Dr. Shivajirao Kadam College of Pharmacy, Kasbe Digraj, Sangli, India.
Cancer remains one of the leading causes of mortality worldwide, and despite advances in chemotherapy, radiotherapy, immunotherapy, and surgery, conventional approaches continue to suffer from limited specificity, systemic toxicity, and drug resistance. Nanotechnology has emerged as a transformative field in oncology, enabling novel approaches for drug delivery, diagnostics, and therapy. Among these, nanorobots—nanoscale devices capable of performing complex biomedical tasks—have attracted increasing attention due to their ability to combine precision targeting, controlled drug release, tumor microenvironment modulation, and real-time monitoring into a single platform. This review highlights the fundamentals of nanorobotics, including structural design, navigation strategies, and therapeutic mechanisms, before exploring their diverse applications in cancer treatment, such as targeted chemotherapy, gene therapy, immunomodulation, photothermal/photodynamic therapy, and combination approaches. Preclinical studies, including DNA origami-based nanorobots for vascular occlusion and magnetically guided or biohybrid systems for tumor targeting, have demonstrated feasibility in animal models. However, challenges including scalable fabrication, biocompatibility, immune clearance, and regulatory approval still hinder clinical translation. Future perspectives emphasize the integration of biohybrids, artificial intelligence, and theragnostic platforms to achieve personalized and minimally invasive cancer treatment. Collectively, nanorobots hold promise to revolutionize oncology by overcoming the limitations of current therapies and establishing a new paradigm in precision medicine.
Cancer is one of the most significant health challenges of the 21st century. According to the World Health Organization (WHO), it is the second leading cause of death globally, with nearly 10 million deaths in 2020 alone [1]. The most prevalent cancers include lung, breast, colorectal, prostate, and liver cancers, which together contribute to the majority of cancer-related deaths. Rapid urbanization, aging populations, lifestyle changes, and genetic predispositions are further driving cancer incidence worldwide [2]. The increasing healthcare burden underscores the urgent need for novel and more effective therapeutic strategies.
Despite advances in medical science, conventional cancer treatments such as surgery, chemotherapy, radiotherapy, and immunotherapy face critical challenges:
Over the past two decades, nanotechnology has revolutionized the biomedical field. Nanomedicine, which employs nanoscale materials such as nanoparticles, liposomes, micelles, and dendrimers, has already improved drug solubility, circulation times, and tumor targeting [5]. Examples include FDA-approved nanoparticle-based drugs such as Doxil® (liposomal doxorubicin) and Abraxane® (albumin-bound paclitaxel), which demonstrate how nanoscale systems can enhance cancer treatment outcomes [6]. Building upon these advancements, the integration of nanorobotics represents a next-generation step in cancer therapy.
Nanorobots are nanoscale machines capable of performing specific tasks at the cellular and molecular level [7]. They are typically fabricated from biocompatible materials such as carbon nanotubes, DNA origami, or metallic nanostructures and can be engineered to detect, navigate, and eliminate cancer cells with high precision [8]. Controlled by external stimuli (magnetic fields, ultrasound, light, or chemical gradients) or pre-programmed molecular logic gates, nanorobots can serve as autonomous therapeutic agents. Their potential lies in integrating diagnosis, therapy, and monitoring into a single nanosystem.
Nanorobots have demonstrated wide-ranging applications in oncology, with particular promise in early detection, therapy, and long-term monitoring. They can identify tumor-specific biomarkers at very low concentrations, thereby enabling early diagnosis and timely intervention. For treatment, nanorobots are capable of transporting drugs directly to tumor sites, significantly reducing systemic toxicity compared to conventional chemotherapy. Another important application lies in overcoming multidrug resistance (MDR); by bypassing efflux pumps or co-delivering resistance modulators, nanorobots can restore the sensitivity of resistant cancer cells. Furthermore, they have the potential to modulate the tumor microenvironment by addressing challenges such as hypoxia, acidity, or stromal barriers, thereby improving therapeutic response. Beyond single modalities, nanorobots facilitate combination therapies, including synergistic approaches such as chemotherapy combined with photothermal or gene therapy. Finally, nanorobots can provide continuous post-treatment surveillance, detecting recurrence or metastasis at early stages through integrated diagnostic capabilities [9,10].
The main objectives of this review are:
Nanorobotics is an interdisciplinary field combining nanotechnology, robotics, materials science, and biomedical engineering. It focuses on the design and application of nanoscale machines or robots that can perform precise tasks at the cellular or molecular level [11]. In oncology, nanorobots are envisioned as intelligent devices capable of navigating through biological environments, detecting malignant cells, and delivering therapeutic payloads directly to tumor sites with minimal collateral damage.
Nanorobots are artificially engineered nanoscale devices, typically ranging from 1–1000 nm, designed to carry out medical tasks such as diagnosis, drug delivery, tissue repair, and real-time monitoring [12]. In the context of cancer therapy, they can be programmed with highly specific functions that enhance precision and therapeutic efficiency. These include the detection of tumor-specific biomarkers, such as overexpressed receptors or circulating DNA and RNA fragments, which enable early and accurate diagnosis. Nanorobots can also selectively deliver drugs or biomolecules to malignant cells, thereby minimizing systemic toxicity and improving treatment outcomes. In addition, they are capable of inducing localized therapeutic effects such as hyperthermia or photothermal therapy, which further enhances cancer cell eradication while sparing healthy tissue. Importantly, nanorobots can also serve as diagnostic tools by reporting real-time information about tumor progression or therapeutic response, providing an integrated approach to both treatment and monitoring [13].
The design of nanorobots depends heavily on biocompatible and biodegradable materials to ensure safety and efficiency.
Different classes of nanorobots have been developed depending on their design and function:
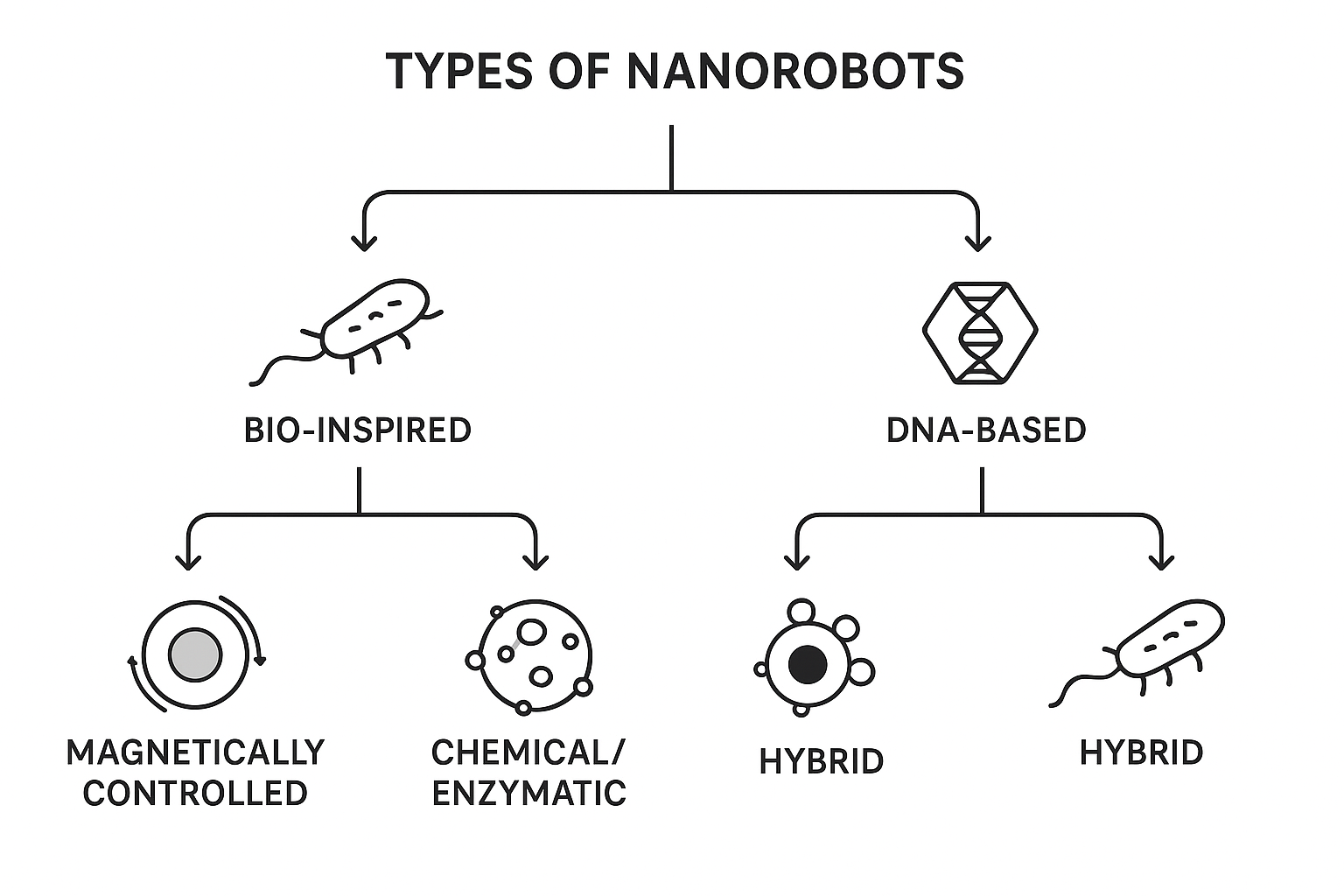
Fig: Types of Nanorobots
Mechanisms of Navigation and Control
Nanorobots require precise control mechanisms to reach tumor sites without affecting normal tissues. Current navigation strategies include:
is one of the most widely studied approaches for controlling nanorobots. In this method, nanorobots are embedded with magnetic nanoparticles such as iron oxide, which respond to external magnetic fields. By applying controlled magnetic gradients, researchers can steer these nanorobots with high precision toward tumor sites, even in deep tissue regions, in a non-invasive manner. This allows for improved accuracy of drug delivery while minimizing collateral damage to healthy cells [24].
provide another strategy for guiding nanorobots within the tumor microenvironment. Tumors are known to release specific metabolites, such as lactate, and exhibit conditions like acidic pH. Nanorobots can be engineered to sense and follow these biochemical signals, enabling autonomous movement toward cancerous tissue. This chemotactic navigation mimics natural cellular behavior and offers the advantage of selective accumulation at the diseased site [25].
uses acoustic waves to generate thrust and direct nanorobot movement in biological tissues. When exposed to ultrasound, nanostructures can oscillate or vibrate, producing mechanical forces that propel them forward. This approach not only enables non-invasive control but also benefits from ultrasound’s ability to penetrate deeply into the body, making it suitable for clinical applications such as targeted drug delivery and localized therapy [26].
employs near-infrared (NIR) or ultraviolet (UV) light to activate or guide nanorobots in specific tissues. NIR light, in particular, has good tissue penetration and can trigger photothermal effects, enabling the nanorobots to release therapeutic payloads in a controlled, site-specific manner. UV light, although less penetrative, can provide precise control in superficial tumors. This optical approach combines spatial accuracy with the possibility of activating nanorobots on demand [27].
harnesses the natural motility of living systems to drive nanorobots. Engineered bacteria, sperm cells, or enzymes can generate autonomous movement within the human body. For example, magnetotactic bacteria can migrate along magnetic field lines, while enzymatic reactions with local fuels like glucose or urea can generate thrust. These biohybrid or enzyme-driven strategies offer the advantage of natural adaptability and enhanced biocompatibility compared to fully synthetic propulsion systems [28].
Understanding the basic principles of size, materials, types, and navigation strategies is essential for applying nanorobots in cancer treatment. These parameters directly influence:
The design of nanorobots for cancer treatment requires the integration of multiple functional components: targeting elements, therapeutic payloads, navigation systems, and diagnostic modules. These systems must work in synergy to ensure precision drug delivery, minimal toxicity, and effective tumor eradication [30].
Effective targeting of cancer cells is the cornerstone of nanorobot design. Two main approaches exist:
Relies on the Enhanced Permeability and Retention (EPR) effect, where leaky tumor vasculature allows nanorobots or nanoparticles to accumulate preferentially in tumors [31].Passive targeting increases drug concentration at tumor sites compared to normal tissues but lacks specificity for individual cancer cell populations [32].
Achieved by attaching ligands, antibodies, peptides, or aptamers on nanorobot surfaces that specifically bind to overexpressed receptors on tumor cells [33].
Examples include:
Nanorobots offer spatial and temporal control over therapeutic release, minimizing systemic side effects.
Beyond therapy, nanorobots can act as diagnostic biosensors, enabling early detection and real-time monitoring:
Nanorobots are versatile and can integrate multiple therapeutic approaches:
Nanorobots can be engineered to encapsulate cytotoxic drugs such as doxorubicin and cisplatin, which are widely used in conventional chemotherapy. By delivering these agents directly to tumor sites, nanorobots ensure localized drug release while minimizing systemic distribution. This approach significantly reduces adverse effects commonly associated with chemotherapy, such as cardiotoxicity, nephrotoxicity, and immunosuppression, while simultaneously improving therapeutic efficacy. As a result, nanorobotic-assisted chemotherapy represents a major advancement over free-drug administration in terms of safety and precision [42].
Another promising application of nanorobots lies in the delivery of genetic material, including DNA, siRNA, and CRISPR-Cas9 systems. These nanodevices can transport gene-editing tools to cancer cells to silence oncogenes, repair mutations, or reprogram cellular functions. For example, siRNA-loaded nanorobots targeting the KRAS mutation in pancreatic cancer have demonstrated potential in selectively inhibiting tumor growth by suppressing key oncogenic pathways. This ability to provide site-specific and controlled delivery of genetic therapeutics makes nanorobots valuable tools for advancing cancer gene therapy [43].
Nanorobots also hold great potential in augmenting cancer immunotherapy. They can deliver immune checkpoint inhibitors, such as anti-PD-1 and anti-CTLA-4 antibodies, or cytokines directly to the tumor microenvironment. This targeted delivery improves immune activation against cancer cells while reducing systemic immune-related toxicities. Additionally, nanorobots may present tumor-associated antigens to the immune system, thereby enhancing antigen recognition and stimulating a stronger, more durable anti-tumor immune response. Such strategies can overcome resistance and improve patient outcomes in immunotherapy [44,45].
Fig: Nanorobot Function Mechanism in Cancer Therapy
Integration of Functions
Modern nanorobot designs often combine multiple features into a theranostic platform (therapy + diagnostics). For instance:
Nanorobots represent a new generation of therapeutic platforms capable of integrating diagnosis, therapy, and monitoring within a single nanosystem. Their applications in cancer treatment extend across the entire clinical spectrum—from early detection and diagnosis to treatment, prevention of metastasis, and post-therapy monitoring [49].
Early detection significantly improves survival outcomes in cancer. Nanorobots offer several diagnostic advantages:
Example: DNA origami nanorobots loaded with molecular beacons have been used for detecting microRNA biomarkers of breast cancer [53].
One of the most promising applications is the precise delivery of chemotherapy agents directly to tumor sites.
Example: pH-sensitive doxorubicin-loaded nanorobots were demonstrated to release the drug selectively in acidic tumor microenvironments [56].
Metastasis is responsible for over 90% of cancer-related deaths [57]. Nanorobots can actively patrol the bloodstream to:
Example: Magnetic nanorobots coated with epithelial cell adhesion molecule (EpCAM) antibodies showed efficiency in binding and removing CTCs in preclinical models [58].
Resistance to chemotherapy is a major limitation in cancer therapy. Nanorobots can overcome MDR by:
Example: Hybrid nanorobots co-delivering doxorubicin and P-glycoprotein inhibitors improved sensitivity of resistant breast cancer cells [61].
The tumor microenvironment (TME) is often hypoxic, acidic, and immune-suppressive. Nanorobots can:
Nanorobots can integrate multiple therapies into a single platform:
Example: DNA origami nanorobots delivering both chemotherapy drugs and CpG oligonucleotides successfully combined chemotherapy with immune stimulation in melanoma models [66].
Nanorobots may act as surveillance systems after therapy:
Example: Smart biosensing nanorobots capable of reporting tumor recurrence through fluorescence signaling have been tested in preclinical models [68].
4.8 Clinical Outlook
While most nanorobot applications remain in preclinical or experimental stages, rapid progress is being made. Ongoing research indicates that nanorobots may soon be applied in:
Table: Application of Nanorobots with advantages
|
Application Area |
Nanorobot Role & Advantage |
|
Early Detection & Diagnosis |
Detect tumor-specific biomarkers at very low concentrations; enables early and accurate diagnosis. |
|
Targeted Drug Delivery |
Transport drugs directly to tumor sites; reduces systemic toxicity and improves therapeutic efficacy. |
|
Overcoming Multidrug Resistance (MDR) |
Bypass efflux pumps or co-deliver resistance modulators; restores sensitivity to chemotherapy. |
|
Tumor Microenvironment Modulation |
Alter hypoxia, acidity, or stromal barriers; enhances therapeutic response and drug penetration. |
|
Combination Therapy |
Enable synergistic approaches (e.g., chemotherapy + photothermal + gene therapy) for improved efficacy. |
|
Post-treatment Monitoring |
Provide continuous surveillance; detect recurrence or metastasis through diagnostic capabilities. |
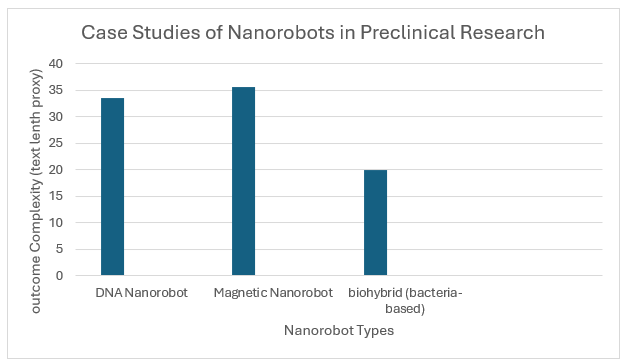
Current Research and Case Studies
A number of preclinical studies have demonstrated the potential of nanorobots in cancer therapy. One of the most significant breakthroughs was reported by Li et al., who designed DNA origami-based nanorobots capable of carrying thrombin and releasing it selectively within tumor vasculature. This caused localized clot formation, cutting off blood supply and significantly inhibiting tumor growth in mice without harming normal tissues [71]. Similarly, Xu et al. developed magnetically guided helical nanorobots that could be loaded with chemotherapeutics and precisely steered to tumors using external magnetic fields. Their results confirmed enhanced drug accumulation and improved therapeutic efficacy compared to free drugs [72]. Gao et al. further introduced enzyme-propelled nanorobots powered by urease, enabling them to actively penetrate gastric mucosa and deliver therapeutic agents. While initially applied to bacterial infections, this approach has been adapted to gastric cancer therapy, showcasing the adaptability of enzyme-powered nanorobots [73]. Biohybrid systems also represent a promising direction; Felfoul et al. demonstrated that magnetotactic bacteria carrying drug-loaded liposomes could autonomously migrate toward hypoxic tumor regions, a major challenge in oncology due to resistance to conventional therapies [74]. Together, these preclinical investigations highlight the feasibility of nanorobots in achieving targeted delivery, precise tumor penetration, and environment-responsive therapy.
While nanorobot applications remain primarily in experimental phases, important steps toward clinical translation have been made. For example, Medina-Sánchez et al. reported that cell-based micromotors could be successfully tested in large animals such as pigs and rabbits, demonstrating targeted navigation and drug delivery within vascular networks [75]. These findings suggest that nanorobot-based approaches may be scalable to human applications. Furthermore, researchers are increasingly integrating artificial intelligence (AI) and machine learning into nanorobotics, enabling enhanced control, autonomous navigation, and patient-specific therapeutic planning [76]. Although no nanorobot-based therapies have yet reached FDA approval, the convergence of nanotechnology, AI, and bioengineering provides a strong foundation for the near-future translation of nanorobots into clinical oncology.
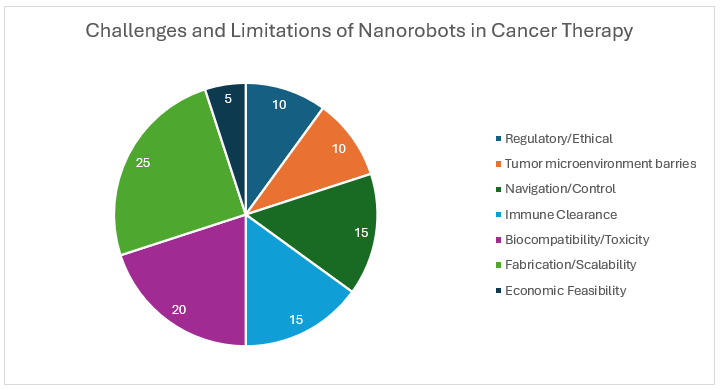
Challenges and Limitations
Although nanorobots have demonstrated remarkable potential in preclinical cancer models, several challenges hinder their transition into routine clinical practice. One of the foremost obstacles is scalable and reproducible fabrication. Current methods allow for laboratory-scale synthesis of nanorobots with precise structural features; however, large-scale production with consistent quality remains difficult. Factors such as uniform size, surface chemistry, and functionalization must be standardized before clinical application [77]. Another major challenge is biocompatibility and long-term safety. While DNA origami, polymeric, and biomimetic nanorobots are generally considered safe, many designs rely on metallic components (e.g., gold, iron oxide, or titanium) that may accumulate in the liver, kidneys, or spleen and cause toxicity [78]. Additionally, nanorobots can be recognized by the immune system, leading to opsonization and clearance by macrophages, which reduces their circulation time and therapeutic efficacy [79]. Strategies such as cell-membrane coating or PEGylation have been explored to improve immune evasion, but these approaches are not foolproof. The navigation and control of nanorobots inside the human body presents another hurdle. While magnetic fields, ultrasound, or chemical gradients have been used successfully in small animals, achieving precise navigation in humans, especially in deep-seated tumors, remains technically demanding [80]. The complexity of the tumor microenvironment (TME) also adds difficulty. Features such as hypoxia, high interstitial fluid pressure, and dense extracellular matrix limit drug penetration and reduce the efficiency of nanorobot-based therapies [81]. In addition to biological and technical barriers, regulatory and ethical challenges must be addressed. Unlike traditional drugs, nanorobots integrate mechanical, biological, and computational functions, which complicates the regulatory framework. Agencies such as the FDA and EMA have yet to establish clear approval pathways for nanorobotic therapies [82]. Ethical considerations also arise regarding autonomous nanosystems operating within the human body, including issues of patient safety, long-term monitoring, and potential misuse. Finally, economic feasibility remains a limitation. The cost of producing sophisticated nanorobots with navigation and sensing capabilities is currently much higher than conventional nanoparticle-based systems. Without cost-effective manufacturing strategies, widespread clinical adoption will be difficult. Collectively, these challenges emphasize the need for interdisciplinary collaboration among nanotechnologists, oncologists, bioengineers, and regulatory experts to refine nanorobot design, ensure patient safety, and accelerate clinical translation.
The future of nanorobots in oncology is highly promising, particularly with advances in materials science, bioengineering, and artificial intelligence (AI). One of the most exciting directions is the development of biohybrid nanorobots, which combine synthetic nanomaterials with living systems such as bacteria, stem cells, or immune cells. These biohybrids can exploit the natural homing ability of biological cells to infiltrate tumors while carrying engineered therapeutic payloads, thus improving biocompatibility and reducing immune rejection [83]. Another emerging trend is the integration of artificial intelligence and machine learning into nanorobotic systems. By processing real-time biological signals, AI-powered nanorobots may autonomously navigate complex tumor microenvironments, optimize drug release schedules, and adapt to patient-specific tumor heterogeneity [84]. This would pave the way for personalized cancer therapy, where nanorobots are tailored to the genetic and molecular profile of each patient’s tumor. The concept of theranostic nanorobots—devices capable of both therapy and diagnostics—is another key area of growth. Such systems could simultaneously detect tumor biomarkers, deliver treatment, and monitor therapeutic response in real time [85]. For example, a single nanorobot might carry chemotherapeutic agents while also emitting optical or magnetic signals to track drug release and tumor regression. In the long term, nanorobots could be combined with gene-editing technologies such as CRISPR-Cas9 to correct oncogenic mutations at the DNA level. Such precision approaches would not only eliminate tumors but also prevent recurrence by addressing cancer at its root cause [86]. Furthermore, localized cancer types, such as bladder or gastrointestinal cancers, may be the first to benefit from nanorobot-based therapies, since these organs are more accessible for external navigation and controlled intervention [87]. While widespread clinical adoption is still a decade or more away, the trajectory is clear. Continued improvements in biodegradable materials, propulsion mechanisms, immune-evasive coatings, and large-scale manufacturing will be critical to translating nanorobots into clinical oncology. Interdisciplinary collaboration among engineers, clinicians, and regulatory authorities will play a vital role in overcoming current hurdles. Ultimately, nanorobots could shift cancer therapy from systemic, toxic treatments to precise, minimally invasive, and patient-pecific interventions, representing a true paradigm shift in oncology.
Research on nanorobots has shown encouraging results in cancer therapy. Preclinical studies demonstrate that they can selectively target tumors, deliver drugs with precision, and reduce systemic toxicity. DNA-based nanorobots, magnetically guided devices, and enzyme-driven systems have all proven effective in reaching tumors and enhancing treatment outcomes, while biohybrid nanorobots show promise in penetrating hypoxic regions that resist conventional therapy. A major strength of nanorobots lies in their multifunctionality. They can integrate both diagnostic and therapeutic roles, enabling early detection, real-time monitoring, and targeted treatment within a single platform. Their ability to combine chemotherapy with gene therapy, immunotherapy, or photothermal therapy positions them as versatile tools for personalized cancer treatment. Despite these advances, challenges remain. Large-scale fabrication is difficult, long-term safety is not fully established, and immune clearance can reduce effectiveness. Controlling nanorobots in deep tissues also remains technically demanding, and regulatory and ethical concerns must be addressed before clinical translation. Looking ahead, advances in biohybrid systems, artificial intelligence, and gene-editing technologies may help overcome current barriers. If these developments continue, nanorobots could provide a major shift in oncology, moving cancer care toward safer, more precise, and patient-specific interventions.
Nanorobots represent one of the most promising frontiers in cancer therapy, offering the potential to overcome many limitations of conventional treatments. By combining advanced materials, precision targeting strategies, and intelligent navigation systems, nanorobots can achieve selective tumor detection, controlled drug delivery, and real-time therapeutic monitoring with minimal systemic toxicity. Preclinical studies have demonstrated their feasibility in diverse applications, including vascular occlusion, targeted chemotherapy, penetration of hypoxic tumor regions, and combination therapies. Early translational efforts, supported by advances in biohybrid systems and artificial intelligence, further underscore their potential clinical relevance. Nevertheless, challenges such as large-scale fabrication, long-term biocompatibility, immune system interactions, navigation in complex biological environments, and regulatory approval remain significant barriers. Addressing these limitations will require strong interdisciplinary collaboration among nanotechnologists, oncologists, bioengineers, and policymakers. Looking ahead, nanorobots are poised to transform cancer treatment by shifting from systemic, invasive approaches to precise, minimally invasive, and patient-specific therapies. If current scientific and technological hurdles can be overcome, nanorobots may soon evolve from experimental tools into practical clinical interventions, ushering in a new era of personalized oncology.
REFERENCES

Saqlain Mirasaheb Mujawar*, Dhanashree Ashok Koli, Alfaj Dastgir Tamboli, Chand Abbas Mujawar, Akash Dhananjay Patil, Use of Nanorobots in The Treatment of Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1214-1231 https://doi.org/10.5281/zenodo.17100266
 10.5281/zenodo.17100266
10.5281/zenodo.17100266
