Sant gadge Baba university Amravati.
Objective To investigate the effect of Stenocereus stellatus on the improvement of sleep quality in insomnia mice and its mechanism through a mice model of insomnia induced by chronic unpredictable stress. Methods A total of 30 swiss albino mice were randomly divided into 6 groups: control group, inducing group, positive drug group (diazepam 2.5 mg·kg-1 ), and high-, and low-dose groups 200 and 400 mg/kg , 6 in each group . swiss albino mice in other groups except the control group were stimulated by multiple factors for 14 days, to build a model of insomnia. After that, diazepam and three different doses of stomach soothing prescription were given for 14 days. Behavioral experiments and sodium pentobarbital-induced sleep experiments were performed separately. Results Compared with the CUS inducing group,. The Forced Swim Test (FST), a standard test for assessing depressive-like behavior, revealed increased immobility time in the stress control group, indicating behavioral despair. Mice treated with EESS showed a significant reduction in immobility time, suggesting antidepressant-like effects. Diazepam, used as a positive control, also significantly decreased immobility.In the Hole Cross Test, another measure of depressive behavior, the stress control group exhibited increased immobility. EESS-treated groups displayed improved activity levels, indicating a reduction in depressive symptoms. Diazepam again showed a strong positive effect.
Sleep is essential for overall health and well-being, and disturbances in sleep can significantly affect both physical and mental health. Insomnia is a common sleep disorder characterized by difficulty in falling or staying asleep and can result in fatigue, mood disorders, weakened immunity, and increased risk of chronic diseases. Sleep disturbances disrupt homeostatic control and increase vulnerability to inflammation-related illnesses. One of the main physiological systems impacted by sleep deprivation is the stress response system, especially the hypothalamic-pituitary-adrenal (HPA) axis.The HPA axis is central to the body’s stress response. When the body perceives stress, the hypothalamic paraventricular nucleus (PVN) releases corticotropin-releasing factor (CRF), which triggers the secretion of adrenocorticotropic hormone (ACTH) from the pituitary gland. ACTH then stimulates the adrenal glands to release glucocorticoids, primarily cortisol. Persistent stress and disrupted sleep can dysregulate this axis, contributing to disorders like anxiety and depression, which are often associated with insomnia. Experimental animal models, particularly rodents, are frequently used in insomnia research due to shared homeostatic and circadian mechanisms with humans. Although there are differences in sleep patterns between species, the underlying regulatory processes are similar, making animal models valuable for evaluating hypnotic drugs and understanding the mechanisms of insomnia. Insomnia is categorized by its duration (acute or chronic) and its cause (primary or secondary). Primary insomnia occurs without underlying conditions, while secondary insomnia results from other medical or psychological issues. Common symptoms include difficulty falling asleep (initial insomnia), frequent night awakenings (middle insomnia), and waking too early (late insomnia). These disturbances often lead to daytime fatigue, cognitive impairment, irritability, and reduced performance in daily activities.The causes of insomnia are multifaceted and include genetic factors, brain activity differences, mental health disorders, chronic medical conditions, stress, and lifestyle factors. Risk factors also include alcohol use, unsafe living environments, and anxiety about sleep. Long-term insomnia can result in complications such as hypertension, diabetes, heart disease, and depression. Diagnosis typically involves a detailed medical history and may include tests like polysomnography, actigraphy, or the Multiple Sleep Latency Test (MSLT) to rule out other sleep disorders. Treatment options for insomnia vary and often include behavioral strategies like improving sleep hygiene, cognitive behavioral therapy (CBT), and medication. Common pharmacological treatments include sedative and hypnotic drugs. These may be prescription medications like benzodiazepines (e.g., temazepam, triazolam), non-benzodiazepine “Z-drugs” (e.g., zolpidem, eszopiclone), dual orexin receptor antagonists (e.g., suvorexant), and sedating antidepressants (e.g., trazodone, doxepin). Melatonin and its synthetic analogs are also used. However, many of these drugs can lead to side effects such as cognitive dysfunction, dependency, and altered sleep architecture. In recent years, herbal medicine has gained popularity as a safer alternative for managing insomnia. Herbal sedatives like valerian root, chamomile, lavender, and kava have traditionally been used to promote relaxation and improve sleep quality. These herbs are believed to interact with neurotransmitters like GABA and serotonin, helping to regulate sleep cycles naturally. Herbal remedies offer several advantages: they tend to have fewer side effects, carry a lower risk of dependence, and provide a more holistic approach by addressing both the physical and emotional aspects of sleep disorders. They are also cost-effective and accessible, making them a practical option for many individuals. In conclusion, insomnia is a complex condition with various contributing factors and significant health consequences. While conventional treatments remain essential, herbal medicines present promising alternatives in the quest for safer and more natural insomnia management strategies.
Experimental animals:
Swiss Albino mice of either sex or 8-12 weeks age were used for study. The animals were housed on a 12-h light/dark cycle under controlled temperature (22°C ± 2°C) and humidity (50 ± 10%). Experiments are performed in accordance with the committee for the purpose of control and supervision of experimental animals (CPCSEA) guidelines after approval of the experimental protocols by the institutional animal ethics committee (IAEC).
Selection of the plant
The medicinal plant Stenocereus stellatus (Family: cactaceae) was selected for sedative and hypnotic activity
Preparation of plant extract
Cactus stem would be collected , The sample will be washed with water, cut into small pieces and then pressed using a hand-press, homogenized with 10 mM Tris-HCl, pH 7.4 at 4 °C and centrifuged 30 min at 3500g at 4 °C. The supernatant was subsequently collected and lyophilized. Before use, the lyophilized extract was dissolved in water. The extracts would be then subjected to different phytochemical tests for identification of different photochemical principles. The plant extracts would be studied for the presence of important phytochemical which may be involved in the action of plant.
Phytochemical screening:
The ethanolic extract of Stenocereus stellatus stem was screened for the presence of various phytochemicals, including carbohydrates, flavonoids, alkaloids, glycosides, phenolic acids, triterpenoids, sterols, fatty acids, tannins, proteins, and amino acids, using standard qualitative methods.
Drugs and chemicals
Diazepam 3mg/kg.
PHARMACOLOGICAL SCREENING
Chronic Unpredictable Stress The study adopted the Chronic Stress Syndrome (CUS) model to study the long-term consequences of various stressors on animals. The stressors were delivered weekly in a varied sequence, with each animal receiving one stress per day individually. The CUS procedure was applied for 14 consecutive days, with the stressors applied at different times in a random order to maximize unpredictability and same stressors were not used for any two consecutive days. .Animals were held in a recovery area for an hour after each stressor, then transferred to a clean cage with new bedding. Mice were housed separately for the same amount of time, and the CUS paradigm involved daily exposure to one of the unpleasant stimuli listed below.
1. Cold Water Swimming
2. Food Deprivation
3. Limbs Restrained
4. Hot water swimming
5. Wet sawdust bedding
6. Cage-Tilting
7. Water deprivation
Instruments and equipment: Centrifuge weighing balance, pipettes, test tube/racks, timer, biochemical analyser, microscope. Preparation of doses and treatments.
I.P. Diazepam 3 mg/kg. Two different concentrations (200 mg/kg, 400 mg/kg) of the EESH were prepared by dissolving the extracts in distilled water. All solutions were freshly prepared at the time of administration to the animals. Extract solution and vehicle (0.9% NaCl) were given orally and standard drug (Diazepam)
Treatment protocol:
The mice were randomly divided into 5 groups of 6 mice each.
Table 1 : Treatment protocol for all groups:
|
Sr.no. |
Group |
No. of Animals |
Treatment and Dose |
Route of Administration |
|
1 |
I (Normal control) |
6 |
Saline treatment |
IP |
|
2 |
II (Negative control) |
6 |
CUS |
|
|
3 |
III (standard dose) |
6 |
Diazepam+ CUS(3mg/kg) |
IP and Oral |
|
4 |
IV (Treatment 1) |
6 |
CUS+ Moderate dose of Stenocereus stellatus stem extract (200 mg/kg bw) |
Oral |
|
5 |
V (Treatment 2) |
6 |
CUS+ High dose of Stenocereus stellatus stem extract (400 mg/kg bw) |
Oral |
Statistical analysis
The data obtained from the screenings were subjected to statistical analysis following TWO-way ANOVA followed by TUKEY Comparison Test to assess the statistical significance of the results using GraphPad prism- software. The difference was considered significant if p < 0.05, moderately significant if p < 0.01, and highly significant if p < 0.001.
The phytochemical screening revealed the presence of flavonoids, alkaloids, glycosides, phenolic acids, sterols, tannins, proteins, amino acids, phenols, and saponins in the extract.
Table: Physico-chemical tests of ethanolic extract of Stenocereus stellatus stem.
|
Sr. No. |
Test |
Standards |
Results |
Method |
|
A |
Physico-chemical tests |
|||
|
1 |
Description |
Light colored powder |
Complies |
Organoleptic |
|
2. |
Odour |
Characteristics |
Characteristics |
Organoleptic |
|
3. |
Identification |
Positive |
Complies |
TLC |
|
4. |
Moisture Content |
NMT-9% w/w |
1.5% |
IP-2020 |
|
5. |
Ash Content |
NMT-6% w/w |
3.4% |
IP-2020 |
|
6. |
Acid insoluble Extract |
NMT-2% w/w |
0.43% |
IP-2020 |
|
7. |
Bulk Density (untapped) |
NLT-0.8% g/ml |
0.51 g/ml |
IP-2020 |
|
8. |
Bulk Density (tapped) |
NMT-0.21g/ml |
0.75 g/ml |
IP-2020 |
|
9. |
50% Alcohol Soluble Extractive |
NLT-80% w/w |
77.2% |
IP-2020 |
|
10. |
Water Soluble Extractive |
NLT-70% w/w |
33.8% |
IP-2020 |
|
11. |
Particle Size |
More than 80% pass through 63 mesh |
Complies |
63 mesh sieves |
|
12. |
pH (1%solution water) |
6-7 |
4.3 |
IP-2020 |
Each mouse, chosen for its size and weight, was delicately placed into an elongated cylindrical glass container measuring precisely 25 cm in height and 10 cm in diameter. The transparent container was meticulously filled with exactly 20 cm of clear water, creating a controlled aquatic environment for the experiment. The room temperature, consistently maintained at 24 ± 1 ?C, provided optimal conditions for the mice. Care was taken to ensure that the mice, upon introduction to the water, floated without any hindrance, their delicate tails carefully positioned to prevent contact with the container's base. After granting the mice a brief 2-minute adjustment period to acclimatize to their surroundings, the experiment commenced, with the focus shifting to measuring the mice's subsequent 4 minute resting time. The resting time was defined as the duration for which the mice maintained a state of buoyancy in the water, exhibiting minimal movement while effortlessly keeping their heads above the water surface. This crucial observation allowed for the evaluation of the mice's natural inclination to remain afloat without requiring significant exertion, shedding light on their innate physiological responses in water.
Figure : Forced Swimming Test
Table : Sedative and hypnotic effect of EESS On Forced swim test
|
Group no. |
Treatment |
Immobility Time (s) |
||
|
Day 1 |
Day 7 |
Day 14 |
||
|
I |
Control Vehicle (10ml/kg) |
155.5±0.34 |
150.5±0.33 |
146.6±0.36 |
|
II |
CUS Group |
185.6±0.41 |
190.4±0.43 |
206.3±0.30 |
|
III |
Diazepam (03mg/kg) |
97.2± 0.55∗ |
80.3±0.30∗ |
74.1±0.29∗ |
|
IV |
EESS (200mg/kg) |
141.5±0.36∗ |
139.3±0.18∗ |
135.2±0.18∗ |
|
V |
EESS (400 mg/kg) |
134.8±0.20∗ |
130.3±0.19∗ |
126.6±0.081∗ |
Values are expressed as Mean ± SEM (n=6) .Data were analysed using two-way ANOVA followed by Tukey,s multiple comparison test to assess significant differences between all groups. Significant differences *(p<0.0001) were primarily observed between CUS group and treatment group (Diazepam and EESS doses), indicating the efficacy of treatment in sedative and hypnotic-like behavior. The study found that mice treated with extract (200 & 400 mg/kg body weight) showed a significant delay in immobility onset and reduced time spent immobile in the forced swimming test after 14 days of treatment. Analysis using Dunnet's t-test multiple comparison test showed that the test treatment considerably shortened the immobility period in comparison to the control group (p<0.0001). In control group the immobility time was 154.5±2.57, 149.7±3.74, 145.6±3.68 seconds up to 14th day. The results were statistically significant in test groups 2 when compared to CUS in which the immobility time was 95.5± 8.2, 79±3.89, and 73.4±2.86seconds. However, all test groups experienced a considerable reduction in immobility time after receiving extracts .i.e. group 3 and 4 to 141.2±0.86, 138.7±1.82, and 134.6±1.68 seconds while in group 4 and 5 the results were 134.2±1.25, 129.6±0.82, 126.7±0.35 and 184.5±2.87, 189.7±4.95 and 205.6±3.57 when compared to CUS group.
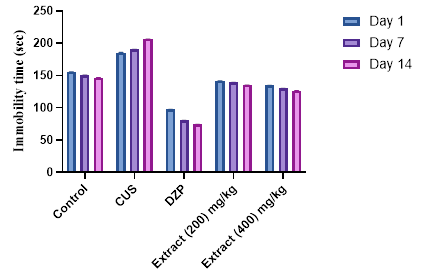
Figure : Effect of extract on immobility time in the Forced Swim Test in mice
Hole Cross Test:
Table : Sedative and hypnotic effect of EESS On Hole cross test
|
Group no. |
Treatment |
Number of Movements |
|
||||
|
0 min |
30min |
60min |
90min |
120 min |
|||
|
I |
Control Vehicle (10ml/kg) |
17.84± 0.21 |
16.43± 0.12 |
16.45± 0.20 |
16.61± 0.30 |
17.40± 0.23 |
|
|
II |
CUS Group |
20.16± 0.23 |
22.03± 0.19 |
26.60± 0.23 |
29.04± 0.24 |
30.11± 0.18 |
|
|
III |
Diazepam (3mg/kg) |
18.33± 0.18 * |
6.52± 0.036 * |
4.76± 0.20 * |
4.28± 0.10 * |
3.91± 0.070 * |
|
|
IV |
Extract (200mg/kg) |
18.33± 0.18 * |
13.3± 0.18 * |
12.50± 0.19 * |
12.08± 0.29 * |
9.90± 0.10 * |
|
|
V |
Extract (400 mg/kg) |
17.9± 0.24 * |
8.13± 0.17 * |
7.00± 0.19 * |
5.88± 0.15 * |
4.71± 0.11 * |
|
Values are expressed as Mean ± SEM (n=6) .Data were analysed using two-way ANOVA followed by Tukey,s multiple comparison test to assess significant differences between all groups. Significant differences *(p<0.0001) were primarily observed between CUS group and treatment group (Diazepam and EESS doses),indicating the efficacy of treatment in sedative and hypnotic-like behavior.

Figure : Effect of Extract on movements in the Hole Cross Test in mice
The number of holes crossed by mice from the control group remained consistent between 0 to 120 minutes when moving from one chamber to another. During the hole cross test, the extracts exhibited a notable decrease in locomotion in the test animals starting from the second observation period. This decline was evident in the reduced number of holes crossed by the treated mice compared to the control group, showing similarity to the effects of the reference drug diazepam. Notably, the 200mg/kg dose displayed less significant results, whereas the 400mg/kg dose yielded statistically significant outcomes *(p < 0.0001) in the experiment when compared to the CUS group.
Stenocereus stellatus is a cactus species known for its rich phytochemical profile, including flavonoids, alkaloids, tannins, saponins, terpenoids, proteins, and carbohydrates. These compounds contribute to a variety of biological activities such as antioxidant, antidiabetic, hepatoprotective, hypotensive, and cardioprotective effects. In the context of neurological and psychological health, these bioactive constituents have shown promising potential in the management of stress-induced disorders.
Stress, in medical and biological terms, refers to any physical, mental, or emotional factor that leads to bodily or mental tension. Chronic stress is a major contributor to several neuropsychiatric conditions, including anxiety, depression, social withdrawal, hypervigilance, and memory impairment. The field of herbal psychopharmacology has increasingly explored plant-based compounds as natural anxiolytic and antidepressant alternatives to conventional medications, aiming for therapies that are cost-effective and have fewer side effects. The present study focused on evaluating the potential neuroprotective and stress-reducing effects of the ethanolic extract of Stenocereus stellatus (EESS) using chronic unpredictable stress (CUS) models in mice. The CUS paradigm is widely used to simulate human-like neuropsychiatric conditions in laboratory animals. In this protocol, seven different stressors were randomly applied to mice over a 14-day period. After a 24-hour rest, behavioral tests were conducted to evaluate the effects of EESS compared to both a stress control group and a diazepam-treated group.
Behavioral Assessments and Findings
The Forced Swim Test (FST), a standard test for assessing depressive-like behavior, revealed increased immobility time in the stress control group, indicating behavioral despair. Mice treated with EESS showed a significant reduction in immobility time, suggesting antidepressant-like effects. Diazepam, used as a positive control, also significantly decreased immobility.
In the Hole Cross Test, another measure of depressive behavior, the stress control group exhibited increased immobility. EESS-treated groups displayed improved activity levels, indicating a reduction in depressive symptoms. Diazepam again showed a strong positive effect.
GABAergic Mechanisms and Chronic Stress
Gamma-Aminobutyric Acid (GABA) is the brain’s main inhibitory neurotransmitter, playing a critical role in promoting relaxation, reducing neuronal excitability, and maintaining emotional balance. Chronic stress disrupts GABAergic functioning in multiple ways: by reducing the production of glutamic acid decarboxylase (GAD)—the enzyme responsible for converting glutamate to GABA—and by downregulating GABA-A receptors, which diminishes their sensitivity. These disruptions collectively reduce GABA levels, heighten neuronal excitability, and impair the brain’s ability to regulate mood and induce sleep. Chronic stress is also associated with increased levels of glutamate, an excitatory neurotransmitter, which creates a neurochemical imbalance skewed toward hyperarousal. This is further compounded by excessive activation of NMDA receptors, contributing to sleep disturbances. High cortisol levels—another hallmark of prolonged stress—impair GABA function and reduce the levels of allopregnanolone, a neurosteroid that enhances GABA-A receptor activity. These changes exacerbate insomnia, anxiety, and depressive symptoms.
EESS and Neurochemical Modulation
Accumulating evidence suggests that restoring the balance of neurotransmitters, particularly GABA and serotonin (5-HT), can improve outcomes in chronic stress disorders. The results of this study imply that EESS may exert its anti-stress effects through modulation of GABAergic pathways. Preliminary findings show that EESS significantly reduced stress-related behaviors in mice and may normalize GABA levels in key brain regions such as the hippocampus, amygdala, and prefrontal cortex. These effects were comparable to diazepam, a benzodiazepine known for its action on GABA-A receptors. Phytochemical analysis supports this theory. EESS contains flavonoids and tannins, both of which are known to influence GABA-A receptor activity. Flavonoids, in particular, have been shown in previous studies to act on benzodiazepine binding sites of GABA-A receptors, leading to sedative and anxiolytic effects. Tannins and other compounds may further support these effects through antioxidant and anti-inflammatory actions that protect neural pathways from stress-induced damage.
In conclusion, the present findings in our study highlight the remarkable sedative and hypnotic properties of Stenocereus Stellatus. The effects of this plant are not only strong but also act swiftly, with a lasting impact that has shown statistical significance across all doses tested in our experiments. Although these results are promising, further comprehensive studies are crucial to identify and isolate the specific bioactive compound or compounds responsible for these pharmacological activities in the plant. Additionally, these future investigations will be essential in elucidating the intricate molecular mechanisms that underlie the potent sedative and hypnotic effects exhibited by Stenocereus Stellatus. Understanding these precise mechanisms will not only deepen our knowledge of the plant's therapeutic potential but may also lead to the development of novel treatments or pharmaceutical interventions derived from these natural compounds. This research pathway holds immense promise in unlocking the full spectrum of benefits that Stenocereus Stellatuscould offer in the realm of health and medicine. By delving into the intricate web of molecular interactions and bioactive components within this plant, researchers can pave the way for innovative therapeutic strategies and potentially groundbreaking pharmaceutical discoveries that could revolutionize the field of natural medicine. Additionally, a deeper understanding of the pharmacological activities of Stenocereus Stellatus could shed light on its potential applications in various medical conditions and provide valuable insights into how traditional remedies can be harnessed for modern healthcare practices. Therefore, the journey to uncover the bioactive compounds and molecular mechanisms driving the sedative and hypnotic effects of Stenocereus Stellatusis not only scientifically compelling but also holds profound implications for the advancement of natural therapeutics and the development of novel treatment modalities in the future. The next step could involve the isolation of active compounds such as flavonoids for in-depth mechanistic studies to better understand their effects. Additionally, there is potential for conducting clinical trials aimed at validating the efficacy of these compounds in human subjects, which would provide valuable insights into their potential therapeutic applications and impact on human health. Expanding these research avenues could significantly contribute to advancing our knowledge of natural compounds and their effects on the human body.
REFERENCES

Nirmal Sarda*, Dr. A. M. Wankhade, Dr. V. V. Paithankar, Sedative And Hypnotic Activity of Stenocereus Stellatus Extract on Chronic Unpredicatable Stress Induced Insomnia in Experimental Animal, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 12-23. https://doi.org/10.5281/zenodo.15566168
 10.5281/zenodo.15566168
10.5281/zenodo.15566168
