
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, College of Pharmaceutical Sciences, Govt. Medical College, Kozhikode, India
Periodontitis is a chronic inflammatory condition that causes damage to the tissues that support teeth, including the gingiva, periodontal ligament, and alveolar bone brought on by pathogenic biofilms and host immune response. It begins with dental plaque and affects periodontal supporting tissues. Furthermore, it is challenging to treat periodontitis efficiently due to its numerous and complex pathological pathways. Therefore, the foundation of effective periodontitis therapy is the development of sophisticated local drug delivery systems and logical therapeutic approaches. Due to their biocompatibility, biodegradability, and ease of administration into the periodontal pocket, hydrogels have garnered significant attention in the field of treating periodontitis. Smart stimuli-responsive hydrogels, which can control drug release in response to stimulation and undergo flexible sol-gel transitions in situ, have become the focus of hydrogel research in recent years. In this review, we provide an overview of the latest developments in the creation, design, and material characterisations of popular injectable hydrogels.
Periodontitis is a chronic inflammatory disease that harms the gums, periodontal ligaments, root cementum, and bone that hold the tooth in its socket. The most frequent cause of periodontal inflammation is bacteria found in large amounts of dental plaque (biofilm) on tooth surfaces. Disproportionate host inflammatory immunological responses brought on by an imbalance in the makeup of oral bacteria and modifications to their metabolic processes are the main causes of this illness. Tooth-supporting tissues are eventually destroyed as a result of this microbial dysbiosis, which promotes the development of inflammatory diseases.[1]
With a frequency ranging from 20% to 50%, periodontal disease was ranked as the eleventh most common ailment worldwide in the 2016 Global Burden of Disease Study.[2] Periodontitis was seen in all states, with 7.8% of cases being severe. Nearly half of all adults (30 years of age or older) in the US have periodontitis, which confirms the disease's significant prevalence. Approximately 11% of people worldwide may suffer from severe periodontitis, which affects 743 million people.[3]
Periodontal diseases are polymicrobial, immune-inflammatory infections that have the potential to destroy the supporting alveolar bone and periodontal ligaments. More than 700 different bacterial species can be found in subgingival plaque, and some of these pathogens are crucial to the development and course of the disease. The most significant pathogens in adult periodontal disease are included in the red complex, which comprises Tannerella forsythia, Treponema denticola, and Porphyromonas gingivalis. Furthermore, linked to deep periodontal pockets and potentially contributing to the advancement of the disease are Fusobacterium nucleatum, Prevotella species, Eikenella corrodens, Peptostreptococcus micros, and Campylobacter rectus.[4,5]
The tissues that support teeth, such as the gingiva, periodontal ligament, alveolar bone, and cementum, are progressively destroyed by periodontitis, a chronic inflammatory disease. Periodontitis is a very common ailment that frequently manifests as tissue recession and tooth movement. In order to lower the pathogenic risk of periodontitis, the first clinical treatment for the condition is surgery or debridement by scaling and root planing, which removes both supragingival and subgingival dental plaque. Adjunctive medications are also necessary for the clinical treatment of periodontitis in order to inhibit the growth of harmful bacteria and create an environment where inflammation is reduced and periodontal tissue healing is possible. Antibiotics such as metronidazole, penicillin, minocycline, doxycycline, and others are used to treat periodontitis. However, high-dose systemic antibiotic therapy is necessary to maintain an effective drug concentration in periodontal tissue, which raises the risk of liver/kidney toxicity, microbial imbalance, and drug resistance. Hydrogel-mediated local drug administration has been suggested for the treatment of periodontitis to improve treatment results. Hydrogels are low-viscosity fluids made of biocompatible and biodegradable matrices that can be smoothly injected using a syringe and perfused into the periodontal pockets' inflammatory areas with stable mucosal adherence.[6] However, it is still difficult to repair the damaged periodontal architecture. Thus, sophisticated biotherapeutic strategies have been put forth to improve long-term clinical results and restore damaged periodontal tissues.[7,8]
Injectable hydrogels, which are adaptable biomaterials that can conform to the geometrically complex dental, oral, and craniofacial (DOC) anatomical structures, are one of the novel alternatives that are attracting more and more attention. In the dentin-pulp complex and periodontal lesions, these hydrogels offer a platform for the direct delivery of cells, growth factors, and other biotherapeutics. They are especially well-suited for regenerative dentistry, where precise, minimally invasive procedures are frequently desired, because of their injectability and capacity to fill irregular lesions.[7,9]
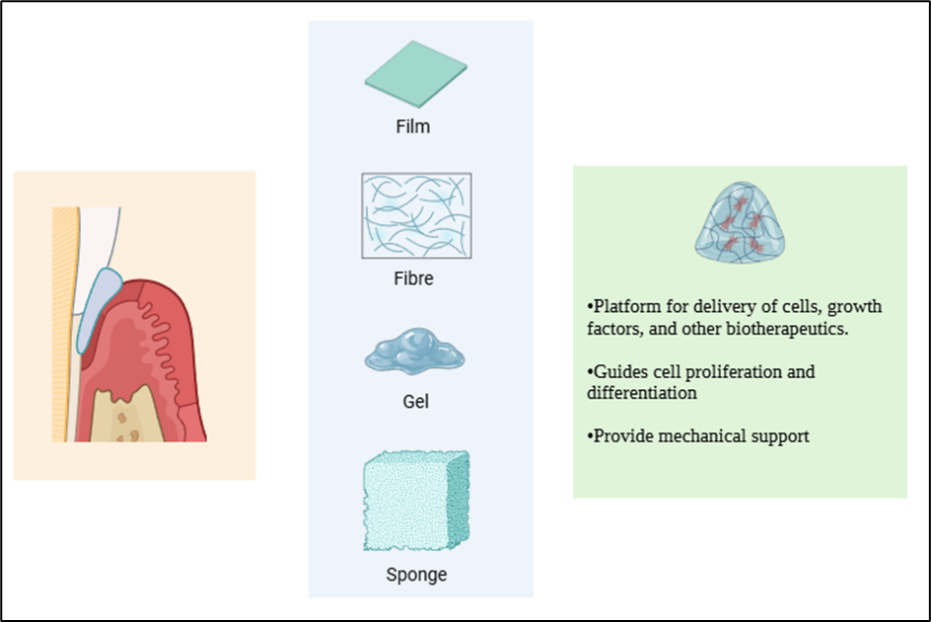
Figure 1: Common scaffold types of hydrogels and their roles in periodontal tissue regeneration. (created in https://www.biorender.com )
Hydrogels
Hydrogels are cross-connected, three-dimensional structures made of water-soluble polymers. Additionally, they can form coatings, incorporate microparticles, nanoparticles, and sections in them.[10] Hydrogels are therefore typically used in clinical practice and trial medication for a variety of applications, such as tissue design and regenerative medicine[11], diagnostics[12], cell immobilisation[13], biomolecule or cell partition[14], and boundary materials to guide natural bonds [15].
Preparation of Hydrogel through different cross-linking
Hydrogels can be produced by one-step procedures such as parallel cross-linking of multifunctional monomers and polymerisation. This enables the creation of networks of polymers with specific properties. Many processes are involved in the creation of reactive group-containing polymer molecules, which are subsequently cross-linked with the aid of suitable agents[16]. Hydrogels can be made using three different techniques: bulk, solution, and radiation polymerization.
Common solvents include water, ethanol, or DMSO; surplus solvent can be eliminated by swelling the gel in water. Cross-linking agents are added straight to the monomer mixture during bulk polymerization. Free radicals produced by radiation, UV light, or chemical initiators can create hydrogels by creating cross-links between polymer chains. Physical interactions such as entanglements, electrostatic forces, and crystallization can also result in cross-linking. The kind of monomers utilized determines the hydrogels' mechanical strength and rate of decomposition. Furthermore, polymerizable groups can be added to natural polymers to improve their hydrogel-forming capabilities.[17]
There are two different cross-linking techniques that use different processes:
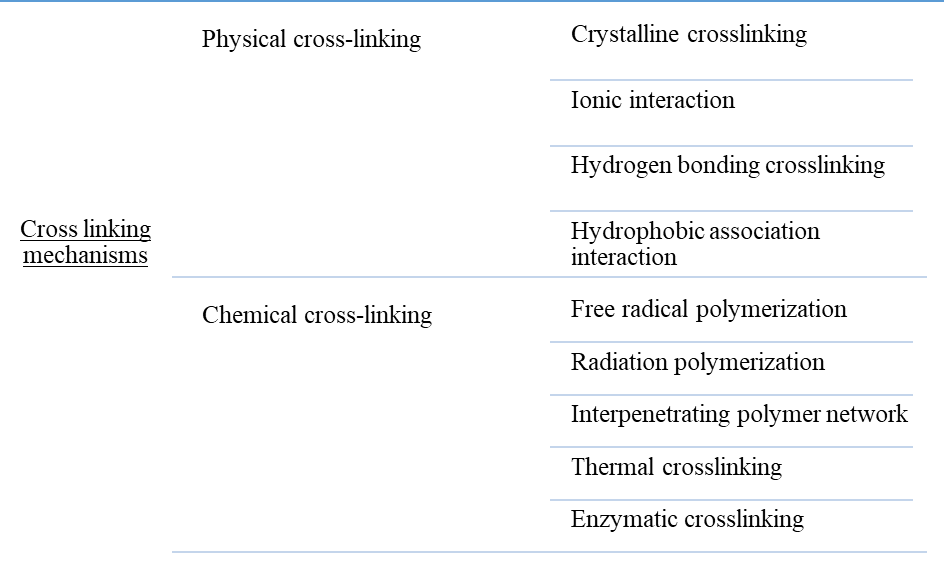
Figure 2: Different cross-linking techniques that use different processes
Hydrogen bonding, electrostatic forces, and entanglements are examples of non-covalent interactions that create physically cross-linked hydrogels. Because of worries about the toxicity of chemical cross-linking agents, they are regarded as safer substitutes for chemically cross-linked hydrogels, which makes them appropriate for biocompatible applications.
Chemically cross-linked hydrogels, on the other hand, have covalent connections that, by avoiding polymer chain degradation during usage, offer increased mechanical strength and structural stability.
Crystalline crosslinking
Crystalline crosslinking occurs when polymer chains crystallize and form hydrogen bonds, creating physical cross-links within a three-dimensional network. This is commonly achieved through stereocomplex formation or freeze–thaw cycles in homopolymers. The type and degree of crystallinity significantly affect the hydrogel’s properties.
For example, in polyvinyl alcohol (PVA) hydrogels, freeze–thaw cycles promote crystallization, which forms cross-links between PVA chains. The regular hydroxyl groups in PVA enable strong interchain hydrogen bonding, leading to crystallite formation and a stable network structure.[18]
Ionic Interaction Crosslinking
Electrostatic interactions between oppositely charged ions or polymers produce ionic-based hydrogels by forming a cross-linked network. This process is appropriate for biological applications since it takes place in mild environments like room temperature and physiological pH.
Alginate hydrogels, which are created via ionic gelation between divalent cations (such as Ca2+, Sr2+, and Ba2+) and the carboxyl groups of guluronic acid units in alginate, are a typical example. When these ions are present, alginate, which is made up of β-D-mannuronic acid and α-L-guluronic acid connected by β-(1→4) glycosidic linkages, experiences a sol–gel transition.
By attaching adjacent guluronic blocks, the divalent ions function as cross-linkers, creating a stable three-dimensional hydrogel network that mimics eggs placed in an egg carton, according to the "egg-box" paradigm.
Hydrophobic Association Interaction Crosslinking
In order to create self-healing hydrogels based on amphiphilic polymers, hydrophobic interactions are essential. Hydrophobic segments limit water contact in aquatic conditions, which promotes entropy-driven self-assembly into stable supramolecular structures. Within the gel, free and related hydrophobic groups are in a dynamic balance. These contacts reversibly dissolve to release energy under external stress, preventing fracture and facilitating self-healing. The ratio and qualities of the hydrophilic and hydrophobic segments can be changed to vary the mechanical properties. Hydrophobic interactions are weaker than hydrogen bonds and van der Waals forces, but they can be strengthened by raising the temperature or ionic strength.[17]
In many self-healing hydrogels, hydrophobic interactions function as reversible physical cross-links, allowing structure and characteristics to restore following mechanical stress. The inclusion of surfactant micelles, which solubilize hydrophobic monomers and produce more cross-linking sites through micellar copolymerization, can improve these interactions. Additionally, interactions between amphiphilic polymers and hydrophobic vesicle or nanoparticle domains can reinforce hydrophobic associations, enhancing the hydrogel's durability and capacity for self-healing.[17,19]
Radiation-induced free radical crosslinking
Free radical-mediated crosslinking, in which polymer chains produce and interact with free radicals to form a three-dimensional network, can be used to construct hydrogels. Free radicals can be created physically by radiation (UV or radiation with high energy) or chemically using ammonium persulfate and TEMED, for example.
There are two primary types of radiation that can cause radiation-induced crosslinking of hydrogels:
(a) Ionizing radiation (such as X-rays, electron beams, and γ-rays) has enough energy to ionize atoms or molecules. Through bond cleavage and radiolysis of solvents or monomers, it immediately produces primary free radicals, resulting in polymerization and crosslinking without the need for further initiators.[20]
(b) Molecules are not directly ionized by non-ionizing radiation, such as microwaves and UV light. Free-radical polymerization is started by UV radiation through direct photochemical activation or photoinitiators. Through dielectric heating, microwaves mainly promote thermally driven radical processes; non-thermal effects are still controversial and system-dependent.[20]
Medical applications benefit from the radiation method's advantages, which include gentle reaction conditions, minimal by-product production, rapid gelation, and the ability to achieve product purity and sterilization in a single process.[21]
Interpenetrating Polymer Network Crosslinking
An interpenetrating polymer network (IPN) is produced when a second hydrogel network is polymerized inside a prepolymerized hydrogel; typically, this is accomplished by immersing a prepolymerized hydrogel in a solution of monomer and polymerization initiator.[22]
Thermal Crosslinking
When creating hydrogel, thermal crosslinking is frequently utilized to create a three-dimensional network that can absorb and hold a lot of water. Heat-induced chemical or physical interactions, such as phase changes, hydrogen bond rearrangement, the production of free radicals, or the breakdown of crosslinking agents, cause crosslinking.
For instance, free radical polymerization in DMF at 65 °C in a nitrogen atmosphere with AIBN (azobisisobutyronitrile) as the thermal initiator can be used to create NiPAAm-co-GMA hydrogels.
Enzymatic Cross-Linking
Enzymes accelerate the creation of covalent connections between polymer chains in enzymatic crosslinking, a type of chemical crosslinking that produces durable hydrogel networks. This technique is ideal for tissue engineering applications since it is gentle and biocompatible, usually taking place in aqueous solutions at physiological temperature and neutral pH. It avoids the harmful effects of organic solvents and photoinitiators. Transglutaminase (TGase), tyrosinase (TYR), laccase, horseradish peroxidase (HRP), glucose oxidase (GOx), phosphopantetheinyl transferase (PPTase), lysyl oxidase, plasma amine oxidase, phosphatases, thermolysin, β-lactamase, and kinase/phosphatase systems are common enzymes used for hydrogel formation.
Types of Hydrogel
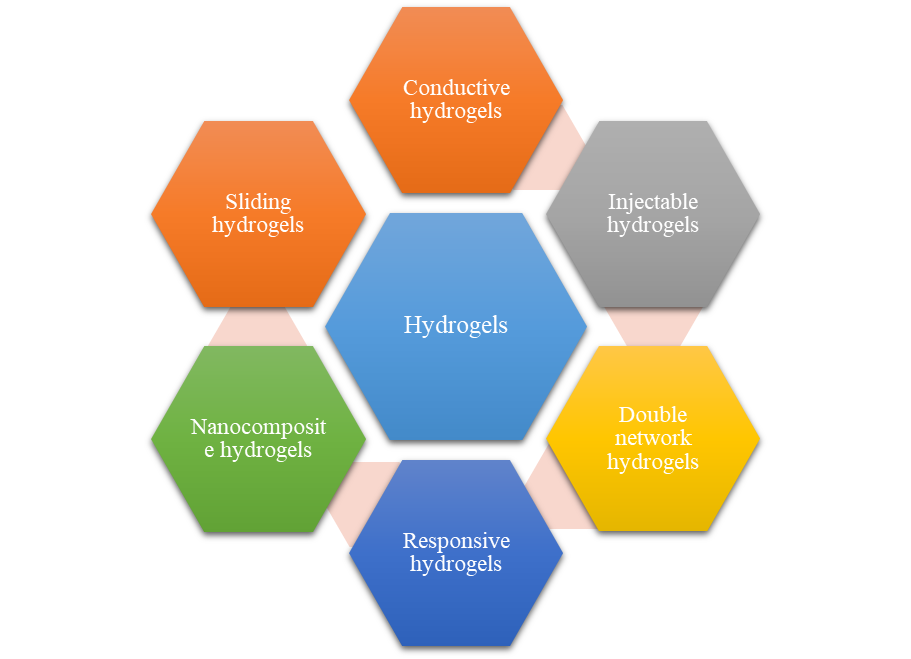
Figure 3: Different types of hydrogels for Periodontitis therapy
Other novel hydrogels
Despite the five biological hydrogels mentioned above, research has led to the development of several additional innovative hydrogels, such as magnetic hyaluronate hydrogels and DNA-enabled hydrogels. By reacting azide-functionalized single-abandoned DNA with dibenzo cyclooctyne-functionalized multiarm poly (ethylene glycol) in aqueous solution without the use of copper click chemistry, DNA-enabled hydrogels were created.
Table 1: Different types of Hydrogels and their characteristics.
|
Type of Hydrogel |
Definition Structure |
Key Feature |
Examples |
Main Advantage |
References |
|
Conductive Hydrogels |
Combined with conducting polymers or metallic nanoparticles, a cross-linked hydrogel network |
Electrical conductivity |
Polythiophene, Polyacetylene, and Poly (phenylene vinylene) |
Better mechanical and electrical qualities |
[23,24] |
|
Injectable Hydrogels |
Hydrogels with sol–gel transition which are administered via injection |
Delivery that is minimally invasive |
Polyethylene glycol, Polyvinyl alcohol |
Localized medication distribution and improved patient comfort |
[25,26] |
|
Double Network Hydrogels |
There are two interpenetrating networks: one flexible and one rigid. |
Absorption of energy and resistance to cracking |
Poly(N,N′-diethyl-acrylamide) |
High toughness and mechanical strength |
[27] |
|
Responsive (Smart) Hydrogels |
Hydrogels that change size in reaction to various stimuli, such as light, temperature, and pH |
Environmental sensitivity |
pH-sensitive gels based on methacrylic acid |
Tissue engineering and controlled drug release |
[6] |
|
Nanocomposite Hydrogels |
Nanoparticles scattered in a polymer matrix (1–1000 nm) |
Reinforced structure |
Metal/metal oxide, polymeric, carbon-based nanoparticles |
Increased stability and strength |
[28,29] |
|
Sliding Hydrogels |
Non-covalent hydrogels with moveable cross-links |
Stretchability and adjustable degradability |
Systems based on β-cyclodextrin pseudo-polyrotaxane |
Flexibility and stable mechanical characteristics |
[30] |
Smart stimuli-responsive hydrogels as advanced drug delivery systems for periodontitis treatment
Particularly for the treatment of periodontitis, hydrogel-based drug delivery methods have developed into "smart hydrogels" in recent years that may react to chemical, biological, or physical stimuli.[31]
Within the periodontal pocket, stimuli responsive hydrogels can undergo reversible phase transitions between the solid and solution phases.
Based on the type of trigger they respond to, Smart hydrogels can be classified to
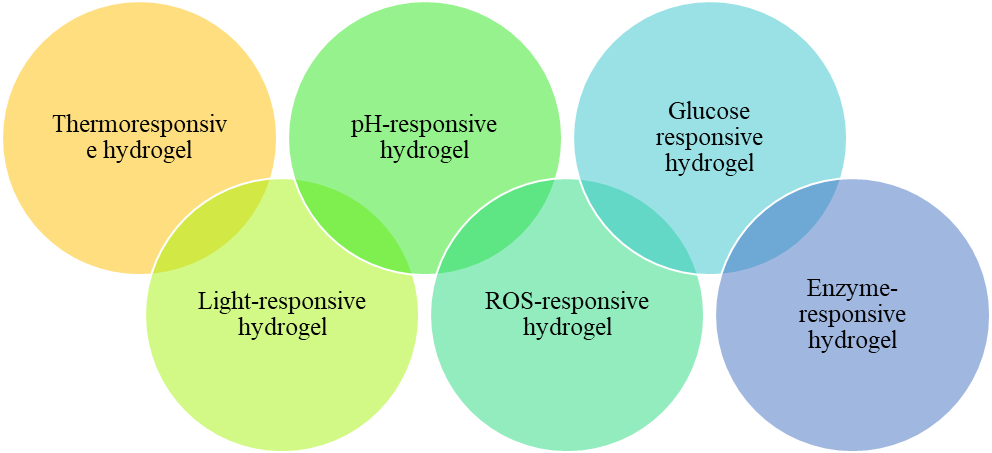
Figure 4: Smart stimuli responsive hydrogels.
At the low temperature, Thermo-responsive hydrogels are liquid, at which they are injected into periodontal pockets, respond in situ, undertake a sol-gel change when the oral environment's temperature is stimulated. The crucial element that controls the phase transition of thermo-responsive hydrogels is a low sol-gel transition temperature (LCST). Because of their decreased LCST, several polymers—like CS, curdlan, and poloxamer—are frequently used in thermo-responsive hydrogels.
CS, also known as a cationic copolymer, is a straight chain cationic deacetylated polysaccharide made up of 2-acetylamino-2-deoxyglucose-D-glucoside (0–50%) and 2-amino-2-deoxyglucose (60–100%).[32]
The molecular weight and level of deacetylation of CS determine its uses. Increased acetylation lowers the sol–gel transition temperature and facilitates hydrogel formation by encouraging physical crosslinking between CS chains.
Thermo-responsive CS hydrogels are often made by mixing CS with β-glycerophosphate (β-GP), which allows for gelation at body temperature (37 °C) via hydrogen bonding and hydrophobic interactions. These systems are extensively employed in biomedical applications, particularly in the treatment of periodontitis.
Bioactive substances like erythropoietin, aspirin, and exosomes have been delivered using CS/β-GP hydrogels, which offer prolonged release, lower inflammation, and encourage tissue regeneration. While hyaluronic acid improves mechanical strength, adhesion, and drug release control, gelatin reduces gelation time and increases injectability.
All things considered, CS-based thermoresponsive hydrogels are promising injectable solutions for periodontal regeneration and regulated medication delivery.[33]
Curdlan is a naturally occurring bacterial polysaccharide composed of β-1,3-linked glucose units. Without the use of chemical crosslinkers, it can be heated to create gels. It is beneficial for biomedical applications like periodontal therapy because it can produce a reversible gel (~55 °C) or a stable, non-reversible gel (~80 °C) depending on the temperature.[34]
Tong et al. created a curdlan-based hydrogel in conjunction with the antibacterial medication chlorhexidine acetate and the photothermal agent polydopamine (PDA) for periodontal therapy.[35] PDA transforms light into heat when exposed to near-infrared (NIR) light, raising the hydrogel's temperature above 40 °C and to roughly 58 °C in 50 seconds. After repeated light exposure, this heat causes regulated medication release and has a potent antibacterial action that eliminates around 74% of Staphylococcus aureus with little tissue damage.
Additionally, the composite hydrogel demonstrated low swelling, structural stability, good water retention, and biocompatibility with periodontal ligament cells. A synergistic antibacterial effect is produced when photothermal heating and antimicrobial medication release are combined.
In conclusion, curdlan-based photothermal hydrogels provide a focused and efficient method of treating periodontal diseases by enabling regulated, on-demand medication release under NIR stimulation.[35]
Poloxamers, sometimes referred to as poloxamer 407 and poloxamer 188, are synthetic polyoxyethylene–polyoxypropylene block copolymers. The lower critical solution temperature (LCST) and the upper critical solution temperature (UCST) are the two crucial temperatures that define their temperature-sensitive behavior.
Within this temperature range, poloxamers form hydrogels at sufficiently high concentrations (about 20–30%). As the molecular weight rises, gel formation becomes easier, especially for poloxamers with a molecular weight of 8000 or more.
Temperature-induced molecular interactions—primarily hydrogen bonding and micelle production in aqueous solution—cause the gelation. Poloxamers are beneficial for thermoresponsive drug delivery systems because the fluid turns into a gel when heated.
A pyrophosphorylated F127 hydrogel (PF-127) containing the glycogen synthase kinase-3 (GSK-3) inhibitor 6-bromoindirubin-3′-oxime (BIO) was created by Almoshari et al. Because of their great affinity for hydroxyapatite, the mineral component of bone, pyrophosphate groups were added. Strong bone affinity was demonstrated by PF-127's extended binding to hydroxyapatite in vitro. Additionally, the change increased BIO's solubility and bioavailability.[36]
BIO may be systemically toxic, yet it possesses osteoprotective and anti-inflammatory properties. The PF-127 hydrogel's local distribution promotes periodontal bone repair while lowering systemic exposure. Studies using micro-CT and histology revealed that PF-127-BIO was more successful than other therapies at preserving alveolar bone, decreasing bone loss, and inhibiting osteoclast-mediated bone resorption. Its capacity to protect periodontal bone is demonstrated by this.
The short medication residence time caused by saliva and swallowing is one drawback of local periodontal delivery, though. Mucoadhesive polymers can be added to poloxamer 407 systems to solve this.[37] Nasra et al. produced an in situ hydrogel loaded with curcumin by combining thermoresponsive poloxamer 407 with carbomer 934, a well-known mucoadhesive acrylic polymer. At body temperature (37 °C) and physiological pH within the periodontal pocket, this formulation solidifies into a sticky gel, however it stays liquid at room temperature (gelation occurs at 28–34 °C). Mucoadhesion prolongs the duration of medication retention and enhances therapeutic efficacy.[38]
By mixing sodium alginate, methylcellulose, and poloxamer 407, Kaczmarek et al. created a thermo-responsive hydrogel matrix that encapsulated a binary mixture of dried Scutellaria baicalensis extract and CS to function as an antibacterial agent in the treatment of periodontitis. Sodium alginate, an ion-sensitive mucoadhesion polymer that can react with salivary ions to stiffen the hydrogel and extend its residence time at the site of administration, was added to reinforce the hydrogel structure of the polymer network. Because thermoresponsive hydrogels tend to be a liquid between 25 and 27ºC and thicken instantly above this temperature, the hydrogel preparation can be injected into periodontal pockets and completely fill them. Furthermore, antibacterial studies have demonstrated that this hydrogel inhibits yeast-like fungi (Candida albicans, Candida tropicalis) and gram-positive bacteria (S. aureus, Staphylococcus epidermidis, Streptococcus mutans, Actinomyces).[39]
Methyl cellulose, ethyl cellulose, hydroxypropyl cellulose, hydroxyethyl cellulose, hydroxypropyl methyl cellulose, sodium carboxymethyl cellulose, and calcium cellulose are common water-soluble cellulose ether derivatives. One quite common characteristic of this family of molecules, is the thermal gelation of aqueous solutions of water-soluble cellulose ether derivatives. The fact that the solubility of the polymer does not rise with temperature indicates that thermal gelation is an essential feature of water-soluble cellulose ether derivatives. Thermo-responsive smart hydrogels for the treatment of periodontitis can be made using the sol-gel transition principle.
Venkatesh et al. used hydroxyethyl cellulose as the matrix and Pluronic F-127 to create a thermoresponsive hydrogel with azithromycin. Pluronic F-127 and hydroxyethyl cellulose interact to strengthen the gel network and promote dehydration by increasing molecular entanglement and hydrogen bonding.
As a result, the hydrogel's durability and efficacy in treating periodontitis are enhanced and the gelation temperature is lowered.
The application of triblock copolymers in smart hydrogel systems has been thoroughly studied. When dissolved in water, these amphiphilic molecules having both hydrophilic and hydrophobic regions create spherical micelles with a core-shell structure. When the micelle volume and intermicellar attraction reach body temperature, they significantly increase and condense to create 3D network hydrogels.[40]
By reacting with anionic poly (acrylic acid), the triblock copolymer PMNT-PEG-PMNT creates a polyionic complex that resembles a flower and produces a thermally irreversible micellar structure. This combination creates an in situ redox-active injectable hydrogel (RIG) when injected into the periodontal pocket. The PMNT segment, which has redox-active side chains and may scavenge reactive oxygen species (ROS), is a crucial component of this hydrogel. Although ROS are a normal component of the immune system, too much ROS in periodontitis leads to oxidative stress, inflammation, and the production of osteoclasts, all of which cause bone loss.[41]
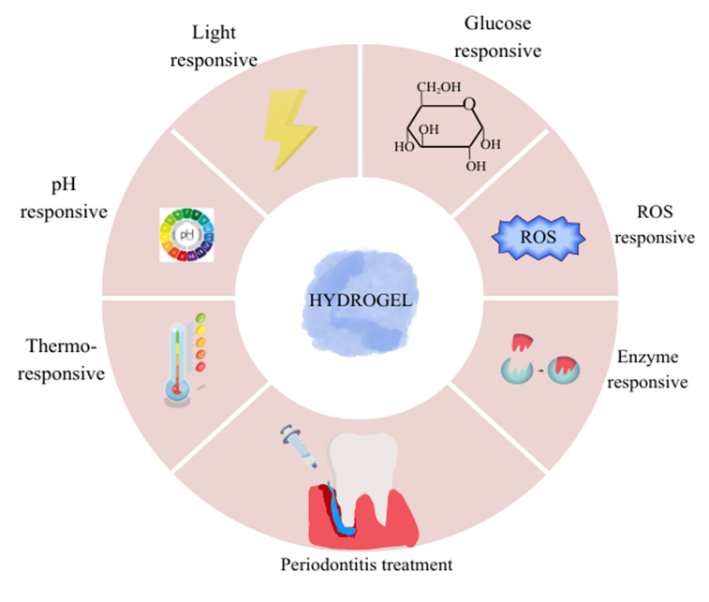
Figure 5: Stimuli-responsive hydrogels for treatment of periodontitis
Since light-responsive groups are present in the polymer backbone or side chains of these clever hydrogel systems, light-responsive hydrogel drug carrier systems regulate the release of drugs by light stimulation.[42]
Light-responsive hydrogels release drugs through two main mechanisms:
In this method, light-sensitive chemical groups within the hydrogel absorb light and undergo a chemical reaction. This reaction changes the polymer structure (such as chain arrangement, solubility, charge, or ion concentration), causing the hydrogel to swell or shrink. The volume change controls and triggers drug release.
This is more commonly used in periodontitis treatment. Light-sensitive agents absorb light (often near-infrared) and convert it into heat. The temperature rise triggers a phase transition in the hydrogel, similar to thermo-responsive systems. Once the gel reaches its transition temperature, structural changes occur, leading to controlled drug release.[42]
Zhang et al. used gold nanocages (GNCs), a phase change material (PCM), and a thermo-responsive polymer (PND) to create a light-responsive thermo-sensitive nano-antibiotic system.
Because they effectively absorb near-infrared (NIR) light and transform it into heat, GNCs function as photothermal agents. Tetracycline, for example, can be loaded into them due to their hollow structure. The PND polymer sealed the nanocage pores to stop early leakage, while PCM was added to regulate drug release at high temperatures.
Without NIR irradiation, drug release was minimal. Upon NIR exposure (808 nm), the system generated heat (up to ~75 °C), triggering controlled, on-demand drug release.
In vitro studies showed that NIR-treated TC-PCM@GNC-PND significantly reduced Staphylococcus aureus colonies due to the combined photothermal and antibiotic effects.[43]
In order to achieve highly selective drug activation, better pharmacokinetics, and improved therapeutic efficacy, pH-responsive DDS are smart systems that can take advantage of the local pathological acidic environment that initiates and exacerbates the progression of periodontitis. This technique shows excellent selectivity and biosafety since it does not require any external stimulus. From the standpoint of practical clinical translation, these benefits make pH-responsive DDS a viable and appropriate method for treating periodontitis.[44]
Since its surface amino groups can be protonated and become positively charged, Chitosan is a water-soluble cationic polyelectrolyte that can form a hydrogel after dissolving at the site of inflammation, making it an effective pH-responsive carrier in acidic conditions (pH < 5). CS is stable in neutral or alkaline media because these amino groups are deprotonated in alkaline environments, which causes the polymer to lose its charge and become insoluble.[6]
Ardiya et al. conducted a study on antibiotic loaded pH sensitive microparticle as potential site specific drug delivery system against periodontitis. Since periodontal infections are associated with localized pH changes, the pH-sensitive DOX-MPs hydrogel can release the drug more effectively in the diseased microenvironment. This targeted release improves antibacterial efficacy against biofilm-forming pathogens such as S. aureus and E. coli, while potentially minimizing unnecessary drug exposure to healthy tissues.
The system also offers advantages such as cost-effectiveness, stability, biocompatibility, biodegradability, and non-toxicity. An ex vivo biofilm model further supported its potential against bacterial biofilms.
However, additional studies—including biocompatibility, immunogenicity, mechanical stability, and in vivo animal evaluations—are necessary before clinical application in periodontal therapy.[8]
For diabetic people, hydrogels provide a way to manage periodontitis. The regulated release of medications from hydrogels may be triggered by the elevated glucose environment in diabetic periodontal tissues. Increased medication release from the hydrogels in the periodontal pockets when the concentration of glucose increases is a characteristic of glucose-responsive hydrogels. One of the main techniques for creating glucose-responsive hydrogels is the addition of GOx.[6]
Using Irgacure 2959-mediated UV crosslinking, glucose oxidase (GOx) and metronidazole (MNZ) were added to a pH-sensitive chitosan matrix to create photo-crosslinked chitosan-methacrylamide (p-CM) hydrogels. Under high-glucose circumstances, GOx produces H? ions that protonate amino groups in chitosan by converting glucose into gluconic acid. Hydrogel swelling, increased pore size, and improved drug release result from this rise in osmotic pressure and electrostatic repulsion.The pore size increased to 214.77 μm (250 mg/dL glucose) from 25.21 μm (0 mg/dL glucose). At high glucose concentrations, about 80% of metronidazole was released in 48 hours. Under high-glucose conditions, the hydrogel demonstrated stronger antibacterial activity against Porphyromonas gingivalis, suggesting its promise as a clever, biocompatible drug delivery system for the treatment of periodontitis in diabetic patients.[45]
Gingival tissue, alveolar bone, periodontal membrane, and other tooth-supporting tissues may suffer oxidative stress and damage as a result of host immunological reactions brought on by bacteria inhabiting the subgingival plaque of patients with periodontitis. Injectable hydrogels with ROS-triggered drug release behavior may be a potent therapy option for periodontal disease because oxidative stress is a key factor in the development of chronic periodontitis.[46]
Zhao et al. developed a ROS-responsive hydrogel (PBA-PEI/OD) based on the H?O?-sensitive degradation of phenylboronic acid. The hydrogel matrix was formed through Schiff base bonds between oxidized dextran and phenylboronic acid-functionalized polyethyleneimine, while doxycycline and metronidazole were incorporated via B–N coordination bonds. In the presence of H?O?, the hydrogel degraded and released nearly 100% of doxycycline within 2 days, compared to 4 days without H?O?, confirming ROS-responsive drug release.The hydrogel exhibited strong antibacterial activity against Staphylococcus aureus, Escherichia coli, and Porphyromonas gingivalis, demonstrating its potential as a smart local drug delivery system for periodontitis treatment.[47]
MMPs are crucial in the breakdown of periodontal tissue, and the degree of periodontal disease is directly connected to the amount of MMP-8 in the gingival sulcus fluid.
Using an MMP-8-sensitive cysteine-containing peptide as a crosslinker, grafted with PEG diacrylate, and loaded with minocycline, Guo et al. created an MMP-8-responsive hydrogel. The hydrogel was made to break down when MMP-8, an enzyme that is increased in periodontitis, is present. Enzyme-responsive drug release was confirmed by in vitro investigations that revealed quicker peptide release in 20 nM MMP-8 solution (full release in ~48 h) compared to PBS (144 h). When exposed to MMP-8, the hydrogel also showed robust antibacterial activity against Porphyromonas gingivalis, underscoring its promise as a targeted drug delivery mechanism for periodontal therapy.[6,48]
Future directions of Hydrogel in periodontal tissue regeneration
Although stimuli-responsive hydrogels have shown encouraging results in laboratory studies, translating these systems into predictable clinical therapies remains challenging. Periodontitis is not a simple infection but a complex inflammatory condition involving microbial imbalance, persistent immune activation, excessive reactive oxygen species (ROS), enzymatic tissue breakdown, and progressive bone loss.[6]
Because the periodontal pocket environment constantly changes in terms of pH, enzyme levels, and inflammatory mediators, designing a hydrogel that can respond accurately and consistently under these fluctuating conditions is difficult. Many currently available systems respond to only one stimulus and may therefore provide limited therapeutic control, sometimes leading to premature or burst drug release.[6]
For successful clinical use, hydrogels must remain stable within the periodontal pocket despite continuous exposure to saliva, gingival crevicular fluid, and mechanical forces generated during chewing. However, increasing mechanical strength often compromises injectability or biocompatibility. At the same time, materials that degrade too quickly may fail to provide sustained therapeutic effects. Achieving the right balance between durability, controlled degradation, and effective drug diffusion remains a key obstacle in material design.
Periodontal healing occurs in stages, beginning with infection control, followed by inflammation resolution, angiogenesis, and finally regeneration of bone and ligament structures. Ideally, hydrogel systems should release therapeutic agents in a sequential and time-controlled manner to match these healing phases. However, many current systems cannot precisely regulate multi-drug release profiles. Future advancements should focus on multi-stimuli-responsive systems and hierarchical designs that enable stage-specific therapeutic delivery.[6]
True periodontal regeneration requires coordinated reconstruction of cementum, periodontal ligament, and alveolar bone. While many hydrogels effectively reduce inflammation or bacterial load, fewer systems successfully guide structural tissue regeneration. Incorporating bioactive molecules such as growth factors, stem cells, or exosomes, along with extracellular matrix-mimicking scaffolds, may enhance regenerative outcomes. Additionally, hydrogels that can modulate immune responses—such as promoting regenerative macrophage phenotypes—may further improve healing.[6]
Even though hydrogels are generally regarded as biocompatible, concerns remain regarding the long-term effects of synthetic crosslinkers, photoinitiators, nanomaterials, and degradation byproducts. Comprehensive in vivo and long-term clinical studies are essential to confirm safety and sustained regenerative benefits. Greater emphasis on naturally derived polymers and mild crosslinking approaches may help improve safety profiles and patient acceptance.[6]
Despite promising preclinical findings, only a limited number of hydrogel systems have progressed toward clinical application. Manufacturing complexity, sterilization challenges, regulatory approval for combination products, and cost constraints remain significant barriers. Simplifying fabrication processes, establishing standardized evaluation criteria, and conducting well-designed clinical trials will be crucial for successful translation into routine periodontal therapy[6].
Looking ahead,the future of hydrogel-based periodontal therapy lies in developing adaptive, multifunctional systems that can sense and respond to the local microenvironment in real time. Self-healing properties, improved adhesion, theranostic capabilities, and patient-specific responsiveness may transform hydrogels from passive drug carriers into intelligent regenerative platforms. With continued interdisciplinary collaboration and rigorous clinical validation, these advanced materials hold the potential to move periodontal treatment beyond symptom control toward predictable and personalized tissue regeneration.[6]
REFERENCES

Aparna E, Ashik T N, Muhammed Danish Haneefa, Dr. Jisha Mohanan, Stimuli Responsive Hydrogels for Periodontitis Therapy: Current Trends and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 2357-2374. https://doi.org/10.5281/zenodo.19142616
 10.5281/zenodo.19142616
10.5281/zenodo.19142616