatic effects are largely attributed to the suppression of eosinophilic infiltration and downregulation of T-helper 2 (Th2) cytokines, including interleukin (IL)-4, IL-5, and IL-13, key drivers of allergic airway inflammation [59,60]. By stabilizing mast cells and inhibiting histamine release, quercetin further alleviates bronchoconstriction and mucus hypersecretion [61]. Preclinical studies using ovalbumin-induced asthma models have demonstrated that quercetin significantly reduces airway hyperresponsiveness, inflammatory cell infiltration in bronchoalveolar lavage fluid, and Th2 cytokine expression [62,63]. Additionally, it restores the activity of endogenous antioxidant enzymes, thereby reducing oxidative stress in pulmonary tissues [64]. Preliminary clinical findings suggest that quercetin supplementation may provide symptomatic relief in patients with allergic asthma phenotypes. Notably, quercetin has shown synergistic potential when combined with corticosteroids or leukotriene receptor antagonists, enhancing anti-inflammatory efficacy while potentially lowering required dosages and minimizing adverse effects.[66]
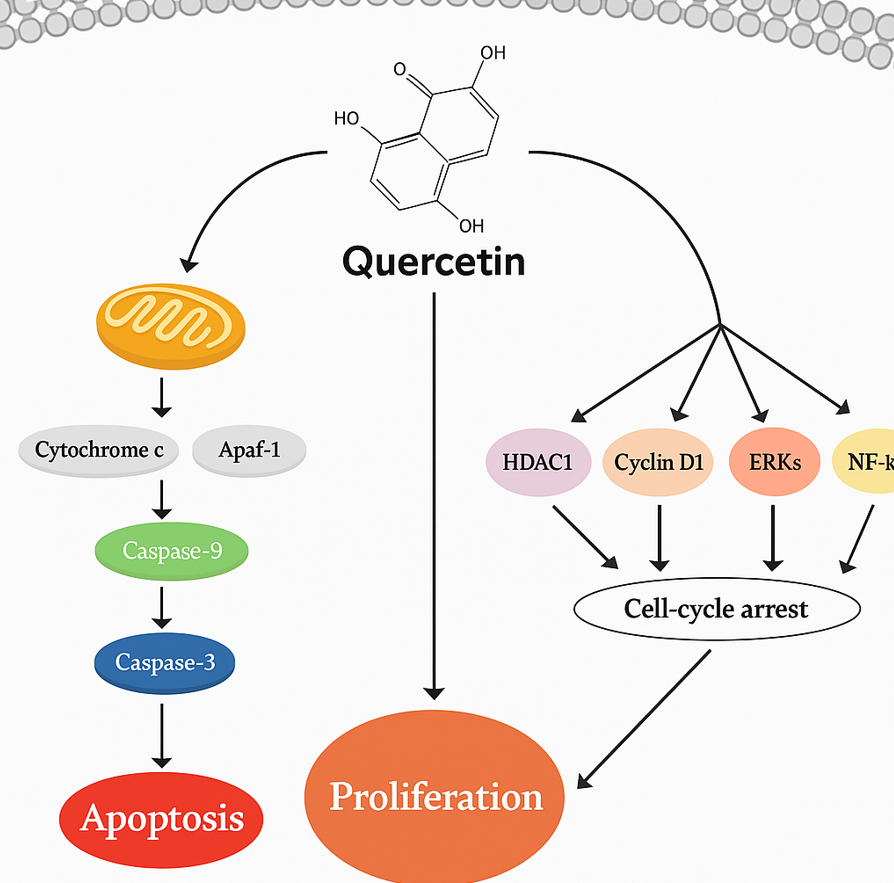
Figure 6: Quercetin-Mediated Modulation of Mitochondrial and Cell-Cycle Pathways
3. Quercetin in Hypertension
Quercetin demonstrates significant antihypertensive potential, primarily through its ability to enhance endothelial function and modulate vascular tone. It upregulates endothelial nitric oxide synthase (eNOS) activity, thereby increasing nitric oxide (NO) production, which promotes vasodilation and reduces peripheral vascular resistance [67]. Additionally, quercetin modulates the renin–angiotensin–aldosterone system (RAAS) by inhibiting angiotensin-converting enzyme (ACE), leading to decreased angiotensin II levels and reduced vasoconstriction and sodium retention [68]. These mechanisms collectively contribute to lowering systemic blood pressure. Clinical studies have reported that quercetin supplementation—particularly at doses ≥500 mg/day—can significantly reduce both systolic and diastolic blood pressure, especially in individuals with stage 1 hypertension [69,70] Mechanistically, quercetin also attenuates vascular oxidative stress by inhibiting NADPH oxidase activity and enhancing endogenous antioxidant defences, thereby preserving endothelial integrity [71]. Furthermore, it improves vascular reactivity by restoring smooth muscle relaxation and mitigating arterial wall inflammation [72]. Taken together, these multifaceted actions position quercetin as a promising adjunctive therapeutic agent for hypertension, offering both vascular protection and blood pressure regulation [73].
cetin in Allergic Rhinitis
Quercetin has demonstrated notable efficacy in the management of allergic rhinitis by targeting key immunological and inflammatory pathways involved in the allergic cascade. One of its primary mechanisms is mast cell stabilization, which prevents degranulation and the subsequent release of histamine, prostaglandins, and leukotrienes [74]. This is achieved through the inhibition of intracellular calcium influx and downregulation of histidine decarboxylase, resulting in reduced histamine synthesis and alleviation of hallmark symptoms such as sneezing, nasal congestion, and rhinorrhea [75]. Preclinical studies in animal models have shown that quercetin significantly reduces eosinophilic infiltration, mucosal edema, and Th2 cytokine expression (e.g., IL-4, IL-5, IL-13) in nasal tissues [76]. Human trials, though limited, have reported symptomatic improvement with both oral and intranasal quercetin formulations, often with a favorable safety profile compared to conventional antihistamines [77]. Notably, quercetin has demonstrated comparable efficacy to agents like cetirizine and loratadine, while offering additional anti-inflammatory and antioxidant benefits [78]. Its dual-phase action—targeting both the early (mast cell-mediated) and late (cytokine-driven) phases of the allergic response—positions quercetin as a promising natural alternative or adjunct to standard pharmacotherapy in allergic rhinitis [79].
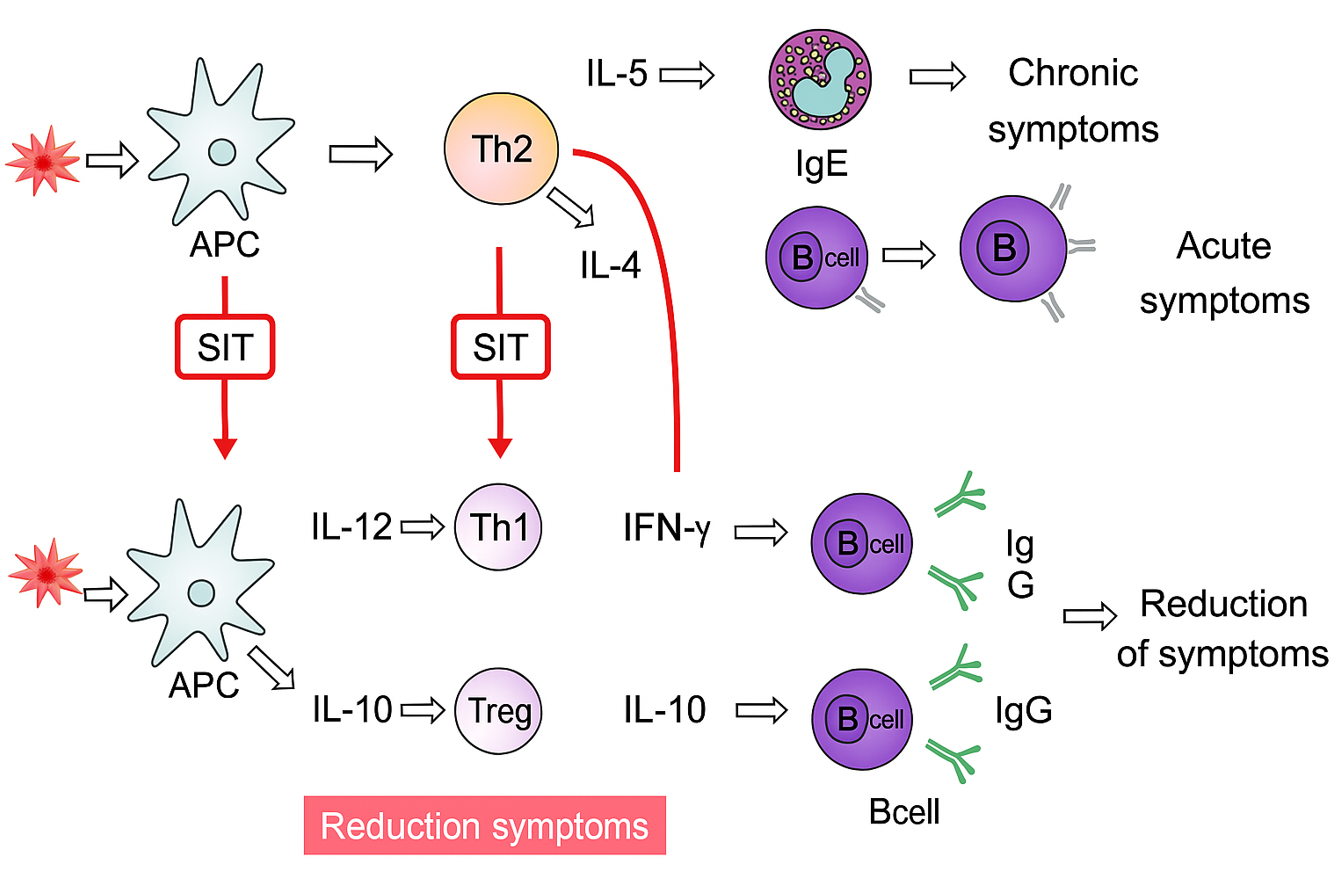
Figure 8: Mechanism of Allergen-Specific Immunotherapy (SIT) in Reducing Allergic Symptoms
5 Quercetin in Neurodegenerative Diseases
Neurodegenerative diseases, including Alzheimer’s disease (AD) and Parkinson’s disease (PD), are marked by progressive neuronal loss, oxidative stress, chronic inflammation, and the accumulation of misfolded protein aggregates. These pathological features contribute to synaptic dysfunction, mitochondrial impairment, and cognitive decline. Quercetin has emerged as a promising neuroprotective agent due to its potent antioxidant and anti-inflammatory properties [80]. It enhances neuronal survival by scavenging reactive oxygen species (ROS) and upregulating endogenous antioxidant enzymes such as superoxide dismutase (SOD) and glutathione peroxidase (GPx) [81]. Additionally, quercetin attenuates neuroinflammation by inhibiting microglial activation and suppressing the expression of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α) and interleukin-1β (IL-1β). These actions collectively contribute to the preservation of neuronal integrity and function in preclinical models of AD and PD [82]. In models of Alzheimer’s disease (AD), quercetin has been shown to attenuate amyloid-beta (Aβ) aggregation, inhibit β-secretase activity, and enhance cognitive performance, including memory and learning [83]. In Parkinson’s disease (PD) models, it confers neuroprotection by shielding dopaminergic neurons from oxidative damage and improving motor function. However, quercetin’s limited permeability across the blood–brain barrier (BBB) remains a major obstacle to its clinical translation [84]. To address this, a range of nano formulation strategies—including liposomes, solid lipid nanoparticles (SLNs), polymeric nanoparticles, micelles, and phytosomes—have been developed to enhance its central nervous system (CNS) bioavailability. These delivery systems improve solubility, protect quercetin from metabolic degradation, and facilitate targeted transport across the BBB. Notably, quercetin-loaded nanocochleates and nanoarchaeosomes have also shown promise in improving CNS uptake and therapeutic efficacy [85]. Collectively, these advances suggest that nanoengineered quercetin formulations may serve as effective disease-modifying agents in the management of neurodegenerative disorders. [84,85].
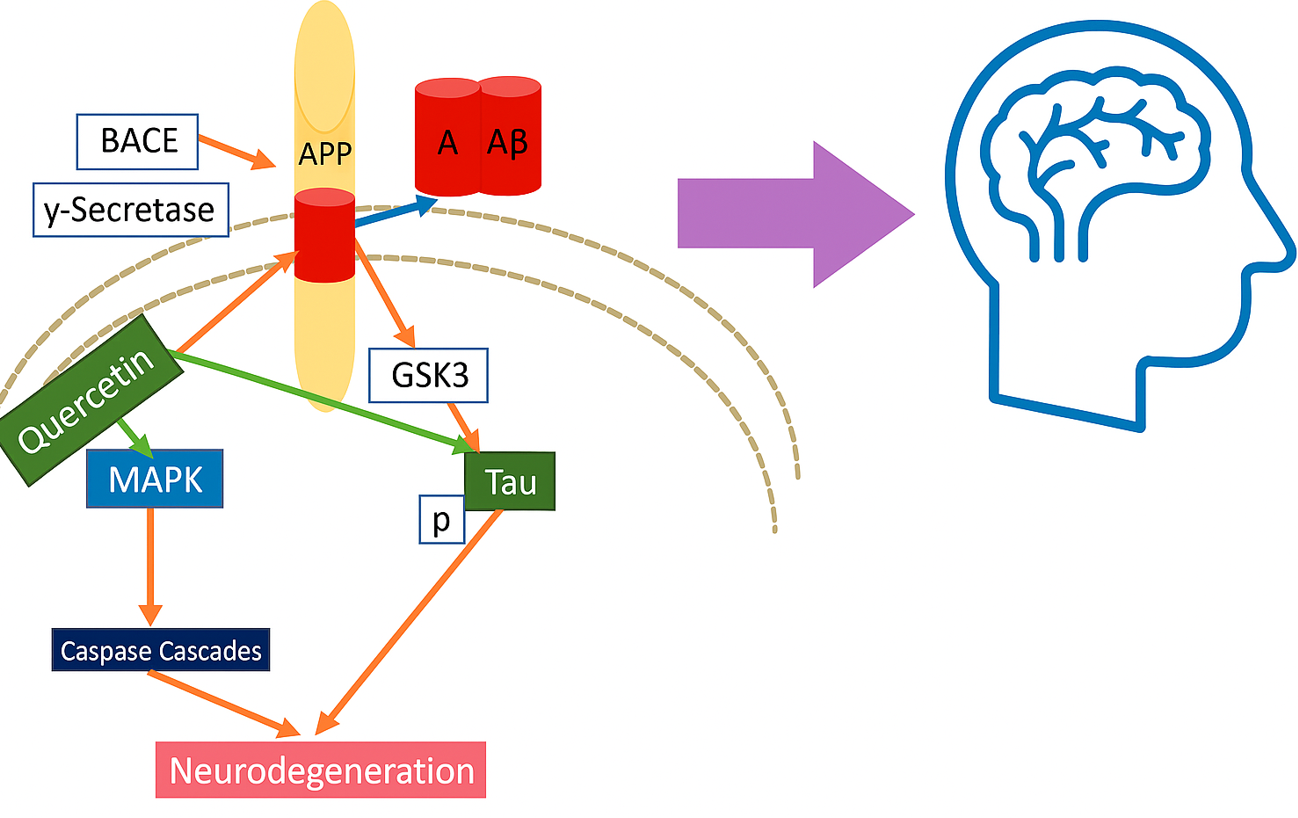
Figure 9: Quercetin Intervention in Amyloid-β and Tau-Mediated Neurodegeneration
6. Pharmacokinetics and Bioavailability
Despite its broad pharmacological promise, the clinical application of quercetin is significantly constrained by its poor oral bioavailability. As a lipophilic molecule with limited aqueous solubility, quercetin exhibits low gastrointestinal absorption. This is further compounded by extensive first-pass metabolism in the intestinal mucosa and liver [86]. Where it undergoes rapid phase II conjugation reactions—namely, glucuronidation, sulfation, and methylation—resulting in minimal systemic availability of the active aglycone form. Moreover, quercetin’s short plasma half-life and rapid renal clearance further diminish its therapeutic efficacy following oral administration.[87]. To address the pharmacokinetic limitations of quercetin, a range of advanced drug delivery strategies have been developed to enhance its solubility, stability, and systemic bioavailability. Among these, nanoformulations—including polymeric nanoparticles, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs)—have demonstrated significant potential in improving oral absorption and extending circulation time. Additionally, liposomes and phospholipid-based phytosomes enhance gastrointestinal permeability and protect quercetin from enzymatic degradation during transit through the digestive tract [84,88]. These nanocarriers not only optimize pharmacokinetic parameters but also enable targeted delivery, which is particularly advantageous in treating site-specific conditions such as neurodegenerative disorders and localized inflammatory diseases. Collectively, these formulation innovations represent a critical step toward translating quercetin’s multifaceted therapeutic potential into effective clinical interventions [85,88].
7. Clinical Evidence and Limitations
Although preclinical studies have consistently highlighted quercetin’s therapeutic efficacy across a range of disease models, clinical evidence remains limited and somewhat inconclusive. Several small-to-moderate scale randomized controlled trials have investigated quercetin supplementation in conditions such as hypertension, allergic disorders, and metabolic syndrome, reporting favorable outcomes [89]. For example, quercetin doses between 500–1000?mg/day administered over 4–10 weeks have been associated with significant reductions in systolic and diastolic blood pressure in hypertensive individuals. Similarly, in allergic rhinitis, quercetin has demonstrated symptomatic relief—reducing nasal congestion, sneezing, and serum histamine levels—though findings are primarily derived from pilot studies or adjunctive therapy settings. Despite these encouraging results, critical gaps persist in the clinical literature. Many studies suffer from small sample sizes, short intervention durations, and inconsistent dosing protocols, limiting the robustness and reproducibility of findings. Additionally, challenges related to poor bioavailability, lack of standardized formulations, and the absence of large-scale, multicenter trials hinder the generalizability of outcomes. From a safety perspective, quercetin is generally well-tolerated at doses up to 1000?mg/day, with adverse effects typically limited to mild gastrointestinal discomfort. However, long-term safety data and comprehensive drug interaction profiles remain insufficiently characterized. To fully realize quercetin’s clinical potential, future research should prioritize rigorous, well-powered clinical trials employing standardized dosing regimens, advanced delivery systems, and extended follow-up periods, particularly in the context of chronic inflammatory and degenerative diseases.[89].
CONCLUSION AND FUTURE PERSPECTIVES
Quercetin, a naturally occurring flavanol, exhibits considerable promise as a multi-target therapeutic agent for managing asthma, hypertension, allergic rhinitis, and neurodegenerative disorders. Its broad-spectrum pharmacological profile—encompassing antioxidant, anti-inflammatory, immunomodulatory, Vaso protective, and neuroprotective activities—enables it to modulate key molecular and cellular pathways implicated in the pathogenesis of these conditions. Mechanistically, quercetin neutralizes reactive oxygen species (ROS), suppresses pro-inflammatory cytokines such as TNF-α and IL-6, stabilizes mast cells to inhibit histamine release, enhances endothelial nitric oxide bioavailability, and protects neurons from oxidative damage and apoptosis. These pleiotropic actions position quercetin as a compelling candidate for therapeutic intervention in chronic diseases characterized by overlapping features such as oxidative stress, immune dysregulation, and persistent inflammation. Despite compelling preclinical evidence supporting quercetin’s therapeutic potential, its clinical translation remains significantly limited. Key pharmacokinetic barriers—including poor aqueous solubility, low gastrointestinal absorption, extensive first-pass metabolism, and a short plasma half-life—result in suboptimal systemic bioavailability and reduced therapeutic efficacy. Moreover, existing clinical trials are constrained by methodological limitations such as small sample sizes, heterogeneous dosing regimens, and brief intervention periods. These factors collectively hinder the establishment of standardized clinical guidelines and limit the generalizability of findings. To bridge the translational gap, future research should prioritize strategies that address quercetin’s pharmacokinetic limitations through the development of advanced drug delivery systems. Nano formulations—such as liposomes, polymeric nanoparticles, solid lipid nanoparticles (SLNs), and phytosomes—have shown considerable promise in enhancing solubility, gastrointestinal absorption, and targeted tissue delivery, particularly to the brain and vascular endothelium. Additionally, exploring quercetin in combination with conventional therapeutic agents may yield synergistic effects, reduce adverse drug reactions, and enable dose minimization of synthetic compounds. Robust, long-term randomized controlled trials (RCTs) are essential to define optimal dosing regimens, assess long-term safety, and validate disease-specific applications across diverse clinical populations. With continued innovation in formulation science and rigorous clinical validation, quercetin may transition from a promising phytochemical to a clinically viable adjunct or standalone therapy for chronic inflammatory and neurodegenerative diseases. Its integration into evidence-based medicine could offer a natural, multi-targeted approach to conditions with limited therapeutic options or burdensome side-effect profiles.
REFERENCES

Priksha Patel*, Jitendra Pandey, Vikram Singh Yadav, Quercetin’s Therapeutic Potential in Chronic Diseases: Mechanistic Insights and Clinical Applications in Asthma, Hypertension, Allergic Rhinitis, And Neurodegeneration, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2190-2209. https://doi.org/10.5281/zenodo.15969392
 10.5281/zenodo.15969392
10.5281/zenodo.15969392
