
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Samarth College of Pharmacy, Belhe, Pune. Maharashtra. India
Transdermal delivery is a non-invasive method of administering medication via the skin's surface. It can provide a local or systemic effect by delivering the medication at a predefined rate through the dermis. It may be utilized as a substitute for hypodermic injections and the oral delivery of medications. Since most diseases are accompanied by either severe or mild pain, analgesics are primarily utilized to treat these conditions. These days, analgesics are frequently utilized as a pain relief patch. A medicated adhesive patch used to treat mild to severe pain is called a transdermal analgesic or pain treatment patch. The patches are currently accessible for a variety of opioids and non-opioid analgesics. Antianginal medications and local anaesthetics. These medications include piroxicam, capsaicin, they come in matrix and reservoir patch varieties. This overview examines the frequency, side effects.
A non-invasive method of administering drugs through the dermis or skin surface is the transdermal drug delivery system, which is now frequently referred to as patches. It may be utilized as a substitute for giving medications orally and injecting hypodermics. With this medication delivery method, an analgesic can be applied topically at a set pace to produce either a local or systemic impact.
The idea of transdermal patches is not new. Scopolamine was first approved in the US in 1979 for use as a three-day patch for systemic distribution to treat motion sickness. Ten years later, increased awareness and use of transdermal medications were brought about by the popularity of nicotine patches [1].
There are currently at least 13 authorized compounds among the more than 35 medications utilized as transdermal patches. Transdermal patches' range of therapeutic applications is currently growing to include hormone replacement, analgesia, heart disease-related chest pain alleviation, quitting smoking, and neurological conditions.
Comparing transdermal patches to oral and hypodermic injections reveals several benefits. In the first stage of hepatic metabolism, it offers improved biocompatibility. Other benefits include painless application, extended application for one week, and increased flexibility in drug delivery through patch removal.
However, a few drawbacks have prevented this medication delivery technology from reaching its full potential. The quantity of medications may be restricted by localized skin irritation and sensitivity. Effective transdermal medications have molecular masses of only a few hundred Daltons, which also restricts the drug's dosage. Other drawbacks include delayed absorption, high prescription costs, and challenges in administering hydrophilic medications [2].
Along with additional advancements to increase safety and effectiveness, transdermal medications will continue to grow in popularity. The development of patches that distribute peptide and even protein molecules, such as insulin, growth hormone, and vaccinations, will be a significant advantage [3].
There are three types of transdermal patches: first generation, second generation and third generation.
They are the first patches and have been used extensively in medical facilities.
In the transdermal patch design, the medication is contained in a reservoir that is adhered to the skin and has an impermeable backing on one side [4]. However, not all medications with appropriate qualities can be supplied because of certain restrictions. Transdermal patches of the first generation are mostly restricted to the stratum corneum, the skin barrier. Therefore, the medications ought to be lipophilic, low molecular weight, and effective at low dosages.
Improvements in patches to improve delivery into the skin, lessen harm to the deeper tissues, and increase skin permeability. Changes like chemical enhancers, non-cavitation ultrasound, and iontophoresis have upset the equilibrium in the strategy to improve delivery while also safeguarding the deeper tissues.
Chemical enhancers: they introduce amphiphilic molecules to improve penetration by upsetting the stratum corneum's highly organized bilayer. However, this may cause skin irritation.
Iontophoresis: Iontophoresis is the process of administering medication using a low voltage current into the stratum corneum. They can be applied to small molecules that carry a charge as well as certain macromolecules up to a few daltons because they don't interfere with the skin barrier. A microprocessor can be used to regulate the rate of medicine delivery.
Non-cavitation ultrasound: physical therapists have shown that applying non-cavitation ultrasound to massage anti-inflammatory drugs into the skin can improve their effectiveness as a skin permeation enhancer [5]. Ultrasound has only had an impact on tiny lipophilic compounds. Its related tissue heating, which has the potential to harm deeper tissue, has limited its use.
It entails further developments to enhance medicine penetration through the skin and safeguard deeper tissues. Human clinical trials have tested the delivery of therapeutic proteins, macromolecules, and vaccinations using microneedles, thermal ablation, and microdermabrasion.
Because the transdermal route is safe and convenient, it is an intriguing choice for delivery. The following are advantages of administering medication through the skin to produce systemic effects:
Numerous parameters, including skin permeability, application location and duration, and skin metabolic activity (i.e., first pass metabolism), influence drug transportation over the skin. Actually, each medication has distinct qualities that may influence transdermal administration. The medication must be non-ionic and somewhat lipophilic to penetrate the skin barrier and achieve sufficient skin absorption and penetration. It is difficult for molecules bigger than 500 Daltons to pass through the stratum corneum, and the drug's therapeutic dosage should preferably be less than 10 mg daily.
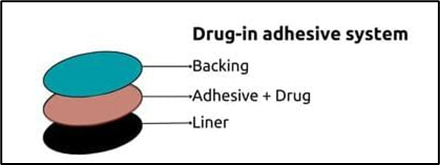
Usually made up of multiple layers, transdermal patches are intended to transfer the drug through the skin and into the bloodstream. The fundamental element of a medicated patch is depicted in Figure 1. Depending on the medication being administered and the intended rate of drug release, the patch's precise composition and structure may change
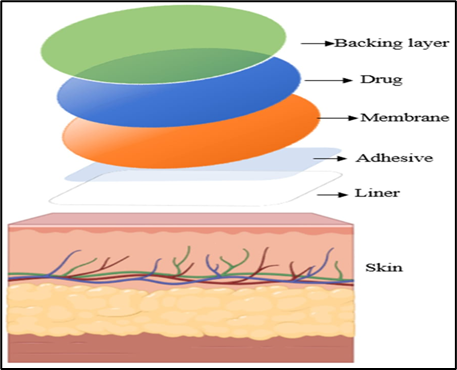
Figure1. Basic component of a transdermal medical patch.
The backing layer, which is the patch's outermost layer, shields the other layers from the elements. Typically, this layer is composed of a waterproof, flexible substance like polyethylene or polypropylene.
Drugs that are administered through the skin are found in the drug layer. It is designed to release the medications consistently throughout time. The rate at which the medications are released from the patch is regulated by the rate-controlling membrane. Drugs can go through membranes at a regulated pace since they are often composed of semi-permeable materials. The patch and glue are shielded by linen. Before applying the patch to the skin's surface, it must be taken off.
(a)
(b)
(c)
(d)
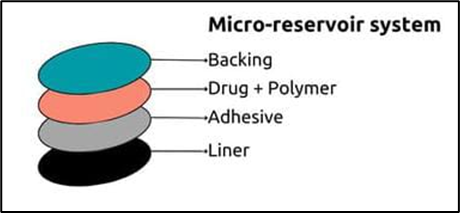
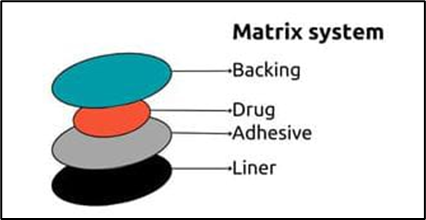
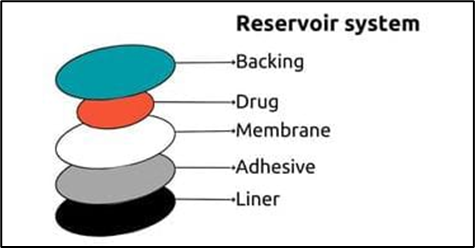
Figure 2: Illustrates the four primary categories of transdermal medical patches: reservoir, matrix, drug-in adhesive, and micro-reservoir systems. The majority of patches that are sold commercially fall into one of two categories: matrix or reservoir systems. [6]
[a] The Micro-Reservoir System
This system combines matrix dispersion with reservoir technology. In order to construct thousands of non-leaching microscopic drug reservoirs, the drug is synthesized by first suspending drug solids in an aqueous solution of a water-soluble liquid polymer, and then evenly spreading the solution in a lipophilic polymer.
[b] The Matrix System
In hydrophilic or lipophilic polymer matrices, drugs are evenly distributed. The final drug-containing polymer is adhered to drug-containing discs with regulated surface area and thickness.
[c] The reservoir system
The medicine is released through the microporous rate-controlling membrane of this device, which holds the drug reservoir between the backing layer and the membrane. The medication may be dissolved in a solid polymer matrix inside the reservoir chamber, or it may be in solution, suspension, gel, or another form.
[d] Drug-in-Adhesive System
This is the simplest form of membrane permeation control system. The adhesive layer in this system contains drugs and serves to glue the different layers together. The drug mixture is sandwiched between the liner and backing.
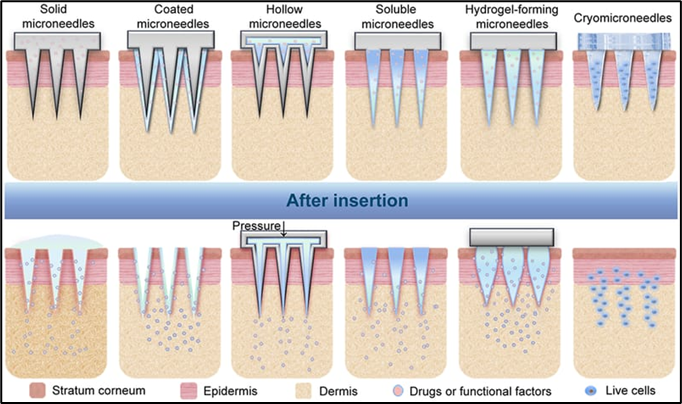
Table lists the various kinds of microneedles, each having special traits and attributes. Solid, hollow, dissolving, and coated microneedles are the four main varieties of microneedle-based patches that have been created thus far. The particular application and user needs determine the type of microneedle to utilize.
Table 1: Microneedle types with their unique features. [7-14]
|
Type |
Material |
Structure |
Use |
Dose |
Delivery Rate |
|
Solid |
Silicon, Metal, Polymer |
Simple |
Can be reuse |
Small dose |
Fast |
|
Hollow |
Silicon |
Simple |
Can be reuse |
Large dose |
Fast |
|
Coated |
Polymer, Sugar, Lipids |
Complex |
Single |
More precise dosing |
Fast |
|
Dissolving |
Polymer |
Complex |
Single |
More precise dosing |
Slow |
Transdermal patches are now are used in pain management for both acute and chronic pain. They are available in various forms which include non-steroidal anti-inflammatory drug patches (NSAID), opioid patches, local anesthetic patches, capsaicin, and nitroglycerine. They are commonly used in pediatric practice.
Popular medications called NSAIDs are used to treat musculoskeletal disorders, both acute and chronic [15]. They benefit from local action without experiencing negative central consequences or cognitive impairments. Ketoprofen, diclofenac, flurbiprofen, and piroxicam patches are among the various NSAID patches that are sold commercially [16].
Topical NSAIDs are intended to promote adherence and reduce systemic side effects. The preparations can offer good levels of pain relief without the systemic side effects associated with oral NSAIDs, according to a comprehensive evaluation of topical NSAIDs for acute musculoskeletal problems (such as strains and overuse-type injuries) that examined 3455 participants [17].
The most often used NSAID patch is 1% diclofenacepolamine, which is approved to treat acute pain from ankle sprains and epicondylitis. It is being used to aid in topical and systemic effects [18], according to a recent review. After three hours, patients with ankle sprains showed a decrease in pain levels. It is believed that the patch must provide analgesia through a local action because diclofenac first enters the plasma at a mean of 4.5 hours after topical application. The plasma diclofenac half-life is around 9–12 hours after patch removal because of a local reservoir effect, as opposed to 1-2 hours after oral ingestion.
Systemic adverse effects are extremely uncommon because systemic transfer after patch removal is only around 2% when compared to oral versions of diclofenac.
Another well-known NSAID that comes in patch and gel form is ketoprofen. In addition to inhibiting COX, it also counteracts the activity of bradykinin and stabilizes the lysosomal membrane. Compared to placebo, patients with rheumatic illnesses or trauma reported improved pain alleviation and functional gain [19].
An NSAID with strong analgesic and antipyretic properties is piroxicam. It is used to treat soft-tissue problems, acute gout, post-operative pain, and musculoskeletal and joint conditions like rheumatoid arthritis, osteoarthritis, and ankylosing spondylitis. Its solubility and permeation-enhancing qualities are high [20]
For moderate to severe pain, especially that which originates in the viscera, opioid analgesics are administered. They are advised for both non-cancerous illnesses, unless a doctor prescribes them. The opioid patch is a medication reservoir with a membrane separating it from the skin. The medication is released gradually. Common opioid patches with low molecular weight and high lipid solubility that facilitate easier dermal penetration are buprenorphine and fentanyl patches.
Fentanyl is a highly effective short-acting narcotic analgesic that is frequently used as a transdermal patch to treat chronic pain and as a surgical anesthetic. They are also employed in the treatment of cancerous discomfort. It can permeate the skin and disperse throughout the body due to its low molecular weight and highly lipophilic characteristics. Over the course of a 72-hour application, each patch is made to maintain a steady plasma fentanyl concentration, with the highest concentrations occurring between 12 and 24 hours. The rate of drug delivery is unaffected by blood flow or the anatomical place of application. Up to one-third more fentanyl can be delivered when exposed to a heat source or when body temperature rises. Under the brand names Duragesic and Durogesic, fentanyl patches come in commercial quantities of 12 µg/h, 25 µg/h, 50 µg/h, 75 µg/h, and 100 µg/h.Patients with osteoarthritis or rheumatoid arthritis who have chronic pain benefit from these patches in terms of pain management and quality of life [21]. They are helpful in situations where severe renal impairment prevents the oral route of morphine from being taken, or when swallowing difficulties or vomiting prevent the oral route from being utilized [22]. According to some research, fentanyl patches are thought to be more successful in treating cancer than oral morphine.Due to the possibility of severe side effects, fentanyl patches should not be administered to opioid-naïve individuals with non-cancer pain. The onset and duration of fentanyl patches are delayedmof action, making it potentially challenging to manage side effects going forward. The most dangerous opioid side effect linked to fentanyl is respiratory depression [23]. Additional adverse effects include skin irritation from the patch adhesive, nausea, and vomiting. Compared to oral morphine, fentanyl produces less constipation [24].
Thebaine is a low molecular weight, lipophilic substance that is used to make buprenorphine, a potent opioid. Its extended duration of action, antihyperalgesic properties, and free renal involvement make it particularly interesting. Both chronic and non-cancer patients found them to be more effective. It offers analgesia for osteoarthritis, low back pain, and other persistent pain syndromes with good efficacy and tolerability in managing chronic pain [25]. Clinical studies show that using buprenorphine for cancer pain reduces the need for rescue medication, improves sleep quality, and reduces pain [26]. Usually, a tiny dosage is introduced, and after three days, it is gradually increased. Three dosage levels are offered: 32, 52.5, and 70 µg/hour for a duration of 72 hours. The patch is placed on the chest, subclavicular area, or upper back. There are two versions of the patch: the 7-day Butrans® patch and the 96-hour Transtec® patch. Both employ a matrix design.
Research revealed improved patient compliance for six to twelve months, however subsequent adverse effects such nausea, vomiting, and constipation are noted when using the patch. It causes respiratory depression as a side effect, particularly when taken with CNS depressants [27].
Clinical trials have recently revealed improved features, such as respiratory depression and free renal impairment, in comparison to other opioids including fentanyl, hydromorphone, methadone, and fentanyl.
To combat the pain and discomfort experienced during venipuncture and intravenous catheter placement, topical anesthetics have been created. It is simple to use and has fewer adverse effects. It must have a direct local activity with little systemic impact in order to be useful in practice. over temporary microchannels, transdermal technologies facilitate the passage of many molecule sizes over the epidermal barrier, contributing to increased anesthesia in less than 20 minutes. It is more tolerant of skin-related adverse effects [28].
Most commonly lidocaine patch/versatis patch is used to help in postherpetic neuralgia. Lidocaine is available in 5% patches and is approved for postherpetic neuralgia treatment and other focal neuropathic syndromes, in which other treatments such as, tricyclic antidepressants, and opioids fail. They help in providing beneficial effects on pain, allodynia, quality of life and sleep, with minimal adverse effects. Versatis has dual mode of action, lignocaine diffusion, and the mechanical action of the hydrogel which protects the hypersensitive area. Small randomized controlled trials have confirmed that versatis produced superior pain relief than placebo in short-term studies [29].
Because of the extremely low systemic concentration of lidocaine, systemic adverse events after proper application of the plaster are uncommon. Skin lesions, lightheadedness, nausea, and hypersensitivity are among the adverse consequences [30].
They have been utilized in medicine and are derived from fiery chili peppers belonging to the genus capsaicin. Initially, it was applied on burnt or itchy extremities. Later, it became commercially available to treat a variety of conditions, including migraines, osteoarthritis, psoriasis, and neuropathic and nociceptive musculoskeletal pain [31]. It has 179 g of capsaicin and comes in an 8% dermal patch form. It readily penetrates the dermal and epidermal layers and is highly lipophilic. Another name for this patch is NGX 4010. Research indicates that the patch is useful for up to 12 weeks following application, particularly in cases of postherpetic neuralgia [32]. Burning, stinging, erythema, and edema are among the main adverse effects; these may also be associated with gradual neuronal defunctionalisation. There have also been reports of transient hypertension accompanied by localized pain. It is not recommended to apply capsaicin to open wounds [33].
An organic nitrate with strong analgesic and anti-inflammatory properties is nitroglycerine. Because it acts on multiple cellular systems as well as the central nervous system, it has historically been used to treat coronary heart disease. On the other hand, there was little improvement in coronary artery dilatation. It is marketed under the names Transderm-Nitro® and Nitro-Dur. Throughout the day, the plasma levels remain stable due to the gradual absorption. The effect lasts for up to six hours after starting at about thirty minutes. Additionally, nitroglycerine was found to be useful in the treatment of varicose vein sclerosis and rotator cuff abnormalities. When compared to a placebo, they lessen acute discomfort.
Headache, palpitations, allergic reactions, contact dermatitis, and flushing are some of the side effects. Peripheral ischemia and sudden myocardial infarction can also be caused by abruptly stopping nitroglycerin [34].
Conventional transdermal patches are only used for medication release and storage.
Traditional patching has numerous difficulties and disadvantages, such as minimal release or restricted dosage, even though this approach has certain benefits. The field of transdermal medication delivery has seen a number of advancements to date. These include the creation of innovative patches that have improved drug penetration and release, increased loading, and precise drug sensing and release capabilities. In general, research and development in the field of transdermal drug delivery is ongoing, with a number of fascinating new advancements anticipated, as detailed below.
Sensors and other technology built into smart patches allow them to track patient status and modify medication distribution as necessary. A team of researchers created a smart patch sensor device based on microneedles in 2014 to provide diabetics with continuous, painless intradermal glucose monitoring. This patch immobilizes the glucose-specific c-enzyme glucose oxidase (GOx) and acts as an electrical mediator for glucose detection using a conducting polymer like poly (3,4-ethylenedioxythiophene) (PEDOT). A smart insulin release patch made of 121 microneedles with nanoparticles was the product of more research and development. The patch enters the interstitial fluid between subcutaneous skin cells without causing any pain. Insulin and the glucose-sensing enzyme glucose oxidase, which changes glucose into gluconate, are found in the nanoparticles in each needle. Hypoxia-responsive polymers envelop these molecules. The hypoxia-responsive polymer senses the oxygen-depleted environment created by increased glucose oxidase activity in response to elevated glucose, as illustrated in Figure 4, which causes the nanoparticles to degrade and release insulin.[35]
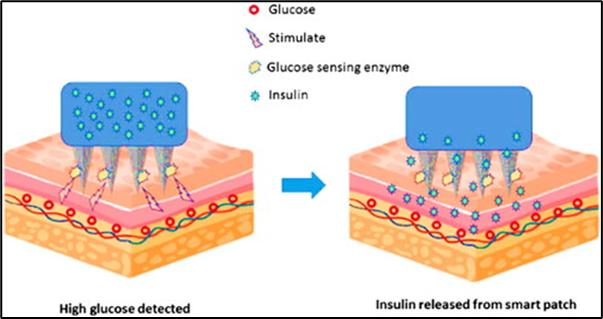
Figure 4: shows how the microneedle-based patch enters the epidermal layer painlessly. Insulin and glucose oxidase, an enzyme that senses glucose and turns it into gluconate, are both present in the smart patch.
The regenerative process of wound healing is intricate and dynamic, with physical and chemical characteristics that are always shifting. Particularly for individuals who are immobile, its care and monitoring provide significant advantages. Iversen et al. described a low-cost, flexible, completely printed smart patch that may be applied to the skin to track variations in fluid volume and wound pH. It is very simple to include these bendable sensors into wound dressings. The sensor measures pH and humidity using a variety of electrodes printed on a polydimethylsiloxane (PDMS) substrate. The sensitivity of the produced sensor patch to the pH of the wound is 7.1 ohm/pH. Results from hydration sensors shown that the change in resistivity can be used to measure the water content of the semi-porous surface.[36]
In addition to wound healing, researchers have created a smart patch to track and manage diabetic foot ulcers (DFU). Conductive hydrogel patches with an ultra-high transparency polymer network are used to create this system. Crucially, extremely transparent conductive hydrogel patches can be utilized to enhance vascularity, encourage collagen deposition, enhance cell-to-cell communication, minimize wound infection, promote hemostasis, and visually monitor the state of wound healing. Angiogenesis is efficiently encouraged, which aids in DFU recovery. Furthermore, the adaptable smart patch can promptly identify motions of human bodies of different sizes and accomplish indirect blood glucose monitoring by detecting glucose levels in wounds.[37]
Additionally, natural substances like curcumin are delivered via smart patches. Paraffin wax and polypropylene glycol, a phase-changing material (PCM), make up the substance. Graphene-based heating elements made by laser-scribing polyimide sheets were coupled with PCM. This setup provides a novel method for smart patches that enable repeated dosage and whose release may be electronically regulated. Permeation only happens when the PCM changes from a solid to a liquid, and emission is created and stopped by carefully heating the PCM as opposed to depending on passive diffusion. The delivery yields of curcumin were determined to be satisfactory and good.Additionally, natural substances like curcumin are delivered via smart patches. Paraffin wax and polypropylene glycol, a phase-changing material (PCM), make up the substance. Graphene-based heating elements made by laser-scribing polyimide sheets were coupled with PCM. This setup provides a novel method for smart patches that enable repeated dosage and whose release may be electronically regulated. Permeation only happens when the PCM changes from a solid to a liquid, and emission is created and stopped by carefully heating the PCM as opposed to depending on passive diffusion. The delivery yields of curcumin were determined to be satisfactory and good.[38]
These patches don't need to be taken off and thrown away because they are made to dissolve on the skin. These patches are often composed of biodegradable materials that the body absorbs after use. In a 2019 proof-of-concept study, scientists successfully used a dissolving patch to deliver the antibiotic gentamicin to a mouse model of bacterial infection [39] (Figure 5). The findings demonstrated that Klebsiella pneumoniae infection could be managed by applying a gentamicin-dissolving microarray patch on mouse ears. Furthermore, lysing patch-treated mice exhibited a lower bacterial burden in their lungs and nose-associated lymphoid tissue as compared to the untreated control. Medicina 2023, 59, x FOR PEER REVIEW Applying a dissolving microarray patch to mouse ears could prevent an infection with Klebsiella pneumoniae
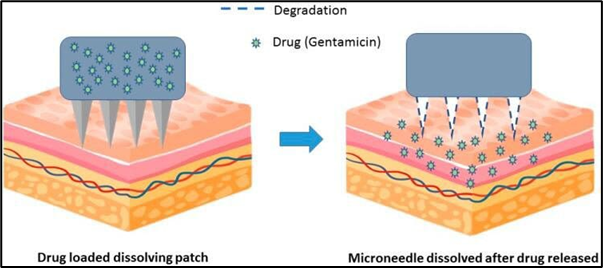
Figure 5: Biodegradable materials are used to make the microneedles in these patches. The microneedle dissolves on the skin once the gentamicin has been released from the patch.
Dissolving microneedles (MNs) are particularly effective at delivering medications and vaccines that are not very permeable. To effectively distribute insulin transdermally and localize it to the needle, a two-step injection and centrifugation procedure was employed. Insulin from Minnesota patches had a relative pharmacological availability of 95.6% and a relative bioavailability (RBA) of 85.7%. This study shows that, in comparison to traditional subcutaneous delivery, the use of dissolving patches for insulin delivery results in a reasonable relative bioavailability (RBA) [40]
However, for preventative cancer immunotherapy, researchers have created a biodegradable microneedle patch that administers hyaluronic acid (HA) antigen-peptide conjugates [41]. To effectively transfer antigens to the skin's immune system, HA loaded biodegradable HA microneedle (MN) patches are coupled with a cytotoxic T-cell epitope peptide (SI-INFEKL). Interestingly, tumo was considerably elevated by a single transdermal immunization using an MN patch carrying the HA-SIINFEKL conjugate.
A hypotensive biodegradable patch was created by a different research team to distribute sodium nitroprusside (SNP) and sodium thiosulfate (ST) transdermally.[42]
Using centrifugal casting, soluble microneedles containing SNPs and STs were created.
Using this technique, SNPs were released into the systemic circulation right away after being securely packaged onto microneedles. Microneedle therapy for antihypertensive (aH-MN) was successful. quick and effective lowering of blood pressure. It satisfied the clinical standards for controlling blood pressure in cases of hypertension.
Concurrent ST medication successfully reduced adverse effects (such as organ damage)brought on by ongoing SNP consumption. An effective and patient-friendly biodegradable patch for hypertension treatment was introduced in this study. The cosmetics industry also makes extensive use of transdermal patches. But when carelessly disposed of in public spaces, the non-biodegradable polymers used in cosmetic patches might harm the environment, which is a matter for concern. Because biodegradable polylactic acid (PLA) is non-toxic, it was suggested in one study. According to the findings, the PLA/phycocyanin-alginate composite with the optimum film flexibility and release characteristics was created with a phycocyanin/alginate ratio of 40/60 at 20 °C for 20 hours [43]. Although the results are encouraging overall, more in vivo or clinical research is necessary for further advancement.
To make transdermal patches that are specific to each patient's needs, researchers are utilizing 3D printing technology [44]. The application of a 3D-printed patch for wound healing is an excellent illustration. Gelatin methacrylate (GelMA) was examined as a potential solution with adjustable physical characteristics in a study by Jang et al.Because hydrogel inks shear thin, GelMA hydrogel with a vascular endothelial growth factor (VEGF)-mimicking peptide was effectively produced using a 3D bio-printer. The hydrogel patch's three-dimensional structure exhibited significant porosity and water-absorption capabilities.The 3D Gel-MA-VEGF hydrogel patch has the potential to be employed as a wound dressing because the VEGF peptide, which is gradually released from hydrogel patches, can encourage cell survival, proliferation, and tubular structure creation [45].
Conversely, transdermal patches were designed and manufactured using a three-dimensional (3D) printing method known as continuous liquid interface production (CLIP). In the end, the better surface coating of the model vaccine components (ovalbumin and CpG) was the consequence of the multifaceted microneedle design's increased surface area in comparison to the smooth square pyramid design. The study evaluated the in vivo charge retention and bioavailability in mice as a function of delivery route using fluorescent tags and live animal imaging. Transdermal administration of soluble components, as opposed to subcutaneous bolus injection, increased both the activation of immune cells in draining lymph nodes and the retention of skin charge. Additionally, dosage sparing was achieved because the administered vaccination produced a robust humoral immune response with increased total IgG (immunoglobulin G) and a more balanced IgG1/IgG2a repertoire. Additionally, it produced a T-cell response that was typified by Th1 (T helper type 1) cytokine-secreting CD8+ and CD4+ T-cells that were functionally cytotoxic. To put it briefly, CLIP 3D-printed microneedles coated with vaccine ingredients offer a practical platform for self-administered, non-invasive immunization [46].
A different team of researchers used a proprietary class I resin and stereolithography (SLA) technology to create and print the patch. They demonstrated the transdermal delivery of high molecular weight antibiotics, including rifampicin (M(w) 822.94 g/mol), using these patches. This medication has significant hepatotoxicity, decreased bioavailability, and stomach chemical instability. To improve the patch array's mechanical strength and integrity, sub-apical holes were incorporated into one-fourth of the needle tip. To assess print quality and uniformity throughout the array, optical and electron microscopy were used to characterize the tips. Additionally, the system was mechanically characterized for penetration and failure analysis. The ex vivo penetration and subsequent transport of rifampicin through pig skin were methodically assessed by the authors. Furthermore, rifampicin delivery through the 3D-printed patch showed effective penetration and favorable bioavailability in an in vivo trial [47] Because it can directly handle pharmaceuticals and excipients in a single step, another method called powder extrusion (DPE) has become the most practical strategy [48].
The study was set to determine whether different grades of ethylene-vinyl acetate (EVA) copolymers could be used as new starting materials for the fabrication of transdermal patches. By choosing two model drugs with different thermal behavior (i.e., ibuprofen and diclofenac sodium), they also wanted to consider the versatility of this EVA excipient in manufacturing patches for custom transdermal therapy. EVA was combined with 30% (w/w) of each model drug. Fourier transform infrared (FT-IR) spectra confirmed that the starting material was effectively incorporated into the final formulation, and thermal analysis revealed that the extrusion process changed the crystalline morphology of the raw polymer, leading to increased crystallization at smaller thicknesses. According to this study, direct powder extrusion technology and EVA might be useful instruments for creating transdermal patches. Drugs with varying melting points can be printed while retaining thermal stability by selecting an EVA type with the right VA concentration. Additionally, it is possible to attain the required drug release and permeability profiles. Indeed, from the perspective of individualized medicine, this is a significant benefit.
The use of 3D printed customized patches that fit the skin's surface for the distribution of acetyl-hexapeptide 3 (AHP-3) was documented by Lim et al. However, creating drug-loaded delivery systems is not a good use for commercially available photocurable resins for 3D printing. In order to increase the final polymer's mechanical strength, polymerization rate, and swelling rate, two liquid monomers—polyethylene glycol diacrylate (PEGDA) and vinylpyrrolidone (VP)—were utilized in varying amounts in this investigation. AHP-3 stayed stable during the production process and had no impact on the finished polymer's physical characteristics, according to optimal drug loading on the resin. . Using a 3D scanned facial model, a personalized patch was designed in CAD (computer-aided design) software and fabricated in optimized resin using a digital light processing (DLP) 3D printer. In vitro characterization of the prepared transdermal patches showed their ability to penetrate human cadaver skin, and they remained intact after compression. The final polymer was also minimally cytotoxic to human dermal fibroblasts. This is the first study demonstrating personalized patches made using photopolymers and may be a novel approach to improve the transdermal delivery of drugs for effective wrinkle management [49].
High drug loading and regulated drug release are necessary for long-acting transdermal medication administration. A new hydroxyphenyl (HP)-modified pressure-sensitive adhesive (PSA) was created to enhance drug-polymer miscibility and accomplish controlled drug release. [50] The findings demonstrate that, in contrast to ionic and neutral H-bonds, the dual-ionic H-bonds between R(3)N and R(2)NH type medications and HP-PSA are reversible and reasonably strong. This made it possible for patches to regulate the medication release rate from 1/5 to 1/2 and greatly increase the drug loading from 1.5 to 7 times without affecting the overall release profile. Pharmacokinetic findings demonstrated the potential for long-acting drug delivery as the HP-PSA-based high-load patch boosted area under the concentration-time curve (AUC), prevented abrupt release, and increased average dwell time by more than six times while achieving sustained drug concentrations in plasma. Its mechanical and safety qualities are also satisfied. According to mechanistic research, ionic drug repulsion in HP-PSA enhances drug loading, and comparatively strong contacts can also regulate drug release. Since its reversibility was defined by incomplete hydrogen bond transfer, the percentage medication release was equivalent to that of non-functional PSA. In summary, the development of long-acting transdermal drug delivery systems will be aided by HP-PSA's high drug loading efficiency, regulated drug release capabilities, and special interactions. Additionally, the creation of double-ionic H-bonds serves as another motivation for different drug delivery methods in non-polar settings.
Strong intermolecular hydrogen and ionic bonds allow pharmaceutical polymers to prevent drug recrystallization, albeit at the expense of transdermal patch drug release rates. A team of researchers devised a novel ionic liquid (drug IL) approach to boost drug loading in order to get around this problem [51] A carboxyl- As a model polymer, pressure-sensitive adhesive (PSA) was used. The PSA medication load increased fivefold, according to the results. This resulted from the drug's carbonyl groups and PSA forming strong ionic and normal hydrogen bonds, which worked in concert. This study offered a potent tool for the creation of high-drug load, high-release patches and revealed a completely novel mode of action. The same team of researchers developed a high-capacity, high-release transdermal patch using COOH polyacrylate polymer (PA-1) in a different trial to administer ibuprofen and other non-steroidal anti-inflammatory medicines (NSAIDs). PA-1's epidermal absorption and drug load were increased by 2.5 and 2.4 times, respectively. . Repulsive interactions weaken the hydrogen bond that forms between the drug (COOH) and PA-1 (COOH), while dielectric spectroscopy, electron paramagnetic resonance (EPR) spectra, the four-point probe method, and molecular modeling with the appearance of COO-all confirmed PA-1's increased conductivity. In conclusion, these findings demonstrate that ion–ion repulsion, achieved through the reduction of hydrogen bonding, can be a practical approach to developing high-emission, large-capacity patches. [52]
10. POTENTIAL APPLICATION OF TRANSDERMAL PATCHES [53-56]
CONCLUSION
The pain and inconvenience of needles, as well as the limited bioavailability of many oral medications, can be effectively addressed by transdermal drug delivery. While third-generation physical enhancers may make it possible to distribute macromolecules and vaccines transdermally, the achievements of first-generation transdermal patches, second-generation chemical enhancers, and iontophoresis are increasing the transport capacities for small molecules. The creation of total dissolved solids units that distribute peptide and even protein compounds, such as insulin and growth hormone, will be another significant advancement.
An underappreciated technique for treating both acute and chronic pain may be the transdermal patch. We anticipate that this drug delivery method will become more widely used and more popular as it offers a greater variety of analgesics and better distribution.
REFERENCE





Prajakta Shingote, Ajay Bhagwat, Kautika Puyad, Aniket Kalpe, Swapnil Auti., Transdermal Patches for Controlled Release of Analgesics: A Novel Drug Delivery Approach, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1389-1407. https://doi.org/10.5281/zenodo.17571913
 10.5281/zenodo.17571913
10.5281/zenodo.17571913