Department of Pharmaceutical Chemistry, Maharashtra Institute of Pharmacy (B. Pharm), Betala, Chandrapur, Maharashtra, India
Cardiometabolic disorders comprise a spectrum of interrelated conditions such as hypertension, type 2 diabetes mellitus, heart failure, coronary artery disease, obesity, and metabolic syndrome, which collectively contribute to increased global morbidity and mortality. The close association between cardiovascular and metabolic abnormalities necessitates integrated therapeutic strategies that address both components simultaneously. Bisoprolol, a highly selective ?1-adrenergic receptor blocker, is widely used in cardiovascular disorders due to its ability to reduce heart rate, myocardial contractility, and renin release with minimal metabolic adverse effects. Dapagliflozin, a sodium–glucose co-transporter-2 (SGLT2) inhibitor, initially developed as an antidiabetic agent, has demonstrated significant cardiovascular and renal protective benefits independent of glycemic control. This comprehensive review highlights the pharmacological profile, pharmacokinetics, pharmacodynamics, clinical applications, safety, drug interactions, and future perspectives of bisoprolol and dapagliflozin. Emphasis is placed on their complementary mechanisms of action and their combined role in the management of cardiometabolic disorders. The integration of these agents represents a rational and effective approach toward improving cardiovascular outcomes, metabolic control, and overall patient prognosis.
Cardiometabolic disorders are among the leading causes of global disease burden. The coexistence of cardiovascular diseases and metabolic abnormalities such as diabetes and dyslipidemia has necessitated integrated therapeutic approaches.[1]Hypertension and type 2 diabetes mellitus frequently coexist and synergistically increase the risk of heart failure and atherosclerotic cardiovascular disease. Advances in pharmacotherapy have shifted focus toward drugs offering pleiotropic benefits beyond primary indications.
Bisoprolol has long been used in cardiovascular disorders due to its cardioselective β1-blocking action, reducing heart rate and myocardial oxygen demand. Dapagliflozin, initially developed as an antidiabetic drug, has demonstrated remarkable cardiovascular and renal protective effects independent of glycemic control. The combination of these agents offers a holistic approach to cardiometabolic management.[2,3] In recent decades, the prevalence of cardiovascular diseases (CVDs) and metabolic disorders, particularly type 2 diabetes mellitus (T2DM), has increased dramatically across the globe. These conditions represent a major public health challenge due to their chronic nature, high treatment costs, and strong association with morbidity and mortality.[3] According to global health reports, cardiovascular diseases remain the leading cause of death worldwide, while diabetes mellitus is recognized as one of the fastest-growing metabolic disorders. The coexistence of these diseases in a single patient is increasingly common and is collectively referred to as cardiometabolic disorders.[4,5]
Bisoprolol Fumarate is a cardio-selective beta-adrenergic blocking agent commonly used in the treatment of hypertension, chronic heart failure, angina pectoris, and arrhythmias. It acts by selectively inhibiting β1-adrenergic receptors located primarily in cardiac tissue, resulting in a decrease in heart rate, myocardial contractility, and cardiac output. This leads to a reduction in blood pressure and myocardial oxygen demand, thereby improving cardiac efficiency and reducing the workload on the heart. Due to its high β1-selectivity, Bisoprolol exhibits minimal β2-receptor inhibition, which reduces the risk of bronchoconstriction and metabolic side effects, making it suitable for long-term therapy in patients with comorbid condition.[2,9]

Dapagliflozin is a newer class of oral antidiabetic drug belonging to the sodium–glucose co-transporter 2 (SGLT2) inhibitors. It exerts its glucose-lowering effect by selectively inhibiting SGLT2 in the proximal renal tubules, thereby preventing glucose reabsorption and promoting urinary glucose excretion.(6,7)This insulin-independent mechanism of action distinguishes dapagliflozin from conventional antidiabetic agents such as sulfonylureas and insulin, significantly reducing the risk of hypoglycemia.[8]
The complementary pharmacological actions of Bisoprolol Fumarate and Dapagliflozin make their combination particularly relevant for patients suffering from both cardiovascular and metabolic disorders. While Bisoprolol primarily modulates cardiac function by reducing sympathetic activity, dapagliflozin improves metabolic control and provides additional cardiovascular protection through hemodynamic and metabolic mechanisms. Therefore, the concurrent use of these drugs represents a rational and effective therapeutic approach in modern cardiometabolic management.[9] With the increasing use of combination therapies, ensuring the quality, safety, and stability of pharmaceutical products has become critically important. Regulatory authorities such as the International Council for Harmonisation (ICH) emphasize the need for comprehensive analytical evaluation of drug substances and drug products. Analytical techniques play a vital role in drug development, quality control, stability testing, and regulatory compliance.[10]
2. DRUG PROFILE OF BISOPROLOL
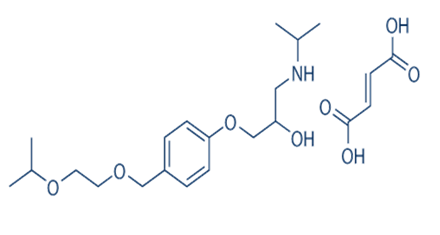
Chemical Structure: Synthetic β1-selective adrenergic blocker
IUPAC Name: (RS)-1-[4-[(2-isopropoxyethoxy) methyl]phenoxy]-3-(isopropylamino)propa-2-ol
Molecular Formula: C??H??NO?
Molecular Weight : 325.44 g/mol
Physical Properties:
Storage: Store below 25°C, protected from moisture, Keep in tightly closed container
Uses: Hypertension, chronic heart failure, angina pectoris, ischemic heart disease [12]
Dosage: Bisoprolol fumarate is administered orally as 5 or 10 mg tablets once daily.
Advantages in Cardiometabolic Disorders:
Adverse Effects: Bradycardia, hypotension, fatigue, dizziness [13,14]
3. DRUG PROFILE OF DAPAGLIFLOZIN
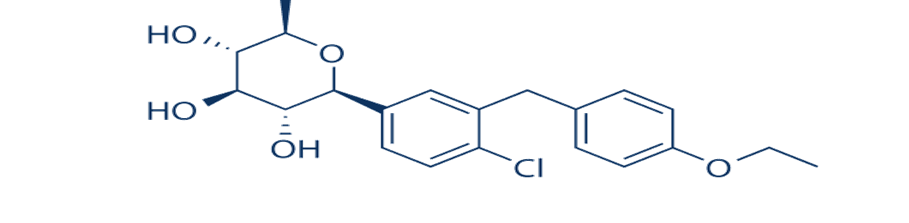
Chemical Structure: SGLT2 inhibitor derived from C-aryl glucoside
IUPAC Name: (2S,3R,4R,5S,6R)-2-[4-chloro-3-(4-ethoxybenzyl)phenyl]-6-(hydroxymethyl) tetrahydro-2H-pyran-3,4,5-triol
Molecular Formula: C??H??ClO?
Molecular Weight: 408.88 g/mol
Physical Properties:
Storage: Store at room temperature(20–25°C),Protect from excessive heat and moisture
Uses: Type 2 diabetes mellitus, heart failure, chronic kidney disease
Dosage: Taken once daily in the morning, with or without food 5 or 10 mg tablet.
Advantages in Cardiometabolic Disorders:
Adverse Effects: Genital infections, dehydration, hypotension [15,16]
4. PHARMACOLOGICAL ACTION
Bisoprolol selectively blocks β1-adrenergic receptors, reducing sympathetic stimulation of the heart.Selective B1 blocker drugs have negative inotropic and chronotropic effects; they decrease heart contractions and heart rate. As a net result, bisoprolol reduces the oxygen consumption of myocardial cells. B1 receptors are also present in the juxtaglomerular cells. By blocking these receptors, bisoprolol leads to a decrease in the release of renin; as a result, this decrease in renin blocks the activation of the renin-angiotensin system.[17]
B1 adrenergic receptors are present in cardiac myocyte cells and juxtaglomerular cells. They couple with the G-stimulatory protein receptor (Gs receptor) and become stimulated by either norepinephrine or circulating catecholamine. Activation of B1 receptors in cardiac myocytes leads to positive chronotropic and inotropic effects; therefore, the net result will be increased heart rate, contraction, and the strength of myocyte contraction by activating Gs receptors (by the exchange of GTP to GDP). Eventually, this activity increases intracellular calcium concentration and promotes heart cell contraction. [ 18,19,20 ] Activation of B1 receptors on juxtaglomerular cells leads to activating the renin-angiotensin system. Releasing renin increases the production of angiotensin I, which is eventually converted by an angiotensin-converting enzyme (ACE) to angiotensin II.
Dapagliflozin inhibits SGLT2 in the renal proximal tubules, promoting urinary glucose excretion. Dapagliflozin is a potent, highly selective reversible, orally active competitive sodium glucose co-transporter-2 (SGLT2) inhibitor with potency at nanomolar stage that effect in the maintenance of glycemic control in patients with type 2 diabetes mellitus by reducing renal glucose reabsorption leading to urinary glucose excretion (glycuresis)[21,22,23]
SGLT-2 is selectively expressed in the kidney with no expression detected in more than 70 other tissues including liver, skeletal muscle, adipose tissue, breast, bladder, and brain. SGLT-2 is the predominant transporter that causes the reabsorption of glucose from the glomerular filtrate back into the circulation. This does not affect the insulin secretion but continues to inhibit the reabsorption of filtered glucose.[21] Even by this inhibition, it causes maintenance. of both fasting and post-prandial plasma glucose levels, thus it results in the consumption of fat as an energy source. [24]But Glomerular Filtration Rate (GFR) and blood glucose concentration are the factors on which the amount of glucose removed by the kidney through this mechanism is depended. Thus, in healthy subjects with normal glucose, dapagliflozin has a low propensity to cause hypoglycemia. Dapagliflozin acts independently of insulin secretion and insulin action. Over time, improvement in beta cell function (HOMA-2) has been observed in clinical studies with dapagliflozin.[21]
5. PHARMACODYNAMICS
Bisoprolol decreases heart rate, myocardial contractility, and renin release. Bisoprolol is a β1-adrenoceptor antagonist which has been shown to be devoid of partial agonist or membrane-stabilising activity. Animal studies have shown that bisoprolol is a more potent antagonist of β1-adrenoceptors than atenolol or metoprolol, but the drug appears to be less potent than propranolol and betaxolol in this regard. Bisoprolol possesses a long duration of action, with significant reductions in exercise tachycardia (about 20%) being observed in subjects with stable angina pectoris 24 hours after oral administration of 5 and 10mg. Both systolic and diastolic blood pressures are reduced by bisoprolol (by up to about 20%, respectively, in healthy subjects and in patients with mild to moderate essential hypertension) as well as myocardial oxygen demand (by up to 34%).[25]
Statistically significant increases in serum triglycerides (p<0.05) and reductions in high density lipoprotein (HDL)-cholesterol (bisoprolol, p<0.01; atenolol, p<0.05) were reported in a 3-month comparison of oral bisoprolol 10 and 20 mg/day and atenolol 50 and 100 mg/day in patients with mild to moderate essential hypertension. However, the overall effects of bisoprolol on lipid metabolism are as yet still unclear and further studies in this area are required.[26]
Dapagliflozin reduces plasma glucose levels and improves cardiovascular outcomes through osmotic diuresis and reduced preload.Increases in the amount of glucose excreted in the urine were observed in healthy subjects and in patients with type 2 diabetes mellitus following the administration of dapagliflozin . Approximately 70 g of glucose was excreted in the urine per day (corresponding to 280 kcal/ day) at a Dapagliflozin dose of 10 mg/day in patients with type 2 diabetes mellitus for 12 weeks. This glucose elimination rate approached the maximum glucose excretion observed at 20 mg/day dose of dapagliflozin. Evidence of sustained glucose excretion was seen in patients with type 2 diabetes mellitus given dapagliflozin 10mg/day for up to 2 years. This urinary glucose excretion with dapagliflozin also results in osmotic diuresis and increases in urinary volume. Urinary volume increases in patients with type 2 diabetes mellitus treated with Dapagliflozin 10 mg were sustained at 12 weeks and amounted to approximately 375 ml/day. The increase in urinary volume was associated with a small and transient increase in urinary sodium excretion that was not associated with changes in serum sodium concentrations.[22]
6. PHARMACOKINETIC
Bisoprolol :- Absorption: Bisporolol is well absorbed, and the bioavailability of bisoprolol is approximately 80%. The time to peak plasma concentration is approximately 2 to 4 hours. Steady-state plasma concentration is achieved in 5 days.[28]
Distribution: Bisoprolol has low lipophilicity; penetration the through the blood-brain barrier is minimal. The volume of distribution of about 3.5 L/kg.[29]
Metabolism: Bisoprolol is primarily metabolized by the CYP3A4 and CYP2D6(minor). First-pass metabolism of bisoprolol is low.[30]
Excretion: Bisoprolol is eliminated by 50% renal excretion (unchanged drug) and 50% by hepatic metabolism to pharmacologically inactive metabolites excreted by the kidneys. Tubular secretion plays an important role in the renal elimination of bisoprolol. Excretion through feces is approximately 2%.[31, 32]
Dapagliflozin:- Absorption: Following the oral administration of drug. maximum plasma concentration (Cmax) is usually attained within 2 hours under fasting state. The Cmax and AUC values increase dose proportionally with increase in dapagliflozin dose in the therapeutic dose range. 78% of absolute bioavailability is attained by 10mg of dapagliflozin drug administered. Also, with co-administration of high fat meal, it causes decreased in its Cmas by upto 50% andprolongs Tmax by approximately I hour, but does not alter AUC as compared with the fasted state. But they are not clinically meaningful and dapagliflozin can be administered with or without food.
Distribution: It is approximately 91% protein bound. Protein binding is not altered in patients with renal or hepatic impairment.[33]
Metabolism: The metabolism pathway of Dapagliflozinis mainly mediated by UGTIA9; CYP mediated metabolism is a major clearance pathway. in human. Drug is extensively metabolized, primarily to yield dapagliflozin 3-0- glucuronide, which is an inactive metabolite". Dapagliflozin 3-O- glucuronide (BMS 801576). The primary metabolite accounts for 61% of the dapagliflozin dose.[34]
Excretion: Dapagliflozin and related metabolites are primarily eliminated by the renal pathway. Following a single dose 50mg dose of [14]-dapagliflozin, 75% and 21% total radioactivity is excreted in urine and feces, respectively. In urine less than 2% of the dose is excreted as the parent drug. In feces approximately 15% of the drug is excreted as parent drug. The mean plasma terminal half life (11/2) for dapagliflozin is approximately 12.9 hours following a single oral dose.[33]
7. CLINICAL ROLE IN CARDIOMETABOLIC DISORDERS
1. Clinical Role of Bisoprolol
a) Hypertension
b) Chronic Heart Failure
c) Ischemic Heart Disease
d) Cardiometabolic Advantage
2. Clinical Role of Dapagliflozin
a) Type 2 Diabetes Mellitus
b) Heart Failure
c) Renal Protection
d) Cardiometabolic Benefits
8. SAFETY AND TOLERABILITY
Bisoprolol is a highly β1-selective adrenergic blocker with a well-established safety and tolerability profile in patients with cardiometabolic disorders. Clinical studies have shown that bisoprolol is generally well tolerated when initiated at low doses and gradually titrated. Common adverse effects include bradycardia, fatigue, dizziness, hypotension, and cold extremities, which are usually mild to moderate and dose-dependent. Due to its β1-selectivity, bisoprolol has minimal adverse effects on glucose and lipid metabolism, making it safer for patients with diabetes mellitus and metabolic syndrome compared to non-selective β-blockers.[40] Large clinical trials such as CIBIS-II have demonstrated a significant reduction in cardiovascular mortality and hospitalization in heart failure patients without compromising safety. However, caution is advised in patients with bronchial asthma, severe bradycardia, or conduction abnormalities, and abrupt discontinuation should be avoided to prevent rebound cardiovascular effects.[41]
Dapagliflozin, a selective sodium–glucose co-transporter-2 (SGLT2) inhibitor, has demonstrated favorable safety and tolerability in both diabetic and non-diabetic patients with cardiometabolic disorders. It is associated with a low risk of hypoglycemia when used alone, as its glucose-lowering effect is insulin-independent.[42] Common adverse effects include genital mycotic infections, urinary tract infections, polyuria, and mild volume depletion, which are generally manageable and reversible. Clinical outcome trials such as DECLARE-TIMI 58 and DAPA-HF have confirmed that dapagliflozin does not increase cardiovascular risk and significantly reduces hospitalization for heart failure, with added renal protective effects.[43] Although a transient decline in estimated glomerular filtration rate (eGFR) may be observed initially, long-term therapy slows the progression of chronic kidney disease. Rare but serious adverse events such as euglycemic diabetic ketoacidosis and Fournier’s gangrene have been reported, necessitating careful patient selection and monitoring.[44]
9. DRUG INTERACTIONS
Bisoprolol interacts with calcium channel blockers. Abrupt discontinuation of clonidine while taking bisoprolol results in a catecholamine surge and can lead to rebound hypertension. Bisoprolol should be stopped several days before the discontinuation of clonidine.[45] Concomitant use of bisoprolol with calcium channel blockers such as verapamil and diltiazem may worsen the myocardial function and result. in hypotension, bradycardia, and AV block.[46] Strong CYP3A4 induces, like rifampin, increases the clearance of bisoprolol. resulting in a short elimination half-life of bisoprolol.[47] Concomitant administration of cholinesterase inhibitors like donepezil with bisoprolol can increase the risk for bradycardia, falls, and syncope. Concomitant use of bisoprolol with digoxin delays AV conduction and can increase the risk of bradycardia.[48]
There were no clinically meaningful drug-drug interactions observed with several concomitant medications used by T2DM patients, like metformin, sitagliptin, digoxin, simvastatin, and warfarin. No drug-drug interactions were observed with drugs that may affect the metabolic pathway of Dapagliflozin (eg, mefenamic acid and rifampin). Also, they demonstrated that dapagliflozin has little potential either to affect metabolism or to have its metabolism meaningfully affected by co administration of other drugs. The mean exposure to dapagliflozin in subjects with moderate and severe hepatic impairment was 36% and 67% higher, respectively, than that of healthy subjects.[34]
10. FUTURE PERSPECTIVES
Bisoprolol
Dapagliflozin
11. CONCLUSION
Cardiometabolic disorders represent a major global health challenge due to the complex interplay between cardiovascular and metabolic abnormalities such as hypertension, type 2 diabetes mellitus, heart failure, and chronic kidney disease. Effective management of these conditions requires therapeutic strategies that provide both cardiovascular and metabolic benefits. Bisoprolol and dapagliflozin have emerged as important pharmacological agents fulfilling these requirements.
Bisoprolol, a highly selective β1-adrenergic blocker, offers significant cardiovascular protection by reducing heart rate, myocardial contractility, and sympathetic overactivity while exerting minimal adverse effects on glucose and lipid metabolism. Its proven efficacy in hypertension, ischemic heart disease, and chronic heart failure makes it particularly suitable for patients with coexisting metabolic disorders. Dapagliflozin, a selective SGLT2 inhibitor, provides insulin-independent glycemic control along with robust cardiovascular and renal protective effects. Its ability to reduce heart failure hospitalization, slow the progression of chronic kidney disease, promote weight loss, and lower blood pressure highlights its expanding role beyond diabetes management.
The complementary mechanisms of action of bisoprolol and dapagliflozin support their combined use in patients with cardiometabolic disorders, offering a holistic and patient-centered therapeutic approach. Clinical evidence strongly supports their safety, tolerability, and long-term benefits in improving cardiovascular outcomes and overall quality of life. With ongoing research and evolving clinical guidelines, the integration of bisoprolol and dapagliflozin is expected to play an increasingly important role in the comprehensive management of cardiometabolic disorders in the future.
REFERENCES


Vishweshwari Dhore, Prachi Mandave, Dr. Anup Barsagade, Dr. Sachin Dudhe, Role of Bisoprolol and Dapagliflozin in the Management of Cardiometabolic Disorders: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1409-1420. https://doi.org/10.5281/zenodo.18559265
 10.5281/zenodo.18559265
10.5281/zenodo.18559265
