1Research Scholar, Department of Pharmaceutics, VYWS, Institute of Pharmaceutical Education and Research, Borgaon (Meghe), Wardha, Maharashtra, India.
2Professor (HOD), Department of Pharmaceutics, VYWS, Institute of Pharmaceutical Education and Research, Borgaon (Meghe), Wardha, Maharashtra, India.
Colon cancer remains a significant health concern due to limited efficacy and high toxicity of current chemotherapeutic agents. The quest for novel anticancer therapies has led to exploration of natural compounds, including chrysin, which exhibits promising anticancer properties. Chrysin, a flavone found in various natural sources, has been extensively studied for its biological effects, particularly its pro-apoptotic activity and ability to inhibit tumor angiogenesis. In preclinical studies, chrysin has demonstrated efficacy against various cancer cell lines including cervical, breast, prostate, liver, ovarian, lung, leukemic, and colon cancer. However, challenges remain in translating these findings into effective treatments, necessitating further research into chrysin's mechanism of action and optimization of its formulation for enhanced bioavailability. This review summarizes the role of chrysin in colon cancer treatment, highlighting recent experimental data on different chrysin formulations and their efficacy in vitro and in vivo. The findings underscore the potential of chrysin as a therapeutic key for colon cancer and emphasize the need for advanced formulations to improve its solubility and absorption, thereby enhancing its therapeutic efficacy.
The latest assessment of the International Agency for Research on Cancer (IARC) on the analysis of cancer statistics worldwide by world region for the year 2022 showed presence of 9.3% colorectal cancer of all cancers globally. In 2022, colorectal cancer accounted for about 2.5 million new cases, of which 609,216 were male and 533,006 were female. It was the third most often diagnosed cancer.1 The rate of incidence of colon cancer can be seen constantly rising in highly developed countries due to their changed lifestyles specifically speaking in the South region of Central and Eastern Asia along with the Europe and America.2the study, which gave an idea of the prevalence of colorectal cancer in 204 nations and provinces on a national, regional, and worldwide scale between 1990 and 2019, showed the number of CRC cases worldwide increased from 842,098 to 2,166,168. With a 95% uncertainty interval, linked deaths climbed from 518,126 to 1,085,797 between 1990 and 2019. In 2019, CRC was accountable for 24,284,087 DALYs. From 1990 to 2019, there was a 157% increase in CRC incidence, an 110% increase in fatalities, and a 96% increase in disability-adjusted life years. The highest rates of CRC occurred in East Asia, Equatorial Guinea, and Southern Latin America; globally, men were more likely to report having CRC than women.3Depending on where the metastatic growth is located, surgery and chemotherapeutic administration are part of the traditional treatment for colon cancer. However, in this type of cancer, the risk of death for the patient stays higher because the current chemotherapeutic agents have high toxicity and severe negative effects.4One of the most crucial therapies for cancer patients is chemotherapy. Nonetheless, for the majority of solid tumours, the efficacy of the chemotherapeutic medications is still restricted.5
More than a thousand different medications have been shown to have notable anticancer effects. Yet there is still a need for scientific research to generate novel anticancer medications from a wide range of natural, biological, and synthetic components. Predictions suggest that leveraging natural goods could significantly decrease cancer-related deaths in the 21st century. These products have emerged as crucial sources of anti-cancer agents.6 Because of their pro-apoptotic properties, natural compounds are promising anti-cancer agents.7Many phytochemicals including polyphenols and flavonoids with potential applications in medicines are found in plants. Flavonoids are a family of compounds that are found in meals derived from fruits and veggies and consist of a broad variety of natural pigments. A broad class of polyphenolic compounds, found in many herbal products and food, make up chysin. These compounds have been linked for a long time to a number of significant pharmacological & biochemical actions in the prevention of cancer and maintenance of health.8Chrysin has been demonstrated in several studies to possess a variety of biological properties.9Furthermore, in different cancer cell lines, namely Cervical cancer Hela cells, leukaemia cells L1210 along with HL-60 and U937 have been shown to undergo apoptosis when exposed to chrysin. Additionally, this plant flavonoid has the ability to prevent tumor angiogenesis, a crucial stage in the spread of cancer cells.10In vitro, chrysin has been shown to have an impact on human colon cancer cells' viability.11 There are number of bioactives which have anticancer activity but very few of them are formulated as an effective dosage forms due to the need of thorough study on their mechanism of action. The present review is based on understanding mechanism of the bioactive chrysin and its impact on colon cancer.
COLON OR COLORECTAL CANCER
Colorectal cancer (CRC) typically initiates with the non-cancerous proliferation of mucosal epithelial cells. These growths termed polyps undergo gradual development over a span of 10 to 20 years before progressing to a cancerous state. This sequence of progression is often referred to as the adenoma-carcinoma sequence.12
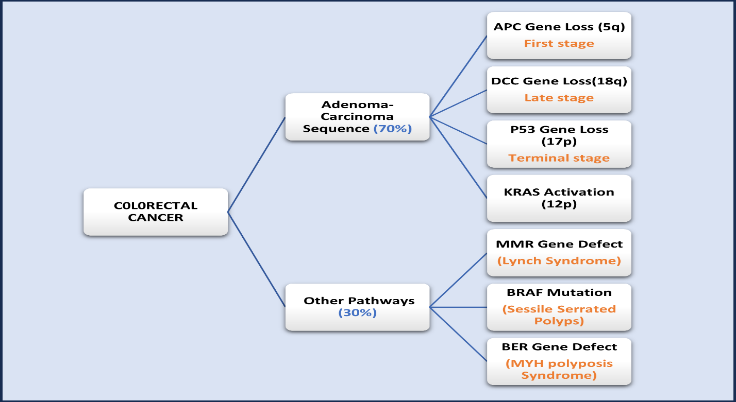
Fig. 1. Colo/ colorectal cancer development pathways through gene defects
In 35–45% of CRC cases, the KRAS oncogene is activated. It is linked to poor survival rates, increased aggressiveness of colorectal cancer, and lower reactivity to several chemotherapeutic drugs, especially those which are epidermal growth factor targeting agents.13 The process of fixing errors created during DNA replication involves MMR genes. Numerous DNA mutations seen in MMR-deficient cells have the potential to cause cancer and MSI. 12–15% of all cases of CRC in the USA are sporadic, involving MSI and somatic mutations in the MMR gene. They almost invariably occur in the right colon. they primarily affect fair toned-middle aged groups with no family history for cancer. a common feature of CRC is methylation of DNA with CpG island and its phenotype methylator. MLH1 methylation linked to CIMP results in isolated instances of MMR deficiency. 3-6% of total CRC cases in the United States are caused by mutations in hMSH2, hMLH1, hPMS1, and hPMS2 genes which are found in hereditary non-polyposis colorectal cancer.14 In CRC cases, the genetic alteration in the BRAF gene causes the emergence of both classic serrated adenoma (TSA) and sessile serrated adenoma (SSA). BRAF-mutated colorectal cancers (CRCs) are typically right-sided, develop in higher age group commonly in women.15 Sporadic microsatellite instability is caused by the CpG island methylator phenotype, which is closely linked to the BRAF mutation in colorectal cancer. CIMP-positive BRAF-mutated colorectal cancer patients shows predominance.16 Thus, tumors that are CIMP-positive are typically the result of serrated adenoma. CIMP-positive tumours have a microsatellite instability rate of about 50%. Ten to twelve percent of total CRCs are CIMP-positive and microsatellite unstable as well as CIMP positive in nature.17
TNM STAGING SYSTEM OF COLON CANCER BY AMERICAN JOINT COMMITTEE ON CANCER (AJCC)
According to latest updated version( 8th Edition published in 2017) under AJCC colon cancer initiates from stage 0 and develops with the progression to stage IVC. It also incorporates quantifiable changes or biologic and genetic markers that personalizes cancer staging.18,19
Table 1. Stages of colorectal cancer by prognostic groups and their criteria (AJCC)19,20,21,22,23,24,25
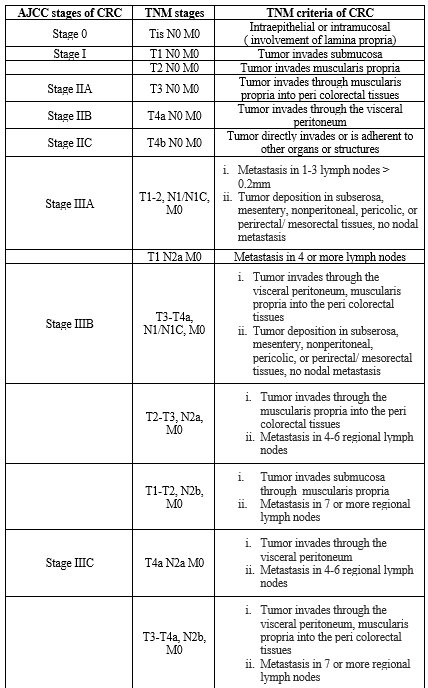
*TNM: Tumor/Nodes/Metastases; Stage 0- Stage IVC; Anatomic stages of colon/ colorectal cancer (CRC); Tis- T4b: prognostic groups representing stages of tumor (T); N0- N2b: prognostic groups representing stages of lymph nodes (N); M0- M1c: prognostic groups representing stages of metastasis (M).
RISK FACTORS RESPONSIBLE FOR COLON CANCER
All the risk factors of colon or colorectal cancer basically alter the pathophysiology of the colonic cells by different mechanisms.26 the most common risk factors are the family history, genetic alterations, obesity, gender, race and ethnicity , High risk genetic syndromes, consumption of alcohol as well as red processed or burned meat , smoking, physical activities and exercises, rapid industrialization and continuously changing life style and diseases like diabetes and inflammatory bowel disease.27,28 Some rare but high-risk factors are acromegaly, hereditary hemochromatosis, ureterosigmoidostomy, childhood cancer, and occupational exposures in firefighting.29 Again, there are multiple severe root causes for development of this type of cancer which may include dietary habits like low-fibre, high-fat diets, insulin resistance, and long-term immunosuppression post renal transplantation. Additionally, androgen deprivation therapy for extended period or family history of colorectal cancer or adenoma, and genetic syndromes such as Serrated Polyposis Syndrome (SPS), familial adenomatous polyposis (FAP), Muir-Torre syndrome, Peutz-Jeghers syndrome, Cowden syndrome, Lynch syndrome, Cronkhite-Canada syndrome, Juvenile Polyposis Syndrome, and non-inherited polyposis syndromes contribute to increased risk.30,31 As per the data published in 2020, their study was documented on 3058 CRC cases which showed that the different parts from colon to rectum pauses varied risk of occurrence of the cancer. It involved sigmoid colon (750 cases), ascending colon (633 cases), rectum (528 cases), cecum (474 cases), transverse colon (250 cases), descending colon (221 cases), rectosigmoid junction (202 cases). the favourable correlations between age and a family history of colorectal cancer with cancer risk were ascertained to be declined from the cecum to the rectum. On the other hand, the inverse relationship with respect to intake of whole grains, cereal fibre and processed red meat was found by endoscopic surveillance from the cecum to the rectum was seen. The correlation between colorectal cancer (CRC) and female sex exhibited a noteworthy non-linear pattern. The risks ratios for ascending and sigmoid colon cancer varied from 1.73 to 0.54. From the cecum to the transverse colon, there was a greater correlation between alcohol use and smoking prior to the age of thirty and proximal colon malignancies. The positive correlation between men's waist circumference and distal colon cancers was stronger for descending than for sigmoid colon cancers.32 Previous research indicates that while male sex and increasing age were found to be significantly associated with increased risk, aspirin use turned out to be strongly linked with lower risk of EOCRC in a case-control study of veterans; the same characteristics were found to alter the risk for CRC onset beyond age 50. One of the early clinical symptoms of EOCRC may be a weight loss.33
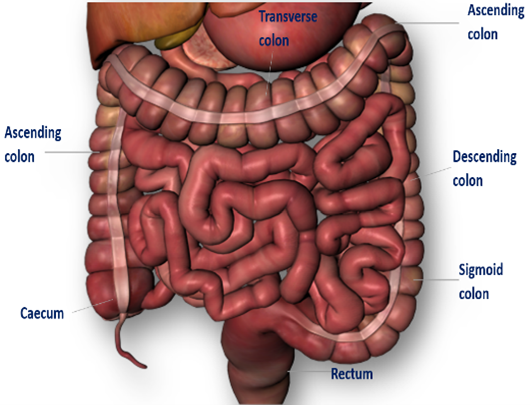
Fig. 2. Parts of colon
MEDITERRANEAN DIET (MD)
In case of the colon cancer age around 50 to 70 years is considered to be a common risk factor but the most significant one is the diet.29 the MD is a blend of several dietary behaviours of population regarding their religious, economic, cultural lifestyle and food customs that have dwelled in the Mediterranean region for thousands of years. Extensive research conducted over many decades has examined the MD as a potential to offer protection against numerous chronic illnesses and cancers, such as colorectal cancer.34
TREATMENT FOR COLON CANCER
Chemotherapy, radiation therapy, surgery, cryosurgery are the major treatment options available for colon cancer. The conventional treatments like monotherapy, combined immunotherapy and combined immunotherapy in combination with chemotherapy they all have their possible side effects as they deliver drug to the non-targeted sites which damages both cancerous as well as non-cancerous cells and produces drug resistance during treatments over a long period of time leading to the death of the patients. Since 1957, 5-Fluorouracil (5-FU) continues to be the primary therapeutic approach for colorectal cancer despite of its high toxicity with very low efficacy.35 To overcome these underlying side effects, the replacement of conventional drugs with herbal bioactives has become active research to discover the activity of herbs and their bioactives for their diagnostic and therapeutic values in cancer.36 As conventional chemotherapy for colon cancer has many limitations, the natural phytochemicals have demonstrated benefits over conventional chemotherapy in the treatment of colon cancer.37currently, vinca alkaloids, roscovitine, camptotecin, irinotecan, paclitaxel, docetaxel. podophyllotoxin and colchicine are some of the most commonly used plant-based compounds for their anticancer activities.38
CHRYSIN
A flavone found in honey, propolis, passion fruit and blue passion flower is a chrysin (5, 7-dihydroxyflavone). The two premium, high-quality sources of chrysin are considered to be the propolis and honey. A dried root of the Scutellariae baicalensis Georgi (Radix scutellariae)39, bitter melon (Momordica charantia)40 and an edible mushroom (Pleurotus ostreatus)41, wild Himalayan pear (Pyrus pashia)42 can be utilized for extraction of chrysin.
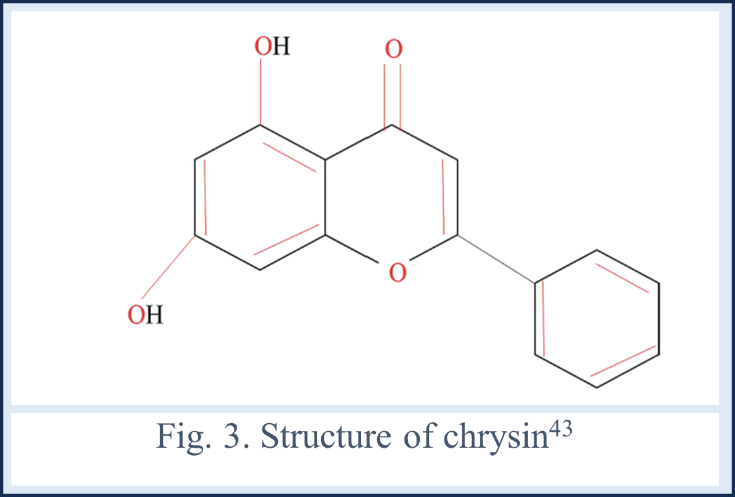
Structurally, the chrysin is classified under the subclass of flavonoids, possesses a distinctive molecular structure with benzene ring A and B along with one central oxygen holding heterocyclic ring. its configuration features a carbonyl group attached to 4rth carbon atom with double bonds, distinguishing it from the other flavonoids with the missing C3H7OH.
Fig. 4. Schematic of major sources and pharmacological activities of chrysin44
Notably, chrysin bears (-OH) group on 5th & 7th carbon, distinguishing it further within its class. Unlike many flavonoids, it does not display oxygenation in B ring, contributing to its unique chemical profile and potentially distinct biological activities.44
DOSE AND TOXICITY
Most people agree that moieties on the A and C rings, where the hydroxyl can have antitoxic effects, are linked to chrysin's pharmacological activity In theory, a moiety like pan-assay interference compounds might be formed by the carbonyl coupled with the double bond at 2nd and 3rd place which could possibly result in toxicities.45Chrysin, however, has been shown in preclinical models to be reasonably safe. A safe dose of chrysin for human is considered 0.5–3.0?g.46 Chrysin was given orally or intravenously, either as a pure molecule or in herbal extracts, at doses ranging from 0.23 to 100 mg/kg in preclinical PK investigations including mice and rats. as a result, herbal extract produced a Tmax of less than one-hour, pure chrysin showed a Tmax of two to six hours, perhaps because of the slower absorption of higher doses. Tmax was considerably reduced by formulations with enhanced water solubility.it is possibly the result of the higher pure chrysin doses than its maximum absorbable dose.47 the half-life of chysin varied from 3 to 11 hours, indicating enterohepatic recycling.48
KINETICS AND BIOAVAILABILITY
according to previous studies on human volunteer with 400 mg chrysin administration, chrysin sulphate was majorly produced in plasma and as compare to this its systemic exposure was 20 folds lower having 64?±?33?ng/mL·hr. of AUC. Chrysin shows elimination through feces and urine. the 90 % and more of it can be seen in form of aglycon in feces. which could be due to the low aqeous solubilty or enterohepatic recycling of chrysin. through urine in shows elimination as a chrysin-glucuronide as well as in its original form without any change in its structure chemically.49 The excreation of chrysin occurs via bile in the form of conjugates like glucuronide and sulfate. this conjugates further in the colon get hydrolyzed to chrysin again due to the action of intestinal microbiome which makes chrysin to have a poor oral bioavailability. while talking about the solubility of chrysin it belongs to BCS class II, poses high permeability but low aqueous solubility giving a poor intestinal absorbtion. Showing / making a need of advanced formulations like nanoparticles, etc.50
ROLE OF CHRYSIN IN COLON CANCER
The recent experimental data of chrysin, its derivatives and chrysin in different pharmaceutical forms from year 2019- 2024 was collected, understood and summarized in the present review.
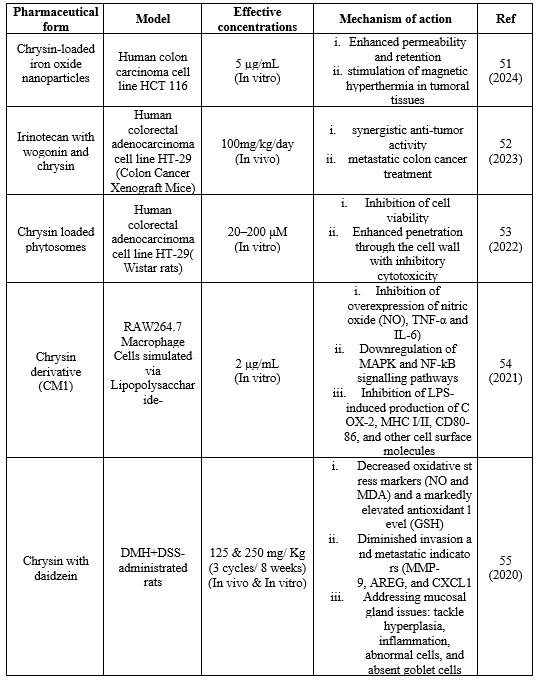
Table 2. Collective data of efficacy of different chrysin formulations on in vitro/ in vivo colorectal cancer models and their doses
Chrysin, a natural flavone, shows potential in treating colon cancer through varied formulations and combinations. Iron oxide nanoparticles loaded with chrysin improve tumor permeability and retention, and irinotecan and chrysin and wogonin together have synergistic anti-tumor actions. Phytosomes loaded with chrysin enhance cell penetration, while chrysin derivatives such as CM1 suppress signalling pathways and inflammatory indicators. As previous findings chrysin poses anticancer activity for number of cancers. But findings suggest that their derivatives also have similar mechanisms of action on colon cancer cells. In recent experimental study, among the novel set of seventeen chrysin derivatives that synthesized in the recent experimental study, compound 33A, a derivative of chrysin, had showed the greatest efficacy against HCT116 cell lines, with an IC50 value of 4.83 ?M.59 5,7- dimethoxychrysin, 5,7-dimethoxy-8-iodochrysin, 5,7-dimethyl-8-trifluoromethylchrysin, 5,7-diacetoxychrysin, 6,8-diiodo-5-hydroxy-7-acetoxychrysin, 6,8-ditrifluoromethyl-5-hydroxy-7-acetoxychrysin, 8-bromo-5-hydroxy-7-methoxychrysin, 5,7-dihydroxy-8-nitrochrysin, 8-iodo-5- hydroxy-7-methoxy-6-nitrochrysin are the derivatives of chrysin found to have anticancer activity against colon cancer cell lines. 8-bromo-5-hydroxy-7-methoxychrysin was the most potent anticancer chrysin derivative on human colon adenocarcinoma cell line HT29.60
CONCLUSION
This comprehensive review provides a structured overview of all possible studies of herbal bioactive chrysin focusing on the anticancer efficacy of b bioactive chrysin specifically on colon cancer cells from 2019 to 2024 with inclusion of studies with their respective models, effective concentrations and mechanisms of action. it indeed would provide a thorough understanding of chrysin's potential by enabling present scenario and clear evidence for effective treatment of colon/ colorectal cancer using a bioactive chrysin indicating a strong need of advancement in chrysin formulation which can increase its aqueous solubility and colonic absorption.
REFERENCES


Chetna K. Dhone, Shagufta A. Khan, Unlocking The Potential Of Chrysin: A Comprehensive Review On Its Role In Colon Cancer Treatment, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 5, 1479-1491. https://doi.org/10.5281/zenodo.11348372
 10.5281/zenodo.11348372
10.5281/zenodo.11348372
