
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
University Institute of Pharma Science, Chandigarh University, Chandigarh Ludhiana Highway, Gharuan, Mohali, Punjab.
The current study will assess the efficacy of Tenecteplase and Alteplase for MI and stroke management. Our study aimed to analyse and compare pharmacological outcomes using literature studies and empirical research. Our extensive investigation proves Tenecteplase's superiority over Alteplase in treating MI and stroke. Tenecteplase's quick thrombolysis, long half-life, and fibrin selectivity make it advantageous. It also has a safety profile like Alteplase but fewer side effects. Tenecteplase may improve blood flow after a stroke, especially when a significant blood artery is blocked. This prevents disability and mortality increases. Our study also found that left-insular stroke predicts cardiac arrest, shedding light on stroke subtypes' broader effects. Tenecteplase at 0.1–0.5 mg/kg within 4 hours improves reperfusion and functional results compared to Alteplase in ischemic stroke. In myocardial infarction (MI), both intravenous medicines work similarly. However, bolus Tenecteplase within 4 hours reduces bleeding and blood transfusion. This discovery is crucial to patient safety. Our study also shows that Tenecteplase and Alteplase have comparable pharmacological interactions, confirming their clinical compatibility and improving treatment decisions. The data strongly supports Tenecteplase as a potential Alteplase alternative in thrombolytic treatment for myocardial infarction and stroke. Tenecteplase improves clinical and reperfusion results, especially in specific patient groups, making it an appealing option for healthcare providers. Our study evaluates thrombolytic medicines to help doctors make educated and practical treatment choices for essential cardiovascular and cerebrovascular illnesses.
Tenecteplase and alteplase are both thrombolytic drugs used for the treatment of conditions such as Stroke and Myocardial Infarction. Both Tenecteplase and Alteplase are tissue plasminogen activators (TPAs) and function as fibrinolytic drugs.[1] They catalyse the conversion of plasminogen to plasmin, promoting the breakdown of fibrin clot. Both drugs are used for the treatment of acute myocardial infarction (AMI) and have been approved for this indication. They aim to restore blood flow in coronary arteries affected by thrombosis.[2] Both Tenecteplase and Alteplase are created using recombinant DNA technology, allowing to produce therapeutic proteins for fibrinolysis. Both drugs have received regulatory approval for use in specific regions, with Tenecteplase approved in the United States (TNKase; Genentech) and Europe (Metalyse; Boehringer Ingelheim) in 2000 and Alteplase being a recognized first-line treatment for AMI.[3], [4] Tenecteplase has a longer half-life (22 minutes) compared to Alteplase (5-10 minutes). This longer duration may impact the dosing frequency and administration schedule. Tenecteplase has a higher level of fibrin specificity compared to Alteplase. This allows for a more targeted action on arterial thrombi, potentially reducing side effects and improving efficacy.[5] Tenecteplase can be administered as a single bolus over 5 to 10 seconds, while Alteplase requires a bolus followed by a 1-hour infusion. The quicker administration of Tenecteplase may be more convenient in certain situations. The dosage of Tenecteplase is weight-based, ranging from 0.5 mg/kg to a maximum dose of 50 mg/kg.[6] Alteplase has a recommended dosage of 100 mg given as a 10-mg intravenous bolus followed by a continuous infusion for three hours, with variations observed in clinical trials. Both drugs appear to be equally effective in patients without large vessel occlusion (LVO), but specific patient characteristics and risk profiles may influence the choice between the two drugs. Alteplase has been subject to assessments regarding its cost-effectiveness due to a higher acquisition cost than alternative thrombolytic medicines. Tenecteplase may present a different economic profile.[7], [8]
1.2 Myocardial Infarction:
Myocardial infarction is the irreversible necrosis of heart muscle (heart attack).MI is secondary to prolonged ischemia.1.5 million cases of MI occur annually in the US.[9] Men had a higher prevalence of AMI and a higher fatality rate compared to women. During data collection, men were hospitalized more than women, but women died more frequently.[10] In terms of the profile of patients with AMI, the age group with the highest mortality was 60 to 80 years old, with a hospital stay of less than 10 days, and SAH was the most significant risk factor in relation to death, with a greater frequency in women, followed by diabetes. Men were more likely to smoke and stop smoking.[11] The prevalence of cardiovascular disease in India has risen over the last two decades due to population growth, aging, and a constant age-adjusted cardiovascular disease death rate. In 1990, the age-standardized prevalence of cardiovascular disease per 100,000 people in India was 5450, while in 2016, it was 5681.[12], [13] It is a dangerous condition caused by a lack of blood flow to the heart muscle. a sticky substance plaque that builds up (atherosclerosis) inside the arteries. the clots block the artery as a result heart muscle will be deprived of blood and cause a heart attack. The heart muscle will begin to die without sufficient blood flow. Death and permanent heart damage can occur. It is the most common form of coronary heart disease (CHD). When a coronary artery is occluded or almost occluded MI occurs which will result in blood flow reduction.[14], [15] The two types of MI incudes, STEMI [ST -Segment elevation myocardial infarction] is recognized by ST- segment elevation changes can typically see on the ECG [electrocardiography]&NSTEMI [non-ST- segment elevation myocardial infarction] on the other hand absence of ST segment elevation can typically see on the ECG [electrocardiography].[16]
1.3 Stroke:
The traditional definition of a stroke is a neurological deficit caused by an immediate, focused lesion to the central nervous system (CNS) due to a vascular source, such as cerebral infarction, intracerebral haemorrhage (ICH), or subarachnoid haemorrhage (SAH). [17] According to recent research, stroke-related morbidity and mortality can be considerably decreased by early detection, immediate interventional treatment for acute ischemic stroke, and treatment in centres specifically dedicated to treating stroke patients.[18] Stroke mortality has been dropping for the past six decades, and as a result, stroke has dropped from second to fifth major cause of death in the US. This tendency could be attributed to recent developments in stroke management, which emphasize the importance of early identification and revascularization.[19] Recent research has demonstrated that early detection, immediate interventional therapy of acute ischemic stroke, and care in dedicated stroke centres can greatly reduce stroke-related morbidity and mortality. Stroke, on the other hand, is the world's second greatest cause of mortality and the major cause of acquired long-term disability, accounting for a global yearly economic burden.[20] A cohort included 28,672 individuals (87.8% of whom had an ischemic stroke). Individuals with ischemic stroke had a higher risk of mortality with severe co-morbidity (adjusted hazard ratio [aHR] 2.20, 95% CI 2.07-2.32) compared to those with intracerebral haemorrhage (aHR 1.70, 95% CI 1.51-1.92; pint<0.001), and those under 75 had a higher risk (aHR 3.20, 95% CI 2.90-3.53) compared to those over 75 (aHR 1.93, 95% CI 1.82-2.05, pint<0.001).[21][22] There was no sexual interaction. The hazard ratio grew gradually at lower ages and was larger after the first 30 days following acute stroke.[23]
2. Mechanism of Tenecteplase and Alteplase
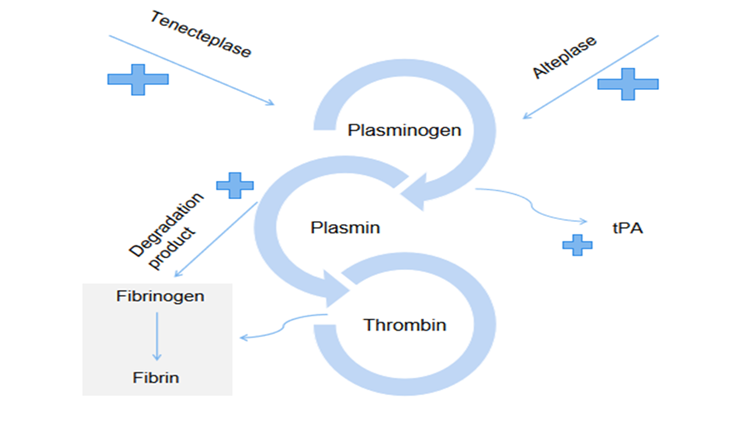
Figure 2: Mechanism of action
Above flow chart representation show combine mechanism of Tenecteplase and alteplase, starts with the activation of platelets change, prothrombin circulates in its active form during thrombosis. Plasminogen is converted into plasmin at the site of the thrombus and on the surface of the fibrin through tissue plasminogen activator, Endothelial cells contain tissue plasminogen activator (tPA), a naturally occurring fibrinolytic. It displays the affinity and specificity of fibrin binding to plasminogen during this therapy. Tenecteplase binds to fibrin-rich clots using the Kringle 2 and fibronectin finger like domains. The Arg/Val link in plasminogen is then broken by the protease domain, releasing plasmin. Active thrombin convert fibrinogen into fibrin ,creating a fibrin matrix .Plasmin from plasminogen accumulate in fibrin matrix ,balanced this action .This plasmin then degrade the fibrin matrix of the thrombus , thereby exerting thrombolytic action , eliminate arterial blockage and blood clot , reduce rate of formation of blood clot and hence MI chance reduce .Half-life- 1.9 hours [mammalian reticulocytes in vitro] , >20 HOURS [yeast, in vivo] ,>10 HOURS [Escherichia coli, in vivo] ,Clearance –99-119ml/min [acute myocardial infarction patients][2], [24]
3. Dosage forms and strengths of Tenecteplase and Alteplase for Stroke
|
|
Tenecteplase |
Alteplase |
|||||
|
S.no |
Weight |
Dose |
|
Weight |
Dose |
Route |
Reference |
|
1. |
60kg |
30mg |
For accelerated infusion |
>67kg |
100mg (15mg bolus in 1st hour, 50mg infusion in 2nd hour& 35 mg infusion in 3rd hour) |
IV bolus/ Infusion |
[2], [25] |
|
2. |
60-70kg |
35mg |
<67kg |
100mg (15mg bolus in 1st hour ,1.75mg/kg infusion in 2nd hour & 0.5mg/kg infusion in 3rd hour) |
IV bolus/ Infusion |
[25], [26] |
|
|
3. |
70-80kg |
40mg |
For 3hour infusion method |
>65kg |
100mg (60mg in 1st hour& 30mg in 2nd and 3rd hour |
IV bolus |
[25], [27] |
|
4. |
80-90kg |
45mg |
|
<65kg |
1.25mg/kg (0.75mg/kg in 1st hour& 0.25mg in 2nd and 3rd hour) |
IV bolus |
[25], [28] |
|
5. |
>90kg |
50mg |
|
|
|
IV bolus |
[25], [29] |
The above table illustrates a dosing regimen for a medicine that is administered intravenously (IV) as a bolus over a time of 5 seconds. This regimen is specifically designed to accommodate patients of varying weight categories. The document delineates five distinct weight categories, ranging from 60kg to over 90kg, each associated with a specific dosage: 30mg, 35mg, 40mg, 45mg, and 50mg, respectively. The dosing strategy adheres to the principle of escalating the drug dosage in tandem with the patient's weight classification, thereby guaranteeing suitable therapy in accordance with the individual's body weight. Simultaneously, it is noteworthy that the selected method of administration remains uniform across all instances, prioritizing the expeditious intravenous delivery. The dosage of tenecteplase administered to patients with myocardial infarction (MI) is dependent on the individual's weight, ranging from a minimum dose of 30mg/kg to a maximum dose of 50 mg/kg. The intravenous (IV) mode of administration was the favoured method within a specified time frame of 5 seconds.
4. Tenecteplase and Alteplase in Ischemic stroke
Tenecteplase act as a thrombolytic for ischemic stroke, and it is currently being examined in several trials. Clinical trials for ischemic stroke have examined in Tenecteplase doses between 0.1 and 0.5 mg/kg.[30] When patients with ischemic stroke were treated within 4.5 hours’ symptoms begin, tenecteplase before thrombectomy was linked to a higher rate of reperfusion and a better functional result than alteplase.[31] The Alteplase-Tenecteplase Trial Evaluation for Stroke Thrombolysis (ATTEST-2; NCT 02814409), which is testing the superiority of tenecteplase, and compared the alteplase to Tenecteplase in Patients with Acute Ischemic Stroke (AcT), which will test the non-inferiority of tenecteplase in actual clinical use, are both significant (NCT03889249).[32], [33] The Tenecteplase in Wake-up Ischemic Stroke Experiment (TWIST, NCT03181360) is a Phase 3 trial that randomizes patients to receive either tenecteplase 0.25 mg/kg or standard care if they can be treated within 4.5 hours of within developing new stroke symptoms.[34]
4.1 Clinical studies and test performed on Tenecteplase and Alteplase for Ischemic Stroke
|
Sr. No |
Objective |
No of subjects used |
Description |
Conclusion |
Reference |
|
1. |
To compare between alteplase .9mg, tenecteplase .1mg/kg& .25mg/kg administered with 6hr for treatment of Ischemic stroke on basis of computed tomography (CT) perfusion & imaging. |
75 participants: at 1:1:1, Group 1 received alteplase (0.9 mg per kilogramme of body weight), while other two groups received tenecteplase (0.1 mg per kilogramme or 0.25 mg per kilogram) respectively. |
Patients with acute ischemic stroke participated in this randomised, open-label, blinded trial and received CT perfusion and angiographic imaging prior to receiving intravenous tenecteplase or alteplase medication, which was given within 6 hours of the stroke's onset. |
In stroke patients who were chosen based on CT perfusion imaging, tenecteplase was linked to noticeably better clinical and reperfusion results than alteplase. |
[35] |
|
2. |
To compare between tenecteplase o.25mg/kg and alteplase .9mg/kg for effective treatment in patient with ischemic stroke with middle cerebral artery, carotid basilar, eligible for thrombectomy. |
202: a total of 202 patients were selected for the test. 101 patients were given Tenecteplase while other 101 patients were given alteplase. |
A Randomized, outcome blinded trials was performed on patients with Ischemic stroke undergoing thrombectomy for occlusion of the internal carotid, basilar, or middle cerebral artery. Patient were divided on 1:1. given Tenecteplase dose of .25mg/kg & alteplase at .9mg /kg. |
On patients with Acute Ischemic stroke who were treated within 4.5 hours of the start of symptoms, tenecteplase given prior to thrombectomy was associated with a greater incidence of reperfusion and a better functional result than alteplase. |
[4] |
|
3. |
To ascertain if 0.40 mg/kg of tenecteplase, as opposed to 0.25 mg/kg, safely enhances reperfusion prior to endovascular thrombectomy in patients with major artery blockage ischemic stroke. |
300: subjects were divided into 2 groups of 150 each with mean age of 72.2 years. First group was administered with .25mg/kg of tenecteplase while another group was administered with .40mg/kg tenecteplase. |
A randomized, multi centre, open-labelled, blinded end point trials was performed on patients with thrombectomy for occlusion of the internal carotid, basilar, or middle cerebral artery within 4.5 hours. Patients were divided on 1:1 basis and were administered with .40mg/kg of tenecteplase & .25mg/kg of tenecteplase respectively. |
Tenecteplase at 0.40 mg/kg versus 0.25 mg/kg did not improve cerebral reperfusion prior to endovascular thrombectomy in individuals with major vessel blockage ischemic stroke. |
[36], [37] |
|
4. |
To assess whether tenecteplase 0.4 mg/kg is superior than alteplase 0.9 mg/kg in treating patients with mild to severe ischemic stroke. |
From Oct.28,2019, to Sept.26, 2021. 216 patients were shortlisted for the test. 204 patients undergo the trials out of these 100 patients were administered with tenectplase while other 104 received alteplase .9mg/kg |
In Norway, 11 hospitals with stroke units conducted a phase 3 randomised open-label, blinded endpoint, non-inferiority trial. Consecutively, patients with suspected acute ischemic stroke who were eligible for thrombolysis and admitted within 4–5 hours of symptom start and had a National Institutes of Health Stroke Scale score of 6 or higher were included. |
Tenecteplase performed more safely and functionally than alteplase at a dose of0.4 mg/kg.As a result, the trial was unable to demonstrate that tenecteplase (0.4% mg/kg) is superior than alteplase in the treatment of moderate to severe ischemic stroke. |
[38] |
|
5. |
To compare between tenectplase.25mg/kg & alteplase .9mg/kg (.09mg/kg bolus & .81 mg/kg infusion). |
Tenecteplase (n=816) or alteplase (n =784) were given to 1600 patients between December10,2019, and January25,2022, of whom 1577 were part of the ITT population (n = 806 for tenecteplase and n = 771 for alteplase). The 1577 patients had a median age of 74 years (IQR63-83), with 755(47%) female patients, and 822(52%) male patients. |
Patients from 22 main and comprehensive stroke centres across Canada were enrolled. Patients were included if they were 18 years of age or older, had been diagnosed with an ischemic stroke that resulted in a debilitating neurological deficit, presented within 4–5 hours after the onset of symptoms, and qualified for thrombolysis according to Canadian standards. eligible patients were randomly assigned (1:1) to receive either intravenous tenecteplase (0.25 mg/kg to a maximum of 25 mg) or alteplase 0.9 mg/kg to a maximum of 90 mg; 0.09 mg/kg as a bolus and the remaining 0.81 mg/kg infused over 60 minutes). |
For all patients who present with an acute ischemic stroke and meet the criteria for thrombolysis, intravenous tenecteplase (0.25 mg/kg) is a viable substitute for alteplase. |
[39] |
The above table offers a concise overview of five clinical trials that have been conducted with the objective of comparing the efficacy of various thrombolytic drugs, with a primary focus on tenecteplase and alteplase, in the management of ischemic stroke. These clinical trials encompass the examination of different dosages and administration regimens, with the aim of evaluating outcomes such as reperfusion, functional results, and safety. The findings derived from these clinical studies offer significant insights on the optimal choice of thrombolytic drugs for the treatment of ischemic stroke. The trials provide evidence that tenecteplase, administered at doses of 0.1 mg/kg, 0.25 mg/kg, or 0.4 mg/kg, exhibits enhanced clinical and reperfusion results when compared to alteplase in distinct patient subgroups, such as individuals eligible for thrombectomy and those afflicted with significant arterial occlusion. Nevertheless, a clinical trial has indicated that the efficacy of tenecteplase, administered at a dosage of 0.4 mg/kg, may not surpass that of alteplase in individuals suffering from moderate to severe ischemic stroke. In general, the results of this study provide evidence that tenecteplase might be considered a suitable substitute for alteplase in specific cases of ischemic stroke. This alternative therapy option shows promise in terms of its effectiveness in treating the condition and improving the outcomes for patients.
5.Tenecteplase [tnkase] and Alteplase for myocardial infarction
TNKase is a replacement for the alteplase molecule. The fibrin-specific chemical TNKase can be given intravenously in a single bolus injection. 27000 myocardial infarction patients were included in a tenecteplase clinical trial, and it was discovered that TNKase is equally as effective as alteplase. It is the only bolus thrombolytic medication for which this equivalence has been officially shown. Tenecteplase has greater potency than alteplase when symptoms last longer than 4 hours. Tenecteplase decreases the chance of bleeding and the requirement for blood transfusions. A new fibrinolytic drug may be developed because of recent clinical trials that show it to be equally effective as primary angioplasty.[40], [41] In a TIMI 10B potency trial conducted among 886 patients in the age range of [18-80 years] with bolus TNKase injection, TIMI grade 3 flow rates of 55%, 63% at 90 min after injection of 30, 40 mg were seen. This flow rate was like that which we observed in the control group. Clinical use of TNKase in the acute myocardial infarction shows a dose dependent increase in Thrombolysis in myocardial. TNKase's safety was examined in 3235 patients who had STEMI at doses of 30, 40, and 50 mg. At 30 days, there was no discernible difference between the groups in the overall stroke rate (1.5%) and intracranial haemorrhage (ICH) rate (0.8%). In patients receiving TNKase and those receiving front loading alteplase, serious risk factors haemorrhage and blood transfusions occurred in 1.4% and 7% of patients, respectively. So, according to the TIMI-10B and ASSENT 1 studies, reducing the heparin dose while also using TNKase will lessen the incidence of ICH. It has been clearly shown that patients receiving tenecteplase experience less non-cerebral bleeding and require fewer blood transfusions, and the death rate in the TNKase group was lower when the medication was administered more than four hours after the onset of symptoms.[2], [4], [42], [43]
6. Contraindication and serious interaction of Tenecteplase and Alteplase
|
Sr. no. |
Drug |
Mechanism |
Inference |
Reference |
|
1. |
Defibrotide |
Defibrotide causes pharmacodynamics synergism effect with Tenecteplase and Alteplase. |
Serious contraindication. Avoid usage/ use alternate therapy. |
[25], [44] |
|
2. |
Prothrombin complex concentrate, human |
Prothrombin complex concentrate, human causes pharmacodynamics antagonism effects with Tenecteplase and alteplase. |
Serious antagonizing effects, use alternate therapy. |
[45] |
|
3. |
Apixaban & Reteplase |
Both drugs increase anticoagulation effects when administered either with Tenecteplase of alteplase. |
These drugs must not be administered together as they both increases anticoagulation. Use any alternate therapy. |
[46], [47] |
|
4. |
Zanubrutinib & Caplacizumab |
Either increases the effect of other by anticoagulation |
Use alternative drugs or avoid using. Risk of Zanubrutinib induced haemorrhage in increased when administered with other anticoagulants. |
[48], [49] |
The table presented offers a full and thorough examination of drug interactions and their corresponding mechanisms, a crucial aspect within the field of clinical pharmacology and the promotion of patient safety. The findings indicate that Defibrotide demonstrates a pharmacodynamic synergistic effect when combined with Tenecteplase and Alteplase. This suggests that the concurrent administration of these medications may result in significant contraindications, necessitating the avoidance of such combinations or the exploration of other therapeutic approaches. The administration of Prothrombin complex concentrate, human, has been found to exhibit pharmacodynamic antagonism when used in conjunction with Tenecteplase and Alteplase. This indicates the possibility of unfavourable antagonistic consequences, which highlights the need for alternate therapeutic approaches. Furthermore, it is worth noting that the administration of Apixaban and Reteplase in conjunction with either Tenecteplase or Alteplase results in heightened anticoagulant effects. This highlights the need of refraining from their simultaneous usage and instead considering alternate therapeutic approaches. In conclusion, the concurrent administration of Zanubrutinib and Caplacizumab leads to a synergistic enhancement of anticoagulant effects. This may increase the likelihood of Zanubrutinib-induced haemorrhage when used alongside other anticoagulants. Therefore, it is imperative to exercise caution, consider substituting medications, or altogether avoid co-administration to mitigate potential risks. The table functions as a vital resource for healthcare professionals, enabling them to make well-informed decisions concerning the use of drug combinations and their associated outcomes in clinical settings. Its primary focus is on ensuring patient safety and promoting the selection of successful therapeutic options. Based on the data presented in the table, it can be noticed that both tenecteplase and alteplase exhibit a shared drug-drug interaction. Most interactions were deemed severe, therefore emphasizing the importance of avoiding drug use, unless alternative options are recommended.
7.Safety profile of tenectplase and alteplase:
7.1 Bleeding Complications:
7.1.1 Intracranial Haemorrhage (ICH): There is an increased risk of bleeding complications with the use of both tenecteplase and alteplase, intracranial haemorrhage is the most common. Frequent bleeding event plays crucial factor while evaluating the safety profile of these two drugs.[50]
7.1.2 Major Bleeding Events: Other than intracranial bleeding, high frequency of bleeding events in other organ systems also plays a crucial role in determining the overall safety of these two drugs.[51], [52]
7.2 Hypersensitivity Reactions: Allergic reactions and hypersensitivity reactions are also associated with both the drugs. To prevent these events monitoring of these events is very essential for evaluating the safety of these drugs.[53], [54]
7.3 Tissue Damage and Reperfusion Injury: Reperfusion injury is the damage caused when blood flow is restored to tissues following a period of ischemia. While thrombolytic therapy tries to restore blood flow and avoid tissue damage, the reperfusion process itself can occasionally cause injury. The evaluation of reperfusion injury entails identifying potential issues caused by the restoration of blood flow. [55], [56], [57]
8. Practical Considerations in Real-World Clinical Practice:
8.1. Cost-effectiveness: The cost effectiveness of thrombolytic therapy is a crucial factor for consideration in healthcare decision makings. Though tenectplase offer logistical advantage, its cost requires careful monitoring. Health economic evaluations should balance the advantages of streamlined administration against the potential economic costs. [58], [59]
8.2. Logistical Factors: Practical issues in real-world contexts include simplicity of administration, storage requirements, and potential impact on workflow. Tenecteplase's single-bolus injection may simplify logistics when compared to alteplase, thereby lowering treatment delays, and improving the overall efficiency of acute stroke care.[60]
8.3. Patient Characteristics and Risk-Benefit Assessment: It is critical to tailor thrombolytic therapy to each patient's unique characteristics, such as age, comorbidities, and stroke severity. A detailed risk-benefit analysis should guide treatment options, considering the possibility of adverse events, bleeding problems, and the overall prognosis.[61], [62]
FUTURE PERSPECTIVE
Recent clinical studies have brought attention to Tenecteplase as a promising contender for developing a novel fibrinolytic medication, showcasing efficacy on par with primary angioplasty in managing ischemic stroke. The significance of this finding lies in its potential to greatly improve stroke outcomes. A significant observation derived from these studies is that the co-administration of Tenecteplase with a decreased dosage of heparin demonstrates a notable reduction in the incidence of intracerebral haemorrhage (ICH), a prominent worry in the context of fibrinolytic treatment. The risk reduction technique outlined in this study focuses on a crucial aspect of stroke therapy, specifically aiming to enhance the safety profile of Tenecteplase as a viable therapeutic choice for patients. The available clinical trial evidence provides robust support for the use of intravenous Tenecteplase at a lower dosage of 0.25 mg/kg as a feasible substitute for Alteplase, an extensively employed fibrinolytic drug in the treatment of ischemic stroke. This dosage has shown similar effectiveness to Alteplase, so it presents a tempting alternative for doctors who need a medication that is both effective and safe for patients suffering from ischemic stroke. To summarise, recent clinical studies have shown that Tenecteplase shows promise as a significant advancement in the treatment of stroke. It has demonstrated comparable effectiveness to primary angioplasty while also reducing the risk of intracerebral haemorrhage when combined with a lower dosage of heparin. This finding implies that the administration of Tenecteplase at a dosage of 0.25 mg/kg has the potential to emerge as a favoured option for the treatment of ischemic stroke, possibly bringing about a transformative impact on stroke management.
SUMMARY
With less systemic haemorrhaging this drug had an equivalent mortality of 30-days. Tenecteplase does not, at this time, have the same level of endorsement from the American Heart Association (AHA)/ American Stroke association (ASA) as alteplase has for intravenous (IV) thrombolysis in acute ischemic stroke patients, nor is it Food and Drug Administration (FDA)-approved for such use. Tenecteplase has also been the subject of clinical trials for ischemic stroke, catheter clearance, and pulmonary embolism. Two study performed on four phase and three study performed on one phase suggest that Tenecteplase superiority in recanalization of large vessel occlusion and non-inferiority in disability- free 3- month outcome, without increase in haemorrhage or mortality. Based on phase 2 trial 0.25mg/kg dose recommended for large vessel occlusions. Alteplase in 1987 approved for the treatment of STEMI. Serious intracranial bleeding complication, limited recanalization rates with Alteplase therapy motivate the researcher for development of variant of alteplase with 80- folds increased resistance to plasminogen activator inhibitor -1 activity,10-fold greater conservation of fibrinogen, reduced plasma clearance, longer plasma half-life, it passes through various clinical trial and come under name Tenecteplase. It developed from modification of natural human TPA complementary DNA. 527 amino acids it includes with a substitution of heroine 103 with asparagine’s and asparagine’s 117 substitution with glutamine within the cringle 1 domain, in the p\rotease domain tetra- almandine substitution at amino acid 296-299.
CONCLUSION
Thorough research found that Tenecteplase is more effective and safer than Alteplase in treating myocardial infarction (MI) and ischemic stroke. Tenecteplase is FDA-approved for weight-based dosage in various countries, including the US. Tenecteplase is equally efficacious as Alteplase in ST-segment elevation myocardial infarction (STEMI) with similar side effects. Both medicines treat MI well intravenously, but Tenecteplase is safer and more efficacious for boluses. The appropriate Tenecteplase dosage depends on age. Tenecteplase works in ischemic stroke at specific dosages, although Alteplase works better. Ongoing studies and research attempt to support these thrombolytic medicines' efficacy. Several studies show Tenecteplase may be chosen over Alteplase, signifying a thrombolytic therapeutic change.
REFERENCES


Dr. Kailash Singh Bisht*, Dr. Rashmi Adhikary, The Clinical Aspects of Tenecteplase in Stroke and Myocardial Infarction Over Alteplase, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1600-1614. https://doi.org/10.5281/zenodo.15864089
 10.5281/zenodo.15864089
10.5281/zenodo.15864089