Chandigarh College of Pharmacy Landran, Mohali, India
It is now well recognized that taking a child's blood pressure is a crucial part of the standard physical checkup. Children's blood pressure has only received significant attention and it is unclear how children's blood pressure has naturally changed throughout time. The frequency of pediatric hypertension is rising in tandem with the epidemic of childhood obesity. The diagnosis of hypertension in children is challenging since normal and abnormal blood pressure levels are hard to recall and change with breakfast, age and sex. Childhood obesity and other cardiovascular risk factors are frequently linked to hypertension. The well-documented pediatric obesity pandemic is contributing to an increase in the prevalence of high blood pressure (BP) among the younger population. Given the prevalence of confirmed hypertension (>3%) and pre-hypertension (>3%) in children and adolescents without symptoms, elevated blood pressure need to be regarded as a typical chronic health issue in childhood.
Hypertension is the major health problem in the children and adolescents that is often overlooked. Prehypertension and hypertension are becoming more common in children and adolescents due to the epidemic of overweight and obesity in children and youth. Children's blood pressure measurements need to be adjusted based on their size and age. Recent substantial declines in coronary heart disease can be attributed in large part to advancements in the detection and treatment of hypertension. A dangerous medical condition, hypertension raises the chance of developing heart, brain, kidney, and other diseases (1). Hypertension is defined as a persistently elevated resting systolic, diastolic, or both blood pressure; in children, the threshold for high blood pressure varies according to age up to 13 (2).
For children under 13 years old, hypertension is defined as blood pressure that is 95th percentile or higher, and raised blood pressure is defined as blood pressure that is 90th percentile higher for the given age, height, and sex. Adolescents 13 years of age and older with raised blood pressure have a systolic blood pressure of 120 to 129 mmHg and a diastolic blood pressure of less than 80 mmHg; hypertension is defined as a blood pressure of 120/80 mmHg or above.
(Ambulatory Blood Pressure Monitoring, or ABPM has greatly improved the detection and monitoring of HTN. It enables more precise staging and classification of HTN in addition to the computation of more complex parameters like the Ambulatory Arterial Stiffness Index, or AASI. Arterial stiffness measurement allows evaluation of arterial dysfunction, which may occur prior to structural vascular alterations assessed by carotid intima media thickness.) Chronic high blood pressure eventually damages end organs, such as the central nervous system and Left Ventricle Hypertrophy (LVH), which raises the risk of cardiovascular illness and death. The current review's findings on recent advancements in kid HTN should help improve childhood HTN screening and treatment (3).
High blood pressure could be
Primary hypertension is the predominant cause after the age of 6, and this is especially true for teenagers. Secondary hypertension is more common before age 6, and especially in children under 3.
Primary hypertension is an exclusion diagnosis by definition because the underlying cause is unknown. Nonetheless, it is recognized that children who are you obese or overweight (the main risk factor for primary hypertension)? possess a family history of hypertension are guys.
Are they Black Americans who are not of Hispanic descent or Mexican Americans? Lead a sedentary existence possess unhealthful eating habits (such as a high salt and calorie intake) had a variety of intrauterine issues (such as small for gestational age, low birth weight, or preterm). Possess social risk factors (e.g., food and/or housing insecurity, family and/or interpersonal violence, abuse of children; the quantity, persistence, and intensity of these problems have an additive effect) (4).
Primary hypertension is primarily assumed to be an adult condition, with a prevalence of 30%.1 However, it is believed to be less prevalent in children, having its origins in childhood (5). The effects of chronically high blood pressure, which show changes in childhood, can cause significant harm to the heart, blood vessels, and other organs by the time essential hypertension is diagnosed in adulthood. However, children's hypertension is often underdiagnosed since it is a more complex diagnostic than adult hypertension (6).
If the source of secondary hypertension is found and treated, the hypertension may be reversible. Children's secondary hypertension is most frequently caused by:
Additional reasons for secondary hypertension consist of
Pathophysiology of Hypertension in Children:
Gaints in the fields of physiology and cardiology addressed the issue if the volume vs hindrance as early as century ago. When compared to normotensive controls, Hayasaka discovered that individual with malignant hypertension and nephrogenic hypertension such as those with acute glomerulonephritis, had much higher volume expressed as CO (9). On the other hand,Burwell and Smith’s investigation found no variation in CO in individual with arterial hypertension(10). Prinzmetal and Wilson provides indirect evidence in 1936 that people with pH exhibited elevated TPR, implying that it was both functional and possibly reversible rather then long term(11). Two major theories about the pathophysiology of pH emerged within the few decades. One, as explained by Author Guyton, concentracted on renal excretory function and the volume factor.(12)
In a laboratory animal[dogs] with dreceased kidney mass and exposed to NaCl load, Guyton et al.’s experimental result show that an increase in volume brought on by a NaCl load rises CO, which in turn induces a gradual rise in TPR. Therefore in order to excrete same quantity of salt, people who are salt sensitive[SS] need to have higher blood pressure. In this paradigm, the primary cause of elevated blood pressure is the renal dysfunction that result in salt retention. Guyton;s mechanistic model, which has been expanded upon, include numerous processes that control blood pressure, including the renin-angiotension system[RAS], stress, and baroreceptors and chemoreceptors. A clinical example of the validity of Guyton’s theory is volume- and salt-dependent hypertension in patients with acute kidney injury or advanced chronic kidney disease. The second hypothesis presented by Folkow states that a structural remodeling of resistance vessels is a cause of sustained hypertension (13). Folkow stated that in PH — as well as in animal models of arterial hypertension, such as in spontaneously hypertensive rats or in renovascular hypertension — the problem lies in vascular remodeling of resistance vessels. It leads to a greater increase in resistance at the same degree of smooth muscle shortening in hypertensive subjects compared to normotensives. From a biophysical point of view, increased BP will increase circumferential wall stress. As circumferential wall stress depends on pressure, internal arterial radius, and wall thickness, in order to decrease or normalize circumferential wall stress, the arterial radius 1must be decreased or the wall thickness increased. Different arteries react in different ways. Large conduit arteries, such as the aorta or common carotid arteries, decrease wall stress by increasing wall thickness. It can be clinically observed as increased carotid intima-media thickness (cIMT), which is well documented in pediatric studies. In contrast, a different reaction dominates in small resistant arteries: it is a decrease in radius which not only decreases wall stress but also controls tissue perfusion
Sign and Symptoms: -
Children with hypertension, or high blood pressure, frequently don't exhibit any overt symptoms. Symptoms may include:
Risk Factor :-
Although it's less prevalent in children than in adults, hypertension, or high blood pressure, in children might have a variety of risk factors. Among the risk factors for childhood hypertension are:
In particular, for children with risk factors, routine check-ups with a healthcare professional are crucial to detecting and treating hypertension in children. For prevention and control, lifestyle changes including eating a balanced diet, reducing stress, remaining physically active, and maintaining a healthy weight are essential.
DIAGNOSIS: -
Blood pressure that is elevated in those under the age of eighteen, sometimes referred to as pediatric hypertension or hypertension in youngsters. Children's blood pressure is usually measured with the proper pediatric cuffs and procedures in order to diagnose hypertension
Using standardized formulas that account for the child's age, sex, and height, the diagnosis is determined based on blood pressure measurements. These variables are used to categorize blood pressure measurements into various percentiles.
A child is diagnosed with hypertension if their blood pressure repeatedly tests at or over the 95th percentile for their age, sex, and height. When making a diagnosis of pediatric hypertension, medical professionals should take into account additional aspects such lifestyle choices, underlying medical disorders, and family history.
In order to diagnose hypertension in children, a number of procedures are usually included, such as taking the child's blood pressure, analyzing lifestyle variables, reviewing family history, and maybe ordering more tests to rule out underlying medical issues. To find out if hypertension is present, blood pressure readings are compared to standard charts that have been modified for age, sex, and height. If high blood pressure is found, more testing could be required to determine any underlying reasons and create a suitable treatment strategy.
MANAGEMENT:
The goal of treating pediatric hypertension is to identify the underlying reason of the high blood pressure as well as to reduce any associated symptoms. Therapy decisions are influenced by comorbid illnesses, end-organ damage, and related risk factors.
Treatment recommendations, both pharmacologic and non-pharmacologic, are contingent upon the child's age, the stage of hypertension, and the patient's reaction to therapy.
Children with hypertension are frequently treated with a combination of pharmaceutical and non- pharmacological methods.
1. Pharmacological:
Depending on the child's age and health, pharmacological treatments may include drugs such as diuretics, ACE inhibitors, angiotensin II receptor blockers (ARBs), and calcium channel blockers. If there is significant obesity along with other coexisting conditions, medication therapy should be taken into consideration. If dietary-behavioral changes are successful, medication therapy may then be discontinued. Children and adolescents are also provided the medications that are now advised for the treatment of adult-onset hypertension: Alizarin, a direct renin inhibitor, has not yet been studied in pediatric settings.
2. Non-Pharmacological:
Non-pharmacological options include dietary adjustments (e.g., increasing foods high in potassium and decreasing salt), regular physical exercise, managing weight, and stress-reduction methods.
These include maintaining a healthy weight, getting regular exercise, eating a low-fat, low-sodium diet, giving up alcohol, and quitting smoking. Obesity favors the development of insulin resistance, hyperlipidemia, and salt sensitivity while tripling the risk of hypertension (23-24).
Significant obesity, regardless of blood pressure level, also raises the risk of LVH.27 Children's blood pressure has been demonstrated to drop with exercise, although left ventricular function is unaffected (25-26).
Data regarding dietary changes in children with hypertension are limited. However, the NHBPEP has advocated a daily consumption of 1,200 mg of salt, taking an extreme approach to sodium limitation. Children's blood pressure may be successfully lowered by following a no-salt-added diet that emphasizes fresh produce, low-fat dairy, and protein, much like the DASH (Dietary Approaches to Stop Hypertension) eating plan (27). Increased consumption of calcium and potassium has also been recommended as a dietary approach to lowering blood pressure (28-29).
AIM: Screening on hypertension and hypotension in children.
Objective:
METHODS:
Although less prevalent than in adults, hypertension in children can nonetheless develop and needs to be carefully managed. Through a retrospective chart review, we gathered clinical history and demographic data from 195 consecutive children who were assessed.
RESULT:
Out of the 195 children who were referred to the clinic due to a history of increased blood pressure. The patients were classified as follows: 50% had normal blood pressure, 20% had white hypotension, 30% had prehypertension. Of the 195 children with hypertension,78(or 43% of the group; boys made up 56% of the group; median age = 12 years; range = 3–17 years) children with hypotension, 29(or 66% of the group; median age = 9 years; range = 0.08–19 years) and children with normal blood pressure are 88(there are rate of normal blood pressure as compare to the hypertension and hypotension.)
Table 1: This table consist of total no. males and female those are the part of our screening. Male candidates are 102, female candidates are 93 and total no. of candidates are 195.(AS SHOWN IN FIGURE:1)
|
Male |
102 |
|
Female |
93 |
FIGURE: 1
Table 2: This table consist of total no. of patients as per the age group. Total no. of infants (having age of new born to 1 year) are 11, no. of childhood (having age between 2 years to 12 years) are 111 and total no. of adolescence (having age 12 years to 18 years) are 73.(AS SHOWN IN FIGURE:2)
|
Infants |
11 |
|
Childhood |
111 |
|
Adolescence |
73 |
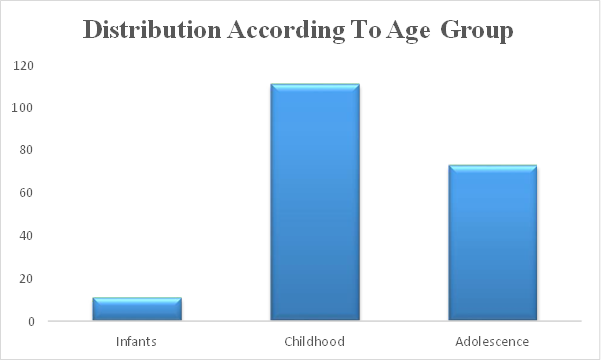
Figure 2:
Table 3: This table consist of the data which contains the information of total no. of male and female of infants (male:7, female:4), childhood (male:60, female:51) and adolescence (male:35, female:38). (AS SHOWN IN FIGURE 3)
|
|
Total |
Male |
Female |
|
Infants |
11 |
7 |
4 |
|
Childhood |
111 |
60 |
51 |
|
Adolescence |
73 |
35 |
38 |
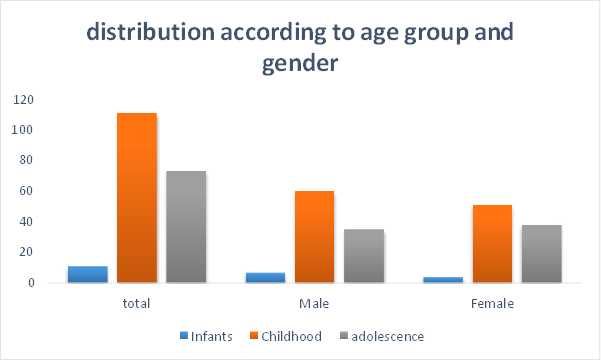
FIGURE 3:
TABLE 4: This consist of the information about the children having hypotension/normal or hypertension. There are approximately 29 patients of children having hypotension, 88 patients having normal blood pressure and 78 are suffering from hypertension. (AS SHOWN IN FIGURE 4).
|
Hypotension |
Normal |
Prehypertension |
|
29 |
88 |
78 |
Screening of hypotension and hypertension
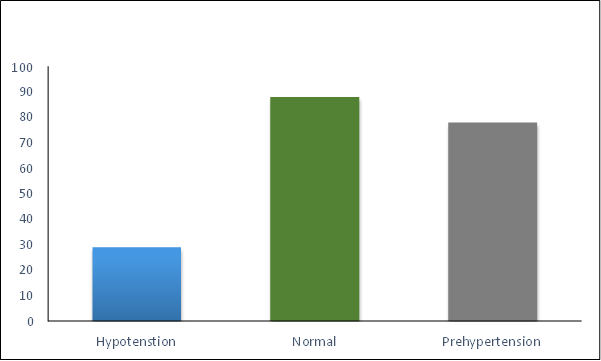
FIGURE 4:
CONCLUSION
Hypertension and prehypertension were frequently undiagnosed in this pediatric population. An increasing number of children and teenagers are being diagnosed with hypertension, a condition that has to be treated carefully and promptly. We can only assume that as obesity rates grow, prehypertension and hypertension will become more prevalent as well. We believe that obesity and then hypertension can be managed without the need for extra pharmaceutical intervention if a well-balanced diet and improved physical exercise are implemented.
REFERENCES







Kashish Sharma, Rakshit Verma, Priya Thakur, Kirpal Singh, Navjot Kaur, Preeti Dhiman, Nikita Choudhary, Screening on Hypertension and Hypotension in Children, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4173-4182. https://doi.org/10.5281/zenodo.18776742
 10.5281/zenodo.18776742
10.5281/zenodo.18776742
