Amity Institute of Pharmacy, Amity University Uttar Pradesh, Lucknow Campus, Lucknow - 226028, Uttar Pradesh, India
Skin wound healing remains a global healthcare challenge, particularly when complicated by infections. Traditional wound dressings fail to address the dynamic physiological environment of infected wounds, where fluctuations in temperature, pH, and microbial activity interfere with tissue repair. Smart biomaterials such as hydrogels have emerged as promising candidates due to their ability to mimic extracellular matrices, maintain moist conditions, and allow controlled drug release. Among them, stimuli-responsive hydrogels, especially temperature- and pH-sensitive hydrogels, have attracted considerable attention for infected wound healing applications. These hydrogels undergo phase transitions in response to environmental cues, enabling on-demand drug release, antibacterial activity, and promotion of tissue regeneration. This review provides a comprehensive overview of temperature- and pH-responsive hydrogels for wound healing, their mechanisms, design strategies, advantages, limitations, and future prospects. Special emphasis is placed on the role of infection-induced pH changes and thermal variations as triggers for responsive drug delivery systems.
Wound healing is a highly dynamic and complex physiological process aimed at restoring the integrity of damaged skin and underlying tissues [1]. The process involves a series of well-coordinated stages including hemostasis, inflammation, proliferation, and remodeling [2]. Any disruption in these stages, particularly due to microbial infection, can significantly delay healing and lead to chronic wounds [3]. Infected skin wounds are a common clinical challenge, associated with prolonged inflammation, bacterial colonization, and impaired tissue regeneration [4]. Traditional wound care approaches, including gauze dressing and ointments, often fail to provide effective protection against infection while maintaining an optimal healing environment [5].Hydrogels have emerged as a promising class of biomaterials for wound management due to their unique physicochemical properties [6]. These three-dimensional, hydrophilic polymer networks can absorb large amounts of water or biological fluids, maintaining a moist environment at the wound site that facilitates cell migration, angiogenesis, and tissue repair [7]. In addition to their inherent biocompatibility and flexibility, hydrogels can be engineered to serve as controlled-release platforms for therapeutic agents such as antibiotics, growth factors, and anti-inflammatory drugs, making them highly suitable for infected wound care [8].The incorporation of stimuli-responsive features in hydrogels further enhances their therapeutic potential [9]. Stimuli-responsive, or “smart,” hydrogels can undergo physical or chemical changes in response to environmental cues such as temperature, pH, ionic strength, or specific enzymes [10]. In the context of wound healing, temperature and pH are particularly relevant stimuli because infected wounds often exhibit elevated local temperature due to inflammation and altered pH due to bacterial colonization and tissue damage [11]. Despite these advancements, challenges remain in optimizing the hydrogel formulation to balance mechanical properties, swelling behavior, drug release kinetics, and biodegradability [12]. Similarly, achieving a sol-gel transition close to human body temperature without compromising mechanical integrity is critical for practical applications [13]. Therefore, careful selection of polymers, crosslinkers, and drug loading strategies is essential for developing clinically effective dual-responsive hydrogels [14].
Wound healing is a complex and dynamic biological process that involves several overlapping but separate stages[15]. This highly monitored process includes intricate relationships between cytokines, growth factors, coagulation factors, and various components of vascular networks and connective tissue[16].Figure 2a illustrates how the hemostasis phase begins as soon as an injury occurs, during which time platelets clump together and release clotting factors to create a fibrin network that stops excessive bleeding [17]. The inflammatory response that follows (Figure 2b)involves neutrophils and macrophages infiltrating the wound site to eradicate infections and remove cellular debris[18]. Following this, fibroblasts deposit extracellular matrix (ECM) components, keratinocytes aid in re-epithelialization, and endothelial cells stimulate angiogenesis during the proliferation phase—all of which are critical for tissue regeneration[19].Figure 2c Ultimately, the remodeling phase ensures appropriate wound closure and functional recovery by strengthening newly created tissue through collagen production, crosslinking, and reorganization[20].Figure 2d illustratespathophysiological processes and clinical results, wounds can be categorized as either acute or chronic[21]. The concentration of particular bioactive components and the biochemical environment at the wound site serve as the primary differentiators between these groups[22]. Acute wounds are typically caused by burns, trauma, or surgical incisions. They typically heal in a few weeks after undergoing the appropriate stages of wound healing [23]. The immune cells in these wounds efficiently eliminate pathogens and necrotic debris, resulting in a well-regulated inflammatory response that permits the ensuing phases of proliferation and remodeling to proceed without major disruption [24]. Growth factors that promote fibroblast migration, collagen synthesis, and angiogenesis include platelet-derived growth factor, vascular endothelial growth factor (VEGF), and transforming growth factor β [25].Consequently, acute wounds typically heal with little scarring and quickly restore the afflicted tissue's functionality [26]. On the other hand, persistent wounds like diabetic foot ulcers and infected wounds frequently do not advance through the normal wound healing cascade, being stuck in the inflammatory phase and impairing tissue regeneration [27].Persistent infection or compromised immunological control, which disrupt the equilibrium between inflammation and tissue regeneration, is a significant contributing factor [28]. Ultimately, this imbalance hinders fibroblast activity and angiogenesis by causing a persistent increase in inflammatory cytokines like tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), as well as the suppression of vital growth factors like VEGF and epidermal growth factor (EGF) [29,30].Tissue regeneration is further hampered by the excessive breakdown of extracellular matrix (ECM) components caused by matrix metalloproteinases (MMPs) overexpression [31].One of the more difficult subtypes of chronic wounds is diabetic ulcers.
Microvascular dysfunction is exacerbated by chronic hyperglycemia, which also slows angiogenesis and damages endothelial function.It also changes the behavior of macrophages and neutrophils, which impairs immunological responses.Decreased keratinocyte migration, decreased collagen deposition, and poor granulation tissue formation are common features of diabetic wounds, all of which lead to partial or delayed re-epithelialization[29]. Furthermore, peripheral neuropathy and ischemia reduce wound sensibility, perfusion, and repair ability, while the buildup of advanced glycation end products and increased oxidative stress accelerate tissue damage [31].Stimuli-responsive hydrogels for diabetic wound healing frequently include enzyme-sensitive degradation pathways and ROS scavenging mechanisms to reduce oxidative stress and facilitate on-demand drug release. For example,a hexapeptide with methionine residues in a supramolecular hydrogel system demonstrates both ROS-responsive degradation and ROS-scavenging capacity.Met residues are oxidized when exposed to high ROS levels, which causes hydrogel disintegration and the consequent release of bioactive compounds or encapsulated medications.This breakdown process actively lowers local oxidative stress in addition to facilitating regulated release [32].Burn injuries can be acute at first, but they frequently become chronic because of the increased risk of infection and poor healing caused by microbial colonization and the breakdown of the skin barrier[33].Pathogens can create biofilms, which are intricate microbial communities covered in an extracellular matrix that they build on their own to protect them from immune clearance and antimicrobial drugs, when bacteria invade an area [34].These biofilms release toxins and proteolytic enzymes that support in tissue deterioration, increase oxidative stress, and prolong inflammation.Biofilm production uses native extracellular matrix (ECM) components as collagen, fibronectin, and fibrinogen as attachment sites [35].Moreover, oxidative damage to cellular structures is caused by elevated reactive oxygen species (ROS) and sustained neutrophil activity, which hinders fibroblast and keratinocyte migration [36].Stimuli-responsive hydrogels that provide physical antibacterial mechanisms or controlled antibacterial agent release are especially beneficial for infected wounds.Alkaline shifts linked to bacterial infection can be detected using pH-responsive hydrogels, which can then release antimicrobial drugs in a site-specific way [37].Additionally, light-responsive or enzyme-degradable hydrogels with photothermal agents incorporated have shown strong biofilm-disrupting action while reducing systemic toxicity [38]. In general, excessive proteolysis, bacterial colonization, and the persistence of inflammatory mediators all work together to delay wound closure and raise the risk of tissue necrosis and systemic infection [40].These pathophysiological differences among wound typesfrom acute surgical wounds to long-term diabetic, infected, or burn woundsemphasize the necessity of specialized treatment approaches.To overcome these obstacles, focused therapies that enhance cellular activity, control inflammation, and encourage extracellular matrix remodeling are needed. Stimuli-responsive hydrogel-based dressings have enormous potential in these domains [41].
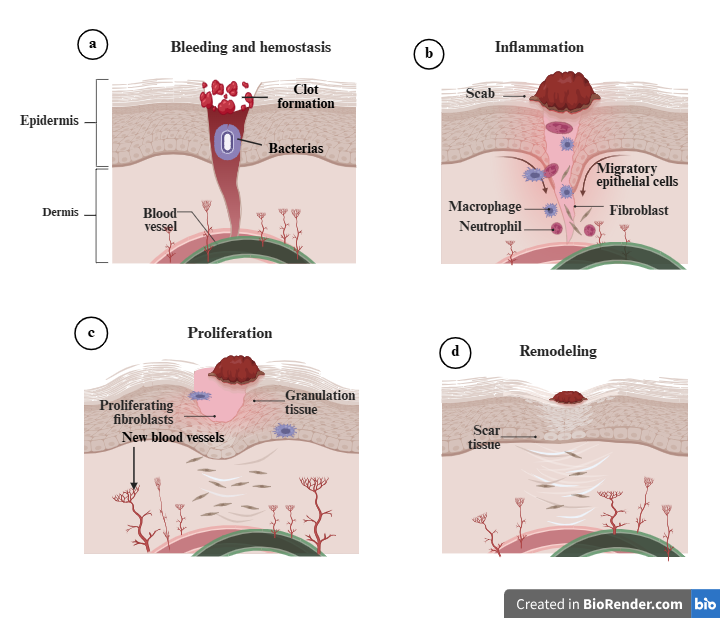
Figure 1:Schematic representation of the four main stages of wound healing: (a) Bleeding and hemostasis, where a clot forms to stop bleeding and bacteria may be present; (b) Inflammation, characterized by the formation of a scab and the migration of immune cells (macrophages, neutrophils) and fibroblasts to the wound site; (c) Proliferation, involving the formation of granulation tissue, new blood vessels, and proliferating fibroblasts to fill the wound; and (d) Remodeling, where the wound matures and scar tissue forms.
Hydrogels are three-dimensional networks of polymers that can absorb a lot of water or biological fluids without disintegrating.Often called "water gels," they have a gel-like consistency and can be made from synthetic materials like polyacrylamide and polyethylene glycol or natural polymers like alginate, collagen, and chitosan[42,43]. Hydrogel dressings are made up of hydrophilic, swelling, and insoluble materials and come in gel and film forms.Their 70–90% water content allows them to efficiently absorb biological fluids at damage sites, making them appropriate for wound treatment[44]. They are widely acknowledged as successful wound dressings due to their biocompatibility, adjustable architectures, potential for functionalization, and flexible production.Hydrogel-based scaffolds that interact with biological molecules or cells for tissue regeneration are the focus of recent developments in polymer research.By promoting vital wound-healing processes like angiogenesis, epidermal restoration, collagen production, and seamless tissue integration, these scaffolds reduce scarring[45]. Because they replicate the natural tissue environment, effectively distribute therapeutic drugs, and react to a variety of stimuli, hydrogels are essential in the treatment of wounds.They guarantee skin hydration due to their hydrophilic nature, which speeds up the healing process[46]. Radiation wounds, dry wounds, minor burns, and chronic diabetic wounds can all be effectively treated with the wet, antibacterial environment that cross-linked, three-dimensional porous hydrogels can create by absorbing water hundreds of times their dry weight.They are perfect for advanced wound care because of their oxygen permeability, ability to load drugs, and ease of topical application.Furthermore, hydrogel dressings are usually transparent, making it possible to monitor wounds without removing them[47]. The different types and characteristics of hydrogel dressings used in wound healing are summarized in Table 1.
Table 1 Exploring Hydrogel-based approaches for wound healing
|
Polymer |
Models used for study |
Drug |
Outcome of Study |
Reference |
|
Polyvinyl alcohol, Polyvinylpyrrolidone |
In vivo study on male Sprague–Dawley (SD) rats |
Sodium fusidate |
Sodium fusidate-loaded FFH provides an efficient and simple way to treat wounds by encouraging the disappearance of granulation tissue and skin regeneration. |
48 |
|
Polyvinyl alcohol, Polyvinyl pyrrolidone and sodium alginate |
In vivo study on male CrlOri: SKH1-hr strain hairless diabetic mice |
Neomycin sulfate |
By removing granulation tissue and replacing it with normal tissue, the neomycin sulfate-loaded hydrogel dressing outperformed commercial treatments in wound healing, demonstrating its potential as a successful wound treatment. |
49 |
|
Polylactic acid ,polyvinyl alcohol, sodium alginate |
In vivo study on male CD1 diabetic mice |
Hydrogen peroxide (H2O2) (matrigel) |
With less granulation tissue, surface keratin, edema, and inflammatory cells, the HG_OMs_MG hydrogel formulation dramatically improved wound healing. Within seven days of the damage, the skin defect was almost completely closed. |
50 |
|
Chitosan, polyvinyl alcohol |
In vivo study on Kunming female mice. |
Lignin |
Compared to the chitosan–PVA hydrogel, the lignin–chitosan–PVA composite hydrogel maintained a moist healing environment and accelerated wound healing, suggesting great prospects for effective skin wound care. |
51 |
|
Sodium alginate |
In vivo study on male Wistar rat |
Naringenin |
According to the study, alginate hydrogel containing 20% naringenin greatly increases cell viability (P <0.05) and promotes wound healing, indicating that it may have practical application in the treatment of skin injuries. |
52 |
|
Sodium alginate, chitosan |
In vivo study on male Wistar rats |
Hesperidin |
In vivo, the alginate/chitosan hydrogel containing 10% hesperidin outperformed the gauze-treated control group and demonstrated the highest wound closure percentage. |
53 |
|
Silk fibroin, gelatin |
In vivo study on rat model |
Artemisinin |
The SF-G-ART composite hydrogel considerably slowed the growth of tumors in vivo while simultaneously promoting quicker wound healing with more fibroblasts, ordered connective tissue, and smoother epithelium. |
54 |
|
Agar |
In vivo study on male Wister albino rats |
Icariin |
Compared to the other groups, the icariin-loaded hydrogel scaffold demonstrated substantial hair follicle development, dense skin creation with an abundance of collagen and fibroblasts, and full epithelial tissue regeneration by day 12. |
55 |
|
Dextran, Sodium hyaluronic acid |
In vivo study on male SD rat model |
Sanguinarine (SA) incorporate in the gelatin microsphere (GMs) |
In comparison to control groups, the study discovered that SA/GMs/Dex-HA dramatically decreased TNF-α levels, accelerated epithelization, collagen deposition, and uniform distribution, suggesting its potential for effective treatment of infected burns and suppression of scar formation. |
56 |
pH responsive Hydrogels
The microenvironment of skin wounds is intimately linked to pH changes. Sweat and sebum glands secrete fatty and amino acids to protect the skin from external threats, resulting in a weakly acidic environment with a pH of 5.0 to 6.0 on normal and healthy skin. Acute wounds have a more neutral pH of about 7.4, but chronic wounds have an alkaline pH of between 7.4 and 9.0, which is caused by the buildup of blood and interstitial blood. It is suggested that pH-responsive hydrogels could be a helpful substance to track the healing process and aid in medication release[57]. Two types of pH sensitivity have recently been widely used in the creation of hydrogel-based wound dressings. In order to obtain a regulated and continuous administration of healing substances, the first method uses polyelectrolyte polymers in which the charged side groups undergo protonation or de-protonation to change the swelling behavior of the hydrogel networks. These networks then expand or shrink. This mechanism has also been extensively documented for hydrogel-based medication delivery in the treatment of cancer.[58]. Numerous factors, such as polymer functionalities, medium pH, ionic strength, and dissociation constants, are crucial in influencing the hydrogel networks' morphological and volume changes[59]. Important metrics to assess the swelling behavior of the polymers in accordance with the medium Ph are pKa and pKb, which are the negative logarithm of the acid (Ka) and basic (Kb) dissociation constants, respectively. The strength of acidity and basicity is inversely proportional to the values of pKa and Pkb. Stronger acids and bases, respectively, have smaller pKa and pKb values. Because pKa + pKb = 14, an acid has a lower pKa than a stronger base.[60,61].Alginate, hyaluronic acid, and xanthan gum are examples of polyanions that typically have a pKa value between 3 and 5. In water or any other media, their hydroxyl and carboxyl groups will deprotonate (give the protons) and form negatively-charged chains when the pKa < pH of the medium. The medications are released as the hydrogel network expands due to the internal repulsion created by those negatively charged chains[59,60].Alginate, hyaluronic acid, and xanthan gum are examples of polyanions that typically have pKa values between 3 and 5. In water or any other media, their hydroxyl and carboxyl groups will deprotonate (give the protons) and form negatively charged chains when the pKa < pH of the medium. The medications are released as the hydrogel network expands due to the internal repulsion created by those negatively charged chains[62,59]. However, polycations like chitosan and its derivatives have a significantly higher pKa (i.e., lower pKb) and have amine groups (-NH2) that, when their pKa is greater than the medium's pH, will be protonated (take a proton) to produce positively charged groups. Drug release increases as a result of the positively charged groups repelling one another and expanding the hydrogel pore size [63, 64]. Tang et al. created a multipurpose hydrogel wound dressing based on a mixture of polyacrylamide (PAAm) and xanthan gum (XG) by employing the previously described technique. The PAAm-XG system showed a much greater swelling ratio from 7.3 to 12 when compared to pure PAAm hydrogel because of the hydrophilicity of XG and the electrostatic repulsion caused by the carboxyl groups from XG molecules. PAAm-XG hydrogels were able to maintain a moist environment and effectively absorb wound extrudes to speed up the healing process thanks to this improvement in swelling behaviors[65]. In a different instance, Chen and colleagues tried to create an injectable, self-healing, anti-microbial wound dressing based on chitosan, which is known to have anti-bacterial and anti-fungal qualities because it can attack intracellular targets and break bacterial cell walls and membranes[66]. As stated, S-Ag coordination was used to crosslink the chitosan after it had been thiolated.A dual-crosslinked chitosan hydrogel was created by further crosslinking the amine groups in the resulting hydrogels with genipin. This hydrogel system showed a significantly higher swelling ratio in the acidic media (pH = 2) compared to the neutral medium (pH = 7.0). This was explained by the amino groups' protonation in the low pH medium (more accessible H+), which caused the polymer chain relaxation and network expansion. As the concentration of crosslinked amino groups increased in both media, the hydrogel's swelling ratio dropped (few amino groups were accessible for protonation), indicating the significance of cationic amino groups in chitosan in determining its swelling behavior [67]. In contrast to polyelectrolytes, another popular method for creating pH-responsive hydrogel for wound healing is based on the Schiff base reaction, which creates dynamic covalent imine bonds (C = N) by crosslinking an aldehyde (or ketone) with a primary amine group to create imine, hydrazone, oxime, benzoic imine, and other compounds. In moderate conditions, these Schiff base bonds can form, and in an acidic environment, they can cleave, improving drug release and causing hydrogel deterioration.The hydrogel possesses self-healing qualities because the broken connections can reassemble after the acid is removed[68]. For example, hyaluronic acids are utilized to make hydrogel wound dressings because of their high water-retaining capacity, biocompatibility, ability to hydrate tissues, and ability to modulate inflammation[69]. Easy oxidation of hyaluronic acid produced aldehyde side groups, which were subsequently crosslinked with the lysine residues in an antimicrobial peptide sequence to generate a Schiff base linkage. In an in-vivo mouse animal model, this hydrogel was found to exhibit improved mechanical properties, injectability, and pH-initiated peptide release. It was also successful in preventing the colonization of Escherichia coli and Staphylococcus aureus in an acidic environment (pH = 5.5) as opposed to pH = 7.4 [70]. In a related study, Qiu et al. created a hydrogel wound dressing in which two essential oils (oregano and eugenol) were complexed with the hydrogel network to act as antibacterial agents. The Schiff base bond was created using aldehyde-modified hyaluronic acid and carboxymethyl chitosan. The resulting hydrogel showed a notable increase in eugenol release profile from 37.5% in neutral environments (pH = 7.2) to 82.1% in a more acidic environment (pH = 5.5). This enhancement was attributed to the breakdown of Schiff base bonds caused by the acid[71].Another attempt involved the development of a pH-sensitive hydrogel using reversible imine linkages between collagen and polyethylene glycol modified with aldehyde.Rats with diabetic foot ulcers were treated by loading hydrogel samples with umbilical cord stem cell factor. Cellular response, collagen deposition, and vascularization all showed signs of healing[72]. Hyaluronic acids can be altered and photo-crosslinked to increase their mechanical performance, which is an important issue for future uses of collagen and hyaluronic acid[73]. The biocompatibility problems brought on by chemical changes still require attention. Apart from hyaluronic acid, self-healing hydrogels containing Schiff base bonds can also be made using cellulose. For instance, tobramycin, a biocompatible crosslinker, was used to create the imine bond in dialdehyde carboxymethyl cellulose. Through their electrostatic interaction with the carbonyl groups in cellulose chains, borneol/β-cyclodextrin inclusion drug compounds were successfully distributed throughout the hydrogel network. Due to the breakdown of imine bonds in response to the weak acid, the hydrogels were demonstrated to be able to self-heal and showed a significantly greater degree of hydrolysis in an acidic environment (pH = 5.0) than in neutral (pH = 7.0) and basic (pH = 9.0) circumstances, as a result of imine bonds being broken in response to the weak acid. It is believed that this kind of slow degradation characteristic can help accomplish regulated release of medications that treat wounds[74]. Most of the research mentioned above concentrates on Shiff base bond-based acid-responsive hydrogels. The ability of these hydrogels to release medications when exposed to an acidic environment has been demonstrated by clear results.However, the precise pH variations in the wound area are quite complicated and can be affected by a variety of factors, including the type of wound, bacterial type, microbial infection, inflammation, diabetes, age, the location of the damage, moisture and perspiration, and more[75].
Temperature responsive Hydrogel
The hydrogels employed in wound healing exhibit a sol-gel transition at about physiological temperatures, which makes medication mixing and distribution exceedingly convenient.The liquid polymer solution is uniformly combined with stem cells, growth factors, medications, and peptides.In order to achieve a controlled release and wound regeneration, the mixes are then injected or sprayed onto the skin wound. When the temperature changes, they turn into a gel state[76]. The polymer solutions for the polymers displaying LCST stay in the sol state and gel at temperatures above LCST, whereas in the case of UCST, the polymer solutions are sol at temperatures above UCST and transition to gel at temperatures below UCST.It is stated that two potential mechanisms for thermoresponsive gelation include hydrophobic associations and conformational changes of the polymer chains[77]. Poly(N-isopropylacrylamide), commonly referred to as polyNIPAAm, is an example of a polymer that experiences an LCST reversible sol-gel transition at around 32–34oC. The hydrophilic-hydrophobic conversion process is one potential mechanism. Water molecules create a hydration barrier beneath the LCST, preventing the hydrophobic interactions between the methyl groups in various polyNIPAAm chains. Heat causes the hydration layer to break down as the temperature rises, enabling the development of hydrophobic associations that serve as physical crosslinkers to join the polyNIPAAm chains to gelate. According to thermodynamics, polymer-solvent interactions are the preferred process below LCST, while interactions between polymer chains are preferred above LCST[78].Depending on the temperature, these polymers self-assemble to create micelles with hydrophilic shells and hydrophobic cores and increasing the hydrophobic segment's molar ratio to the hydrophilic segment facilitates the hydrophobic association and gelation process[76].Due to its LCST being close to physiological temperature and its high viability of forming interpenetrating hydrogel networks and triblock co-polymers, where polyNIPAAm is integrated with other selected polymers to optimize the overall properties of the final hydrogel product, polyNIPAAm is a popular candidate for hydrogel wound dressing.For example, a semi-interpenetrating hydrogel network containing anti-cancer medications, such as doxorubicin for the treatment of melanoma and skin regeneration, has been created using polyNIPAAm and poly (vinyl alcohol) (PVA). Here, polyNIPAAm was utilized to start the LCST behavior, which resulted in the controlled release at skin temperature, while PVA was utilized to enhance the water-absorbing capacity, porosity, and adhesion capabilities[78]. Considering many benefits of PVA, its biodegradability problem may restrict its use in biomedical applications[79]. As a material for wound dressings, the PEP triblock copolymer including segments of polyNIPAAm and polyethylene glycol was also made to incorporate reduced graphene oxide nanosheets embellished with silver nanoparticles.This hydrogel system showed an irreversible sol-gel transition at 30°C due to the coordination between the silver particles and amino groups in polyNIPAAm chains. This structural stability made this hydrogel system a promising option for the wound dressing material to prevent the infection caused by methicillin-resistant Staphylococcus aureus (MRSA) [80]. Xanthan gum (XG) is a polysaccharide with a linear β-1,4-D-glucose backbone and a charged trisaccharide (β-d-mannose-(1,4)-β-d-glucuronic acid-(1,2)-α-d-mannose) on each alternate glucose unit. In addition to the synthetic polymers previously discussed, a number of biopolymers with temperature responsiveness are also widely reported to fabricate hydrogel for wound healing[81].The conformational change of XG in aqueous solution, from a random and flexible coil at high temperatures to a stiff and ordered double helical strand state at low temperatures, is the source of its thermosensitivity. This shift occurs at a temperature of around 40 to 50 oC, below which the helical strands form a gel-like behaviour and show shear thinning characteristics, which makes XG a valuable substance for injectable hydrogel wound dressings[81]. The methyl cellulose (MC) on the other hand shows an LCST sol-gel transition. The hydroxyl groups in MC chains make hydrogen bonds with the water below the LCST point, and the resulting hydration layers filter and stop the methyl groups from forming hydrophobic associations. When the temperature rises over LCST, the heat energy causes the hydration layer to rupture, enabling the development of hydrophobic associates that gelate the MC network[82]. An injectable and temperature-responsive hydrogel was created using XG and MC together. The researchers observed that the mixture gelled at 37 °C, with XG and MC forming a double network. They ascribed this gelation to XG's double helical strands and MC's hydrophobic association, respectively[81]. Another study used XG and konjac glucomannan (KGM) to create a hydrogel-based treatment for wounds that was subsequently seeded with human fibroblasts. In addition to improving the weak mechanical qualities of KGM, a commonly used thickening in the food business, the presence of XG made the gel system thermoresponsive (gelated at or below 37oC)[82].Chitosan and its derivatives are widely known for being thermoresponsive since they are a byproduct of chitin's deacetylation.Anti-cancer drug delivery that experienced a sol (25oC) to gel (37oC) phase transition to provide a controlled in vivo release profile have been prepared using its temperature-induced gelation activity.The gelation period was greatly reduced by increasing the chitosan concentration because more hydrogen bonds were accessible for the formation of the gel network[83]. Finally, agarose and gelatin are examples of UCST thermoresponsive biopolymers. They dissolve in aqueous solution at temperatures higher than UCST and move to a gel at lower temperatures.Finally, in contrast to LCST polymers, agarose and gelatin are UCST thermo-responsive biopolymers [84].
CONCLUSION
Temperature- and pH-sensitive hydrogels have emerged as an advanced and promising strategy for the treatment of infected skin wounds. These smart biomaterials are designed to respond to changes in the wound microenvironment, particularly variations in temperature and pH that occur during bacterial infection and inflammation. Such responsiveness allows hydrogels to undergo structural changes that enable controlled and targeted release of therapeutic agents directly at the wound site. As a result, antibiotics, antimicrobial compounds, and bioactive molecules can be delivered more effectively, reducing infection and promoting faster healing. Temperature-responsive hydrogels are particularly beneficial because they can undergo sol–gel transition at body temperature, allowing easy application and in situ gel formation on the wound surface. Meanwhile, pH-responsive hydrogels can selectively release drugs in acidic environments typical of infected wounds, ensuring precise therapeutic action. Recent advances in polymer science and nanotechnology have further improved the functionality of these hydrogels by incorporating antibacterial nanoparticles, growth factors, and self-healing properties. Despite these promising developments, challenges such as large-scale production, long-term stability, and clinical validation still need to be addressed temperature and pH-sensitive hydrogels represent a highly effective and innovative approach for infected skin wound healing, offering controlled drug delivery, improved infection management, and enhanced tissue regeneration.
REFERENCES

Neha Raj, Abhishek Singh, Narahari Palei, Temperature and pH Sensitive Hydrogel for Infected Skin Wound Healing, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1053-1067 https://doi.org/10.5281/zenodo.19451371
 10.5281/zenodo.19451371
10.5281/zenodo.19451371
