1Professor and HOD, Department of Microbiology, Siddaganga Medical College and Research Institute, Tumkuru, Karnataka, India.
2,3,4Pharm D Intern, Sree Siddaganga College of Pharmacy, Tumakuru, Karnataka, India.
The utilization of antibiotics for the treatment of infections is increasing; however, their misuse or overuse can lead to resistance. The WHO AWaRe classification groups antibiotics into Access, Watch, and Reserve to improve use and reduce resistance. This study aims to determine the antibiotic prescription pattern using the WHO AWaRe classification and assess the knowledge of the prescribing physicians regarding AWaRe classification in a tertiary care hospital. A descriptive cross-sectional study included 180 prescriptions from various departments that contain atleast one antibiotic. Antibiotics were grouped based on the WHO AWaRe classification system. A structured questionnaire was used to assess the knowledge among prescribing physicians. Data was analysed using descriptive statistics. Out of 228 antibiotics prescribed, 40.4% were from Access group, 37.3% from Watch group, 0.4% from Reserve group, and 21.9% were from Not Recommended from WHO. Cephalosporins and tetracyclines were the most prescribed classes of antibiotics. Only 39.1% of surveyed physicians were familiar with AWaRe, with varying knowledge levels. Most supported increased education and use of AWaRe to improve prescribing. The study shows good use of Access antibiotics but highlights gaps in generic prescribing and AWaRe system awareness. Implementing an antibiotic stewardship program can enhance antibiotic use and reduce resistance.
Antimicrobials are the most prescribed medications globally, with the increasing usage in recent decades, especially in low- and middle-income countries (LMICs)[1] . Antibiotics use has become an essential part of modern medicine and it’s hard to imagine any treatment without their use, whether for treating minor infections or performing complex surgical or cosmetic operations. However, the rising issue of antimicrobial resistance, makes these drugs ineffective against specific pathogens, which highlights the urgent need to protect this essential resource[2].
Managing antimicrobial resistance (AMR) presents a significant economic challenge due to increased healthcare expenses through prolonged illness and more complex treatment plan. It is estimated that by 2050, AMR could cause up to 10 million death each year, resulting in a potential global economic burden[3]. AMR remains a major concern for global public health, particularly in developing countries[4]. The over and misuse of antimicrobials greatly impacts AMR. In 2017, India introduced the National Action Plan on AMR, emphasizing research and surveillance through an Antimicrobial Stewardship Programme (AMSP). The World Health Organization (WHO) also updated its essential drug list (WHO-EML), classifying antibiotics into ACCESS, WATCH, and RESERVE categories to enhance prescribing practices[5].
The goal of this classification is to limit at least 60% of prescribed antibiotics from the Access group to reduce the irrational prescribing and resistance, while limiting the use of Watch and Reserve groups[6,7].
Therefore, cross-sectional studies that assess drug utilization in hospitals, like prescription pattern monitoring play a vital role in promoting the rational and appropriate use of antibiotics agents[6].
There is lack of studies on the prescribing patterns of antibiotics using the WHO AWaRe classification in this part of South India. This study aims to determine the prescribing pattern of antibiotics using WHO AWARE classification and also to know the knowledge of prescribing physicians about AWaRe groups which helps in educational intervention, antimicrobial stewardship programs and formulation of antibiotic policy of the institution, finally for the containment of antimicrobial resistance.
MATERIALS AND METHODS
Study design and Setting:
A descriptive cross-sectional study was conducted for six months at Siddaganga Medical College and Research Institute (SMCRI), Tumakuru, a tertiary care hospital, to assess antibiotics prescribing patterns in adults and evaluate physicians knowledge of the WHO AWaRe classification.
Study Population and Sample Size:
The study included adult patient prescriptions (≥18 years) with at least one antibiotic, from General Medicine and allied, General Surgery and allied departments, along with participating physicians from the same departments. Based on a 4.11% prevalence of Reserve group antibiotic use, 3% precision, and 95% confidence interval, the required sample size was calculated as 169 prescriptions using Clarke’s formula:
N = Z² * P(1−P) / d².
Sampling Method:
Universal sampling technique was employed. All eligible and willing physicians and prescriptions meeting inclusion criteria during the study period were included.
Ethical Considerations:
The study was approved by the Institutional Ethics Committee of SMCRI (approval ID. SMCRI/IEC/2023-2024/48). Informed consent was obtained from all participating physicians. Participation was voluntary, confidentiality was maintained, and no direct patient interventions were involved. The study adhered to the ethical principles.
Data Collection Procedure:
Following Institutional Ethical Committee approval, data collection began with informed consent from physicians at SMCRI. Only prescriptions from consenting physicians were included. Data were collected from adult patients in both outpatient and inpatient departments.
The study has two components.
1. Prescription Audit:
Data were collected from adult patients (aged ≥18 years) whose prescriptions included at least one antibiotic, from both outpatient and inpatient departments of SMCRI. Prescriptions containing topical antibiotic were excluded. Data extracted included patient demographics, department, antibiotics agents (generic name, dose, route, duration), and indication for the antibiotics. Prescriptions were evaluated for appropriateness (right drug, dose, duration) based on WHO and Indian Council of Medical Research (ICMR) guidelines and classified according to the WHO AWaRe classification.
2. Physician Questionnaire:
Physicians at SMCRI who consented to participate completed a pre-validated, structured questionnaire assessing their awareness and understanding of the WHO AWaRe classification. The study purpose was explained, and informed consent was obtained prior to participation.
Statistical Analysis:
Data were compiled and analysed using Microsoft Excel 2019. Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarize both categorical (e.g., gender, antibiotic class, route of administration) and continuous variables (e.g., average number of antibiotics per prescription). WHO prescribing indicators were applied to assess prescription rationality, and antibiotics were categorized by the WHO AWaRe classification to examine usage trends. A scoring system was used for knowledge-based questions, assigning one point per correct response, while incorrect or unattempt responses received zero to quantify awareness and understanding of the AWaRe system. Total scores were analyzed to assess overall knowledge levels among participants.
RESULTS
Patient’s demographics: This study included 180 patients and their prescriptions containing at least one antibiotic were analysed. Of these, 50.5% (n=91) were prescribed to male patients, and 49.4% (n=89) were prescribed to female patients. Antibiotic prescriptions for outpatients accounted for 51.7% (n=93), while 48.3% (n=87) were for inpatients (Table 01).
Majority of the patients were in the age group of 19-38 years, comprising 44.4% (n=80), followed by 39-58 years age group with 35% (n=63). Additionally, 18.9% (n=34) of patients were in the 59-78 years age group, and 1.7% (n=3) were in the 79-98 years age group (Table-01). The highest number of prescriptions were collected from the General Medicine department (58.3%, n=105), followed by the Respiratory medicine department (24.4%, n=44). Prescriptions from the ENT and General Surgery departments accounted for fewer cases, comprising 11.7% (n=21) and 5.6% (n=10), respectively. (Table 01).
Table 1. Patients Demographic
|
Characteristics |
Number of patient (n=180) |
Percentage (%) |
|
Gender |
|
|
|
Male |
91 |
50.5 |
|
Female |
89 |
49.4 |
|
Age |
|
|
|
19-38 |
80 |
44.4 |
|
39-58 |
63 |
35 |
|
59-78 |
34 |
18.9 |
|
79-98 |
3 |
1.7 |
|
Admission type |
|
|
|
Out patient |
93 |
51.7 |
|
In patient |
87 |
48.3 |
|
Department |
|
|
|
General Medicine |
105 |
58.3 |
|
Respiratory Medicine |
44 |
24.4 |
|
ENT |
21 |
11.7 |
|
General Surgery |
10 |
5.6 |
Indication for prescribed antibiotics: Respiratory tract infections and acute febrile illnesses were the most common indications for antimicrobial use, each accounting for 27.2% (n=49). These were followed by gastrointestinal infections at 14.4% (n=26), ear, nose, and throat (ENT) infections at 11.7% (n=21), urinary tract infections at 8.9% (n=16), and skin and soft tissue infections at 5.6% (n=10). Other indications accounted for 5.0% (n=9) and included dengue fever, jaundice, hyponatremia, anaemia, and uncontrolled diabetes mellitus (DM) (Figure 01).
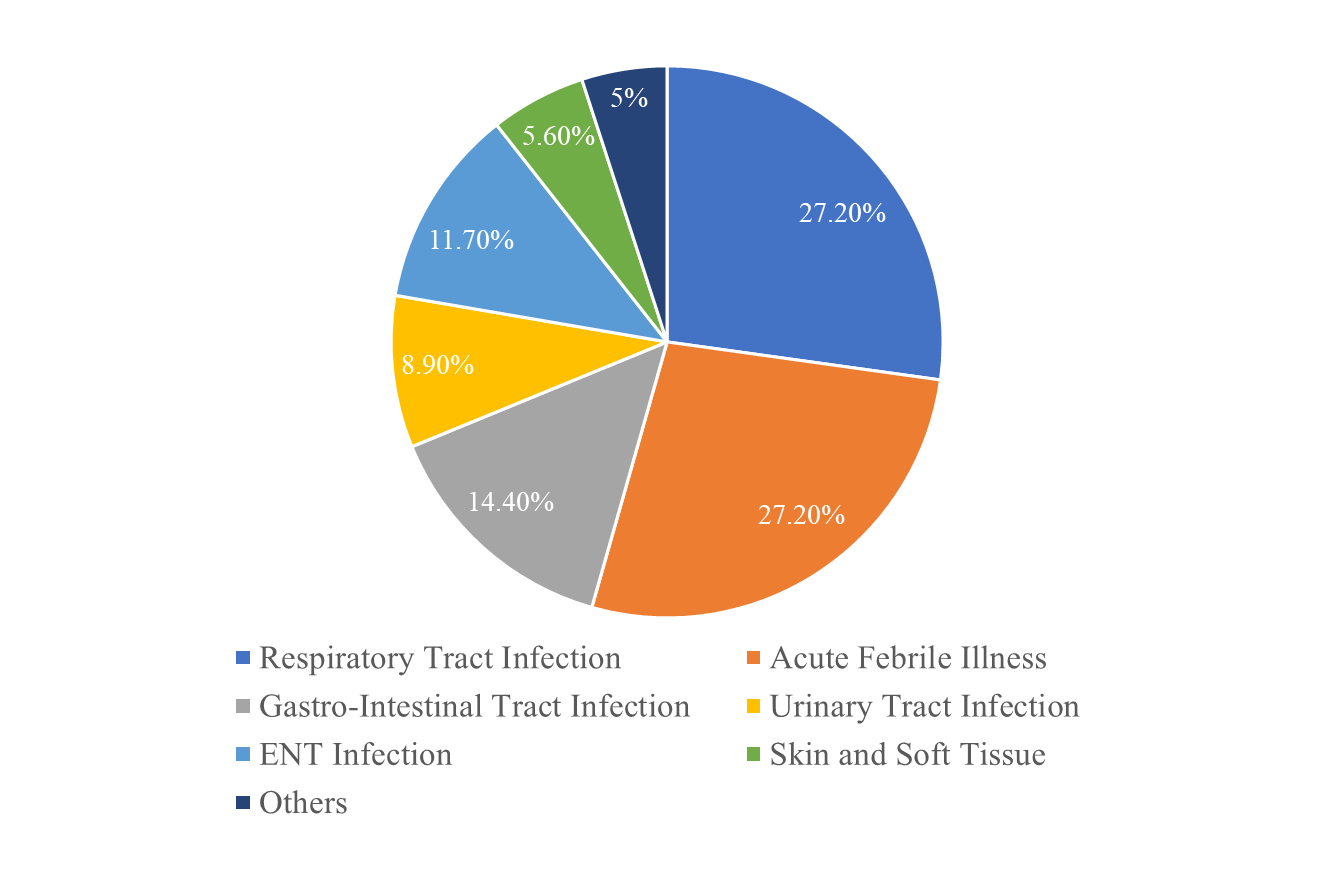
Figure 1. Indication for prescribed antibiotics
Commonly prescribed antibiotics: The prescriptions were classified into those containing a single antibiotic, which accounted for 74.4% (n=134), and those containing multiple antibiotics, which accounted for 25.5% (n=46). (Figure 02).
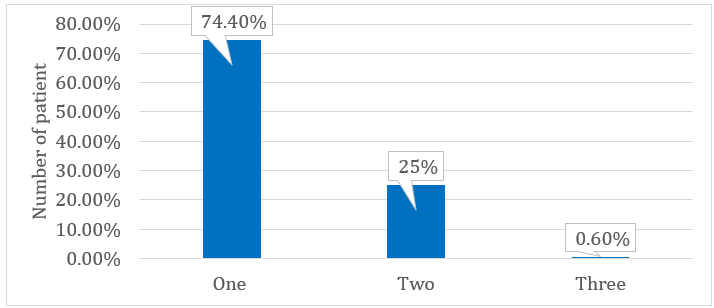
Figure 2. Antibiotics per prescription
A total of 228 antibiotics were prescribed in 180 prescriptions.
Among different antibiotic classes, Cephalosporin group was the most commonly prescribed, accounting for 29.4% (n=67), followed by Beta-lactam/beta-lactamase inhibitor at 19.7% (n=45) and tetracycline at 18.4% (n=42). Macrolides and fluoroquinolones were prescribed in 12.3% (n=28) and 11.4% (n=26), respectively, showing a minimal difference in their usage. Other antibiotic classes constituted 8.8% (n=20) of total antibiotics prescribed and included nitroimidazoles, nitrofurantoin, rifamycins, carbapenems, and sulphonamides. (Table 02). A total of 61.4% (n=140) patients were prescribed antibiotics orally, while 38.6% (n=88) patients were prescribed antibiotics through intravenous (IV) route. No outpatients were prescribed IV antibiotics. (Table 02). Analysis of antibiotic prescriptions revealed that doxycycline was the most commonly prescribed drug, comprising 18.4% (n=42) of the total. This was followed by amoxicillin + potassium clavulanate at 12.7% (n=29). Cefoperazone + sulbactam (8.3%, n=19), clarithromycin (7.4%, n=17), ceftriaxone and ceftriaxone + sulbactam (6.6%, n=15), azithromycin (4.8%, n=11), and piperacillin + tazobactam (4.4%, n=10) showed relatively close prescription frequencies, indicating no significant difference in their usage. Other antibiotics, comprising 7.0% (n=22), included Amoxicillin, rifaximin, ofloxacin, meropenem, faropenem, cefixime, Cefpodoxime-proxetil, and fixed-dose combinations such as levofloxacin + ornidazole, Cefixime+ofloxacin and trimethoprim + sulphamethoxazole. Most antibiotics were prescribed as monotherapy (60.5%, n=138), with doxycycline and clarithromycin being the most frequently used agents. Fixed-dose combinations accounted for 39.5% (n=90) of prescriptions, predominantly involving amoxicillin + potassium clavulanate and cefoperazone + sulbactam. (Table 02).
Table 2. Commonly prescribed antibiotics
|
Class of antibiotics |
Number of antibiotics (n=228) |
Percentage (%) |
|
Cephalosporins |
67 |
29.4 |
|
Beta-lactam/beta-lactamase inhibitor |
45 |
19.7 |
|
Tetracycline |
42 |
18.4 |
|
Macrolide |
28 |
12.3 |
|
Fluroquinolones |
26 |
11.4 |
|
Others |
20 |
8.8 |
|
Route of administration |
|
|
|
Per oral (PO) |
140 |
61.4 |
|
Intravenous (IV) |
88 |
38.6 |
|
|
Antibiotic prescribed as monotherapy |
|
|
Doxycycline (PO) |
28 |
12.3 |
|
(IV) |
14 |
6.1 |
|
Clarithromycin (PO) |
17 |
7.5 |
|
Ceftriaxone (IV) |
15 |
6.6 |
|
Azithromycin (PO) |
11 |
4.8 |
|
Ciprofloxacin (PO) |
7 |
3.1 |
|
(IV) |
3 |
1.3 |
|
Levofloxacin (PO) |
6 |
2.6 |
|
(IV) |
1 |
0.4 |
|
Metronidazole (PO) |
2 |
0.9 |
|
(IV) |
5 |
2.2 |
|
Nitrofurantoin (PO) |
7 |
3.1 |
|
Others |
22 |
7.0 |
|
|
Antibiotic prescribed as fixed dose combination |
|
|
Amoxicillin+potassium clavulanate (PO) |
25 |
11 |
|
(IV) |
4 |
1.7 |
|
Cefoperazone+sulbactum |
19 |
8.3 |
|
Ceftriaxone+sulbactum |
15 |
6.6 |
|
Ceftriaxone+tazobactum |
7 |
3.1 |
|
Piperacillin+tazobactam |
10 |
4.4 |
|
Others |
10 |
4.4 |
Prescribing indicators: The results for various indicators, including dose, dosing frequency (interval), duration of therapy, antibiotics prescribed with generic name and injection, the average number of antibiotics per encounter and antibiotics prescribed from EML are presented in Table 03.
Table 3. WHO prescribing indicators
|
Indicators of drug use |
Value |
WHO Optimal value |
|
Average number of antibiotics per encounter. |
1.3 |
1.6-1.8 |
|
Percentage of prescriptions with generic name. |
37.7% |
100% |
|
Number of encounters with an injection prescribed. |
48.3% |
13.4-24.1% |
|
Percentage of encounters with drugs prescribed from EML. |
82.7 |
100% |
|
Percentage of prescriptions with correct dosage. |
97.7% |
100% |
|
Percentage of prescriptions with correct duration. |
93.1% |
100% |
|
Percentage of prescriptions with correct frequency. |
98.6% |
100% |
Antibiotic prescribing pattern based on WHO “AWaRe” classification: Out of 228 antibiotics reviewed, the majority of antibiotic use was from the Access category (n=92, 40.40%), which aligns with WHO recommendations. However, the usage of Watch antibiotics was also notably high (n=85, 37.30%), The Reserve group accounted for only 0.40% (n=1) of use, suggesting appropriate restriction. A relatively high proportion (n=50, 21.90%) of antibiotics classified as Not Recommended, a category that predominantly comprises fixed-dose combination antibiotics. (Figure 03).
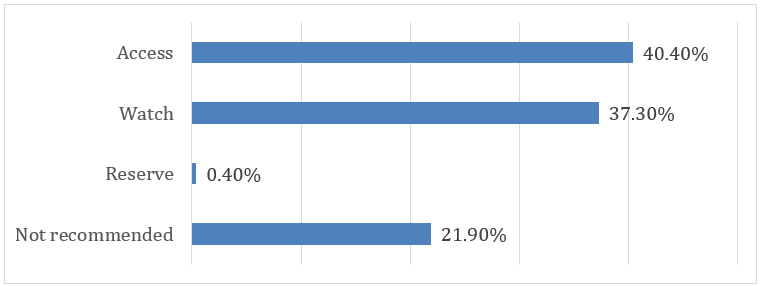
Figure 3. Classification of antibiotics as per WHO AWaRe classification
Knowledge on WHO-AWaRe classifications of Antibiotics among Prescribers: The study included 23 doctors from the General Medicine, respiratory, ENT and surgery departments, 52.2% males (n=12) and 47.8% females (n=11). Most were aged 25–35 years (78.3%, n=18), followed by 36–45 (17.4%, n=4) and 46–55 years (4.3%, n=1). The group consisted of 11 senior residents (47.8%) and 12 faculty members (52.2%). The majority had less than 5 years of experience (69.6%, n=16), with others having 11–20 years (17.4%, n=4), 5–10 years (8.7%, n=2), and over 20 years (4.3%, n=1). (Table 04)
Table 4. Prescribing doctors profile
|
Respondents’ characteristics |
Values n=23 (%) |
|
Age |
|
|
25-35 |
18 (78.3) |
|
36-45 |
4 (17.4) |
|
46-55 |
1 (4.3) |
|
Gender |
|
|
Male |
12 (52.2) |
|
Female |
11 (47.8) |
|
Designation |
|
|
Senior resident |
11 (47.8) |
|
Faculty |
12 (52.2) |
|
Number of years been practice |
|
|
Less than 5 years |
16 (69.6) |
|
5-10 years |
2 (8.7) |
|
11-20 years |
4 (17.4) |
|
More than 20 years |
1 (4.3) |
The pooled analysis revealed limited awareness and understanding of the WHO AWaRe classification among respondents. Only 39.1% had heard of it, and over half (54.5%) reported being not familiar. Objective knowledge was variable while 100% correctly identified amoxicillin as Access and 86.6% identified linezolid as Reserve, correct responses for other antibiotics ranged from 40% to 60%, indicating inconsistent understanding. The average knowledge score, based on a 10-point system, was moderate. Most participants (77.7%) supported implementing AWaRe to promote rational antibiotic use, and all (100%) agreed on the need for more education on AMR and the AWaRe framework. (Table 05)
Table 5. Pooled analysis of the Knowledge of AWaRe Classification questionnaire
|
Question related to respondents’ knowledge |
Values (%) |
Score |
|
1) Have you heard of WHO AWaRe classification of antibiotics? (n=23) |
|
|
|
Yes |
09 (39.1) |
9 |
|
No |
14 (60.9) |
0 |
|
2) How familiar are you with the AWaRe classification system? (n=22) |
|
|
|
Not familiar |
12 (54.5) |
12 |
|
Somewhat familiar |
06 (27.3) |
12 |
|
Familiar |
4 (18.1) |
12 |
|
Very familiar |
0 (0) |
0 |
|
3) Identify which category the following antibiotic belong to? (n=15) |
|
|
|
a) Amoxicillin: (correct response: Access)- Access |
15 (100) |
15 |
|
Watch |
0 (0) |
0 |
|
Reserve |
0 (0) |
0 |
|
b) Linezolid: (correct response: Reserve)- Access |
1 (6.7) |
0 |
|
Watch |
1 (6.7) |
0 |
|
Reserve |
13 (86.6) |
13 |
|
c) Ceftriaxone: (correct response: Watch)- Access |
07 (46.7) |
0 |
|
Watch |
08 (53.3) |
8 |
|
Reserve |
0 (0) |
0 |
|
d) Meropenem: (correct response: Watch)- Access |
0 (0) |
0 |
|
Watch |
06 (40) |
6 |
|
Reserve |
09 (60) |
0 |
|
e) Amikacin: (correct response: Access)- Access |
07 (46.6) |
7 |
|
Watch |
04 (26.7) |
0 |
|
Reserve |
04 (26.7) |
0 |
|
f) Piperacillin +tazobactam: (correct response: Watch)- Access |
3 (20) |
0 |
|
Watch |
09 (60) |
9 |
|
Reserve |
3 (20) |
0 |
|
4) Should AWaRe be used in the hospital to promote rational use of antibiotics and combat AMR? (n=18) |
|
|
|
Strongly Disagree |
1 (5.6) |
|
|
Disagree |
0 (0) |
|
|
Neutral |
3 (16.7) |
|
|
Agree |
08 (44.4) |
|
|
Strongly Agree |
06 (33.3) |
|
|
5) Do you feel we need more education on Antimicrobial Resistance and the AWaRe classification among healthcare prescribers? (n=20) |
|
|
|
Yes |
20 (100) |
|
|
No |
0 (0) |
|
DISCUSSION
Antibiotics are essential tool against bacterial infections, saving countless lives by effectively controlling and treating disease. However, when they are misused through overuse, incorrect prescribing, or improper patient adherence they contribute to the growing threat of AMR, making infections harder to treat and increasing the risk of severe illness and death. Monitoring prescribing patterns is essential to promote rational use and guide stewardship efforts. In the present study, males (50.5%) and females (49.5%) were nearly equally represented among those prescribed antibiotics, indicating no significant gender disparity in usage. These findings are consistent with those reported by Jokandan SS et al.,[8] who observed a slight male predominance but no substantial difference in antibiotic use between genders. The lack of significant gender disparity may be due to the fact that infections are common across both sexes, and treatment decisions are generally based on the nature and severity of the infection rather than on patient gender. Age-wise distribution showed most patients were aged 19–38 years (44.4%), followed by 39–58 years (35%), similar to findings by Jokandan SS et al.,[8] who also identified younger adults as the primary recipients of antibiotic prescriptions. This may reflect higher infection exposure and healthcare use among younger adults due to occupational and lifestyle factors[8]. Additionally, younger adults tend to self-report symptoms earlier and demand quicker relief, often prompting empirical prescriptions. Their increased mobility and social interaction further increase their infection risk. Without adequate diagnostic confirmation, this pattern could drive unnecessary antibiotic use and long-term resistance. General Medicine accounted for the highest proportion of antibiotic prescriptions (58.3%), followed by Respiratory Medicine (24.4%) and ENT (11.7%). This departmental distribution aligns with findings from a tertiary care hospital study in Andhra Pradesh, where Medicine and Pediatrics departments showed high antibiotic utilization, mainly due to the management of febrile illnesses and respiratory infections. The significant contribution of respiratory illnesses to antibiotic use emphasizes the need for targeted stewardship interventions in these departments[9]. The distribution of prescriptions between outpatient (51.7%) and inpatient (48.3%) settings was nearly balanced. This is comparable to data from a study in Mudenda et al.,[10] which reported outpatient prescriptions at 53.6% and inpatient at 36.4%. These findings highlight the pervasive use of antibiotics across both hospital settings, emphasizing the importance of monitoring in both areas. Outpatients often receive empirical antibiotics for mild infections, sometimes without diagnostic confirmation, increasing the risk of inappropriate use. In contrast, inpatients typically require broader-spectrum agents for severe or hospital-acquired infections. The complexity of care and longer hospital stays in IP settings further elevate the AMR risk. Therefore, both settings require tailored stewardship strategies and regular prescription audits to ensure rational antibiotic use. Respiratory tract infections and acute febrile illnesses were the most common indications for antibiotic use (27.2% each), followed by gastrointestinal (14.4%) and urinary tract infections (8.3%). Similar trends were noted by Mudenda et al.,[10] where respiratory infections (26.3%) were most common, followed by gastrointestinal and ENT infections. The high rate of respiratory infections may reflect factors like air pollution, socioeconomic conditions, and empirical antibiotic use, highlighting the need for improved diagnostics and prescriber education. Cephalosporins (29.4%) were the most frequently prescribed antibiotic class, followed by BL/BLI and tetracyclines. This aligns with findings from BGS Hospital, Bangalore, where cephalosporins accounted for 32.44% of prescriptions. The prevalent use of broad-spectrum agents, particularly third-generation cephalosporins and BL/BLI is concerning giving their association with rising antimicrobial resistance (AMR). These broad-spectrum antibiotics are useful, but using them too much can make bacteria stronger and harder to treat. This underscores the urgent need for robust antibiotic stewardship programs to promote rational prescribing and curb resistance trends[11]. The most commonly prescribed individual antibiotics in our study were Doxycycline (12.3%) Clarithromycin (7.5%), and Ceftriaxone (6.6%), along with fixed-dose combinations (FDCs) such as Cefoperazone + Sulbactam (8.3%). This finding is supported by the study by Rathinavelu et al.,[12] where Ceftriaxone was also the most frequently prescribed antibiotic, followed by Amoxicillin + Clavulanic acid and Azithromycin. The frequent use of broad-spectrum antibiotics, driven by their wide coverage, empirical use, and diagnostic uncertainty, contributes to AMR by disrupting microbial balance and promoting resistant strains. This reduces antibiotic effectiveness, limits treatment options, and increases the risk of treatment failure and prolonged illness. Our study showed rational antibiotic prescribing with an average of 1.26 antibiotics per prescription and a lower overall drug count (3.48), indicating reduced polypharmacy compared to Chenchula et al[13]. Generic prescribing was observed in 37.71% of cases, better than previous studies but still below the WHO target of 100%. Antibiotic use was high (86.85%), as was injection use (43%). Notably, adherence to the WHO-EML was 100%, reflecting strong compliance with national guidelines. While medicine selection and EML adherence were strengths, improvements are needed in generic and injectable antibiotic use[13]. The result of WHO AWaRe classification system align with those of Negi G et al.,[5] which also utilized the WHO AWaRe classification in a tertiary care setting. Both studies found a substantial proportion of prescriptions in the Access and Watch categories, with 40.4% in Access in our study, compared to 57.6% in Negi et al.,[5] and 37.3% in Watch, similar to their finding of 38.27%. These results reflect a common trend towards reliance on broad-spectrum antibiotics, raising concerns about potential resistance due to overuse. Both studies highlight the importance of promoting appropriate prescribing practices to ensure that Access antibiotics are prioritized while reducing unnecessary Watch antibiotic use. The present study reveals that 21.9% of prescribed antibiotics belonged to the Not Recommended category, with a predominant contribution from fixed-dose combinations (FDCs) such as Amoxicillin + Potassium Clavulanate, Cefoperazone + Sulbactam, and Ceftriaxone + Sulbactam. These findings closely align with the study by Kakumba JM et al.,[14] which reported that 20.3% of antibiotics prescribed in their study setting were also from the Not Recommended group. The consistency of these results across different regions and time periods highlights a significant and ongoing concern regarding irrational antibiotic prescribing practices. FDCs continue to dominate the Not Recommended category. Notably, Cefoperazone + Sulbactam appears in both our data and in the study by Bhardwaj A et al.,[15] despite having minimal justification based on pharmacological synergy or robust clinical outcomes. The persistently high proportion of Not Recommended antibiotic use may be attributed to several factors, including a lack of awareness of the WHO AWARE classification among prescribers, the continued marketing and availability of irrational FDCs, and inadequate implementation of AMSP at both institutional and policy levels. The present study involved 23 prescribers from the General Medicine department, including both senior residents (47.8%) and faculty members (52.2%). Despite their roles in frontline patient care, awareness of the WHO AWaRe classification was limited, only 39.1% of participants had heard of the classification system, and 54.5% were unfamiliar with its use. Similar knowledge gaps in antibiotic prescribing were reported by Negi et al.,[5] contributing to inappropriate antibiotic use. Both their findings and ours indicate a moderate level of awareness about AWaRe classification among healthcare professionals. This can be due to the factors such as limited training, high workloads, and inconsistent implementation of AMR guidelines. These challenges highlight the need for focused education programs and more effective integration of AMR protocols into daily clinical practice. With the widespread use of antibiotics and rising issues with the increase of AMR in developing countries, it is important to help physician better understand and adopt tools like AWaRe classification for antibiotics which is the key step toward more responsible and effective antibiotics prescribing. The physicians preferred AWaRe classification tool in the study conducted by Hassan H et al.,[16] for better antibiotic selection, supporting the successful implementation of AMSP. In our study, while most participants correctly identified Amoxicillin (Access) and Linezolid (Reserve) classification, accuracy for other antibiotics was inconsistent (40–60%), which is consistent with findings from Mudenda et al[10] in Zambia. Despite these knowledge gaps, 77.7% of participants supported the implementation of the AWaRe classification, and all respondents expressed support for the need for further education. Similar positive attitudes towards educational interventions were noted by Priyadharsini et al[17]. These results point out to the importance of targeted education and awareness initiatives to promote appropriate antibiotic use, which could significantly improve prescribing practices and contribute to combating AMR.
CONCLUSION
This study provides valuable insights into trends in prescribing antibiotics at a tertiary care hospital through a dual approach combining prescription pattern analysis with an assessment of prescriber’s knowledge of the WHO AWaRe classification. A key positive finding was adherence to the National Essential Medicines List and a low rate of polypharmacy, reflecting rational prescribing habits. However, suboptimal use of generic names and a high rate of injectable antibiotic prescriptions highlight areas needing targeted improvement. While the encouraging use of Access antibiotics indicates progress, the predominance of respiratory tract and febrile illnesses as common indications underscores the need for improved diagnostic accuracy to reduce unnecessary empirical antibiotic use. Additionally, we observed limited awareness and inconsistent application of the AWaRe classification, particularly among early-career prescribers. Despite this, the general willingness of clinicians to adopt rational antibiotic use principles presents a promising opportunity for intervention. To further enhance prescribing quality and combat antimicrobial resistance, it is essential to implement continuous education programs, integrate AWaRe guidelines into clinical protocols, and conduct regular prescription audits as part of a robust antimicrobial stewardship program. Strengthening these strategies will support more rational antibiotic use and contribute significantly to global efforts against antimicrobial resistance. One limitation of this study is its single-center design and relatively small sample size, which may affect the generalizability and statistical power of the findings. Nonetheless, the comprehensive methodology offers valuable real-world insights into antibiotic use trends and healthcare professionals’ awareness, forming a strong foundation for future stewardship initiatives.
ACKNOWLEDGMENTS
The authors express their sincere gratitude to the physicians and staff of Siddaganga Medical College and Research Institute (SMCRI) for their cooperation and support during the data collection phase of this study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
ETHICAL APPROVALS
The study was approved by the Institutional Ethics Committee of SMCRI (approval ID. SMCRI/IEC/2023-2024/48).
REFERENCES




Renushri B.V.*, Umea Hani B., Dinesh Kumar V., Mohammed Mateen Maaz, The Prescribing Pattern of Antibiotics Agents in Adult Population Using Who Aware Classification in a Tertiary Care Hospital, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2102-2115 https://doi.org/10.5281/zenodo.17394497
 10.5281/zenodo.17394497
10.5281/zenodo.17394497
