Krishna school of pharmacy & Research, Drs. Kiran & Pallavi Patel Global University (KPGU) Vadodara-Mumbai National Highway 8, Varnama, Vadodara - 391240, Gujarat, India.
CRISPR technology is an innovative technology used in the genome editing process which has the capacity of revolutionizing healthcare. cancer study and treatment. Its accuracy in striking and altering particular genetic driver mutations that feed tumor growth provides new scope on making more functional, individualized treatments of cancer. This involves such strategies as inactivation of tumor promoting genes, enhancing immune system of attacking cancer cells, rectifying the cancer-causing genetic mutations, and directing cancer-killing molecules to tumor’s. There are problems persistence preclinical research, clinical trials that test its safety and delivery are taking place potential. The CRISPR system originates as a means of bacterial defense. When it encounters a large piece of viral DNA, system inserts the complement of an existing spacer into the CRISPR array to create a new spacer to prevent future replication of this type of virus enters a bacteria. Methods using CRISPR are being pioneered to better the immune. The reaction of the immune system to cancer cells and silencing genes that encourage tumor growth. CRISPR is applied to discover and bring novel drugs. CRISPR-Cas9 In Agricultural biotechnology it has opened up possibilities in this area and it can increase the yields, enhance nutritional value as well, etc. increase crop resistance. We shall end up with a summary of the prospects. The issues that CRISPR-mented cancer treatment has to deal with today and discussing possible ones in the future research and development channels. The CRISPR system could turn the terrain. the reason the study is to provide an overview of where the field is today and the challenges which need to be done away with so as to tap this potential.
The use of CRISPR (Clustered Regularly interspaced short palindromic repeats).The technology has revolutionizing opportunities in cancer treatment and aids the accuracy and efficiency of cancer treatment. Genome editing to combat maladaptive genetic alterations that are the cause of cancer.[1]. The Findings of CRISPR technology in 2012 were an important breakthrough in the area of genome programmable editing of CRISPR-linked enzymes, including Cas9, can be assorted to edit particular DNA sequences, and in combination with guide RNAs, edit, delete or cut a gene exactly [2]. There is so much potential of its use in cancer research. Increased attention was paid, especially to its ability to act against the genetic mutations by which tumour grows as apoptosis, proliferation and metastasis.[3]
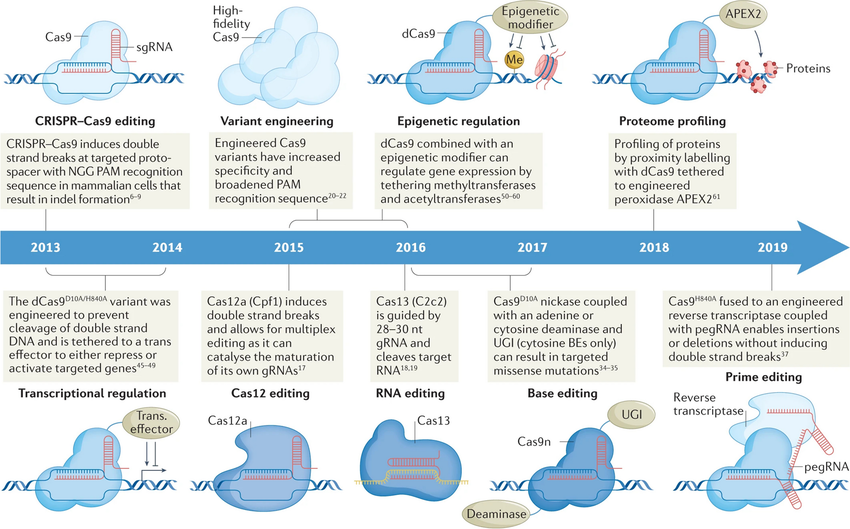
Fig 1: The invention of the CRISPR technology has transformed research concerning cancer. since the introduction of Cas9-associated CRISPR gene editing on mammalian cells. The swift growth of CRISPR technology has brought about specialised CRISPR variants which respond to difficulties. Such variations have been developed through intent. The design and evolution: furnishing them with additional versatility in recognition more precisely selecting targets better protospacer adjacent motifs. Researchers have successfully exploited naturally occurring variants of CRISPR in different bacteria, like Cas12a and Cas13, to enable combinatoric knockout and further RNA specificity, respectively. CRISPR base editing has allowed placement of targeted mutations at the transition level A Cas9 nickase fused with an adenine or cytosine deaminase can also be used. Base editing of cytosine A uracil glycosylase inhibitor is used by the enzymes to ensure there is an increased mutation that is C > T in nature. The latter is depicted in Figure 1 with respect to the development of CRISPR tools in the context of exploring cancer biology. The CRISPR associated enzymes can be programmed and used to target a specific DNA sequence like Cas9 and be used to cut, modify or delete specific genes in a precise way particularly with a guide RNA. [2]
CRISPR?based strategies for cancer therapy:
The introduction of CRISPR based gene editing technology can have dramatic relevance in cancer treatment, to enable the genome to be corrected accurately to respond and attack the malignancy mutations that cause proliferation and metastasis of tumours.[4]. An explanatory description begins by the initial phases of CRISPR screening that includes the organization of genome-specific targets. Then, a custom-design and fabrication of CRISPR guide would be done. RNA libraries are introduced, the central role of which is to help determine precise genomically. The next section explores the service models used in the service delivery. CRISPR reagents into other cells. Additionally, it is the application of selective pressures how to select cells bearing desired genetic changes is then described, and this leads to the analysis of the resultant screening data. Several different CRISPR-based strategies have been proposed for cancer therapy, each with their own advantages and limitations.[5]
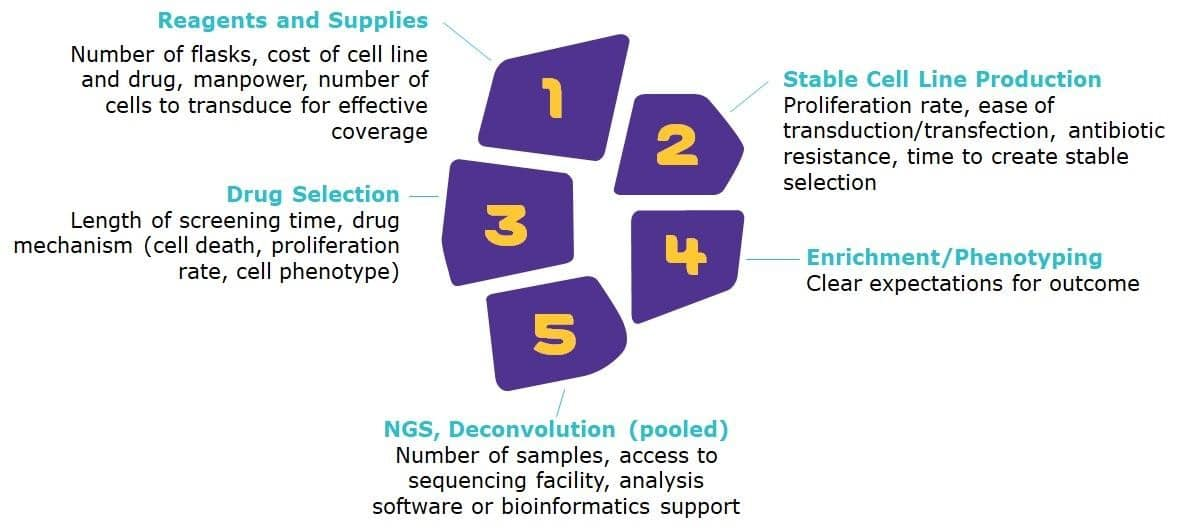
Fig 2: General Considerations for CRISPR Screening
Reagents and Supplies:
When designing a CRISPR screen, the initial consideration pertains to the availability of requisite materials. Variables including the cost and scalability of reagents and cellular models significantly influence screen design. For instance, the substantial number of cells necessitated by screening protocols may be impractical when utilizing primary cells, thereby necessitating the adoption of a cell line boasting heightened proliferative capabilities. Moreover, the cost and availability of reagents assume paramount importance due to their potential to impinge upon screen scope.
The genesis of cell lines expressing the Cas9 nuclease represents a crucial preliminary stage in numerous CRISPR screening workflows. This process can exhibit considerable variability in terms of duration and methodologies employed, contingent upon the chosen cell line and the transfection strategy adopted, whether transient or stable. Optimal stability in Cas9 nuclease expression, resulting in uniform nuclease levels throughout the screen, can be achieved via stable cell line production. Nevertheless, generating stable Cas9 transfectants is a labour-intensive process compared to transient expression. The isolation of Cas9-expressing cells can be accomplished through either antibiotic selection or fluorescence-activated cell sorting (FACS), contingent upon the presence of an antibiotic resistance gene or a fluorophore within the expression vector.
The mechanism of action for the drug selected for the screen determines the required screening time as well as dictates the phenotype to screen.
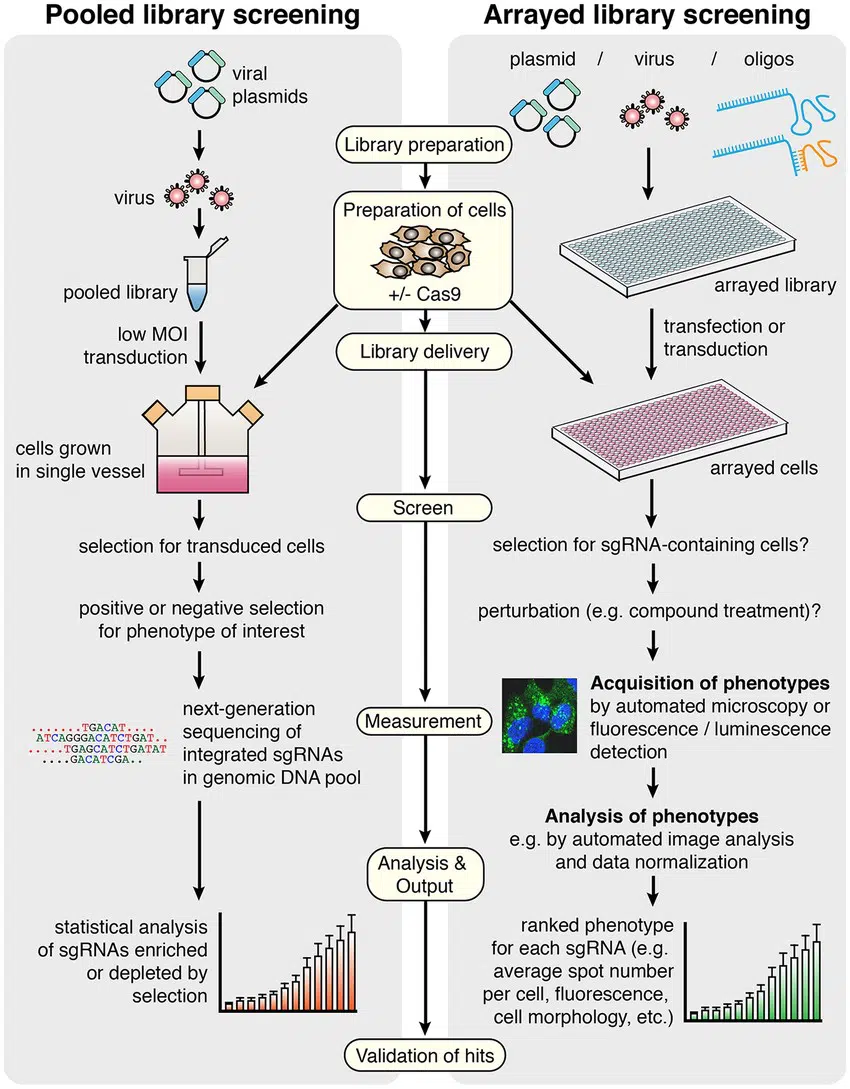
Fig 2: CRISPR/Cas9-based screen general workflow in pooled versus arrayed strategies. 2015 Agrotis and Ketteler [5], licensed under CC BY 4.0. MOI, multiplicity of infection; sgRNA, single guide RNA.
CRISPR Knock-in Screens: To achieve CRISPR-mediated gene knock-ins, which entail the insertion of a nucleic acid sequence into a predetermined gene locus, involve the simultaneous delivery of a donor DNA template in conjunction with the CRISPR machinery. This methodology presents technical complexities, rendering it less feasible for large-scale applications compared to knockout strategies, and limiting its scalability to target individual genes.
CRISPRa and CRISPRi Screens: Both CRISPRi or CRISPRa are scalable and allow screening of genes through both repression and activation of transcription.[7] These systems use a nuclease-deficient version of Cas9 (dCas9), which can still bind and recruit additional domains to a gRNA target site but cannot cut the target DNA. [8, 9]. In CRISPRi, dCas9 is fused with a transcriptional repressor, such as KRAB, while CRISPRa requires transcriptional activators, including VP64.[9]. The most effective CRISPRa system uses the CRISPR Synergistic Activation Mediator (SAM) complex. This system uses a dCas9-VP64 complex, with two additional transcriptional activators introduced into the cell alongside the gRNA. [9,10,11].
Synergistic Use of Screens: Utilizing multiple screening formats provides complementary insights into the same pathways. [7,8]. A notable instance of CRISPR's utility in cancer research is evident in a published study. The examination, employing CRISPRa-mediated tumor growth screening and CRISPRi-based loss-of-function assessment, elucidated crucial tumor suppressors in K562 cells and essential housekeeping genes respectively. Furthermore, the integration of CRISPRa with a CRISPRi-based toxicity screen provided enhanced insight into cytotoxicity pathways. Notably, the concomitant use of CRISPRa and CRISPRi identified genes with disparate effects on cell sensitivity to ricin treatment, including both sensitizing and desensitizing genes.[8].
CRISPR Drug Screening
CRISPR screening utilizes a CRISPR- Cas9 complex with a gRNA library to tune the activity of several genes together. The CRISPR method allows simultaneous, Loss-Of-Function (LOF) and Gain-Of-Function (GOF) screens through the use of dCas9 used as covalent fusions to transcriptional repressors or activators. This pooled LOF/GOF design enables the discovery of repressing and activating components in pathways under study, thus making possible the identification of genes involved in mediating downstream effects of a resistance to some drugs or a drug. This synergistic strategy further facilitates the identification of prospective targets for supplementary investigation. CRISPR screens can be executed in either arrayed or pooled formats, wherein arrayed screens possess increased analytical simplicity but are resource-intensive, whereas pooled screens are more cost-effective but necessitate complex downstream data analysis due to deconvolution requirements.
CRISPR in Oncology—Preclinical Use
In normal cellular development, proto-oncogenes serve as pivotal regulatory molecules governing cell differentiation and proliferation. However, aberrant mutations or modifications of these proto-oncogenes can transform them into oncogenes, thereby facilitating carcinogenesis. Conversely, tumor suppressor genes function as crucial barriers to unbridled cellular proliferation, exerting a braking influence on aggressive cell divisions. When oncogenes assume an active form, tumor suppressor genes are capable of curtailing aberrant growth. In healthy cells, these tumor suppressors play a protective role against cell cycle overexpression, and their functions encompass monitoring cell division rates, repairing mismatched DNA sequences, and modulating the process of programmed cell death.[12]. Three major tumor suppressor genes, BRCA1, BRCA2, and TP53, regulate distinct stages of the cell cycle.[13]. The complex phenomenon of tumorigenesis as a consequence of the mutations of DNA may be subdivided into four specific forms: tumorigenic initiation, promotive upsurge, cancerous transformation, and proliferative overhead. Although each separate mutation may not be very significant in the harmful effect, combination of the effects of age-related mutations eventually leads to a rise in the frequency of carcinogenesis and the development of tumours. Genomic instability in malignant cells Another characteristic of malignant cells is their genomic instability, more precisely chromosomal instability, whereby there is a frequent change in chromosomal morphology. The time of emergence of the genomic instability throughout cancer initiation remains obscure. Unstable genes undergo more rapid cell cycles and thus circumvent normal cell division checkpoints hence encouraging cell malignancy transformation.[14] The increased knowledge in the process of carcinogenesis process triggered new opportunities to develop new measures to prevent abnormal cell growth. This entails the use of gene-editing technologies, namely, CRISPR, which allows a precise change of the DNA sequence using nucleotide changes to correct the harmful mutations, thus obtaining control and possibly preventing the development of carcinogenesis.[15] CRISPR/Cas9 has many potential uses in oncology, including creating cancer models, identifying targetable genes, evaluating for resistance mechanisms, and modulating efficacy of immunotherapies [16,17]. The increasing approval of checkpoint inhibitors and T cell therapies as initial treatments necessitates optimized efficacy. The CRISPR/Cas9 system's capacity for precise gene knockout is highly desirable for addressing longstanding challenges, such as T cell exhaustion and the immunosuppressive effects of the tumor microenvironment. Moreover, the gene-editing capabilities of CRISPR/Cas9 facilitate the development of novel targeted oncology therapies. Clinical and preclinical trials have demonstrated the efficacy of CRISPR/Cas9 systems in various settings. T cell exhaustion poses a substantial limitation to both endogenous antitumor responses and CAR-T cell efficacy, particularly in immunosuppressive microenvironments.[18] Previous research has identified T cell exhaustion signatures as predictors of clinical outcome in patients with relapsed/refractory CLL treated with CD19+ chimeric antigen receptor T (CAR-T) cells.[19]
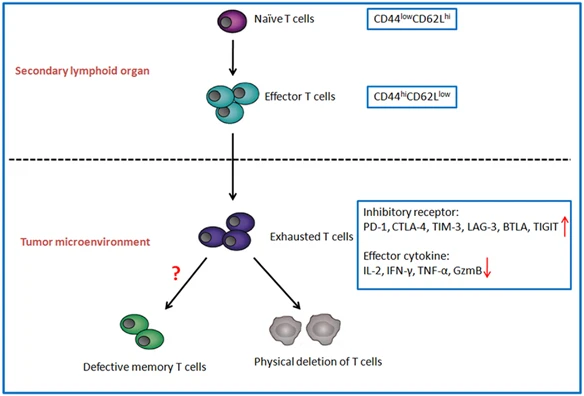
Fig:03 T-cell exhaustion and differentiation in TME. Naive T cells (CD44lowCD62Lhi) activate and differentiate into effector T cells (CD44hiCD62Llow) in secondary lymphoid organ. When effector T cells enter TME, they are polarized into exhausted T cells, with decrease in effector cytokines (IL-2/IFN-γ/TNF-α/GzmB) and increase in inhibitory receptors (PD-1/CTLA-4/TIM-3/LAG-3//BTLA/TIGIT). Subsequently exhausted T cells may turn to be defective memory T cells or be deleted physically
The initial observation of T-cell exhaustion was in chronically infected mice, followed by this in individuals with cancer. There is an elevated number of inhibitory receptors on T-cells in the cancerous environment secrete reduced levels of effector cytokines and cytotoxic compounds leading to tumour cell. Exhausted T cells In a model of the chronic lymphocytic choriomeningitis virus (LCMV), T cells have the largest have been identified as. Namely, LCMV-specific CD8+ T cells, characterised co-expressing activation markers (CD69hiCD44hiCD62Llow) and impaired, as indicated by, antiviral activity.[20]
T-cell exhaustion refers to T-cell dysfunction in persistent environment, worn-out T cells have high amounts of inhibitory receptors which includes:
Characteristics of exhausted T cells are primarily marked by the progressive decline of function in a hierarchical order. Initial impairments are observed in the capacity for interleukin-2 (IL-2) production and ex vivo killing ability, followed by deficiencies in tumor necrosis factor-alpha (TNF-alpha) production, and ultimately, disruptions in interferon-gamma (IFN-gamma) and granzyme B (GzmB) production as exhaustion advances. [27,28].
Endogenous Processes Participating in T-Cell Exhaustion and Differentiation in
TME: Full activation of T cells necessitates three signals,
• the initial cue is the engagement between antigenic peptide MHC complex with TCR,
• the second signal is costimulatory or co-inhibitory signal by the antigen presenting cells,
• the third message is stimulation by extracellular cytokines like IL-2.[29]
Activation or inhibition of T-cell activity is regulated further by the second signal, which is a set of coinhibitory signals that do not produce excessive inflammation, except in the case where promotion of the second signal is excessive, leading to suppression of T-cells.[30]The adverse regulators of T cell functionality and survival can be removed in CAR-T cells using CRISPR/Cas9, in theory, enhancing the therapeutic response.[31] Notably, a preclinical intervention in lung cancer has been achieved through the application of CRISPR technology to eliminate mutated EGFR gene variants, leading to diminished cellular proliferation in vitro and in vivo settings. Moreover, targeted disruption of EGFRs in a non-small-cell lung cancer (NSCLC) cell line has been accompanied by the induction of apoptosis and resultant decrease in tumor size in vivo. [32,33]. Diagnostic tools used in CRISPR: The FPGAs role in the CRISPR Diagnostic Workflow.
The data analysis part of the diagnostic workflow is merged with FPGAs:
Raw Data Acquisition: A CRISPR-based assay is carried out, which produces a signal (e.g., fluorescence) which a detector captures. This signal is related to the existence or inexistence of a target biomarker.
Signal Processing: The detector output is an input to an FPGA. The custom hardware of the FPGA can be configured to handle an assortment of signal processing functions, including noise removal and signal amplification of the signal of interest.
Data Analysis and Interpretation: The FPGA processes the data and identifies and counts the target biomarkers. This may include sophisticated bioinformatics sequence-alignment and sequence-comparison algorithms. The speed of the FPGA is such that results can be interpreted quickly giving a diagnosis within minutes.
Diagnostic Devices: FPGAs are also applied to compact, portable diagnostic devices, which are therefore applicable in point-of-care testing in a clinics or field environment. FPGAs also used low power which is an added benefit to these battery powered machines.[65].
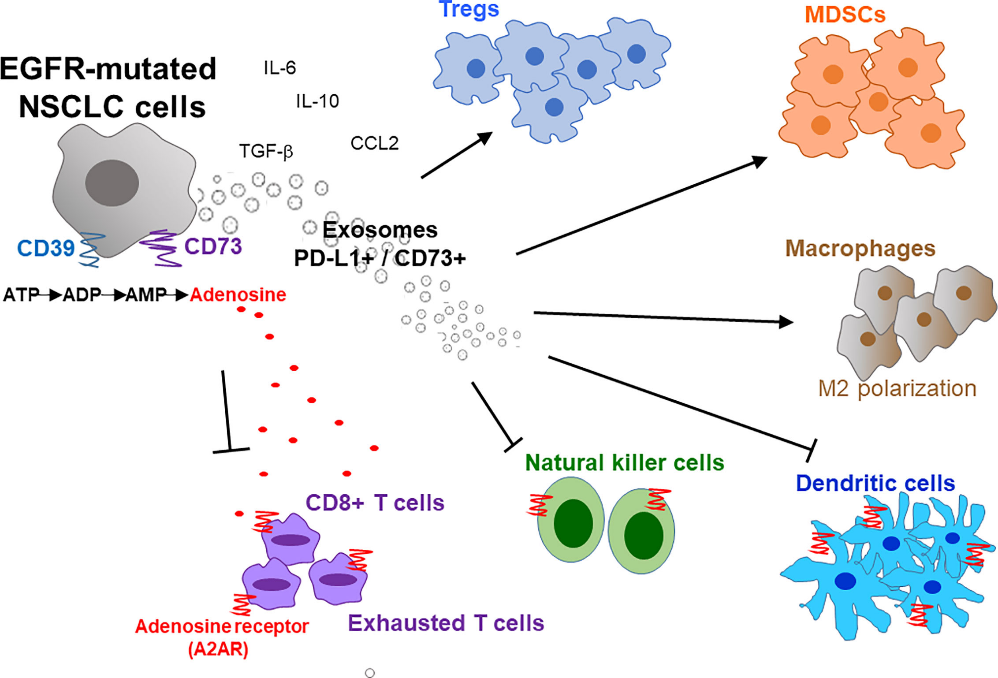
Fig: 04 The tumor microenvironment (TME) associated with epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (NSCLC) exhibits immunosuppressive characteristics. This immunosuppression is facilitated by EGFR mutations interfering with various intracellular signalling pathways and modulating the function of accessory immune cells within the tumor, including lymphocytes, natural killer cells, regulatory T-cells, myeloid-derived suppressor cells, and tumour-associated macrophages.[34]
Since 2018, scholarly research has applied the CRISPR/Cas9 technology to develop targeted treatment strategies tailored to specific cancer subtypes.[35] Presently, various therapeutic approaches involving proteins with potential oncogenic properties are being explored. A study by Ebright et al. demonstrated the utility of CRISPR/Cas9 as a genome-wide screening tool to identify genes associated with metastasis, notably the overexpression of RPL15, a component of the 60S ribosomal subunit implicated in the metastatic progression of breast cancer.[36]. Studies have demonstrated that CRISPR/Cas9-mediated knockout of the FASN gene, which is involved in estrogen receptor signaling, can significantly attenuate the proliferation and migratory capabilities of breast cancer cells.[37] Furthermore, while the utility of CRISPR/Cas9 technology for triple-negative breast cancer remains to be explored, recent findings indicate that 80% of BRCA1 mutations are associated with the development of this subtype. Notably, given the synthetic lethality exhibited in BRCA1-deficient cells, CRISPR/Cas applications may be harnessed to target the PARP1 gene, thereby offering a novel therapeutic approach for breast cancer treatment, particularly for BRCA1-deficient cells.[38]. Research has successfully utilized CRISPR technology to eliminate the estrogen receptor β (ERβ) gene in prostate cancer. Although androgen receptors are predominantly responsible for regulating prostate function, ERβ is implicated in the differentiation of prostate cells and exerts various inhibitory effects on cancerous cells. This finding highlights CRISPR's potential application in cancer treatment by targeting alternative mechanisms beyond androgen receptors.[39].
CRISPR Use in Cancer Prevention
Cancer is primarily a genetic disorder, resulting from genetic and epigenetic alterations that jointly lead to uncontrolled cell proliferation. As genome editing technologies, particularly those based on CRISPR/Cas9, continue to advance, the objective of cancer gene therapy may shift from treatment to prevention. Nevertheless, before utilizing CRISPR for cancer prevention in healthy individuals, achieving accurate and efficient correction of genetic mutations while minimizing unintended consequences is crucial. Hereditary cancer conditions linked to well-defined cancer-promoting mutations present a promising therapeutic opportunity for utilizing CRISPR-assisted mutation correction. The ability to adapt the CRISPR/Cas9 system for targeting and repairing cancer-causing mutations in cell cultures and animal models has been extensively validated. However, the effectiveness of these genome editing approaches in nonclinical trials, several barriers exist before these strategies can be employed as a powerful family cancer prevention strategy in families with hereditary cancer predisposition. [40,41,42]. Other types of hereditable cancer, including TP53 in Li-Fraumeni syndrome, mismatch repair genes in hereditary non-polyposis colorectal cancer, and BRCA1 and BRCA2 in breast and ovarian cancer syndromes, may also confer susceptibility to many organs as well as overgrowth and neurodevelopment in a variety of cell types.[40,41,42]
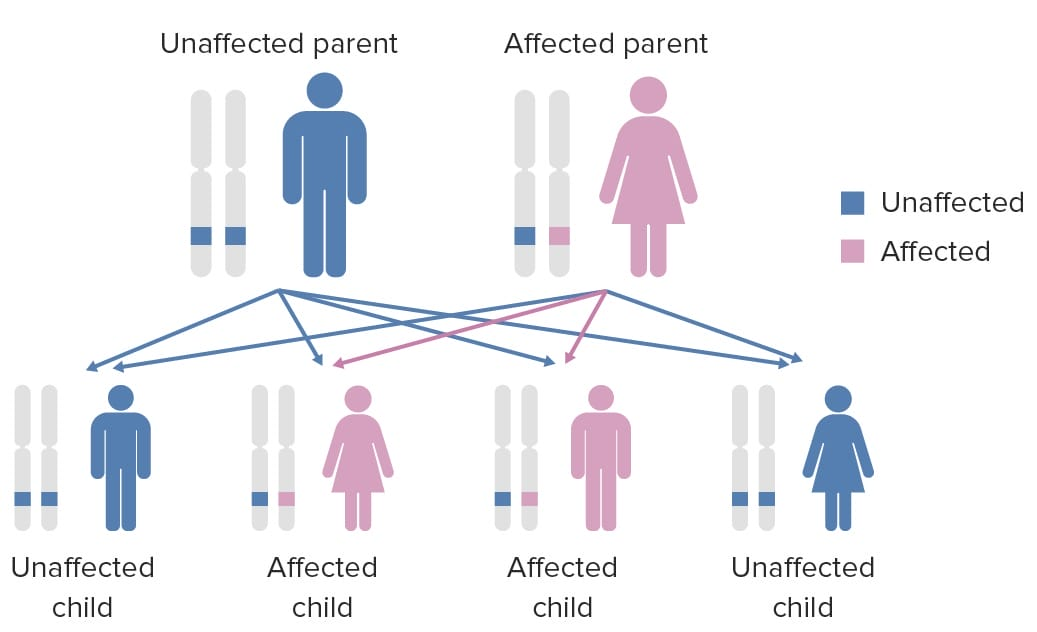
Fig: 05 Li Fraumeni Syndrome: Li-Fraumeni syndrome (LFS) is a rare, inherited cancer predisposition syndrome caused by mutations in the TP53 gene. Individuals with LFS have a significantly increased risk of developing various cancers, including sarcomas, breast cancer, brain tumors, and adrenocortical carcinoma, often at an early age.[43]
Existing CRISPR delivery systems, such as adeno-associated viruses (AAVs), enable stable and tissue-specific expression of DNA in targeted cells. However, repeated administration of AAV may be necessary to maintain high levels of repaired cells, raising potential safety issues. Persistent Cas9 activity can increase the risk of off-target DNA damage over time. [44,45] Furthermore, the host may develop an immune response to Cas9 due to peptides acting as MHC-binding epitopes. Studies have also found that cells edited by CRISPR exhibit functional impairments, including reduced proliferation and differentiation capabilities, reportedly due to activation of the p53-mediated DNA damage response.[46]. Studies have shown that employing CRISPR/Cas9 to target the HPV E6 and E7 genes successfully reverses the malignant characteristics of cervical cancer cell lines.[47] Additionally, CRISPR/Cas9 has been utilised to target HBV and HCV in cellular and mouse models with the potential to prevent hepatocellular carcinoma.[48,49,50] Furthermore, preclinical research has successfully applied the CRISPR/Cas9 system to inhibit EBV replication in a Burkitt’s lymphoma B cell line.[51,52].
CRISPR use for Clinical Cancer Treatment
Preliminary investigations of CRISPR/Cas9 have indicated considerable promise in its application for cancer therapy, with recent developments advancing to Phase I clinical trials.[53]. A phase I clinical trial was performed by Stadtmauer et al. to perform an important preliminary study of the potentialities of the CRISPR-Cas9 gene editing system to use it in generation T cells with immunotherapy use. Investigators in this first study examined the evidence. They used CRISPR-Cas9 to make specific gene modifications on T cells of three patients who had resistant malignancies. The effectiveness of eliminating the expression of endogenous T cell receptor (TCR) components by using CRISPR-Cas9 and increasing a TCR transgene that binds to tumor cells was tested.[54] In addition, CRISPR-Cas9 was used to knock out one of the genes participating in programmed cell death protein 1 (PD-1) encoding. The effectiveness of administering and sustained presence of the engineered T cells in the participants of the study in up to nine months proved to be a strong fact on the possibility of utilizing CRISPR-Cas9 tool in the field of immunotherapy in gene editing. The landmark trial has led to the development of targeted immunotherapies and has played a great role in enhancing the survival rate of patients in the process the effectiveness of currently available immune therapeutic regimens. Studies conducted via two phase I trials have validated the safety and efficacy of CRISPR/Cas9-mediated T cell modifications in treating lung cancer. A research trial initiated by Lu et al. involved 22 patients with advanced non-small cell lung cancer, where 12 individuals underwent T cell treatment incorporating PD-1 gene editing executed by CRISPR/Cas9 gene editing technology.[55]. Edited T cells were found in peripheral blood following infusion without any severe adverse reactions. The study reported a median progression-free survival of 7.7 weeks and an overall median survival of 42.6 weeks. In order to assess potential off-target outcomes, the research utilised next generation sequencing, revealing a median mutation frequency of 0.05%. This further underscores the safety and viability of CRISPR/Cas9 edited T cells. More recently, 15 patients with solid tumours expressing the mesothelin antigen participated in an investigation conducted by Wang et al., where CRISPR/Cas9 was employed to generate T cells deficient in PD-1 and T cell receptor components, engineered to target mesothelin and capable of dose escalation.[56]. Recently, Foy et al. conducted a phase I trial, using CRISPR/Cas9 technology to knockout two T cell receptor genes in 16 patients with refractory solid cancers. In a dose-escalating clinical trial, patients received up to three gene-edited TCR products, with only two experiencing adverse reactions, including cytokine release syndrome and neurotoxicity. Remarkably, five patients showed stable disease as the best response to the treatment, which proved the practicality of CRISPR/Cas9 usage to isolate endogenous T cell receptors and simultaneous modification of genes.[57]. Many phase I and II clinical trials are currently ongoing to further investigate the utility of CRISPR/Cas9 technologies in cancer treatments. One long-standing barrier to widespread implementation of T cell therapy has been inherent limitations of autologous donation to manufacture the engineered T cell therapy. Patients with cancer often have suboptimal T cell populations for harvesting, and their malignancy may progress during the in vitro expansion period. Allogeneic T cell immunotherapy remains a highly desirable goal and area of considerable ongoing pre-clinical and clinical research. Currently, there are number of ongoing phase 1 clinical trials utilizing T cells donated by healthy donors and modified to express CRISPR/Cas9 engineered CAR cells [58,59,60]. Another phase I trial is evaluating autologous T cells engineered to target CD19 and CRISPR gene edited to eliminate endogenous HPK1 in CD19+ leukaemia or lymphoma (XYF19 CAR-T cells).[61]. Utilizing CRISPR/Cas9 mediates precise and homologous integration of transgenes, thereby mitigating the variability in transgene expression often associated with conventional retro- or lentiviral transduction techniques. This methodological approach is exemplified by CTX110 and CTX112, chimeric antigen receptor (CAR) T-cell therapies targeting the CD19 antigen, which are currently being evaluated for the treatment of relapsed or refractory B-cell malignancies. [62,63].
Table: 01 Current Clinical Trails
|
Clinical Trail |
Cancer Types |
Related CRISPR Method |
References |
|
Phase 1 |
Refractory cancers |
Delete two genes that encodes endogenous TCR and a gene encoding PD-1 |
[63] |
|
Phase 1 |
Advanced NSCLC |
Edite PD-1 ON T cells |
[57] |
|
Phase 1 |
Mesothelin-positive solid tumors |
Generate PD-1 and TCR deficient CAR-T cells specific to mesothelin |
[58] |
|
Phase 1 |
Osteosarcoma |
PD-L1 possible target for knockout |
[59] |
|
Phase 1 |
Refractory solid cancers |
Knockout two T cell receptor genes |
[61] |
CRISPR Limitations:
As genome editing using CRISPR/Cas-based strategies advances in terms of efficacy, specificity, and delivery to various cell types, it may soon usher in a new period of significant progress in cancer prevention and treatment modalities. Nevertheless, there remains considerable uncertainty regarding the long-term safety implications of in vivo CRISPR utilization, which will substantially influence our capacity to apply this technology in clinical settings for primary cancer prevention or treatment purposes. The widespread adoption of CRISPR/Cas9 technology is also constrained by the risk of off-target mutations, which, although demonstrated to be infrequent, pose a substantial limitation to its broader utilization.[55] Other constraints include the potential for immune-mediated toxicity arising from pre-existing antibodies against commonly employed bacterial nucleases and the ethical complications associated with gene editing in germ-line cells. [64]. Furthermore, considerations surrounding the cost of manufacturing and delivering CRISPR/Cas9-based therapies must be considered, as well as the possibility that limited availability in non-academic settings may restrict the application of this technology as a therapeutic option.
CONCLUSION:
CRISPR technology represents a revolutionary leap in the fight against cancer, offering unprecedented precision in gene editing that holds immense promise for transforming treatment protocols. Its ability to accurately modify or disable specific genes implicated in cancer development and progression has opened new avenues for therapeutic intervention. CRISPR in oncology has many potential benefits. The current review focuses on the role of CRISPR/Cas9 in oncology, its use with oncolytic viruses and in epigenetics, ongoing clinical trials, applications in cancer immunotherapy, and its potential to combat carcinogenic viral infections. The technology offers remarkable promise as a genome-level tool for cancer treatment, making individualized and precise treatments highly promising for future cancer therapy. Achievements of CRISPR/Cas9 have been documented in immunotherapy, tumor therapy, and research. Future studies will build on the pathophysiology and therapeutic sciences of malignancies. Genome editing with CRISPR/Cas9 is significantly faster, more cost-effective, and superior. CRISPR/Cas9 cell treatments are capable of avoiding transplant rejection issues associated with donor compatibility requirements. Autologous operations involve altering a patient's own genes to correct mutations in their tissues. The technology is particularly promising for disorders treatable by correcting cells with readily correctable mutations.
REFERENCES


Zalak D. Dave*, Vama A. Bhavsar, Recent Advances in CRISPR: Combat Against Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1476-1493 https://doi.org/10.5281/zenodo.17115465
 10.5281/zenodo.17115465
10.5281/zenodo.17115465
