Cancer continues to represent one of the foremost public health challenges worldwide, with conventional systemic chemotherapy constrained by its inability to discriminate between malignant and healthy tissue. Targeted drug delivery systems (TDDS) have emerged as a transformative paradigm designed to concentrate therapeutic agents selectively at tumour sites while substantially reducing off-target toxicity. This review comprehensively examines the conceptual basis, mechanistic diversity, and nanocarrier platforms that underpin modern oncological drug targeting. We explore passive and active targeting strategies, detailing the enhanced permeability and retention (EPR) effect, receptor-ligand interactions, and multi-order targeting hierarchies. Key nanocarrier categories — including liposomes, polymeric nanoparticles, magnetic nanoparticles, quantum dots, carbon nanotubes, dendrimers, aquasomes, and nanorobots — are evaluated with respect to their structural properties, drug-loading mechanisms, surface modification potential, and therapeutic applications in solid and haematological malignancies. The review further analyses monoclonal antibody-based conjugates and their clinical translation. Challenges encompassing nanoparticle stability, immunogenicity, drug-loading efficiency, and scalable manufacturing are discussed alongside prospective directions in combination nano-theranostics, vascular-targeted delivery, and personalised oncology.
Cancer constitutes a leading cause of morbidity and mortality globally, with the World Health Organization projecting a rise in annual incidence from approximately 14 million cases in 2012 to over 22 million within two decades [1]. The pathophysiology of cancer is characterised by uncontrolled cellular proliferation, evasion of apoptotic signals, angiogenic remodelling, and ultimately metastatic dissemination to distant organs, each stage presenting distinct barriers to effective pharmacological intervention [2].
Conventional chemotherapy remains the cornerstone of systemic cancer management; however, its pronounced lack of selectivity results in indiscriminate cytotoxicity toward rapidly dividing normal tissues — notably haematopoietic precursors, gastrointestinal epithelium, and hair follicles. The consequent adverse-effect burden impairs patient quality of life, necessitates dose reductions, and frequently compels treatment discontinuation, thereby undermining therapeutic outcomes [3]. Radiotherapy, although more localised, similarly damages healthy perilesional tissue and is ineffective against systemic metastatic disease [4].
These limitations have catalysed intensive research into targeted drug delivery systems, defined as formulations capable of preferentially concentrating pharmacologically active molecules at the intended site of action while minimising systemic exposure [5]. Current estimates indicate that up to 95% of candidate therapeutics in early development possess suboptimal pharmacokinetic or biopharmaceutical profiles, underscoring the urgency of novel delivery strategies [4]. The theoretical advantages of TDDS include improved therapeutic indices, reduced effective dosing requirements, prolonged drug circulation half-lives, and the capacity to exploit tumour-specific molecular markers for precision targeting [2].
Carrier systems under investigation span a broad structural spectrum: soluble macromolecular carriers (modified plasma proteins, monoclonal antibodies, peptide conjugates), cellular vehicles (erythrocyte ghosts, neutrophils, fibroblasts), and particulate platforms (liposomes, polymeric nanoparticles, microspheres, dendrimers, carbon nanotubes, magnetic nanoparticles, quantum dots, and nanorobots). Each category presents distinct pharmacokinetic behaviour, drug-loading capacity, surface engineering potential, and biological interaction profiles [6].
2. Rationale for Targeted Drug Delivery in Oncology
The principal impetus for developing TDDS in oncology stems from the stark disparity between systemic drug exposure and therapeutic effect at the tumour site. Conventional intravenous administration distributes drug molecules throughout the entire vascular compartment, subjecting healthy organs to concentrations comparable to those reaching neoplastic tissue [3]. In contrast, a precisely engineered delivery system can exploit the unique molecular and physiological characteristics of solid tumours — including abnormal vascular architecture, acidic interstitial pH, elevated interstitial fluid pressure, and overexpressed surface receptors — to achieve preferential accumulation and controlled drug release [7].
Furthermore, advances in molecular oncology have identified a rapidly expanding catalogue of tumour-associated antigens, overexpressed receptors, and signalling pathway components that serve as actionable molecular addresses for targeted delivery. Signal transduction pathways — including HER2/neu, epidermal growth factor receptor (EGFR), folate receptor, and integrin clusters — are differentially expressed in various malignancies and offer high-selectivity anchoring points for ligand-conjugated nanocarriers [9].
3. Classification and Mechanisms of Drug Targeting
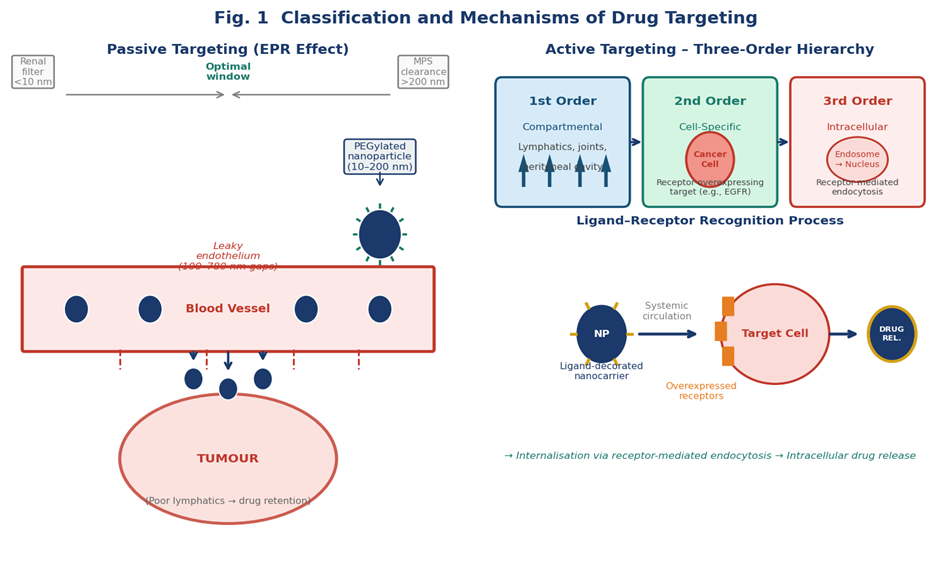
Fig. 1. Classification and Mechanisms of Drug Targeting: Passive targeting via the EPR effect (left) showing optimal nanoparticle size window (10–200 nm), PEGylated stealth carriers, and tumour extravasation; Active targeting hierarchy (right) illustrating first-, second-, and third-order targeting levels with ligand–receptor recognition process.
3.1 Passive Targeting
Passive targeting exploits the pathophysiological features intrinsic to solid tumours rather than relying on active molecular recognition. The most extensively characterised mechanism is the enhanced permeability and retention (EPR) effect, arising from two co-operative phenomena: first, tumour neovascularisation produces vessels with irregular architecture and large inter-endothelial gaps (100–780 nm), permitting preferential extravasation of macromolecular carriers; and second, deficient tumour lymphatic drainage impairs clearance of extravasated material, resulting in sustained intratumoral accumulation [7].
Exploitation of the EPR effect requires precise control over nanocarrier physicochemical properties. Particles below 10 nm are subject to rapid renal filtration, whereas those exceeding 200 nm activate mononuclear phagocyte system (MPS) clearance via opsonisation in the liver and spleen. An optimal size window of approximately 10–200 nm therefore maximises tumour accumulation [4]. Surface charge also critically influences in vivo fate: neutral or mildly negative zeta potentials minimise opsonisation and extend plasma half-life, whereas PEGylation creates a steric hydrophilic barrier that confers 'stealth' properties, markedly reducing macrophage uptake [6].
3.2 Active Targeting
Active targeting superimposes molecular recognition onto the passive distribution achieved via circulatory delivery, employing ligands conjugated to the nanocarrier surface to bind specific receptors or antigens preferentially expressed on tumour cells or tumour vasculature [5]. This interaction occurs post-extravasation and augments cellular internalisation rather than gross tumour biodistribution, which remains primarily EPR-driven [7].
Active targeting strategies are hierarchically organised into three mechanistically distinct orders:
First-order targeting confines drug carrier distribution to the capillary bed of a predetermined anatomical compartment (e.g., lymphatics, peritoneal cavity, cerebral ventricles, or synovial joints). This level of selectivity is primarily spatial rather than cellular [3].
Second-order targeting achieves selective delivery to specific cell phenotypes within a target tissue — most critically, tumour cells while sparing adjacent normal stromal cells. An example is the selective loading of cytotoxic agents into Kupffer cells of the liver via galactosyl-decorated carriers [3].
Third-order targeting achieves precision at the sub-cellular level, directing drug cargo to specific intracellular compartments (e.g., nucleus, mitochondria, lysosomes) via receptor-mediated endocytosis, membrane fusion, or pH-triggered endosomal escape mechanisms [3,8].
Table 1. Comparative Overview of Passive vs Active Targeting Strategies
|
Characteristic |
Passive Targeting |
|
Mechanism |
EPR effect; physicochemical accumulation |
|
Requirement |
Controlled nanoparticle size (10–200 nm), PEGylation |
|
Selectivity Level |
Tissue/organ (anatomical) |
|
Internalisation |
Non-specific endocytosis |
|
Limitations |
EPR heterogeneity; no sub-cellular precision |
|
Best Suited For |
Solid tumours with leaky vasculature |
|
Characteristic |
Active Targeting |
|
Mechanism |
Ligand–receptor molecular recognition |
|
Requirement |
Surface-conjugated ligand; receptor overexpression |
|
Selectivity Level |
Cell-specific to sub-cellular |
|
Internalisation |
Receptor-mediated endocytosis |
|
Limitations |
Receptor heterogeneity; potential immunogenicity |
|
Best Suited For |
Receptor-overexpressing tumours; intracellular targets |
3.3 Strategies of Drug Targeting
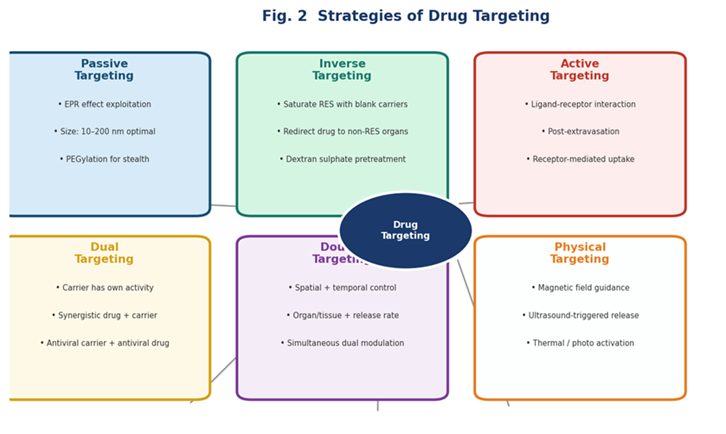
Fig. 2. Strategies of Drug Targeting: Hub-and-spoke overview showing the six major targeting strategies — Passive, Inverse, Active, Dual, Double, and Physical — centred on the unifying principle of drug targeting with their respective mechanisms and clinical applicability
Inverse Targeting: Aims to circumvent natural RES uptake by pre-saturating phagocytic capacity with blank colloidal carriers or dextran sulphate, redirecting subsequent carrier uptake toward non-RES organs [4].
Dual Targeting: Employs carrier molecules that possess intrinsic pharmacological activity in addition to their drug cargo, generating synergistic therapeutic effects [4].
Double Targeting: Integrates both spatial (organ/tissue) and temporal (controlled release rate) delivery control, enabling precision over both anatomical distribution and pharmacokinetic profile [4].
4. Desirable Properties of Targeted Drug Delivery Systems
For a carrier system to fulfil its therapeutic mandate in oncological settings, it must satisfy a demanding set of physicochemical, pharmacokinetic, and biological criteria [4]:
Table 2. Essential Properties of an Ideal Tumour-Targeted Drug Delivery System
|
Property |
Rationale |
|
Non-toxic, biodegradable, biocompatible |
Prevents carrier-induced toxicity and facilitates safe elimination |
|
Physicochemical stability (in vivo & in vitro) |
Ensures integrity during storage and systemic transit |
|
Confined, uniform capillary distribution |
Restricts drug action to target tissue/organ |
|
Predictable, controllable drug release rate |
Allows therapeutic window maintenance |
|
Drug release independent of delivery mechanism |
Prevents premature leakage triggered by carrier design |
|
Therapeutic drug payload delivery |
Ensures clinically relevant local concentrations |
|
Minimal drug leakage during transit |
Limits systemic exposure and off-target effects |
|
Biodegradable/readily eliminable carrier |
Prevents bioaccumulation; no disease-state modulation |
5. Nanocarrier Platforms in Cancer Targeted Drug Delivery
5.1 Liposomes
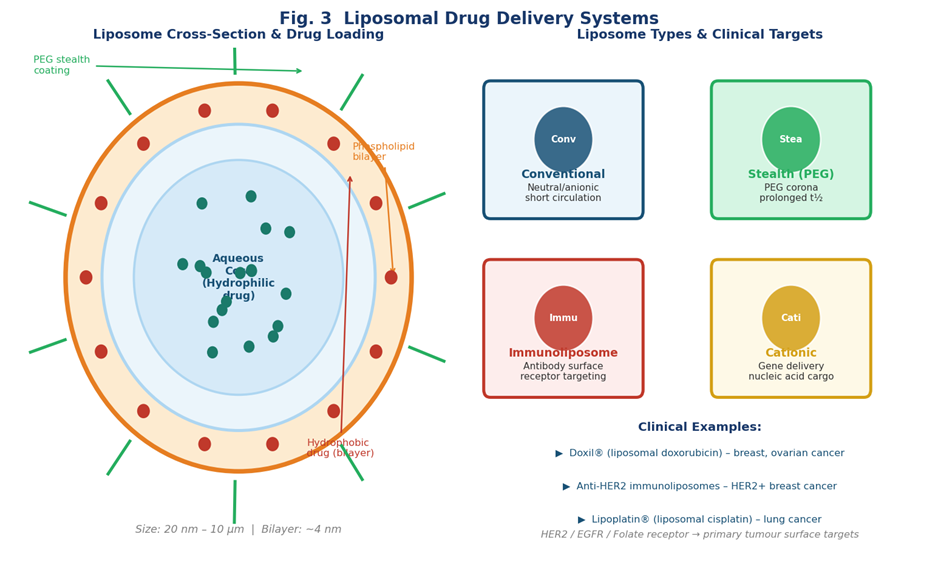
Fig. 3. Liposomal Drug Delivery Systems. (Left) Cross-sectional architecture showing the phospholipid bilayer, aqueous core containing hydrophilic drugs, hydrophobic drug intercalation in the bilayer, and PEG stealth corona. (Right) Four liposome types (Conventional, Stealth, Immunoliposome, Cationic) with clinical examples including Doxil® and anti-HER2 immunoliposomes.
Liposomes are spherical, self-assembling vesicular structures comprising one or more concentric phospholipid bilayers encapsulating an aqueous core. Their diameter ranges from approximately 20 to 10,000 nm, and their amphiphilic architecture enables simultaneous encapsulation of both hydrophilic drugs (within the aqueous compartment) and hydrophobic agents (intercalated within the lipid bilayer), conferring exceptional versatility across drug classes [6].
Four principal liposomal architectures are clinically and experimentally relevant. Conventional liposomes with neutral or anionic surface charges exhibit relatively rapid clearance by the MPS. Sterically stabilised ('stealth') liposomes display surface-grafted PEG chains that create a dynamic aqueous shield, preventing opsonin adsorption and extending circulatory half-life from hours to multiple days. Immunoliposomes incorporate monoclonal antibodies or antibody fragments on their outer surface, enabling receptor-specific binding to tumour-associated antigens such as HER2 and EGFR. Cationic liposomes carry a net positive charge that facilitates electrostatic complexation with negatively charged nucleic acids, making them particularly suited for gene delivery applications [5,6].
Clinically significant applications include liposomal doxorubicin (Doxil/Caelyx), the first FDA-approved nanomedicine, which demonstrated markedly reduced cardiotoxicity compared with free doxorubicin in breast and ovarian cancers. In HER2-overexpressing breast cancer (20–30% of cases), anti-HER2 immunoliposomes conjugated with magnetic nanoparticles have been employed for hyperthermic tumour ablation [5].
5.2 Polymeric Nanoparticles
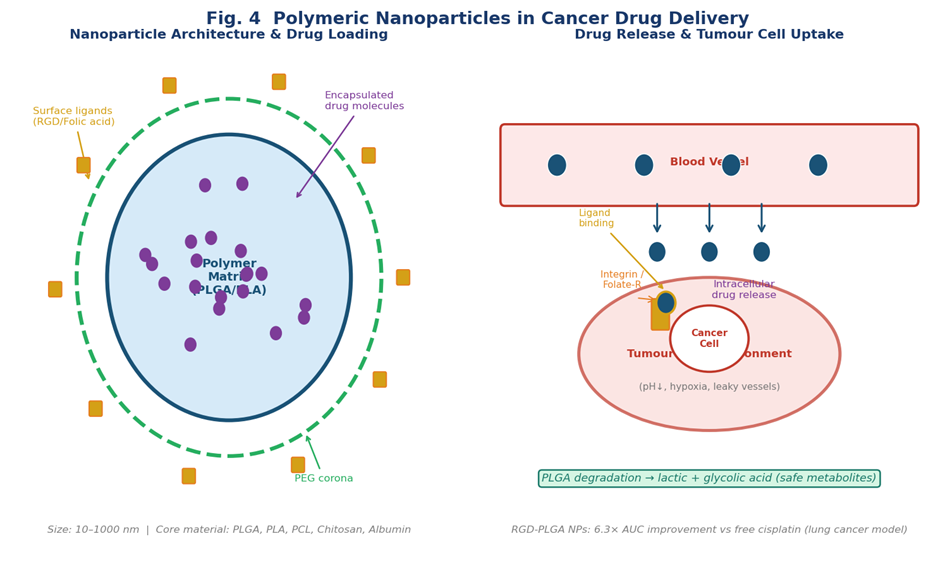
Fig. 4. Polymeric Nanoparticles in Cancer Drug Delivery. (Left) Nanoparticle architecture showing PLGA/PLA polymer matrix with encapsulated drug molecules, PEG corona, and surface-conjugated RGD/Folic acid ligands. (Right) Tumour-targeting pathway illustrating EPR-mediated extravasation, receptor-mediated cellular uptake, and PLGA biodegradation.
Polymeric nanocarriers represent a powerful and highly adaptable platform for tumour-targeted chemotherapy delivery. These systems offer substantial advantages including superior physiological stability, higher drug encapsulation efficiency for a broader spectrum of molecules (hydrophobic and hydrophilic drugs, proteins, DNA, and RNA), ease of surface functionalisation, and scalable manufacturing compatible with GMP standards [15].
Drug molecules are incorporated via adsorption onto particle surfaces, encapsulation within the polymer matrix, or covalent conjugation. Commonly employed polymers include poly(lactic-co-glycolic acid) (PLGA), polylactic acid (PLA), polycaprolactone (PCL), PLGA–PEG block copolymers, and natural polymers such as alginate, chitosan, gelatin, and albumin [15].
PLGA merits particular attention as an FDA-approved biomaterial. RGD peptide-conjugated PLGA nanoparticles developed for integrin-targeted cisplatin delivery in lung cancer demonstrated a 6.3-fold elevation in area under the plasma concentration–time curve (AUC) relative to conventional injection, along with negligible systemic toxicity and minimal pulmonary tissue damage [15].
5.3 Magnetic Nanoparticles
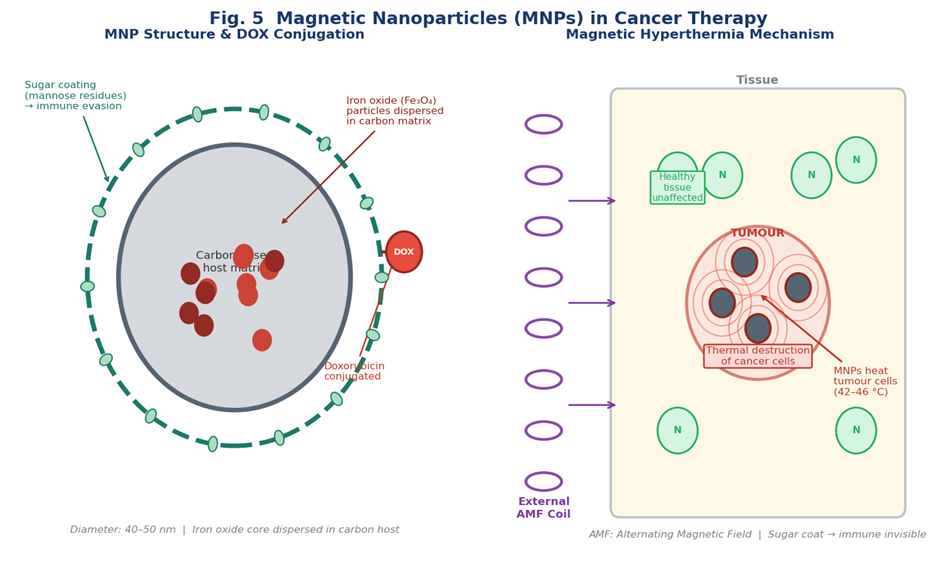
Fig. 5. Magnetic Nanoparticles (MNPs) in Cancer Therapy. (Left) CMNP architecture showing iron oxide (Fe?O?) particles dispersed in carbon matrix, sugar (mannose) coating for immune evasion, and doxorubicin conjugation. (Right) Magnetic hyperthermia mechanism: AMF coil generates alternating field, MNPs heat to 42–46°C selectively destroying tumour cells while healthy tissue remains unaffected.
Magnetic nanoparticles (MNPs) occupy a unique position in oncological TDDS by enabling physical, field-directed guidance to tumour sites. Carbon magnetic nanoparticles (CMNPs) — spherical structures of 40–50 nm diameter consisting of iron oxide particles dispersed within a carbon-based host matrix — have demonstrated efficacy as drug delivery vehicles when conjugated with doxorubicin (CMNP-DOX conjugates) [5].
Under the influence of an external alternating magnetic field, sugar-coated MNPs generate localised hyperthermia sufficient to induce tumour cell death through thermal denaturation of proteins and disruption of cell membrane integrity, while surrounding normothermic healthy tissue remains unaffected — a therapeutic modality known as magnetic hyperthermia [5]. Beyond hyperthermia, MNPs serve as contrast agents for MRI, enabling simultaneous diagnostic imaging and therapeutic delivery — a theranostic strategy of growing clinical relevance [7].
5.4 Quantum Dots
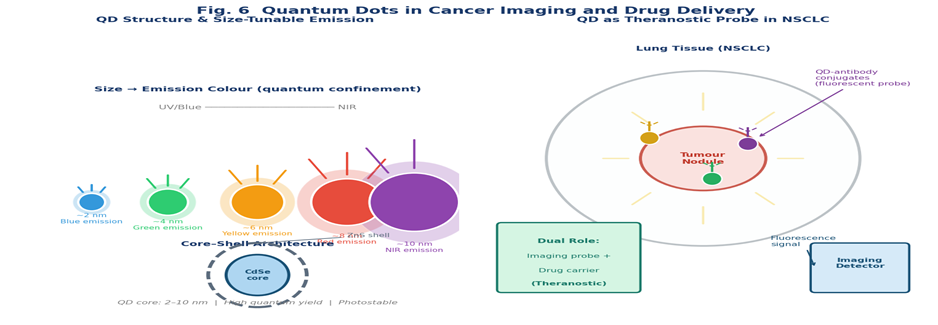
Fig. 6. Quantum Dots in Cancer Imaging and Drug Delivery. (Left) Size-tunable emission spectrum from blue (~2 nm) to NIR (~10 nm) via quantum confinement; Core–shell (CdSe/ZnS) architecture. (Right) Theranostic application in NSCLC: QD–antibody conjugates accumulate in lung tumour nodule enabling simultaneous fluorescence imaging and drug delivery (dual theranostic role).
Quantum dots (QDs) are semiconductor nanocrystals with diameters typically in the range of 2–10 nm that exhibit quantum confinement effects, resulting in discrete, size-tunable optical and electronic properties distinct from bulk semiconductor materials. Their ability to confine the motion of conduction band electrons, valence band holes, and exciton pairs in all three spatial dimensions produces exceptional photostability and fluorescence quantum yields far exceeding conventional organic fluorophores [7].
In oncological drug delivery, QDs serve dual roles as both imaging probes and drug carriers. Surface functionalisation enables conjugation with tumour-targeting ligands, antibodies, or aptamers, facilitating real-time fluorescence tracking of drug biodistribution and intracellular trafficking. Their applications extend beyond oncology to tissue engineering, catalysis, filtration technologies, and solid-state quantum computation [3,7].
5.5 Dendrimers
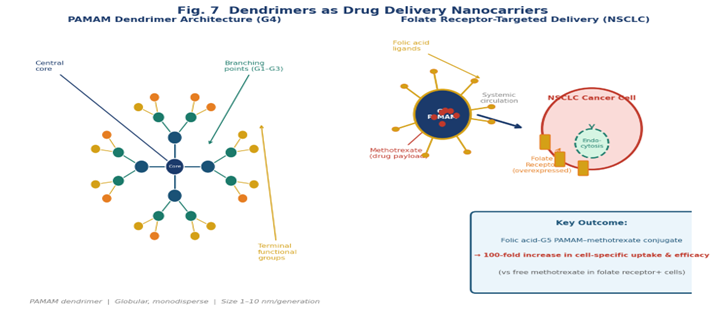
Fig. 7. Dendrimers as Drug Delivery Nanocarriers. (Left) G4 PAMAM dendrimer tree architecture showing the central core, iteratively branched G1–G3 dendritic arms, and densely functionalised peripheral terminal groups capable of drug loading. (Right) Folate receptor-targeted delivery in NSCLC: folic acid-conjugated G5 PAMAM dendrimers bearing methotrexate achieve 100-fold efficacy increase via receptor-mediated endocytosis.
Dendrimers are precisely engineered, three-dimensional, hyperbranched macromolecules characterised by a symmetric branching architecture emanating from a central core molecule through iteratively layered branching points (generations) to densely functionalised peripheral groups [13]. Their multivalent surface and internal cavity architecture confer versatile drug loading by covalent conjugation, electrostatic complexation, hydrophobic encapsulation, and physical entrapment.
Polyamidoamine (PAMAM) dendrimers have been extensively characterised as gene and oligonucleotide delivery vectors. A landmark study demonstrated that folic acid-conjugated G5 PAMAM dendrimers increased cell-specific uptake and the in vitro and in vivo efficacy of conjugated methotrexate by 100-fold through folate receptor-mediated internalisation in cancer cells overexpressing this receptor [13]. Surface modification strategies employing neutral hydroxyl, acetyl, or anionic carboxyl groups effectively mitigate cationic cytotoxicity while preserving targeting capability [13].
5.6 Carbon Nanotubes
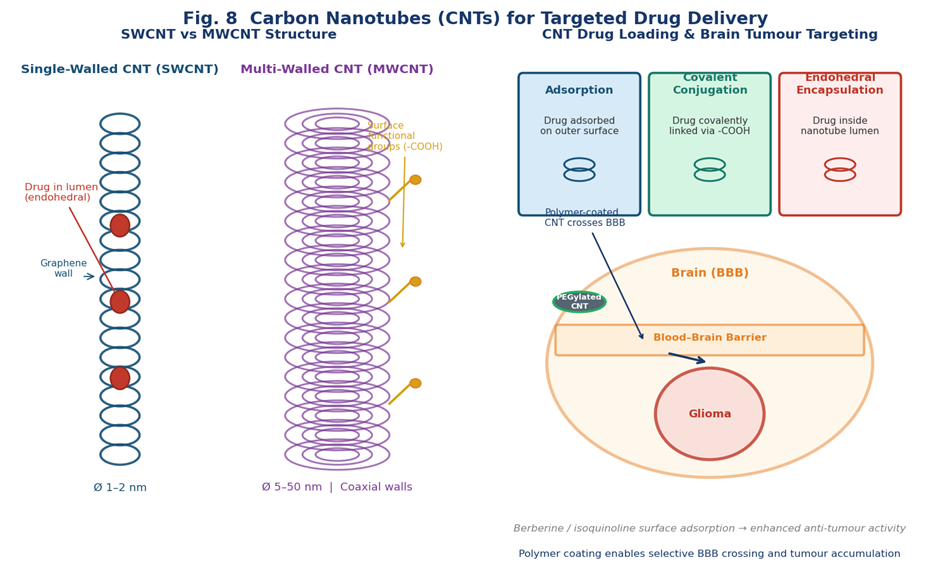
Fig. 8. Carbon Nanotubes (CNTs) for Targeted Drug Delivery. (Left) Structural comparison of SWCNT (1–2 nm, drug in lumen) vs MWCNT (5–50 nm, coaxial walls, surface functionalisation). (Right) Three drug-loading modes (adsorption, covalent conjugation, endohedral encapsulation) and polymer-coated CNT crossing the blood–brain barrier for glioma-targeted drug delivery.
Carbon nanotubes (CNTs), also referred to as buckytubes, are cylindrical allotropes of carbon consisting of one or more coaxially nested graphene sheets rolled into seamless cylinders with diameters on the order of 1–50 nm [14]. CNTs possess extraordinary physicochemical attributes — tensile strength exceeding steel, exceptional thermal and electrical conductivity, and large specific surface area — that render them attractive multifunctional carriers.
In drug delivery, CNTs interact with therapeutic molecules through three primary mechanisms: non-covalent surface adsorption, covalent attachment to functionalised surface groups (carboxylic acid, amine), and endohedral encapsulation within the nanotube lumen. Polymer-coated CNTs have demonstrated selective accumulation in brain tumours following systemic administration, with surface-adsorbed alkaloids such as berberine and isoquinoline showing enhanced anti-tumour activity in preclinical models [8].
5.7 Nanorobots (Nanobots)
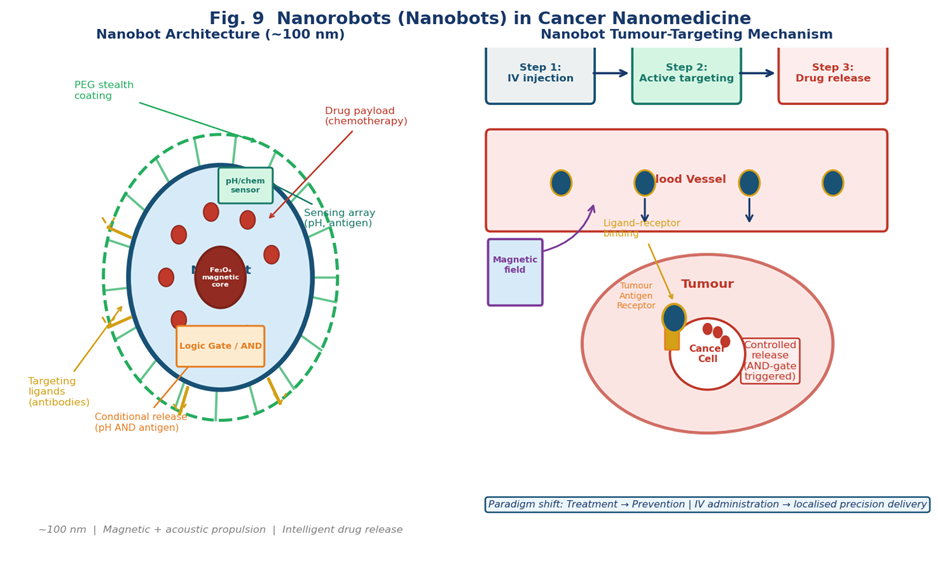
Fig. 9. Nanorobots (Nanobots) in Cancer Nanomedicine. (Left) Modular nanobot architecture (~100 nm): magnetic Fe?O? propulsion core, drug payload, PEG stealth shell, antibody targeting ligands, pH/antigen sensing array, and AND-logic gate for conditional drug release. (Right) Three-step mechanism: IV injection → active targeting via magnetic guidance and ligand–receptor binding → controlled intracellular drug release.
Nanorobots represent the frontier of nanomedicine, integrating principles of nanotechnology, synthetic biology, and robotics engineering into autonomous or remotely actuable nano-scale machines capable of targeted navigation, sensing, and drug delivery within living organisms [12].
The modular architecture of nanorobots integrates multiple functional components: a drug payload compartment, targeting ligands (antibodies, aptamers), a stealth shell (PEG coating), propulsion and steering mechanisms (magnetic cores, acoustic receivers), sensing arrays (chemical sensors, pH-responsive elements), and integrated logic circuits enabling disease microenvironment-conditional drug release [12]. Critical developmental challenges include inefficiency of positional nano-assembly, limitations of DNA-based approaches, and biosafety concerns attendant upon bacteria-integrated designs [12].
5.8 Aquasomes
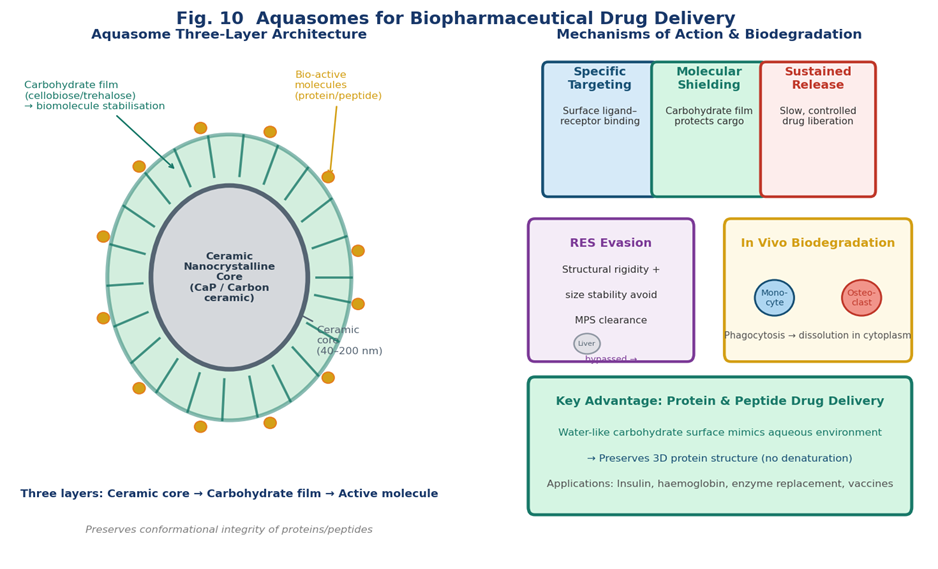
Fig. 10. Aquasomes for Biopharmaceutical Drug Delivery. (Left) Three-layer architecture: ceramic nanocrystalline core (CaP/carbon ceramic), polymerised carbohydrate film (cellobiose/trehalose), and adsorbed bioactive molecules. (Right) Mechanisms of action: specific targeting, molecular shielding, and sustained release; RES evasion via structural rigidity; in vivo biodegradation by monocytes/osteoclasts; key advantage of preserving protein/peptide conformational integrity.
Aquasomes are three-layered nanoparticulate carriers consisting of a solid ceramic nanocrystalline core (typically calcium phosphate or carbon ceramic), a stabilising carbohydrate film (e.g., cellobiose, pyranose sugars, trehalose) polymerised onto the core surface, and an outer layer bearing the adsorbed or conjugated biochemically active molecule [16].
Their water-like surface chemistry of the carbohydrate film preserves the conformational integrity and biochemical activity of delicate biomolecules — a critical advantage for protein and vaccine delivery [16]. Drug release is governed by surface chemistry through a combination of specific molecular targeting, molecular shielding effects, and sustained zero-order release kinetics. Due to their size and structural rigidity, aquasomes evade RES clearance more effectively than soft nanocarriers under equivalent surface conditions [16].
6. Comparative Analysis of Nanocarrier Platforms
Table 3. Comparative Summary of Major Nanocarrier Platforms
|
Nanocarrier |
Key Advantages |
Primary Limitations |
|
Liposomes |
Biodegradable; dual encapsulation; clinically approved; surface modifiable |
Short shelf-life; batch variation; RES clearance without PEGylation |
|
Polymeric NPs |
High stability; tuneable release; GMP scalable; broad payload flexibility |
Organic solvent residues; immunogenicity of synthetic polymers |
|
Magnetic NPs |
Field-directed targeting; hyperthermia; MRI theranostics |
Iron toxicity concerns; limited payload; external field dependence |
|
Quantum Dots |
Superior photostability; size-tuneable emission; multiplexed imaging |
Heavy metal toxicity (Cd, Pb); potential genotoxicity; limited drug loading |
|
Dendrimers |
Precise architecture; multivalent surface; internal cavity loading |
Cationic toxicity; batch inconsistency; synthesis complexity |
|
Carbon Nanotubes |
Large surface area; multiple loading modes; intrinsic conductivity |
Biopersistence concerns; pulmonary toxicity; dispersibility issues |
|
Nanorobots |
Autonomous navigation; programmable release; multi-function |
Pre-clinical stage; assembly challenges; biosafety unclear |
|
Aquasomes |
Protein/peptide integrity preservation; sustained release; RES evasion |
Limited drug loading for small molecules; complex surface chemistry |
|
Monoclonal Abs / ADC |
Exquisite target specificity; FDA-approved platforms; ADCC activity |
Immunogenicity (murine); antigen modulation; manufacturing cost |
7. Challenges and Barriers to Clinical Translation
Despite remarkable advances in nanocarrier design, the gap between preclinical promise and clinical utility remains substantial. Several systemic challenges constrain progress across all platforms.
EPR Effect Variability: The EPR effect is highly heterogeneous in human patients, varying by tumour type, vascularisation density, interstitial fluid pressure, and prior therapy, undermining predictive validity of murine biodistribution data [10].
Protein Corona: Upon systemic administration, nanoparticles are rapidly enveloped by serum proteins forming a 'corona' that fundamentally alters their surface identity, often abrogating targeting ligand functionality and redirecting biodistribution toward MPS organs [10].
Drug Loading and Release: Achieving simultaneously high drug encapsulation efficiency and precisely controlled release remains technically challenging. Small particle size and large surface-to-volume ratios promote burst release [4].
Regulatory Complexity: The physicochemical complexity of nanocarrier formulations complicates regulatory approval pathways regarding batch-to-batch reproducibility, sterility, and shelf-life stability [10].
8. Future Perspectives
The trajectory of cancer-targeted drug delivery converges toward several transformative directions. Stimuli-responsive nanocarriers engineered to release drug payload in response to endogenous tumour microenvironmental cues — acidic pH, elevated glutathione, tumour-specific enzymes, or elevated temperature — represent a logical evolution beyond passive EPR-dependent accumulation [8]. Combination nano-theranostics integrating diagnostic imaging functionality with therapeutic drug delivery within a single multifunctional nanoplatform enable real-time monitoring of carrier biodistribution and treatment response [7].
The next few years will witness particular emphasis on the development of systems which can not only recognise specific targets on cancer cells but also are capable of efficiently internalising into the cells. Combination targeting approaches, utilising specific molecular addresses on the vascular endothelium, magnetic field guidance, and ultrasound, are emerging concepts which hold immense promise for drug targeting in cancer therapy [2].
CONCLUSION
Targeted drug delivery systems represent a paradigm transformation in cancer pharmacotherapy, addressing the fundamental selectivity limitations of conventional chemotherapy through the rational exploitation of tumour physiology, molecular biology, and materials engineering. This review has systematically documented the mechanistic diversity underlying passive and active targeting strategies, the physicochemical and biological requirements that define effective carrier design, and the expanding landscape of nanocarrier platforms advancing toward clinical implementation.
Liposomes have demonstrated the most mature clinical translation, with multiple approved products establishing proof of concept for improved therapeutic indices in haematological and solid malignancies. Polymeric nanoparticles, magnetic nanoparticles, dendrimers, and carbon nanotubes offer complementary advantages suited to specific drug types and tumour targets. Quantum dots and nanorobots represent the technological frontier, with transformative potential tempered by unresolved biosafety and manufacturing challenges. Monoclonal antibody–drug conjugates have achieved the most reliable clinical translation of active targeting, with multiple approved products and an extensive clinical trial pipeline.
With continued integration of molecular tumour profiling, advanced materials engineering, and rigorous clinical evaluation frameworks, targeted drug delivery systems hold compelling promise to meaningfully improve survival outcomes and quality of life for cancer patients.
Conflicts of Interest: The authors declare no conflict of interest.
Funding: This research received no specific grant from any public, commercial, or not-for-profit funding agency.
REFERENCES


Saranya Sankar, Shivprasad Sanjay Dhage, Targeted Drug Delivery Systems for Cancer Therapy: Mechanisms, Nanocarrier Platforms, and Emerging Clinical Strategies , Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 788-800. https://doi.org/10.5281/zenodo.19421711
 10.5281/zenodo.19421711
10.5281/zenodo.19421711
