We use cookies to make sure that our website works properly, as well as some ‘optional’ cookies to personalise content and advertising, provide social media features and analyse how people use our site. Further information can be found in our Cookies policy
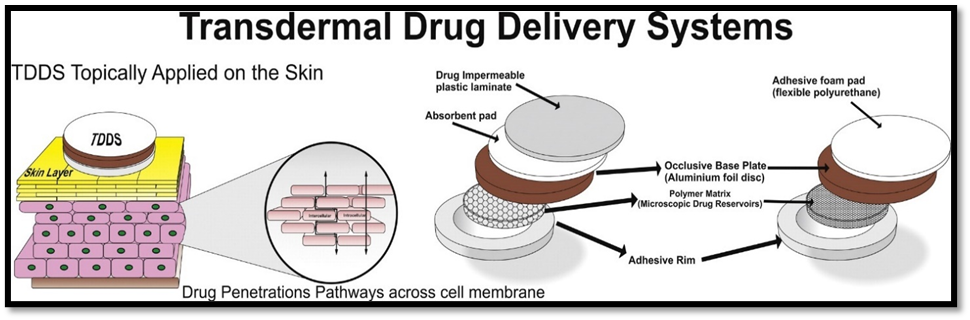
Transdermal drug delivery systems, or TDDS, are a cutting-edge, non-invasive method of systemic medication delivery. Bypassing first-pass metabolism and gastrointestinal breakdown, these systems administer therapeutic chemicals through the skin for a regulated and sustained release. The principles of TDDS, drug permeation mechanisms, formulation elements, transdermal system types, evaluation criteria, and recent developments are all covered in this overview. Compared to more conventional medication delivery methods, the transdermal route offers a number of benefits. These consist of stable medication plasma concentrations, no first-pass hepatic metabolism, good bioavailability, and non-invasive therapy. The stratum corneum, the skin's outermost layer, is the primary barrier to medication molecules penetrating it. It is explained how penetration enhancers and retarders work, as well as how they might be used in clinical settings.
Patches, another name for transdermal drug delivery systems (TDDS), are dosage forms intended to apply a therapeutically effective quantity of medication to a patient's skin. It is necessary to consider the entire morphological, biophysical, and physicochemical characteristics of the human skin to administer medicinal substances through it for systemic effects. By improving patient compliance and preventing first-pass metabolism, transdermal administration offers a significant advantage over injectables and oral methods.(2)
More effective and efficient techniques for transdermal medication delivery have been developed as a result of recent technological developments. With the development of microneedles and nanoparticles, pain has decreased, and the precision of direct medication administration into the bloodstream has improved, potentially revolutionizing medicine and improving patient outcomes. Transdermal Drug Delivery Systems (TDDSs) release medication gradually over time to maintain a constant therapeutic dose in the body(4)
Scopolamine (for motion sickness), nicotine (for smoking cessation), estrogen (for menopause and to prevent osteoporosis after menopause), nitroglycerin (for angina), and lidocaine (for shingles pain; herpes zoster) are among the medications applied as skin patches.
TDDS are specified surface area adhesive drug-containing devices that apply a fixed dosage of medication to intact skin at a preprogrammed pace to enter the systemic circulation. (13-14)
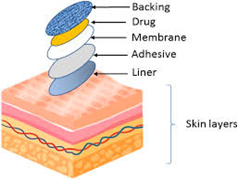
Transdermal Drug Delivery System :
Fig. 1 Transdermal drug delivery system
Definition: A transdermal patch or skin patch is a medicated adhesive applied to the skin to deliver a specific dose of medication through the skin into the bloodstream.(2)
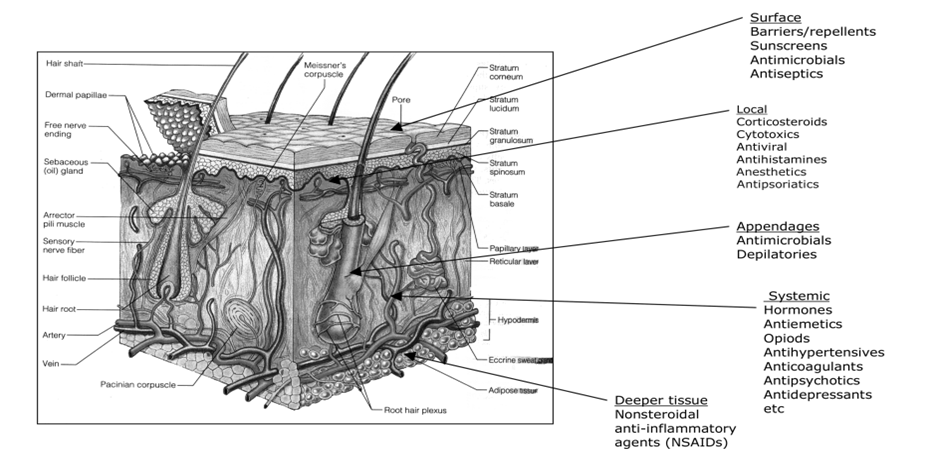
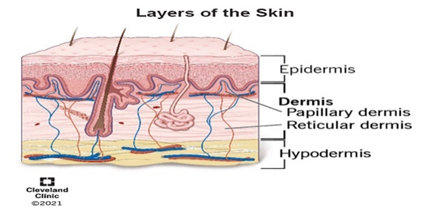
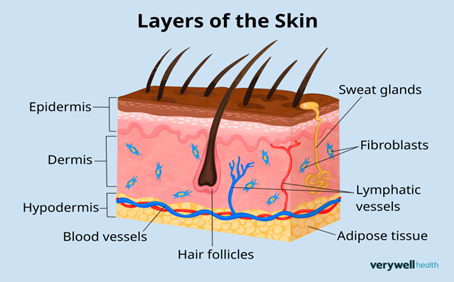
Anatomy of the skin
FIG: 2 Anatomy and physiology of the skin show the potential targets or sites of action(9-15)
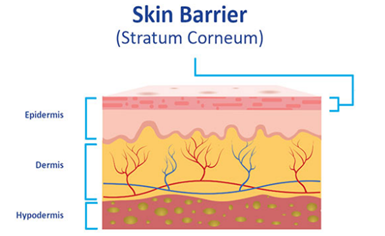
1. Stratum corneum :
This is the outermost layer of skin, also called horney layer
It is flexible but relatively impermeable. The stratum corneum is the principal barrier for penetration
It is approximately 10 mm thick when dry, but swells to several times this thickness when fully hydrated.
The stratum corneum is the principal barrier for penetration. The barrier nature of the horney layer depends critically on its constituents: 75 to 80% proteins, 5 to 15% lipids, and 5 to 10% ondansetron material on a dry weight basis.
Lipid constituents vary with body site (neutral lipids, sphingolipids, polar lipids, cholesterol). Phospholipids are largely absent, a unique feature of mammalian membranes(4)
Fig :3 Stratum Corneum
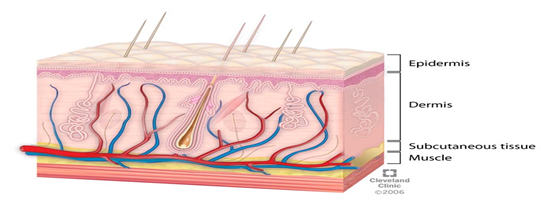
2. Epidermis:
The epidermis, the outermost layer of skin measuring 10–20 mm, comprises dead cells forming the stratum corneum, functioning as a robust barrier. Dead cells that make up the stratum corneum create the epidermis, the skin's outermost layer, which is 10–20 mm thick and acts as a strong barrier. The stratum corneum (SC or horny layer), stratum lucidum (clear layer), stratum granulosum (granular layer), stratum spinosum (spinous or prickle layer), and stratum germinativum (basal layer) (4)
Fig: 4 Epidermis layer
3. Dermis:
The dermis is the second layer after the viable epidermis and ranges in thickness from 3 to 100 mm. It is made up of a wide variety of cells with different roles, such as hair follicles, connective tissue, vascular tissue, a network of lymphatic capillaries, sweat and sebum glands, and macrophages. The cutaneous blood
Fig: 5 Dermis layer
4. Hypodermis:
The loose connective tissue that lies beneath the dermis is called the hypodermis or subcutis. This layer, which mostly contains adipocytes, helps to store fat, regulate body temperature in cold weather, and act as a cushion against external shocks. It may include sensory pressure organs and acts as a conduit for principal blood vessels and nerves to reach the skin. In addition, the dermis and epidermis are supported by the hypodermis, or subcutaneous fat tissue. (4)
Fig :6 Hypodermis Layer
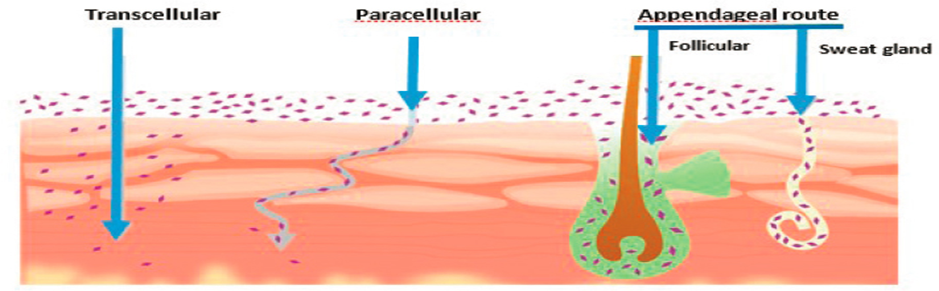
Structure of Skin and Permeation Pathways:
Transcellular route (through cells)
Intercellular route (between cells)
Appendageal route (via sweat glands and hair follicles) (8)
Components of TDDS :
Backing membrane: Protects the system from the external environment
Release liner: Removed before application
Adhesive layer: Keeps the patch attached to the skin
Drug reservoir: Contains the active pharmaceutical ingredient
Permeation enhancers: Improve skin penetration of drugs (8)
Advantages of TDDS :
Hepatic first pass metabolism, salivary metabolism, and intestinal metabolism are avoided.
Adverse effects are minimized due to a steady and optimum blood concentration time profile.(1)
Transdermal drug delivery enables the avoidance of gastrointestinal absorption with its associated pitfalls of enzymatic and pH-associated deactivation.(9)
Provide utilization of drugs with short biological half-lives and a narrow therapeutic window.
Lowers drug concentration, improving bioavailability.
Enables the permeation of both lipophilic and hydrophilic drugs. (15)
Drug therapy may be terminated rapidly by removal of the application from the surface of the skin.
Allows rapid termination of drug therapy by removing the skin application. (8)
Disadvantages of TDDS :
Cutaneous metabolism can affect the medication’s efficacy.
A transdermal drug delivery system cannot deliver ionic drugs.
Sufficient aqueous and lipid solubility, a log P (octanol/ water) between 1 and 3 is required for permeate to transverse the stratum corneum and underlying aqueous layer.(9)
Sufficient aqueous and lipid solubility, a log P (octanol/ water) between 1 and 3 is required for permeate to transverse the stratum corneum and underlying aqueous layer.
It can be used only for chronic conditions where drug therapy is desired for a long period of time, including hypertension, angina, and diabetes.(10)
The drug, the adhesive, or other excipients in the patch formulation can cause erythema, itching, and local edema.
Some drugs, e.g., scopolamine transdermal patch placed behind the ear, it is uncomfortable.(12)
Limitations of TDDS :
Limited to potent drugs due to dose constraints
The drug may undergo degradation in the skin
Highly soluble Drugs cannot be given by this route due to their low solubility in both water and fat
TDDS cannot deliver drugs in a pulsatile fashion
TDDS cannot develop if the drug or formulation irritates the skin
Limitations of TDDS can be overcome to some extent by novel approaches such as Iontophoresis, electroporation, and ultrasound (6,18,14)
Routes of Penetration :
Fig :7 Routes of Penetration
Transcellular route :
Hydrophilic medications can flow across the aqueous environment created by corneal cells' highly hydrated keratin.
Drugs entering the skin via the transcellular route pass through the corneocytes.
The transcellular pathway requires not only partitioning into and diffusion through the keratin bricks but also into and across the intercellular lipids.
Using the transcellular method, medications enter the systemic circulation by going straight through the stratum corneum's corneocytes, which are keratinized dead cells.
Intercellular route:
The intercellular route involves drug diffusion through the continuous lipid matrix.
Two factors make this path a major challenge: (i) Referring back to the "bricks and mortar" paradigm of SC, the corneocytes' interdigitating nature produces a
Convoluted route for drug penetration between cells, as opposed to the transcellular route's comparatively straightforward trajectory.
The region of alternating structured bilayers is known as the intercellular domain. A medication must therefore successively partition into and permeate through a number of lipid and aqueous domains.
The appendageal route :
The trans appendageal routes, sometimes referred to as the shunt routes, involve penetration through the sebaceous glands that are connected to the sweat glands and the hair follicles.
Recent studies have re-examined the long-held assumption that the follicles occupy approximately 0.1% of the surface area of the human skin
Skin appendages provide a continuous channel directly across the SC barrier
demonstrated that when it comes to drug administration through these appendages, the follicular number, opening diameter, and follicular volume are crucial factors. (4,13)
TRANSDERMAL PATCH :
A transdermal patch is a sheet-like device that sticks to the skin and is filled with medication molecules. This allows the drug to diffuse into the bloodstream through the skin and have therapeutic effects all over the body.(5,13)
Fig : 8 Transdermal Patches
It is a medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the bloodstream in a controlled manner to show therapeutic effect. (8,19)
Components of transdermal patches:
Polymer Matrix: The polymer controls the release of the drug from the device. The following criteria should be satisfied for a polymer to be used in transdermal patches.
Molecular weight, chemical functionality of the polymer should be such that the specific drug diffuses properly and gets released through it
The polymer should be stable.
The polymer should be inexpensive
Large amounts of the active agent are incorporated into it.(8)
The medication is included directly in the skin-contacting adhesive, which sets it apart.
In this form, the medicine is present in the sticky layer. The adhesive layer is in charge of delivering the medication onto the skin in addition to holding the several layers together. A backing and a temporary liner encircle the adhesive layer.
The adhesive in this transdermal system design acts as the formulation foundation, holding the medication and all of the excipients under a single backing film, in addition to attaching the system to the skin.
The rate at which the medication diffuses through the skin affects the medication release rate of this kind of system.
The medication is also included in this system's sticky layer. In this kind of patch, the adhesive layer is in charge of both releasing the medication and holding the numerous layers and the complete system to the skin together.
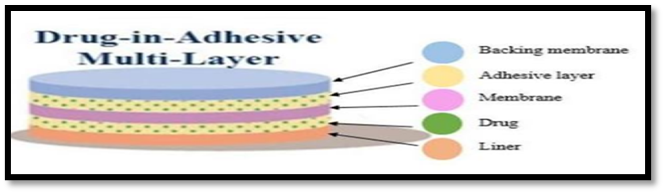
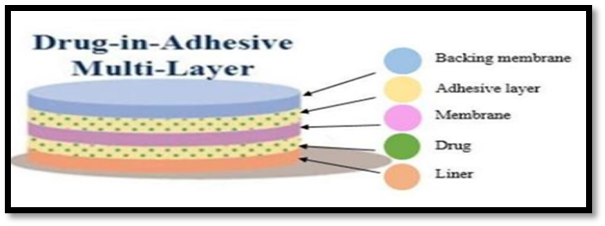
Multi-layer drug-in-adhesive :
Fig :10 Multi-layer drug-in-adhesive
Since the medication is integrated straight into the adhesive, it is comparable to the single-layer drug-in-adhesive.
The phrase "multi-layer" describes the addition of a membrane or several drug-in-adhesive layers sandwiched between two distinct drug-in-adhesive layers beneath a single backing film.
This kind is comparable to the single layer as well, but it has an immediate medication release layer in addition to an adhesive layer with a regulated release.
The medicine is released due to the action of the sticky layer. Additionally, this patch features a permanent backing and a temporary liner layer
These multilayer patches offer a practical way for sustained drug release and are used in hormone therapy, pain management, and smoking cessation.
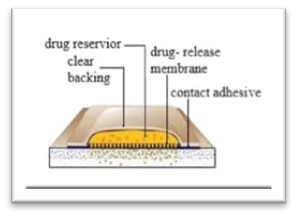
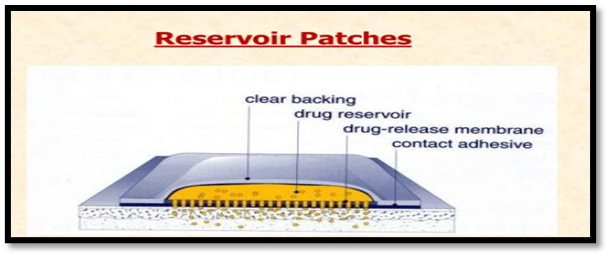
Reservoir Patch :
Fig :11 Reservoir Patch
This technique embeds the drug reservoir between a rate-controlling membrane and an impervious backing layer.
The drug is released only through the rate-controlling membrane, which can be micro-porous or non-porous. In the drug reservoir compartment, the drug can be in the form of a solution, suspension, gel, or dispersed in a solid polymer matrix.
A drug solution or suspension is separated by the adhesive layer. This patch is also backed by the backing layer.
It is distinguished by the presence of a liquid compartment with a drug suspension or solution that is kept apart from the release liner by an adhesive and semi-permeable membrane.
The product's adhesive ingredient that promotes skin attachment can be incorporated into a concentric design around the membrane or in a continuous layer between the membrane and the release liner.
Continuous layer between the membrane and the release liner or in a concentric configuration around the membrane.
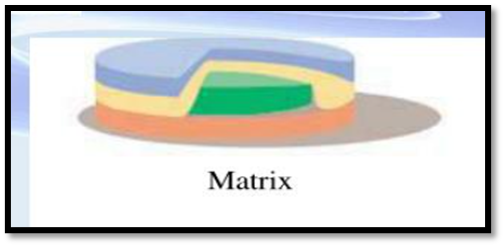
Matrix patch :
Fig :12 Matrix patch
The drug layer of the matrix system is a semi-solid matrix that contains a drug suspension or solution. In this patch, the medication layer is partially covered by the adhesive layer.
Numerous other kinds of vape patches on the market are intended to enhance sleep quality and lessen the effects of cigarette smoking.
It is characterized by the inclusion of a semisolid matrix containing a drug solution or suspension, which is in direct contact with the release liner
The adhesive layer of this patch partially surrounds the drug layer. Notably, this particular transdermal type lacks a membrane
The Matrix system has a drug layer of a semisolid matrix containing a drug solution or suspension. The adhesive layer in this patch surrounds the drug layer, partially overlaying it
A) Drug-in-adhesive system: This kind creates a drug reservoir by dispersing the medication in an adhesive polymer, which is then applied to an impermeable backing layer by solvent casting or melting (for hot-melt adhesives).
B) Matrix-dispersion system: In a compartment made of a drug-impermeable backing layer, this drug-containing polymer disk is fixed to an occlusive base plate. The adhesive is applied around the perimeter of the drug reservoir to create an adhesive rim strip rather than on the front of the reservoir.
Vapour patch :
Fig :13 vapour Patch
In this type of patch the adhesive layer not only serves to adhere the various layers together but also to release vapour
Other controller vapour patches that enhance sleep quality are available on the market. There are also vapour patches on the market that lower the number of cigarettes a person smokes in a given month.
The adhesive layer in this kind of patch releases vapor in addition to holding the different layers together.
The essential oils are released by the recently released vapor patches for a maximum of six hours. Vapour patches, which may release essential oils for up to six hours, are just beginning to be introduced to the market. Essential oils are released by the vapor patches, which are mostly used to treat decongestion cases.
Alternatives include controller vapour patches, which improve the quality of sleep. Additionally, there are vapour patches available.
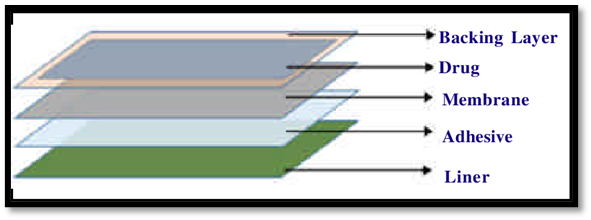
Components of a transdermal patch :
Liner: Protects the patch during storage. The liner should be removed before its use
Drug: Drug solution is in direct contact with the release liner.
Adhesive: It serves to both stick the patch to the skin and hold its constituent parts together. For instance, silicone, acrylic, and polyisobutylene (PIB) are adhesives with numerous pharmacological uses.
Membrane- It controls the release of the drug from the reservoir and multi-layer patches.
Backing- The film protects the patch from the outer environment
Pouching Material: The pouching material should be inert and should maintain the stability and integrity of the product. When there are two films with similar desired characteristics, the one with the lower cost, better function and printability will be chosen.
Heat Sealable Layer: This layer play an important role in the functionality, stability and protection of the patch. Several plastic films or coatings can be used for its formation, including polyethylene.(8)
Various methods for preparation of TDDS :
Asymmetric TPX membrane method : A heat-sealable polyester material with a concave 1 cm diameter can be utilized to create a prototype patch, which will serve as the backing membrane. The TPX {poly- (4-methyl-1-pentene)} asymmetric membrane is placed over the drug sample, which is then distributed into a concave membrane and sealed with an adhesive.
Circular Teflon mould method: In an organic solvent, solutions with different ratios of polymers are employed. Half as much of the same organic solvent is used to dissolve the calculate amount of medication The other half of the organic solvent is used to dissolve enhancers at varying quantities before they are applied.
Mercury substrate method: This approach involves dissolving the medication and plasticizer is a polymer solution After stirring the aforementioned solution for ten to fifteen minutes to create a uniform dispersion, it should be placed onto a flat mercury surface and covered with an inverted funnel to regulate solvent evaporation.
“IPM membranes” method: Using a magnetic stirrer, the medication is dissolved in a solution of water and propylene glycol that contains the carbomer 940 polymer and swirled for 12 hours. Triethanolamine is added to the dispersion to neutralize it and make it viscous If the drug's solubility in aqueous solution is extremely low, solution gel can be made using buffer pH 7.4.
“EVAC membranes” method: Polyethylene (PE), ethylene vinyl acetate copolymer (EVAC) membranes, and 1% carbopol reservoir gel can all be utilized as rate control membranes to produce the intended transdermal therapeutic system. Gel is made with propylene glycol if the medication is insoluble in water. Propylene glycol is used to dissolve the drug. (8)
Physicochemical evaluation of transdermal patch:
Thickness:
A digital micrometer is used to measure the thickness of the drug-prepared transdermal patch at several locations. The average thickness and standard deviation are then calculated to guarantee the patch's thickness.(9)
Weight Uniformity:
Weight variation is studied by individually weighing 10 randomly selected patches and calculating the average weight. Individual weight should not deviate significantly from average weight. (1)
Drug content determination:
Drug content is important for determination of percent content of drug product. Accurate quantity of drug material is weighed and added into the 100 ml of suitable solvent. Mixture of solvent is shacked continuously for 24 h in shaker incubator. The complete mixture of drug containing specific dilutions (11)
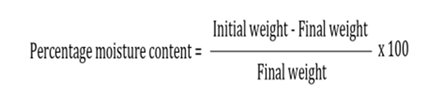
Percent Moisture content:
Prepared films are weighed individually and kept in desiccators containing calcium chloride at room temperature for 24 h. The films are weighed again after a specified interval until they show a constant weight. Percentage moisture content is calculated using following formula.
Flatness:
Three longitudinal strips are cut from different portions of the films. Length of each strip is measured and variation in length because of non-uniformity in flatness
Percentage moisture uptake:
Weighed films are kept in a desiccator containing saturated solution of potassium chloride in order to maintain 84% RH. After 24 h, reweigh patch and determine the percentage moisture uptake from the below mentioned formula:
Tensile strength:
To determine tensile strength, a modified pulley system was used. It has two clamps: a stationary clamp and a moveable clamp. A 2x2 cm2 patch strip was cut and sandwiched between two clams. To raise the pulling force until the patch broke, the weight on the pan was progressively increased. Tensile strength (kg/cm2) was defined as the force needed to break the film. The following formula was used to calculate the tensile strength. Tensile strength = F/a x b (l+L/l) (14)
Flux and Permeability coefficient:
Flux (mg cm-2 hr-1) of meclizine HCl was calculated from slope of plot of cumulative amount of meclizine HCl permeated per cm2 of skin at steady state against time using linear regression analysis. steady state permeability coefficient (Kp) of drug through rat epidermis was calculated by using following equation.
Tack properties:
It is the ability of the polymer to adhere to substrate with little contact pressure. Tack is dependent on molecular weight and composition of polymer as well as on the use of tackifying resins in polymer. (13)
Thumb tack test:
The force required to remove thumb from adhesive is a measure of tack. Rolling ball test: This test involves measurement of the distance that stainless steel ball travels along an upward facing adhesive. The less tacky the adhesive, the further the ball will travel.
Quick stick (Peel tack) test:
The peel force required breaking the bond between an adhesive and substrate is measured by pulling the tape away from the substrate at 90? at the speed of 12 inch/min. Probe tack test: Force required to pull a probe away from an adhesive at a fixed rate is recorded as tack.
In vitro drug release studies :
The drug release from the produced patches can be evaluated using the paddle over disc method (USP equipment V). Dry films having a given thickness must be cut into a specific form, weighed, and adhered to a glass plate. After that, the apparatus was adjusted to 32 ± 0.5°C and the glass plate was submerged in 500 mL of the phosphate buffer or dissolving media (pH 7.4). After that, the paddle was positioned 2.5 cm away from the glass plate and ran at 50 rpm.
In vitro skin permeation studies :
Diffusion cells can be used to conduct in vitro permeation research. We chose male Wistar rats weighing 200–250 g with full-thickness abdomen skin. Before beginning the experiment, the dermal side of the skin was thoroughly cleaned with distilled water to remove any adhering tissues or blood vessels, allowed to equilibrate for one hour in dissolution medium or phosphate buffer pH 7.4, and then placed on a magnetic stirrer with a small magnetic needle to ensure uniform dispersion of the diffusant. Carefully remove any hair from the abdominal region using an electric clipper. (17)
Factors affecting transdermal patches :
Hydration of Skin :
Hydration leads to stratum corneum swelling, providing fluidity to the skin. This increased hydration enhances permeant solubility and partitioning, facilitating drug molecule permeation
Skin Temperature :
Elevated skin temperature increases percutaneous drug absorption by fluidizing lipids and dilating blood vessels, which elevates blood flow and enhances drug absorption
Skin Age :
Skin permeability is assumed to be higher in younger and elderly individuals compared to middle-aged individuals. Premature infants lack a stratum corneum, making children more susceptible to drug effects via the skin.
Blood flow
Changes in peripheral circulation influence transdermal absorption. Increased blood flow alters the concentration gradient across the skin, reducing the residence time of drug molecules in the dermis
Pathology of the Skin :
Skin diseases or injuries alter skin penetration by disrupting lipid layers in the stratum corneum. Pathogens and injuries can rupture skin layers, changing skin integrity
Regional Site of Skin :
Variations in anatomical features such as stratum corneum thickness, hair follicles, and sweat gland density per unit area result in differing percutaneous absorption rates
Skin Flora and Enzymes :
The skin hosts metabolizing enzymes and microbes that metabolize drugs passing through the skin. Most drugs undergo varying degrees of metabolism in the skin before reaching the circulation. For example, about 95% of absorbed testosterone gets metabolized in the skin. (13,15)
CONCLUSION :
Transdermal drug delivery systems represent a beneficial innovation for drug delivery, particularly in patients who cannot swallow or remember to take their medications. Transdermal drug delivery offers controlled release of the drug into the patient, it enables a steady blood level profile, resulting in reduced systemic side effect and sometimes, and improved efficacy over other dosage form. It offer the delivery of drug at lowered dose that can save the recipient from the harm of large doses with improved bioavailability. Transdermal patches have become a proven technology that offers variety of significant clinical benefits over other dosage form. (7,10)
The transdermal drug delivery system (TDDS) review articles offer useful insights on the transdermal drug delivery systems and its evaluation procedure as a handy reference for the research scientist working on TDDS. The information above demonstrates that TDDS have significant potentials, since they can be used to create promising deliverable medications from both hydrophobic and hydrophilic active substances. More knowledge of the various biological interactions and polymer mechanisms is needed to optimise this drug delivery technology. The next generation of drug delivery systems, TDDS, has a realistic, practical use. (3,19)
Transdermal drug delivery system is a non-invasive delivery approach that is generally regarded as being easy to administer even in more vulnerable age groups, such as paediatric and geriatric patients, whilst circumventing some bioavailability concerns that arise from oral drug delivery due to poor absorbability and metabolism concerns.(22)
Even with this remarkable expansion, there are still significant obstacles that limit the use of TDD to a small number of medications. Few medications that use chemical TDD techniques have been successfully brought to market. Chemical TDD systems like niosomes and nanocrystals are not the ultimate dosage forms and must be transformed into an appropriate dosage form (such as patches, creams, gels, etc.) before being used; this may be the manufacturing complexity of chemical TDD systems that is impeding commercialization.(22)
REFERENCES
Patel, A. and Shah, B. (2018). TRANSDERMAL DRUG DELIVERY SYSTEM: A REVIEW.pp-378-390
Shingade, G.M., Aamer, Q., Sabale, P.M., Grampurohit, N.D., Gadhave, M.V., Jadhav, S.L. and Gaikwad, D.D., 2012. Review on: recent trend on transdermal drug delivery system. J. Drug Deliv. Ther, 2(1), pp.66-75.
Brown, M.B., Martin, G.P., Jones, S.A. and Akomeah, F.K., 2006. Dermal and transdermal drug delivery systems: current and future prospects. Drug delivery, 13(3), pp.175-187.
Gaikwad, A.K., 2013. Transdermal drug delivery system: Formulation aspects and evaluation. Compr J Pharm Sci, 1(1), pp.1-10.
Arunachalam, A., Karthikeyan, M., Vinay Kumar, D., Sethuraman, S., Ashutoshkumar, S. and Manidipa, S. (2010). Transdermal Drug Delivery System: A Review. Current Pharma Research.pp-70-81
Purushotham, K. and Vijetha, K.A., 2023. A review on transdermal drug delivery system. GSC Biological and Pharmaceutical Sciences, 22(2), pp.245-255.
Ashutoshkumar, S. and Manidipa, S., 2010. Transdermal drug delivery system: a review. Journal of Current Pharma Research, 1(1), p.70.
Mali, A.D., 2015. An updated review on transdermal drug delivery systems. skin, 8(9), pp.244-254.
Deulkar, D.A., Kubde, J.A., Hatwar, P.R. and Bakal, R.L., 2024. A review on transdermal drug delivery system. GSC Advanced Research and Reviews, 18(2), pp.347-361.
Upadhyay, G., Verma, S., Parvez, N. and Sharma, P.K., 2014. Recent trends in transdermal drug delivery system-a review. Adv Biol Res, 8(3), pp.131-8.
Nikam, N.M. and Nikam, D.N., 2021. Journal Of Pharmacy And Experimental Medicine
Rajaram, Sonawane Vivek, et al. “Transdermal Drug Delivery System.” INTERNATIONAL JOURNAL of NOVEL RESEARCH and DEVELOPMENT, vol. 8, no. 12, Dec. 2023, pp. c278–c284c278–c284
Rastogi, V. and Yadav, P., 2012. Transdermal drug delivery system: An overview. Asian Journal of Pharmaceutics (AJP), 6(3).
Dipen Patel*, Sunita A. Chaudhary, Bhavesh Parmar, Nikunj Bhura. Transdermal Drug Delivery System: A Review. Pharma Innovation 2012;1(4):66-75.
Tanwar, H. and Sachdeva, R., 2016. Transdermal drug delivery system: A review. International journal of pharmaceutical sciences and research, 7(6), p.2274.
Karthikeyan, E. and Sivaneswari, S., 2024. Advancements in transdermal drug delivery systems: enhancing medicine with pain-free and controlled drug release. Intelligent Pharmacy.
Ramteke, K.H., Dhole, S.N. and Patil, S.V., 2012. Transdermal drug delivery system: a review. Journal of Advanced Scientific Research, 3(01), pp.22-35.
Patel, D. and Kavitha, K., 2011. Formulation and evaluation aspects of transdermal drug delivery system. J Pharm Sci, 6, pp.1-12.
Ashok Kumar, J., Pullakandam, N., Lakshmana Prabu, S. and Gopal, V. (2010). TRANSDERMAL DRUG DELIVERY SYSTEM: AN OVERVIEW. International Journal of Pharmaceutical Sciences Review and Research,pp-49-54
Shinde, S. (2024). A REVIEW ON TRANSDERMAL DRUG DELIVERY SYSTEM. [online] 12(1), pp.2320–2882
Aman, et al. “Transdermal Drug Delivery System: A Comprehensive Review.” IJCRT - International Journal of Creative Research Thoughts (IJCRT), vol. 13, no. 5, May 2025, pp. q262–q264q262–q264, Accessed 3 Nov. 2025
Alkilani, A.Z., Nasereddin, J., Hamed, R., Nimrawi, S., Hussein, G., Abo-Zour, H. and Donnelly, R.F., 2022. Beneath the skin: a review of current trends and future prospects of transdermal drug delivery systems. Pharmaceutics, 14(6), p.1152.
Reference
Patel, A. and Shah, B. (2018). TRANSDERMAL DRUG DELIVERY SYSTEM: A REVIEW.pp-378-390
Shingade, G.M., Aamer, Q., Sabale, P.M., Grampurohit, N.D., Gadhave, M.V., Jadhav, S.L. and Gaikwad, D.D., 2012. Review on: recent trend on transdermal drug delivery system. J. Drug Deliv. Ther, 2(1), pp.66-75.
Brown, M.B., Martin, G.P., Jones, S.A. and Akomeah, F.K., 2006. Dermal and transdermal drug delivery systems: current and future prospects. Drug delivery, 13(3), pp.175-187.
Gaikwad, A.K., 2013. Transdermal drug delivery system: Formulation aspects and evaluation. Compr J Pharm Sci, 1(1), pp.1-10.
Arunachalam, A., Karthikeyan, M., Vinay Kumar, D., Sethuraman, S., Ashutoshkumar, S. and Manidipa, S. (2010). Transdermal Drug Delivery System: A Review. Current Pharma Research.pp-70-81
Purushotham, K. and Vijetha, K.A., 2023. A review on transdermal drug delivery system. GSC Biological and Pharmaceutical Sciences, 22(2), pp.245-255.
Ashutoshkumar, S. and Manidipa, S., 2010. Transdermal drug delivery system: a review. Journal of Current Pharma Research, 1(1), p.70.
Mali, A.D., 2015. An updated review on transdermal drug delivery systems. skin, 8(9), pp.244-254.
Deulkar, D.A., Kubde, J.A., Hatwar, P.R. and Bakal, R.L., 2024. A review on transdermal drug delivery system. GSC Advanced Research and Reviews, 18(2), pp.347-361.
Upadhyay, G., Verma, S., Parvez, N. and Sharma, P.K., 2014. Recent trends in transdermal drug delivery system-a review. Adv Biol Res, 8(3), pp.131-8.
Nikam, N.M. and Nikam, D.N., 2021. Journal Of Pharmacy And Experimental Medicine
Rajaram, Sonawane Vivek, et al. “Transdermal Drug Delivery System.” INTERNATIONAL JOURNAL of NOVEL RESEARCH and DEVELOPMENT, vol. 8, no. 12, Dec. 2023, pp. c278–c284c278–c284
Rastogi, V. and Yadav, P., 2012. Transdermal drug delivery system: An overview. Asian Journal of Pharmaceutics (AJP), 6(3).
Dipen Patel*, Sunita A. Chaudhary, Bhavesh Parmar, Nikunj Bhura. Transdermal Drug Delivery System: A Review. Pharma Innovation 2012;1(4):66-75.
Tanwar, H. and Sachdeva, R., 2016. Transdermal drug delivery system: A review. International journal of pharmaceutical sciences and research, 7(6), p.2274.
Karthikeyan, E. and Sivaneswari, S., 2024. Advancements in transdermal drug delivery systems: enhancing medicine with pain-free and controlled drug release. Intelligent Pharmacy.
Ramteke, K.H., Dhole, S.N. and Patil, S.V., 2012. Transdermal drug delivery system: a review. Journal of Advanced Scientific Research, 3(01), pp.22-35.
Patel, D. and Kavitha, K., 2011. Formulation and evaluation aspects of transdermal drug delivery system. J Pharm Sci, 6, pp.1-12.
Ashok Kumar, J., Pullakandam, N., Lakshmana Prabu, S. and Gopal, V. (2010). TRANSDERMAL DRUG DELIVERY SYSTEM: AN OVERVIEW. International Journal of Pharmaceutical Sciences Review and Research,pp-49-54
Shinde, S. (2024). A REVIEW ON TRANSDERMAL DRUG DELIVERY SYSTEM. [online] 12(1), pp.2320–2882
Aman, et al. “Transdermal Drug Delivery System: A Comprehensive Review.” IJCRT - International Journal of Creative Research Thoughts (IJCRT), vol. 13, no. 5, May 2025, pp. q262–q264q262–q264, Accessed 3 Nov. 2025
Alkilani, A.Z., Nasereddin, J., Hamed, R., Nimrawi, S., Hussein, G., Abo-Zour, H. and Donnelly, R.F., 2022. Beneath the skin: a review of current trends and future prospects of transdermal drug delivery systems. Pharmaceutics, 14(6), p.1152.
Chetan Mali
Corresponding author
Jes's College of Pharmacy, Waghoda Road, Nandurbar 425412
Jes's College of Pharmacy, Waghoda Road, Nandurbar 425412
Jayshree Naik
Co-author
Jes's College of Pharmacy, Waghoda Road, Nandurbar 425412
R. R. Patil
Co-author
Jes's College of Pharmacy, Waghoda Road, Nandurbar 425412
Chetan Mali, Nitin Mali, Srushti Mali, Jayshree Naik, R. R. Patil, Recent Trends on Transdermal Drug Delivery System, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 549-562. https://doi.org/10.5281/zenodo.18165837




 10.5281/zenodo.18165837
10.5281/zenodo.18165837
