
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Krishnarao Bhegade Institute of Pharmaceutical Education and Research, Talegaon Dabhade 410407.
Nasal spray could be a promising approach to preventing respiratory tract infection. This study explored lay people’s perceptions and experiences of using nasal sprays to prevent RTI’s to identify barriers and facilitators to their adoption and continued use. Nasal spray is the most common dosage form for intranasal drug delivery system to ease of administration and efficient nasal deposition compared to drop installation . With the nozzle of a spray bottle inserted into nostril, liquid dosage forms ( including solution , suspensions and emulsions) are atomized into fine droplets for nasal deposition. Its aims to inspire scientist to develop new delivery system to provide effective symptoms management for this group of patient. The intranasal delivery is preferable route for administration of the drug for local, systemic as well as central nervous system drug delivery. Advantages of nasal spray dosage form such as it is cost-effective, easy to use/carry and self-administrable, it has high patient compliance make this dosage form growing opportunity for nasal drug delivery. This article outlined the relevant aspects of nasal anatomy, physiology and histology, and the biological, physicochemical and pharmaceutical factors that must be considered during the formulation development of nasal spray. It is intuitively expected that this review will help to understand nasal formulation and it’s in- vitro characteristics.[1].
Nasal spray is defined as a medicament that consist of therapeutically active substance dissolved or suspended in a mixture of additives or solution, delivered through non-pressurized dispenser providing a metered dosage of active substance. Intranasal drug delivery is recognized to be a useful and reliable alternative to oral and parenteral routes. The nasal route of drug delivery can be used for both local and systemic drug delivery. For instance, localized nasal drug delivery is usually used to treat conditions related to the nasal cavity, such as congestion, rhinitis, sinusitis and related allergic conditions. A diverse range of drugs including corticosteroids, anti-histamines, anti-cholinergic and vasoconstrictors can be administered locally. In recent years, achieving a systemic drug action using the nose as the entry portal into the body has received more attention. Also, the nasal delivery seems to be a favorable way to circumvent the obstacles for blood- brain barrier (BBB) allowing the direct drug delivery in the biophase of central nervous system (CNS)-active compounds. It has also been considered to the administration of vaccine .

In recent time, the nasal drug delivery received a great deal of attention for its convenient, promising, and reliable way of systemic administration for drugs, especially for those drugs which are ineffective orally and those which must be administered by injections. This route provides a large surface area, porous endothelial membrane, high total blood flow, bypassing the first-pass metabolism, and ready accessibility. Furthermore, nasal mucosa is permeable to more compounds than the gastrointestinal tract due to the absence of pancreatic, gastric enzymatic activities, and interference by gastrointestinal contents. The early recorded historical application of nasal drug delivery was restricted to topical applications of drugs intended for only local effects. However in recent times, its application grown to include a wide range of targeted areas in the body to produce local and systemic effects. Nasal drug delivery also finds a special place in the traditional system of medicine such as the Ayurvedic system of Indian medicine which is called as “Nasya karma” and is a well- recognized way of treatment .In therapeutics, nose forms an important part of the body for faster and higher level of drug absorption with the possibility of self-administration. Drugs are ranging from small micromolecules to large macromolecules such as peptide/proteins, hormones, and vaccines, are being delivered through the nasal cavity. It is reported that lipophilic drugs are generally well absorbed from the nasal cavity with pharmacokinetic profiles often identical to those obtained following an intravenous injection with a bioavailability approaching up to 100% in many cases. Large absorption surface area and high vascularization lead to fast absorption. In emergency, nasal route can be used as a substitute route of parenteral administration . Drugs are rapidly absorbed from the nasal cavity after intranasal administration, resulting in rapid systemic drug absorption. An approach if made for increasing the residence time of drug formulations in the nasal cavity can result in improved nasal drug absorption. Depending on the desired site of drug action, the drug to be inhaled needs to be adjusted to particle size, concentration, and chemical form to ensure a local or systemic drug action .[2],[3],[4],[5].
Anatomy And Physiology of Nose:
Nasal depression is lined with mucus and hairs which are involved in those functions, gobbled patches and pathogens. Also resonance of produced sounds mucus MMC [immunological conditioning and metabolism of endogenous substances are also essential functions of nasal structures. The mortal nasal depression has a total volume of 15- 20 mL and a total face area of roughly 150 cm2 The nasal halves correspond of four areas( nasal entranceway, patio, respiratory region and olfactory region) that are distinguished according to their anatomic and histological characteristics.
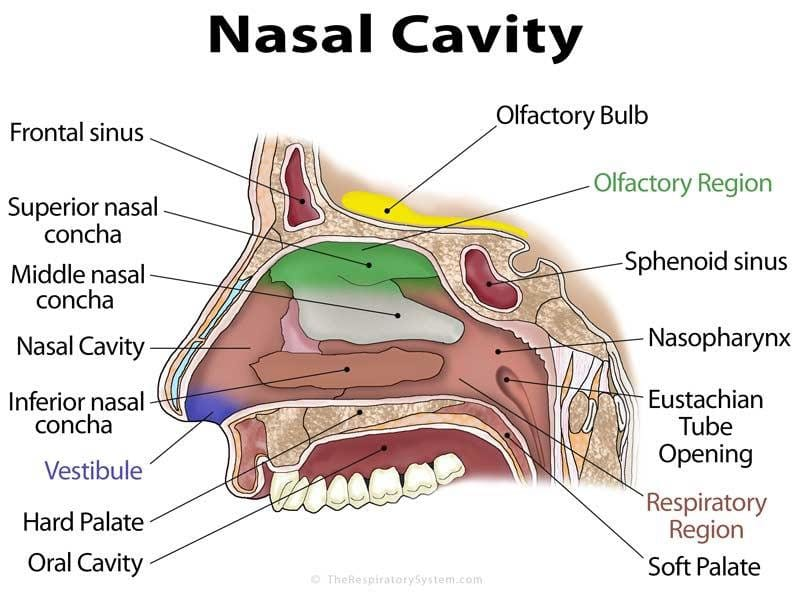
1) Nasal vestibule
In this area of nasal depression, there are nasal hairs, also called vibrissae, which filter the gobbled patches. Nasal vestibular characteristics are desirable to go high resistance again poisonous environmental substances.
2) Atrium
Between the nasal vestibule and the respiratory region, there is an atrium. A stratified squamous epithelium makes up its anterior part, and the by pseudo stratified columnar cells in the posterior region showing off microvilli.
3) Respiratory region
Divided into upper, middle and lower nasal turbinate protruding from the sidewall. These special structures are Humidification and temperature control of the inhaler air. Between them there is a space called a way these are the passages through which the air flow is created Ensure intimate contact with inhaled air the mucosal surface of the respiratory tract lower and middle . The tract receives the nasolacrimal ducts and sinuses these are air-filled pockets inside the bone around the face and nasal cavities. Nose the most important airway mucosa Sections are formed for systemic delivery of drugs via epithelium, basement membrane, and lamina exclusive use Nasal discharge is essential for many people Physiological functions.
4) Olfactory region
The olfactory region is located on the roof of the Extends a short distance under the nasal cavity and nasal septum and side walls. Its epithelium is the only part central nervous system directly exposed to the outside world Surroundings. Similar to respiratory epithelium, the sense of smell is also pseudo stratified, but included Special olfactory receptor cells important for odors Perception.[10,11].
Advantages of Nasal Drug Delivery System :
1. Intranasal administration offers several practical advantages from the viewpoint of patients (non-invasiveness, essentially painless, ease drug delivery and favorable tolerability profile)
2. Rapid drug absorption.
3. Quick onset of action.
4. Hepatic first – pass metabolism is absent.
5. The bioavailability of larger drug molecules can be improved by means of absorption enhancer or other approach.
6. Better nasal bioavailability for smaller drug molecules
Limitations:
1. Dose is limited because of relatively small area available for the absorption of drug.
2. Time available for drug absorption is limited.
3. Diseased condition of nose impairs drug absorption.
4. The absorption enhancers used to improve nasal drug delivery system may have histological toxicity which is not yet clearly established.
5. Absorption surface area is less when compared to GIT.
6. Nasal irritation
7. Certain surfactants used as chemical enhancers may disrupt and even dissolve Membrane in high concentration.[13].
Oxymetazoline:
Brand name : Afri

The product is indicated for symptomatic relief of nasal congestion due to hay fever ,common cold and sinusitis .
Oxymetazoline HCL is a sympathomimetic agent which exerts a local vasoconstriction action in nasal mucosa reducing nasal congestion . Afrin nasal spray is described as No-Drip formulation because it becomes more viscous when spread and remains on mucosal membrane more effectively than a standard aqueaous solution clinical studies have shown than oxymetazoline acts within a few minutes and its effect may last upto 12 hours .
|
Sr No |
Ingredients |
Purpose |
|
01 |
Oxymetazoline HCL |
Active ingredient |
|
02 |
Benzalkonium chloride |
Preservative |
|
03 |
Disodium edetate |
Antioxidant |
|
04 |
Polyethylene glycol |
Viscosity modifier |
|
05 |
Povidone |
Viscosity modifier |
|
06 |
Propylene glycol |
Moisturizing agent |
|
07 |
Sodium phosphate |
Buffer |
|
08 |
Purified water |
Solvent |
Marketed Formulations:
|
Drug Substance [Product Name] |
Indication |
Dosage Form |
Status |
Manufacturer |
|
Salman calcitonin |
Osteoporosis |
Solution (spray) |
Marketed |
Novartis Pharma |
|
Desmoprassin |
Antidiuretic Hormone |
Solution (spray) |
Marketed |
Ferring Arzneimitted |
|
Buserelin |
Buserelin |
Solution(spray) |
Marketed |
Aventis Pharma |
|
Nafarelin |
Endometriosis |
Solution(spray) |
Marketed |
Pharmacia |
|
Oxytocin |
Lactation Induction |
Solution (spray) |
Marketed |
Novartis Pharma |
|
Zolemitriptan |
Migraina |
Solution (spray) |
Marketed |
Astra Zeneca |
|
Protirelin |
Thyroid Diagnostics |
Solution(spray) |
Marketed |
Aventis Pharma |
|
Estradiol |
Hormone Replacement |
Solution(spray) |
Marketed |
Servier |
Future needs and further research and development :
It is not surprising to find a lot of research focusing to develop nasal drug delivery system and its contribution in therapeutic management .In general, a concise overview of the pharmacotherapy of nasal drug delivery system has highlighted that in spite of the availability of new drugs and several specialized devices.[9]
CONCLUSION:
The nasal cavity has a large surface area and a highly vascularized mucosa. Drugs absorbed by the rich network of blood vessels pass directly into the systemic circulation, thereby avoiding the first-pass metabolism. Agrowing body of evidence relating to nasal drug delivery suggests it might use for challenging drugs which can facilitate the pharmaceutical manufacturing and drug delivery challenges. Considering the wealth of activity and interest in the area of nasal drug delivery, together with the potential benefits from this route of administration, we should expect to see a range of novel nasal products reaching the market shortly.
REFERENCES





Vaishnavi Rakshe, Sanika Asawale, Sanskruti Phule, Manasi Deshmukh, Review on Nasal Spray, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2451-2458 https://doi.org/10.5281/zenodo.17626974
 10.5281/zenodo.17626974
10.5281/zenodo.17626974