Department of Pharmaceutical technology, JIS University
People with type 1 diabetes require insulin therapy to control their blood glucose levels, and advanced type 2 diabetes patients frequently take it as well. The traditional method of delivering insulin is subcutaneous injection with a hypodermic needle or pump-mediated infusion, although these methods may cause pain, needle anxiety, poor adherence, and an increased risk of infection. Transdermal insulin administration has so been extensively researched as a desirable alternative to subcutaneous techniques for the management of diabetes in recent years. Transdermal methods that deliver controlled, continuous insulin release and limit insulin breakdown may be preferable for patients and improve adherence and glycemic results. Due to the protein drug's high molecular weight, passive insulin absorption via the skin is inefficient, which presents a problem for transdermal insulin delivery. In this review, we concentrate on the many transdermal insulin administration strategies, including chemically promoted, electrically enhanced, mechanical force-triggered, and microneedle-assisted ones, along with their corresponding benefits and drawbacks.
Transdermal insulin delivery is a novel drug delivery method that offers an alternative to traditional insulin injections for people with diabetes. The transdermal delivery of insulin involves the use of patches that are applied to the skin and release insulin over a period of time. This method of insulin delivery is still in development and is not yet widely available, but has the potential to improve the management of diabetes by offering a more convenient and less painful alternative to injections [1]. Insulin is a hormone that is produced by the pancreas and helps to regulate the level of glucose in the blood. In people with diabetes, the body either does not produce enough insulin or is unable to use insulin effectively, which can lead to high blood glucose levels. Insulin therapy is used to help manage diabetes by replacing the missing insulin or helping the body use insulin more effectively. Traditional insulin therapy involves injections of insulin, which can be painful and inconvenient for many people [2]. Transdermal insulin delivery offers a potential solution to these issues. The transdermal insulin patch is designed to be applied to the skin and release insulin over a period of time, typically for several days. This offers a more convenient and less painful method of insulin delivery, and could potentially improve adherence to insulin therapy and glucose control in people with diabetes [3]. The development of transdermal insulin delivery has been ongoing for several decades, but has been hampered by a number of challenges. One of the main challenges has been developing a patch that can deliver insulin effectively and consistently. Insulin is a large molecule that does not easily penetrate the skin, and developing a patch that can deliver insulin in a consistent and predictable manner has been a significant hurdle [4]. There have been several approaches to developing transdermal insulin delivery systems. One approach involves using microneedles, which are tiny needles that can be used to penetrate the skin and deliver insulin directly to the underlying tissue [5]. Microneedle patches have been shown to be effective in delivering insulin, but the needles can be painful and may cause skin irritation [6]. Another approach involves using a chemical enhancer, which can be used to increase the permeability of the skin and allow insulin to be absorbed more effectively. This approach has been successful in some animal studies, but has not yet been shown to be effective in humans [7]. There are also several different types of transdermal insulin patches that are currently in development. One type of patch uses a reservoir system, in which insulin is stored in a reservoir within the patch and released through a small opening. Another type of patch uses a matrix system, in which insulin is dispersed throughout the patch and released as the patch comes into contact with the skin [8].
Administration (FDA) approved the first transdermal insulin patch for use in people with diabetes [9]. The patch, called V-Go, is a disposable patch that is worn on the skin and delivers a continuous dose of insulin over a 24-hour period. The patch is changed daily and is designed to be a more convenient and less painful alternative to insulin injections [10]. Other companies are also developing transdermal insulin delivery systems. One company, Zosano Pharma, is developing a patch that uses micro-projection technology to deliver insulin through the skin. The patch is applied to the skin and uses small, painless micro-projections to deliver insulin to the underlying tissue [11]. The company has completed several clinical trials of the patch and is currently seeking approval from the FDA. There are several potential benefits to transdermal insulin delivery for people with diabetes. One of the main benefits is convenience. Transdermal insulin patches can be worn for several days, which eliminates the need for daily insulin injections. This can make insulin therapy more convenient [12].
AIM& OBJECTIVE:
The aim of this review paper is to deliver insulin through transdermal route of administration while taking mechanical force triggered delivery system into action. The objective of this review is to deliver insulin inside the body through transdermal route other than the conventional one.Make a easy way of insulin delivery along with reducing pain and hazardless while injecting insulin and apply one of the novel drug delivery system approach in insulin delivery.
DIABETES
Diabetes is a chronic condition characterized by high blood sugar levels that result from the body's inability to properly produce or use insulin. Insulin is a hormone that regulates blood sugar levels and is produced by the pancreas [13]. Common symptoms of diabetes include increased thirst, frequent urination, blurred vision, fatigue, and slow wound healing. If left untreated, diabetes can lead to serious complications such as heart disease, kidney disease, and nerve damage [14].
CLASSIFICATION OF DIABETES MELLITUS
Type 1 diabetes
Type 1 diabetes is a chronic autoimmune disease in which the body's immune system attacks and destroys the insulin-producing beta cells in the pancreas. As a result, the body is unable to produce insulin, a hormone that regulates blood sugar levels. This leads to high levels of glucose in the blood, which can cause a variety of health problems. Type 1 diabetes is usually diagnosed in children and young adults, but it can occur at any age. The exact cause of type 1 diabetes is not known, but it is thought to be a combination of genetic and environmental factors [15]. The symptoms of type 1 diabetes include increased thirst, frequent urination, extreme hunger, weight loss, fatigue, blurred vision, and slow healing of cuts and bruises. If left untreated, type 1 diabetes can leads to serious health complications, including nerve damage, kidney damage, eye damage, and an increased risk of heart disease and stroke [16].
Type 2 diabetes
Type 2 diabetes is a chronic metabolic disorder in which the body becomes resistant to the effects of insulin or does not produce enough insulin to maintain normal blood sugar levels. Type 2 diabetes is the most common form of diabetes and typically develops in middle-aged or older adults, although it can occur at any age [17]. The exact cause of type 2 diabetes is not known, but it is thought to be related to a combination of genetic and environmental factors, including obesity, lack of physical activity, and a diet high in refined carbohydrates and sugars [18].
The symptoms of type 2 diabetes include increased thirst, frequent urination, fatigue, blurred vision, slow healing of cuts and bruises, and tingling or numbness in the hands or feet. However, many people with type 2 diabetes do not experience any symptoms and are only diagnosed through routine blood sugar testing [19].
INSULIN
Insulin was first discovered in 1921 by Canadian scientists Sir Frederick Banting and Charles Best [20]. Banting and Best, along with their colleagues John James Macleod and James Collip, were investigating the role of the pancreas in diabetes when they made the breakthrough discovery. Their experiments involved surgically removing the pancreas from dogs and then attempting to extract a substance from the pancreas that could be used to treat diabetes. After several failed attempts, they eventually discovered a method for extracting insulin from the pancreas of cows and pigs [21].
In 1922, the team successfully treated a 14-year-old boy with severe diabetes using insulin, marking the first successful use of insulin to treat diabetes in a human. The discovery of insulin revolutionized the treatment of diabetes and has since saved countless lives around the world. Banting and Macleod were awarded the Nobel Prize in Physiology or Medicine in 1923 for their discovery [22]. Insulin is a hormone produced by the pancreas that plays a crucial role in regulating the metabolism of glucose in the body. Insulin helps to lower the level of glucose in the blood by stimulating the uptake and utilization of glucose by cells throughout the body. This hormone is essential for the body's ability to use carbohydrates, fats, and proteins for energy and to maintain normal blood sugar levels. Insulin is available in various forms, including rapid-acting, short- acting, intermediate-acting, and long-acting formulations, which differ in their onset and duration of action. The type of insulin prescribed and the dose needed may vary depending on the individual's blood sugar levels, dietary habits, physical activity, and other factors [23]
Chemical properties and Structure of Insulin:
Insulin is a peptide hormone composed of two polypeptide chains, A chain and B chain, which are linked by disulfide bonds. The A chain contains 21 amino acids, while the B chain contains 30 amino acids, and the two chains together contain a total of 51 amino acids (Fig-1) [24]. The sequence of these amino acids determines the three-dimensional structure of the insulin molecule. The insulin molecule has a unique shape, with a central core formed by the B chain, surrounded by two extended arms formed by the A chain. Insulin is a relatively stable molecule, with a melting point of around 60-70°C, and is soluble in water and dilute acids. It is stable in acidic pH, but undergoes rapid denaturation and aggregation at alkaline pH. Insulin is sensitive to heat, acid, and proteolytic enzymes [25].

Fig 1: Insulin
Insulin synthesis & secretion:
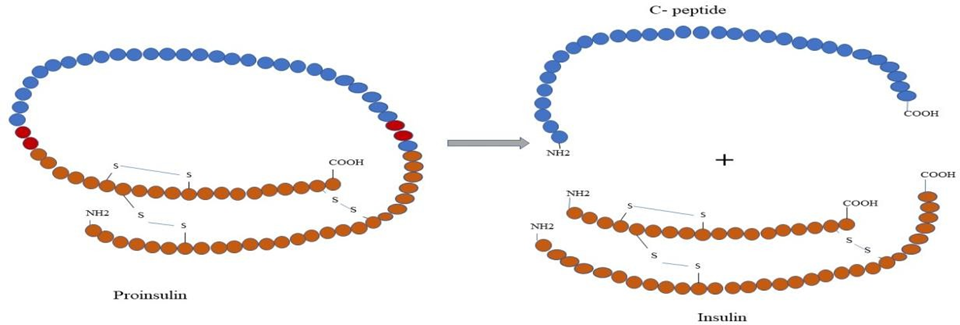
Fig 2: Synthesis of Insulin
Only the beta cells in the pancreas produce large amounts of insulin. Proinsulin is produced when the signal peptide from the insulin mRNA is removed after insertion into the endoplasmic reticulum [26]. Insulin mRNA is translated as a single-chain precursor called pre-proinsulin. It is composed of three domains: an amino-terminal B chain, a carboxy- terminal A chain, and a connecting peptide in the middle (Fig2). As proinsulin passes through the endoplasmic reticulum, several specific endopeptidases excise the C peptide, thus producing mature insulin. Free C peptide and insulin are packaged in the Golgi into secretory granules and accumulate in the cytoplasm [27]. When the beta cell is stimulated appropriately, insulin is secreted by exocytosis and diffuses into the islet capillary blood. The C peptide is also secreted into the bloodstream, but it is not known to have any biological properties. The secretion of insulin is primarily prompted by elevated blood glucose levels. The reason for this is that insulin facilitates glucose entry into cells. Additionally, certain neural stimuli (e.g., sight and taste of food) and increased blood concentrations of other fuel molecules, such as amino acids and fatty acids, stimulate insulin release [28].
Diabetes is part of a larger global epidemic of non- communicable diseases. It has become a major public health challenge globally. This disease affects 6.6% (285 million people) of the world's population in the 20-79 years age group [29]. According to the International Diabetic Federation (IDF), this number is expected to grow to 380 million by 2025 [30]. The IDF published findings revealing that in 2007, the country with the largest numbers of people with diabetes is India (40.9 million), followed by China (39.8 million), the United States (19.2 million), Russia (9.6 million) and Germany (7.4 million) [31]. Diabetes is a significant health concern in India, with an estimated 77 million adults (aged 20- 79) living with diabetes in 2019. India has the second-highest number of people with diabetes in the world, after China. The prevalence of diabetes in India has been rising rapidly over the past few decades, primarily due to changes in lifestyle and diet, as well as increasing urbanization and sedentary lifestyles. According to the International Diabetes Federation, the prevalence of diabetes in India is projected to increase to 101.2 million by 2030 [32]. One of the most concerning aspects of diabetes in India is the high number of undiagnosed cases. It is estimated that over 50% of people with diabetes in India are unaware of their condition, which can lead to complications such as blindness, kidney disease, and cardiovascular disease [33]. Type 2 diabetes is the most common form of diabetes in India, accounting for approximately 90% of all cases. Risk factors for diabetes in India include a high prevalence of obesity, physical inactivity, and an unhealthy diet [34]. Disease patterns in India mortality from communicable, maternal, neonatal, and nutritional illnesses (CMNNDs) has fallen dramatically, whilst NCDs and injuries have significantly increased their proportion to overall disease burden and mortality. This reversal is the result of
an epidemiological transition. The total disability-adjusted life years (DALYs) from CMNNDs, NCDs, and injuries in India in 1990 were 61%, 30%, and 9%, respectively. The overall DALYs from CMNNDs have, however, fallen to 33% due to significant epidemiological changes in India over time, whereas those from NCDs and injuries have climbed to 55 and 12%, respectively, in 2016 (Fig-3). When compared to the top individual causes of DALYs in India, most NCDs have seen an increase in rank since 1990, with diabetes exhibiting a substantial increase, moving from 35th place in 1990 to 13th place in 2016. The disease burden or DALY rate for diabetes across India was four times higher in 2016 [35].
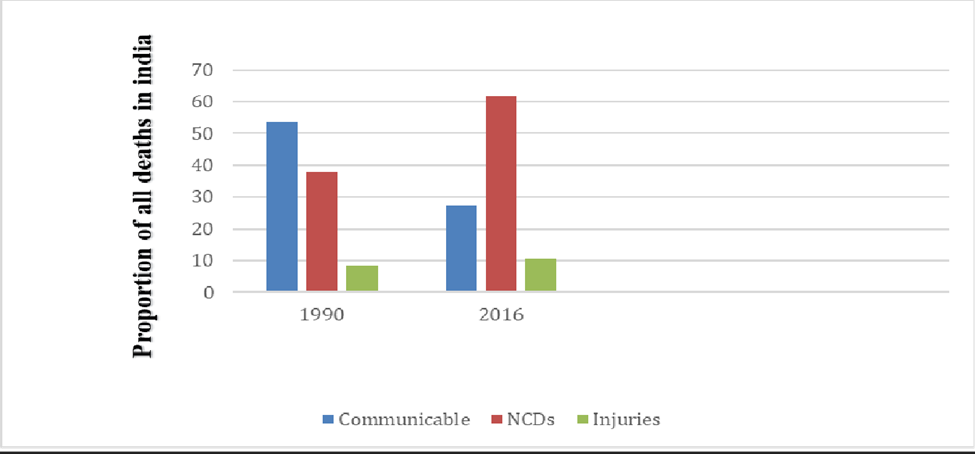
Fig 3: Causes of total deaths in India, 1990 and 2016 (Communicable vs noncommunicable vs injuries)
The largest nationally representative epidemiological dataset for the India Diabetes study by the Indian Council of Medical Research overview directed in India on diabetes and prediabetes, the information from 15 states/UT of the country (Table 1) showed that the prevalence of diabetes went from 3.5 to 8.7% in rural to 5.8 to 15.5% in urban regions.
Table 1: Weighted prevalence of diabetes and prediabetes in 15 states/Union territory of India ? the ICMR INDIAB Study
|
States/ UT |
Prevalence of Diabetes (%) |
Prevalence of prediabetes (%) |
||||
|
|
Urban |
Rural |
Total |
Urban |
Rural |
Total |
|
Assam |
12.4 |
4.4 |
5.5 |
13.6 |
11.6 |
11.9 |
|
Arunachal Pradesh |
5.8 |
4.9 |
5.10 |
14.2 |
12.3 |
12.8 |
|
Andhra Pradesh |
12.6 |
6.3 |
8.4 |
11.1 |
9.6 |
10.1 |
|
Bihar |
10.5 |
3.5 |
4.3 |
15.5 |
9.3 |
10.0 |
|
Chandigarh |
14.2 |
8.3 |
13.6 |
14.5 |
14.7 |
14.6 |
|
Gujarat |
9.5 |
5.1 |
7.1 |
8.4 |
11.5 |
10.2 |
|
Jharkhand |
13.5 |
3.0 |
5.3 |
10.7 |
7.4 |
8.1 |
|
Karnataka |
11.1 |
5.6 |
7.7 |
14.1 |
10.2 |
11.7 |
|
Manipur |
7.1 |
4.4 |
5.1 |
7.2 |
7.5 |
7.5 |
|
Maharashtra |
10.9 |
6.5 |
8.4 |
15.2 |
11.1 |
12.8 |
|
Meghalaya |
8.9 |
3.5 |
4.5 |
7.4 |
10.6 |
10.0 |
|
Mizoram |
7.9 |
3.6 |
5.8 |
6.2 |
5.8 |
6.0 |
|
Punjab |
12.0 |
8.7 |
10.0 |
8.6 |
7.8 |
8.2 |
|
Tamil Nadu |
13.7 |
7.8 |
10.4 |
9.8 |
7.1 |
8.3 |
|
West Bengal |
15.5 |
7.2 |
9.4 |
16.2 |
14.2 |
14.7 |
ROUTES OF ADMINISTRATION:
Insulin can be administered through several routes, including:
Subcutaneous injection: This is the most common route for administration insulin. Insulin is injected into the fatty tissue just under the skin, usually in the abdomen, thighs, buttocks, or upper arms [36].
Insulin Pen: An insulin pen is a device that contain a pre-filled cartridge of insulin and a needle. It is used to inject insulin under the skin, and it can be more convenient and discreet than a traditional syringe [37].
Insulin Pump: An insulin pump is a small device that is worn outside the body, usually on a belt or in a pocket. It delivers insulin through a small catheter that is inserted under the skin [38].
Inhaled insulin: Inhaled insulin is a type of insulin that is delivered through the lungs using a specialized inhaler device. The inhaled insulin is in the form of a dry powder that is breathed in through the mouth and into the lungs. The insulin then enters the bloodstream through the lungs and works to lower blood sugar levels. Inhaled insulin can offer several benefits over traditional insulin injections, including faster onset of action, more convenient administration, and potentially improved quality of life. However, it may not be suitable for everyone and should only be used under the guidance of a healthcare professional [39].
Intramuscular injection: In rare cases, insulin may be injected into the muscle. This is usually only done in medical setting, and not recommended for routine use [40]
Novel drug delivery refers to the development of new methods and technologies for delivering drugs to the body in a more efficient and targeted manner. Traditional drug delivery methods, such as oral pills or injections, often have limitations in terms of how much of the drug reaches the intended target and how quickly it is absorbed and metabolized by the body [41]. Novel drug delivery methods have the potential to improve the efficacy and safety of many drugs, as well as reduce side effects and the need for frequent dosing. However, the development of these technologies often requires significant research and testing to ensure their safety and effectiveness [42].
Transdermal drug delivery is a method of administering medication through the skin, directly into the bloodstream [43]. This approach uses specialized patches, gels, or creams that contain medication, which is then absorbed into the bloodstream through the skin. Transdermal drug delivery has several advantages over other methods of drug delivery, including providing a constant and consistent level of medication over an extended period of time, reducing the need for frequent dosing [44]. It can also avoid first-pass metabolism in the liver, which can reduce the risk of side effects, and provide a more convenient and non-invasive alternative to injections or oral medications [45]. Transdermal drug delivery is used to deliver a wide range of medications, including pain relievers, diabetes, hormone therapy, nicotine replacement therapy, and motion sickness medication. However, not all medications can be delivered through the skin, and the effectiveness of transdermal drug delivery can vary depending on the medication and the patient [46].
Advantages of transdermal drug delivery system
Preventing first-pass metabolism of drugs. Transdermal medication delivers a steady infusion of a drug over a prolonged period [47]. The simplified medication regimen leads to improved patient compliance and reduced side effects, and inter and intra-patient variability [48]. No interference with gastric and intestinal fluids. For a longer period, keeps blood levels stable, constant, and under control. Comparable characteristics with intravenous infusion [49].
Disadvantages of transdermal drug delivery system:
The skin's barrier function varies from one spot to another on the same person, between individuals, and with increased age. Because of the natural restrictions on drug entrance imposed by the skin's impermeability, only potent medicines make good candidates for
transdermal patches. Rashes, localized irritation, erythema, or contact dermatitis could be brought on by the medication, the adhesive, or the excipients in the patch formulation. Only 5 mg or less of a dose can be given per day. Because some skin types may not respond well to adhesives, the patch may be challenging to wear. High drug levels in the blood or plasma cannot be achieved using transdermal drug delivery systems. Transdermal drug delivery cannot be used for ionic medications [50]
Table 3: Classification diagram of several transdermal insulin drug delivery system
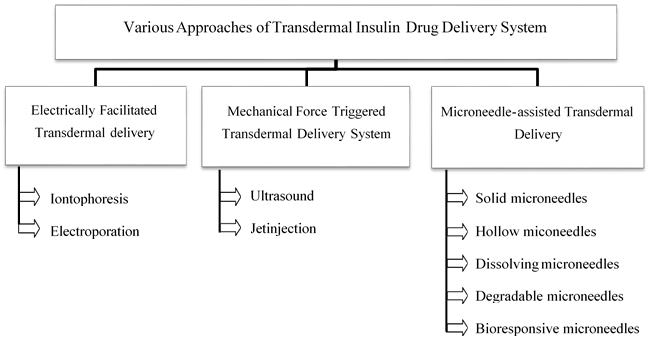
It's crucial to keep in mind that transdermal insulin delivery systems are still in the early stages of development and testing, even though they have the potential to be more practical and comfortable than conventional insulin injections. Before they are widely accessible for use, it can take a few years [51,52].
Transdermal insulin delivery using microneedles:
Solid Microneedle: Solid microneedles are often utilised for skin prep by pores appearing.The capillaries absorb the medication to cause a systemic reaction. It can also be used for a local impact. Solid microneedles distribute the medication to the skin's layers via passive diffusion. Tetramethylammonium hydroxide etching was used by Narayanan et al. to create solid silicon long and tapered microneedles. Successfully constructed microneedles had bases that were 110.5 m wide and 158 m tall on average.Later, he produced solid silicon microneedles coated with gold that had the following dimensions: height of 250 m, base width of 52.8 m, aspect ratio of 4.73, tip angle and diameter of 24.5° and 45 m. The outcomes showed enhanced bioavailability and mechanical strength. In their study of polylactic acid microneedles, Li et al. discovered that biodegradable polymer solid microneedles had the mechanical strength to penetrate the stratum corneum and can improve medication absorption. It was discovered that microneedles with an 800 m depth and 256 MNs per cm2 density improved medication penetration. Numerous researchers also study stainless steel microneedles.Following the use of stainless steel MN arrays, the enhanced distribution of captopril and metoprolol tartrate was investigated.
Hollow Microneedle: Hollow MNs are created to make it easier to inject medications via the inside of needles into the skin. Through hollow glass, Prausnitz and colleagues injected insulin into the diabetic rat's skin. MNs through microinfusion, causing a consistent decline of up to 70% in preinfusion BGLs over the course of 5 hours . In order to distribute insulin transdermally, they also devised and made hollow metal MN arrays. These MNs were powerful enough to puncture the whole skin without breaking, according to the mechanical investigation. Additionally, silicon hollow MNs have been investigated for the delivery of insulin. A "controlled release"-designed MN patch with an active dispensing feature was created by Nordquist, Roxhed, and colleagues. It can deliver insulin under control at low flow rates in the microliter range. The mechanically operated dispenser included a liquid reservoir, an expanding composite, and a heating layer. Insulin solution could be ejected through the hollow silicone MNs when current was fed through the heater, heating the composite, which then served as the liquid reservoir. This technology was connected to a 5-times greater plasma insulin concentration in a diabetic rat model compared to passive diffusion with a considerable drop in BGLs. In human research, the effectiveness of hollow MNs' delivery has also been examined. two individuals with type 1 diabetes were first studied for the transdermal administration of insulin via hollow metal MNs. To regulate the insulin infusion rate, an insulin pump was attached to the MNs and placed on the belly skin. The results showed that when MN was inserted into the skin at a depth of 1 mm, there was a quick absorption of insulin and a decrease in BGLs. Additional clinical studies have also been carried out to assess the efficacy and safety of hollow MNs for the administration of insulin to humans.
Dissolving Microneedle: One kind of microneedle that may administer medications, including insulin, via the skin is a dissolving microneedle. These tiny needles disintegrate when they come into touch with the skin and release the medication into the body since they are made of a water-soluble substance. Dissolving microneedles may offer a viable alternative to conventional injection techniques for the administration of insulin, such as insulin pens or syringes. This is due to the fact that many diabetics find injections to be uncomfortable, which can result in reduced treatment compliance and poorer health outcomes.
Because they only penetrate the epidermis, the top layer of skin, dissolving microneedles can be painless. Within minutes, the microneedles disintegrate, releasing the medication into the skin where it may be absorbed into the circulation.
Numerous studies have demonstrated that dissolving microneedles used to deliver insulin can successfully regulate blood glucose levels in both humans and animals. Although this technology is still in the experimental stage, it has the potential to completely change the way insulin is delivered while also enhancing the quality of life for those who have diabetes.
Degradable microneedle: Another kind of microneedle that can be used to administer insulin is degradable. After usage, the body may quickly degrade the biocompatible and biodegradable materials used to make these microneedles.
Degradable microneedles, like dissolving microneedles, can provide a less uncomfortable and more practical option to conventional insulin administration procedures. The microneedles are placed into the skin, where they gradually disintegrate and release the insulin over time.
One benefit of degradable microneedles is that they may be made to deliver insulin gradually, preventing sharp rises and falls in blood glucose levels. The importance of this can't be overstated for diabetics who battle to keep their blood sugar levels steady. Numerous studies have demonstrated that degradable microneedles used to deliver insulin can successfully regulate blood glucose levels in both humans and animals. Although this technology is still in the testing phase, it has the potential to enhance the delivery of insulin and make it simpler for those who have diabetes to manage their condition.
Bioresponsive microneedle: A particular kind of microneedle known as a "bioresponsive microneedle" can dispense medications, such as insulin, in reaction to changes in biological signals in the body. These microneedles are made to only release the medication under specific circumstances, including changes in pH, glucose levels, or temperature. Bioresponsive microneedles can be a possible replacement for conventional injection techniques for the administration of insulin since they can administer insulin in response to variations in blood glucose levels. Thus, the microneedles can only release insulin when it is actually required, potentially lowering the risk of hypoglycemia and enhancing overall blood glucose control. Microneedles that are bioresponsive can be made to react to a range of biological signals, including variations in pH, glucose levels, or temperature. One type of bioresponsive microneedle, for instance, employs a glucose-responsive polymer that may release insulin when blood sugar levels exceed a certain amount. Numerous studies have demonstrated that both animals and people can successfully control their blood glucose levels by administering insulin through bioresponsive microneedles. Although this technology is still in the testing phase, it has the potential to enhance the delivery of insulin and make it simpler for those who have diabetes to manage their condition.
Zhang et al., formulated Alginate and maltose microneedle patch is a promising approach for transdermal insulin delivery. This patch consists of biodegradable microneedles made of alginate and maltose, which are coated with insulin. The patch is applied to the skin, and the microneedles penetrate the outer layer of the skin, allowing for the delivery of insulin into the bloodstream. The use of alginate and maltose as the microneedle materials offers several advantages, such as biocompatibility, biodegradability, and ease of fabrication. This approach has shown promising results in animal studies, demonstrating the potential for the development of a safe and effective transdermal insulin delivery system (Zhang et al.,2018).
Seong et al., using the bullet-shaped double-layered microneedle (MN) arrays with water- swellable tips are a promising approach for transdermal drug delivery. The MN arrays are made of two layers, with the outer layer composed of a water-soluble polymer that swells in contact with skin interstitial fluid, and the inner layer made of a hydrophobic polymer that ensures the mechanical strength of the MNs. The bullet-shaped design of the MN tips enables a better penetration into the skin, reducing pain and skin irritation. The water-swellable tips enhance drug delivery by increasing the contact area between the MNs and the skin, promoting the rapid diffusion of the drug through the skin. This approach has shown promising results in animal studies, indicating the potential for the development of an efficient and minimally invasive transdermal drug delivery system (Seong et al.,2017).
Zhang et al., explores the use of polymeric nanoparticles based on carboxymethyl chitosan (CMCS) in combination with painless microneedle therapy systems for enhancing transdermal insulin delivery. The researchers synthesized CMCS nanoparticles loaded with insulin and evaluated their physicochemical properties, release behavior, and skin permeation in vitro. They also investigated the efficacy of the CMCS-insulin nanoparticles in combination with a microneedle therapy system using diabetic rats as a model. The results showed that the CMCS nanoparticles had good stability and controlled release properties, and when combined with the microneedle therapy system, they significantly enhanced insulin permeation through the skin and lowered blood glucose levels in the diabetic rats. This study suggests that CMCS nanoparticles and microneedle therapy systems could be a promising strategy for improving transdermal insulin delivery, providing a potential alternative to traditional injection methods (Zhang et al.,2020).
CONCLUSION:
Transdermal insulin delivery is a method of administering insulin through the skin, which can be an attractive alternative to traditional insulin injections for people with diabetes. The technology behind transdermal insulin delivery has been evolving for several decades, and while there have been some promising developments, it has not yet been widely adopted as a mainstream treatment. One of the main challenges with transdermal insulin delivery is getting the insulin to penetrate the skin barrier and reach the bloodstream in sufficient quantities to regulate blood glucose levels. Various approaches have been taken to address this issue, including the use of different types of insulin, enhancers, and delivery devices. Several transdermal insulin delivery devices have been developed, including patches and microneedle arrays. These devices have shown promise in clinical trials, with some studies reporting that they can effectively deliver insulin and improve glycemic control. However, there are still some limitations, such as the need for frequent device replacement and potential skin irritation or allergic reactions. In conclusion, transdermal insulin delivery is an innovative approach to diabetes treatment that has the potential to improve patient outcomes and quality of life. However, further research and development are needed to address the current limitations and challenges associated with this approach, and to make it a more widely accessible and viable option for people with diabetes
REFERENCES

Debarghya karforma*, Pintukimar De, Hirak Bhowmik, Transdermal Insulin Delivery Emphasizing on Microneedle Delivery System: A Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 176-190. https://doi.org/10.5281/zenodo.14967666
 10.5281/zenodo.14967666
10.5281/zenodo.14967666
