IQVIA, San Francisco, California, USA
Real-world evidence (RWE) has been a keenly desired complement to randomized controlled trials (RCTs) in oncology drug development, offering essential information on the treatment's efficacy in real-world clinical practice environments. The review systematically reviewed the peer-reviewed literature published 2019 through 2024 in order to characterize the role of RWE in drug development, regulatory clearance, and methodological refinement. The evidence demonstrates that RWE is increasingly being applied along the continuum of drug development, and regulatory authorities are increasingly placing value on it - 13 of 706 oncology drug approvals in 2015 through 2020 were approved on the basis of RWE. Its most important applications are external control arms in single-arm trials, post-market surveillance, and evidence in support of clearance in the rare tumors in which RCTs are typically not practical. Even though RWE potentially facilitates expedited clearance of a drug, cost reduction, and evidence in support of underrepresented populations, in order to be fully utilized, challenges with data standardization, quality control, and methodological consistency are needed to be overcome.
The oncology product development paradigm has been transformed in the past decade, driven by advances in precision medicine, molecular diagnostics, and personalized therapeutic approaches[1]. Traditional randomized controlled clinical trials (RCTs), though still considered the ultimate proof tool for establishing efficacy and safety of medicines, are faced increasingly in the modern-day cancer therapy era by several challenges. These include stringent eligibility criteria excluding large proportions of real-world patient populations, exorbitance, lengthy durations, and challenges in recruitment of patients with rare forms of cancer[2]. Real-world evidence (RWE) emerged as a complement to traditional clinical evidence developed through data obtained under routine clinical practice conditions, and inferences are made on the effectiveness, safety, and value of therapies through it[3]. The description by the FDA of real-world data (RWD) is that of patient health status and healthcare provision data that are gathered in a systematic fashion from a single or more than a single source, including electronic health records (EHRs), medical claims databases, patient registries, and electronic health technologies. RWE is utilized as a term in reference to clinical evidence developed through analysis of RWD[4].
1.1. Problem Statement
The larger and more broad-based oncology drug development, and greater diversity and representativeness in evidence needed, have left wide gaps among populations within clinical trials and real-world cancer patients in clinical practice. Research has established that 40% of the patients within registries for cancer would be excluded from typical clinical trials by general exclusion rates[5]. This gap in evidence erodes trial outcome generalizability and generates uncertainty regarding treatment effectiveness in daily clinical practice. In addition, escalating oncology care costs and greater focus on value-based models of healthcare delivery require evidence that goes beyond conventional efficacy endpoints to encompass real-world effectiveness, quality of life measures, and economic burden[6]. The need for evidence generation has also been heightened by the COVID-19 pandemic, which unsettled conventional clinical trial execution and underscored the necessity for adaptable, flexible evidence generation methods.
Table 1: Summary of Most Impactful Citations Contributing to This Review
|
Title |
Authors |
Publication/ |
Year |
Citation |
|
Use of Real-World Evidence to Support FDA Approval of Oncology Drugs |
B. A. Feinberg, A. Gajra, M. E. Zettler, et al. |
Value in Health |
2020 |
[2] |
|
Real-world evidence in support of oncology product registration: A systematic review |
B. Arondekar, M. S. Duh, R. H. Bhak, et al. |
Clinical Cancer Research |
2022 |
[3] |
|
Artificial intelligence to unlock real-world evidence in clinical oncology |
A. K. Bryant, R. Zamora-Resendiz, X. Dai, et al. |
Cancer Medicine |
2024 |
[1] |
|
Real-world evidence in new drug and biologics license application approvals |
G. K. Innes, K. A. Smith, A. Kuzucan, et al. |
Clinical Pharmacology & Therapeutics |
2024 |
[9] |
|
The use of real-world evidence to support FDA post-approval study requirements |
M. E. Zettler |
Expert Review of Anticancer Therapy |
2022 |
[11] |
|
The role of real-world evidence in FDA-approved new drug and biologics license applications |
C. A. Purpura, E. M. Garry, N. Honig, et al. |
Clinical Pharmacology & Therapeutics |
2022 |
[10] |
|
Real-world data for clinical evidence generation in oncology |
S. Khozin, G. M. Blumenthal, & R. Pazdur |
Journal of the National Cancer Institute |
2017 |
[7] |
|
A systematic review of real-world evidence supportive of new drug approvals in rare diseases |
S. Vaghela, K. A. Tanni, G. Banerjee, & V. Sikirica |
Orphanet Journal of Rare Diseases |
2024 |
[12] |
|
Real-world evidence and real-world data for evaluating drug safety and effectiveness |
J. Corrigan-Curay, L. Sacks, & J. Woodcock |
JAMA |
2018 |
[8] |
|
Real-world evidence — what is it and what can it tell us? |
R. E. Sherman, S. A. Anderson, G. J. Dal Pan, et al. |
New England Journal of Medicine |
2016 |
[6] |
1.2 Research Objectives
2. METHODOLOGY
This extensive review was conducted by undertaking a systematic examination of peer-reviewed literature from 2019 to 2024, with an emphasis on RWE application in oncology drug development. The literature was searched across various databases and focused on studies investigating regulatory applications of RWE, methodological challenges, and emerging technology in treating cancer. Inclusion included original research reports, systematic reviews, regulatory guidance documents, and case studies on the use of RWE in oncology drug development, approval processes, or post-marketing surveillance. Not included were studies before 2019, non-oncologic use with no direct relationship to cancer care, or industry white papers that were not peer published. Data extraction was on study design characteristics, drug development phase applications of RWE, regulatory effects, methodological concerns brought up, and future research recommendations. Quality was judged by applying prevailing schemes in rating regulatory science evidence and real-world evidence.
3. RESULTS
3.1. Current Applications Across Drug Development Stages
3.1.1. Discovery and Early Development
RWE application in early oncology clinical development has been extraordinarily pragmatic in the search for targets and biomarkers. Examination through large-scale genomic sequencing and longitudinal clinical endpoints has made it possible to identify sets of high-responding patients and biomarkers of therapeutic response and resistance[7]. The method has been most productive in oncology, in which more decisions on how to treat are made on a patient and tumor-specific molecular basis. Extraction from electronic clinical notes has made it possible to characterize disease burden and recognize unmet need in well-defined populations of patients. In rare presentations of cancer, RWE has made it possible to obtain crucial epidemiologic data that are impossible by prospective clinical outcome trails within time horizons considered reasonable[8].
3.1.2. Clinical Trial Design and Optimization
Real-world evidence has transformed clinical trial designs by various mechanisms. Protocol optimization by the use of RWE gives development of eligibility criteria achieving a balance among scientific rigor and generalizability in routine clinical practice in the real world. Trends in routine everyday clinical practice have informed dosing regimen, frequency of assessment, and choice of endpoints as a reflection of routine clinical care provision [9]. Site feasibility and selection have been optimized by RWE evaluation among potential sites by the patient populations themselves. This has reduced screen failure rates and afforded quick enrollment time through designation of the appropriate patient populations and clinical capacity in sites [10].
3.1.3. External Control Arms and Single-Arm Trials
Arguably the most important regulatory use of RWE in oncology has been the utilization of external control arms to validate single-arm trial designs. This has proved especially useful in rare cancers for which randomized trials are impractical because of limited patient numbers and ethical issues involving withholding potentially beneficial treatments in control arm participants [11]. Between 2015 and 2020, analysis of FDA oncology drug approvals revealed that 13 of 706 approvals included RWE as supporting evidence, with external control studies being the most common application [12]. These approvals demonstrated the feasibility of using historical controls derived from real-world data to provide context for single-arm trial results, particularly in settings with well-characterized natural history and established standard of care treatments.
Table 2: Applications of Real-World Evidence Across Oncology Drug Development Stages
|
Development Stage |
RWE Applications |
Primary Data Sources |
Key Benefits |
|
Discovery |
Target identification, biomarker discovery |
Genomic databases, EHRs |
Identify high-responding cohorts |
|
Early Development |
Disease characterization, unmet need assessment |
Cancer registries, claims data |
Inform trial design and endpoints |
|
Clinical Development |
External control arms, protocol optimization |
EHRs, registries |
Reduce trial size and duration |
|
Regulatory Submission |
Supporting efficacy evidence, safety data |
Multiple integrated sources |
Enable approval in rare indications |
|
Post-Marketing |
Safety surveillance, effectiveness studies |
Claims, EHRs, registries |
Monitor real-world performance |
Table 2 illustrates the range of uses of real-world evidence throughout all phases of oncology drug development, with the major sources of data and major advantages at each phase.
3.2. Regulatory Acceptance and Framework Development
3.2.1. FDA Leadership and Guidance
The FDA Oncology Center of Excellence (OCE) has developed a specialized Real World Evidence Program aimed at facilitating proper use of RWD for oncology product development [13]. The program has formed several research collaborations and published guidance documents on standards for data quality, study design factors, and regulatory submission specifications for RWE studies. The 21st Century Cures Act of 2016 gave legislative authority to FDA to create guidelines for the use of RWE for regulatory decision-making.
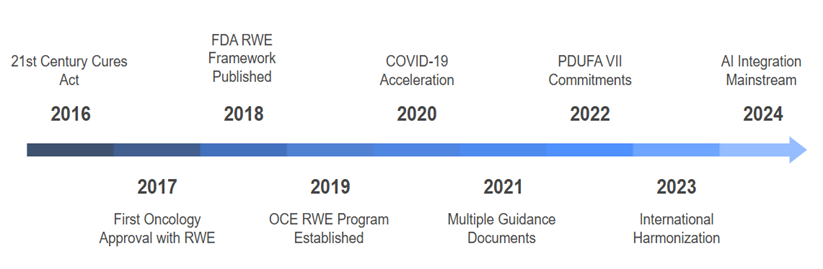
Figure 1: Timeline of Regulatory Milestones for RWE in Oncology
Figure 1 graphically depicts the swift development of regulatory acceptance and framework evolution for real-world evidence in oncology drug development, depicting significant milestones from legislative mandate to the present AI integration.
3.2.2. International Regulatory Harmonization
Regulatory acceptance of RWE has grown worldwide, with the European Medicines Agency (EMA) and other world-wide regulatory agencies creating parallel frameworks and guidance documents. The EMA review of marketing authorization applications for 2018-2019 reported that RWE was featured in all phases of oncology drug development, including discovery to post-authorization lifecycle management.
3.3. Data Sources and Infrastructure
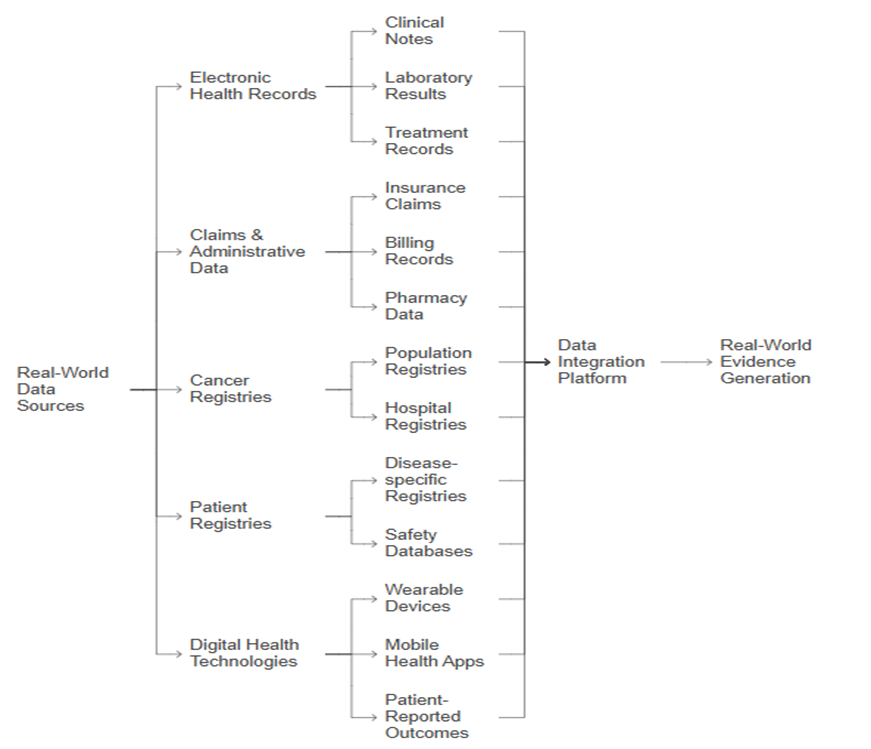
Figure 2: Real-World Data Sources and Integration in Oncology
Figure 2 illustrates the wide range of real-world data in oncology and its integration into end-to-end platforms for evidence generation, illustrating the complexity and interconnectedness of contemporary RWD infrastructure.
3.3.1. Electronic Health Records
Electronic health records are the largest source of real-world evidence data for oncology use cases, offering complete longitudinal patient data such as diagnoses, treatments, laboratory findings, and clinical outcomes. EHR platforms in specialized oncology have developed advanced features for collecting cancer-specific data elements, such as staging details, biomarker test results, and response to treatment. Some of the quality issues for RWE derived from EHR include completeness of data, standardized terminology and coding systems, and validation of critical clinical endpoints. Privacy protection frameworks should be a necessity while carrying out multi-institutional oncology RWE studies involving sensitive genomic and treatment information of patients [13]. Sophisticated natural language processing and artificial intelligence technologies are increasingly used to extract structured data from unstructured clinical reports and notes.
3.3.2. Claims and Administrative Databases
Healthcare claims databases allow for population-level coverage and long-term follow-up capacity, making them useful for large-scale effectiveness and safety studies. Disadvantages include a lack of clinical detail, possible coding errors, and not being able to capture over-the-counter medications or treatment received outside the claims system.
3.3.3. Cancer Registries and Specialized Databases
Population-based cancer registries offer excellent data on cancer incidence, stage at diagnosis, treatment, and survival. These registries have special utility in studies of rare cancers and in long-term survival analysis. Combination of registry information with other sources of real-world data has expanded the reach and quality of RWE studies.
3.4. Methodological Challenges and Quality Considerations
3.4.1. Data Quality and Standardization
Quality data assurance is among the most significant oncology RWE study challenges. Particular emphasis should be placed on missing data management, outcome definition standardization, and validation of critical endpoints such as progression-free survival and overall response rate. It has been recommended by regulations to have pre-specified study protocol, clear inclusion and exclusion criteria, and confounding minimization and measurement of confounding variable accounting by regulatory recommendations.
Table 3: Methodological Challenges and Solutions in Oncology RWE Studies
|
Challenge |
Impact |
Current Solutions |
Future Directions |
|
Data Quality |
Incomplete/ inaccurate data |
Validation algorithms, data cleaning |
AI-powered quality assurance |
|
Missing Data |
Reduced study power |
Multiple imputation, sensitivity analysis |
Real-time data collection |
|
Confounding |
Biased effect estimates |
Propensity scoring, instrumental variables |
Machine learning adjustment |
|
Endpoint Definition |
Inconsistent outcome measurement |
Standardized definitions, validation |
Automated endpoint detection |
|
Causal Inference |
Uncertain causality |
Target trial emulation |
Advanced causal methods |
Table 3 summarizes the key methodological challenges of oncology RWE studies and the emerging solutions in development to overcome these limitations.
3.4.2. Study Design and Analytical Considerations
Retrospective observational analyses, which form the bulk of present-day oncology RWE use cases, have inherent biases such as selection bias, confounding by indication, and incomplete capture of data. Advanced methods like propensity score matching, instrumental variable analysis, and emulation of target trial have been developed as a means of addressing these biases. The "fit-for-purpose" concept of evidence has emerged as a philosophic principle, recognizing different regulatory and clinical questions require different levels of evidence quality and methodological intensity. This provides appropriate use of RWE without compromising scientific standards for regulatory decisions.
3.5. Integration with Artificial Intelligence and Machine Learning
3.5.1. Natural Language Processing and Data Extraction
Artificial intelligence technology has greatly increased the possibility and extent of oncology RWE research through the automated extraction of data from clinical unstructured text. Natural language processing algorithms can recognize and extract pertinent clinical concepts such as disease stage, response to treatment, and adverse reactions from physician notes, pathology reports, and radiology reports. Machine learning techniques have been showing better performance than classical rule-based approaches in a variety of clinical data extraction problems, and they have made it possible to analyze larger datasets in a more accurate and consistent way.
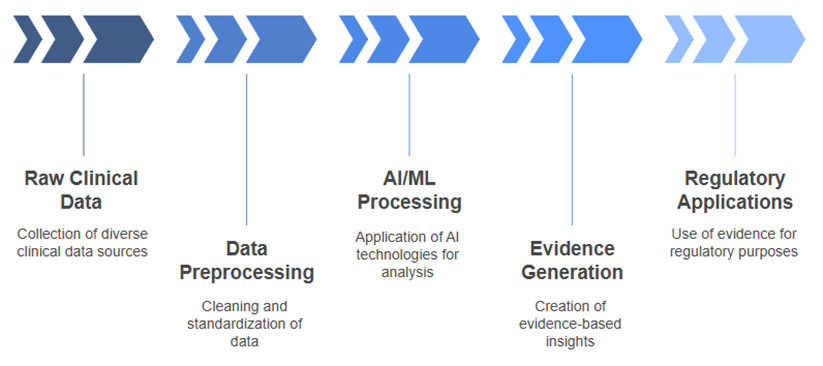
Figure 3: AI-Enhanced Real-World Evidence Generation Pipeline
Figure 3 depicts how the integration of machine learning and artificial intelligence technologies into the real-world evidence generating pipeline advances data processing and more complex evidence generating capabilities in regulatory applications.
3.5.2. Predictive Modeling and Risk Stratification
AI-augmented RWE analyses have made it possible to develop advanced prediction models for treatment response, survival, and toxicity risk. These models integrate highly multimodal datasets such as genomic data, imaging data, and longitudinal clinical variables in order to enable personalized prediction and prognosis. Real-time risk prediction models embedded in electronic health record systems have demonstrated promise for clinical decision support, allowing for the recognition of high-risk patients and the tailoring of treatment approaches based on unique patient characteristics.
4. DISCUSSION
4.1. Current Capabilities and Regulatory Impact
The application of RWE to the creation of oncology medicines has impacted regulatory decision-making and access to new treatments by patients. FDA application of RWE to guide drug approvals, especially for rare cancer conditions, has shortened development time and facilitated approval of treatments that may otherwise not have had enough clinical trial evidence to justify them. The COVID-19 pandemic hastened the use of RWE approaches, as inpatient clinical trial conduct was dramatically impacted. The process was, however, able to demonstrate the effective use of flexible and agile evidence generating approaches, which are efficient and effective and can be sustained in environments that are unsupportive.
4.2. Limitations and Challenges
Despite Herculean efforts, there are specific serious gaps in current RWE applications. Data quality and data completeness represent a threat to the rigor of RWE research. This is most completely true in the case of complex clinical endpoints such as progression-free survival requiring precise time-definition and consistency in evaluation criteria. These are methodological issues of sufficient management of missing data, adjustment for confounding, and making cause-and-effect inferences on the basis of observational data. Source variability in real-world data as well as methodological variability in analytical techniques have precluded the development of routine methodologies and quality standards.
4.3. Economic and Access Considerations
RWE has been promising in the saving of cost and time in drug development through more efficient study designs and smaller, less costly randomized studies. Front-end expenses entailed in infrastructure investment required in reaching RWE at a high level, i.e., in data standardization, technological platform, and analytical capability, are lofty ones, however. The intercountry inequity in healthcare data infrastructure and regulatory status has translated into inequities in RWE capability by region and by health system. Such inequities are going to require closing if globally, in oncology drug development, the promise of RWE is going to be realized.
4.4. Quality Framework Development
The earlier work was intended as a contribution to efforts on quality standards and quality oncology RWE study designs. The European Society for Medical Oncology Guidance on the Reporting of Oncology Real-World Evidence (ESMO-GROW) published reporting standards on publicly reporting RWE studies, and several organizations issued a description on how data and study design quality could be assessed.
5. FUTURE OPPORTUNITIES AND POTENTIAL
5.1. Technological Advancement Integration
The extension of RWE ability has great potential in the crossing over into new areas such as electronic health platforms, machine learning, and artificial intelligence. Real-time data collection through wearable devices, patient-reporting outcome platforms, and electronic biomarkers potentially offer a more comprehensive and expedited understanding of effect on therapy and patient experience. Blockchain and distributed ledger systems potentially enable data sharing and privacy protection, offering numerous institutions and healthcare systems an opportunity to collaborate on RWE studies with coverage of patient confidentiality and data security.
5.2. Precision Medicine and Personalized Care
The intersection of genomic medicine and molecular diagnostic and RWE can enable innovation of strategies in precision oncology. Through application of large-scale genomic data and longitudinal paired clinical follow-up, therapy targets and biomarkers can be confirmed and defined and evidence can be produced in support of individualized regimens of treatment. Experimental evidence science work based on data in molecular profiling has already been shown effective in the definition of patient subgroups most likely to benefit from precise therapies and in guiding development of companion diagnostic and precision medicine strategies.
5.3. Global Health and Access Equity
RWE approaches can bridge healthcare gaps and broaden coverage on novel oncology treatments in low-resource settings. The in-country developed data collection processes and analytical procedures could support evidence development in situations in which it is impossible or infeasible for conventional clinical trials. Data sharing and worldwide collaboration could adopt RWE and address worldwide oncologic burden globally with a commitment that different patient populations and systems of healthcare are included in evidence development.
5.4. Regulatory Evolution and Harmonization
Subsequent regulatory advancements are most likely on the horizon in harmonizing standards and requirements on RWE by the world regulatory bodies. Harmonization in this area would enable having common plans in drug development and sanction the same evidence requirements with flexibility in data systems and infrastructure for data in the healthcare on the regional level. Creation of adaptive regulatory pathways in a product lifecycle, from initial first-time approval and post-marketing surveillance up to label extension, presents a profound potential in obtaining a more responsive and efficient regulatory outcome.
CONCLUSION
Real-world evidence has been a cornerstone in recent oncology product development as complementary evidence in favor of classical clinical evidences and filling informative gaps in oncology patient treatment. Demonstrated regulatory acceptance in product approvals by RWE, particularly in orphan therapies in oncology, has validated the scientific and practical value of the methodology. Applications range from the early development stage of a product during discovery and drug/target identification, through post-marketing surveillance and monitoring of drug safety. Combining artificial intelligence and machine learning capabilities has widened the scope and increased the feasibility of RWE analyses while overcoming conventional limitations of observational studies. However, the primary challenges are standardizing data quality, methodology, and the development of infrastructures. These will be overcome through ongoing interagency cooperation between regulatory agencies, higher education institutions, healthcare systems, and technology companies to develop strong frameworks for the generation and analysis of RWE. The future prospect of RWE in oncology is promising with the potential to enhance precision medicine strategies, expand access to novel therapies across the world, and to accelerate cancer care development at a quicker rate. To achieve this prospect, there will be a need for long-term data infrastructure investment, analytic capacity, and international coordination to maintain RWE on its true end point, and that is to optimize outcomes for cancer patients across the world.
REFERENCES

Hemanth Dandu, The Role of Real-World Evidence in Oncology Drug Development: Current Capabilities and Future Potential, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2869-2879. https://doi.org/10.5281/zenodo.17193786
 10.5281/zenodo.17193786
10.5281/zenodo.17193786
