
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Srinivas College of Pharmacy, Valachil, Farangipete Post, Mangalore, Karnataka, India.
Background: Inhaler non-adherence results in suboptimal asthma control, escalated healthcare utilization and costs, and decreased health-related quality of life. Improper inhaler usage is frequently linked with poor adherence. It is imperative to provide instruction for even the simplest of devices. The present study evaluated the relationship of asthma control and inhaler use technique in non-adherent patients. Methodology: A community based prospective study was carried out with 106 non-adherent adult asthma patients in Mangalore from March 2023 – August 2023. These subjects were randomly allocated to control and intervention group, 53 in each. Result: In the present study majority were females (54 of 106). Mean age was 50.09±11.17. Patients with controlled asthma and those with % predicted PEF?80% had efficient inhaler technique with significance p<0.001. Conclusion: The study found a strong relationship between asthma control and inhaler technique. Using the right inhaler technique can improve asthma patients' general health and reduce hospitalizations and asthma flare-ups.
Asthma is defined as chronic inflammatory disease of the airway which involves recurrent episodes of shortness of breath, chest tightness, wheezing, and coughing in response to stimuli like allergens, medications, stress, and occupational irritants. This disease affects about 300 million people globally, and its prevalence rises by 50% every ten years.[1] Asthma is mainly treated with inhaled medications in several forms, primarily including Dry Powder Inhalers (DPI), Metered-Dose Inhalers (MDI) and Soft Mist Inhalers (SMI). Easy-to-use and the ease with which a medical practitioner can instruct a patient in the proper inhalation technique should be factors in the selection of an inhaler when a patient is prescribed an inhaled medication.[2]
Noncompliance with inhaled pharmaceuticals results in suboptimal asthma control, escalated healthcare utilization and costs, and decreased health-related quality of life. [3] Improper inhaler usage is frequently linked with poor adherence. It is imperative to provide instruction for even the simplest of devices. The most effectual training method to teach the inhaler technique is verbal instruction combined with a physical demonstration.[4] With their current inhalers, only 46–59% of asthma patients use an effective inhalation technique.[2]A precise inhaler technique is of utmost importance for the optimum delivery of drugs to the lungs while also avoiding local adverse effects, such as oropharyngeal candidiasis and dysphonia, which may arise with the use of inhaled corticosteroids (ICS).[5]
Given that over 34 million persons in India suffer from asthma, a sustainable approach that may be used in clinical settings to increase controller therapy adherence is required. Pharmacists may therefore easily instruct patients on correct breathing techniques and contribute significantly to the improvement of asthma control status.[6] Effective communication is needed to identify individual barriers and interventions to improve adherence.[7] More than 25% of patients do not receive adequate instructions on how to use inhalers, according to studies. Ineffective inhalation methods can increase the likelihood of both local and systemic side effects and have a detrimental impact on the way medications are deposited in the pulmonary target region.[8] Therefore, the present study evaluated the relationship between inhaler use technique and asthma control in non-adherent patients.
MATERIALS AND METHODS:
Study Design: A community based prospective study was carried out to evaluate the relationship between asthma control and inhaler use technique in non-adherent adult patients in Mangalore.
Study Duration: The study was conducted for a duration of 6 months from March 2023 – August 2023.
Sample Size: The sample taken for the study was 106 which was based on convenience sampling method. These subjects were randomly allocated to control and intervention group, 53 in each.
Ethical Clearance: Ethical Clearance was obtained from the Institutional Ethics Committee (IEC) of Srinivas Institute of Medical Science and Research Centre (SIMS & RC), Mangalore.
Study Criteria:
Inclusion Criteria:
Exclusion Criteria:
Data Collection:
Data(s) were collected using data collection form through direct interaction with the study subjects at their residences. The data collection forms were prepared which included patient name, gender, age, and height along with information regarding asthma control, inhaler adherence and technique. Adherence to treatment was assessed using a validated TAI questionnaire, while asthma control was evaluated through ACT and % predicted PEF using a peak flow meter.
Assessment Of Inhaler Adherence:
All recruited patients were given the 10-item TAI to assess their level of adherence to chronic inhalation therapy and determine whether improper device use could contribute to non-adherence. The 10-item TAI, which identifies patients with poor adherence and their degree of adherence, is one of two complementing questionnaires that can be utilized independently based on care needs. The degree of adherence increases with the 10-item TAI score (50 points = good adherence; <50 xss=removed>[9]
Assessment Of Asthma Control:
The Asthma Control Test (ACT) was used to evaluate the patients' asthma control. The ACT consists of five questions with a response scale from 1 (poor control) to 5 (excellent control), which are separated into four areas. Controlled asthma is indicated by total scores greater than 19, and uncontrolled asthma is indicated by scores less than 19. [10]
Assessment Of Inhaler Technique:
A validated checklist for each device was used to evaluate the patients' inhaler technique. With 10 steps for DPIs and SMIs, 11 steps for MDIs, and 12 steps for MDI with valved holding chamber (VHC) and autohaler, these checklists included all the necessary processes. The ratio of the number of right steps to the total number of steps was used to compute the inhaler score. Critical mistakes are those that, on their own, will seriously hinder the drug's ability to reach the lungs. (For instance, failing to remove the device's cap, failing to shake a MDI or autohaler, improperly loading a DPI or SMI or autohaler, or failing to take a deep and forceful breath via a DPI).[11]
Study Procedure:
Statistical Analysis:
The data collected were analysed using Microsoft Excel and SPSS. Suitable statistical test such as student T test and Chi square test were applied. P-value of <0>
Result:
Demographic Details And Baseline Clinical Characteristics:
In the present study majority were females (54 of 106). Mean age was 50.09±11.17. 106 non adherent subjects identified were eligible for the intervention phase of the study. They were randomly assigned to either the intervention group or the control group, with 53 patients in each group. Patients in both the intervention and control group had similar demographic characteristics, ED/hospital visits, asthma control and technique at baseline. (Table 1). Out of 106 inhalers there were 59 MDIs, 37 DPIs, 9 SMIs and 1 Others. (Fig 1).
Table 1: Baseline demographics and clinical characteristics of patients in both group
|
Characteristics |
Control Groupn=53 |
Intervention Groupn=53 |
Total N=106 |
|
Male |
25 |
27 |
52 |
|
Female |
28 |
26 |
54 |
|
Age in years |
50.56±10.12 |
49.63±12.23 |
50.09± 11.17 |
|
Height in cm |
154±2.7 |
146±3.4 |
150±3.01 |
|
ED/hospital visit due to asthma symptoms in past 3 months |
25 |
19 |
44 |
|
Possess a peak flow meter |
13 |
14 |
27 |
|
Efficient inhaler technique |
18 |
20 |
38 |
|
Controlled asthma (ACT?20) |
8 |
5 |
13 |
|
% Predicted PEF |
64.99±14.49 |
62.73±13.49 |
97.72±13.94 |
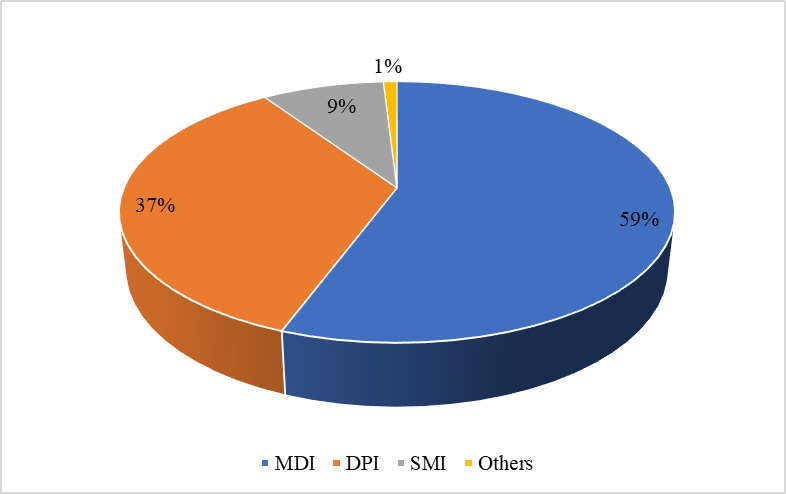
Fig 1: Percentage of non-adherent asthma patients according to inhaler sub-types
Table 2: Relationship between Inhalation technique and Asthma control using ACT and %predicted PEF in post-test (N=106)
|
|
Inhalation technique(Control group)n=53 |
p-value |
Inhalation technique(Intervention group)n=53 |
p-value |
|
Inhalation technique(Cotrol group)n=53 |
p-value |
|
Efficient(19) |
Inefficient(34)
|
|
Efficient(41)
|
|
Efficient(19) |
|
|
|
Asthma control test score (ACT) |
|
||||||
|
Controlled |
3 |
1 |
<0> |
27 |
Controlled |
3 |
<0> |
|
Partially controlled |
5 |
7 |
|
10 |
Partially controlled |
5 |
|
|
Un-controlled |
11 |
26 |
|
4 |
Un-controlled |
11 |
|
|
%predicted PEF |
|
||||||
|
?80 |
5 |
4 |
<0> |
31 |
?80 |
5 |
<0> |
|
<80> |
14 |
30 |
|
10 |
7 |
|
|
Values are expressed as n. ACT=Asthma Control Test. PEF=Peak Expiratory Flow
Relationship Of Asthma Control And Inhaler Technique:
Table 2 delineates the relationship of inhaler technique and asthma control. The current study, found that subjects in the intervention group, who received education on proper inhaler technique, were more likely to have controlled asthma and efficient inhaler technique than subjects in the control group, who did not receive education on proper inhaler technique (27 vs 3). Fig 2 illustrates in the intervention group that more number of patients with controlled asthma had efficient inhaler technique. Also, more number of patients with un-controlled asthma had in-efficient inhaler technique. Further, subjects with inefficient inhaler technique were more likely to have uncontrolled asthma and lower predicted PEF than subjects with efficient inhaler technique. This association was statistically significant, with a p-value of <0>
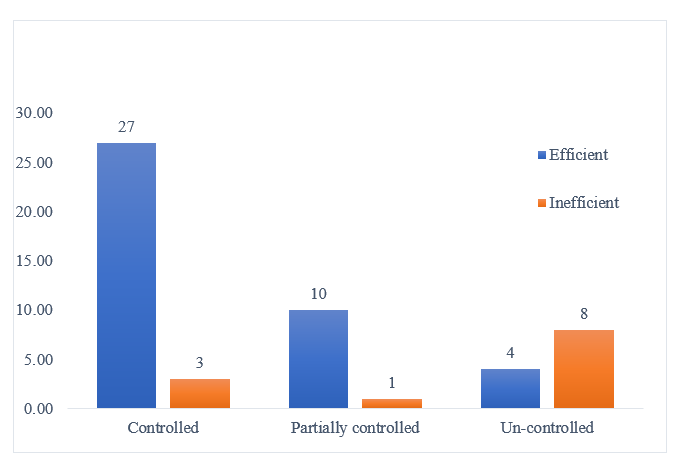
Fig 2: Post-test comparison of asthma control test score between patients with efficient and inefficient inhaler technique.
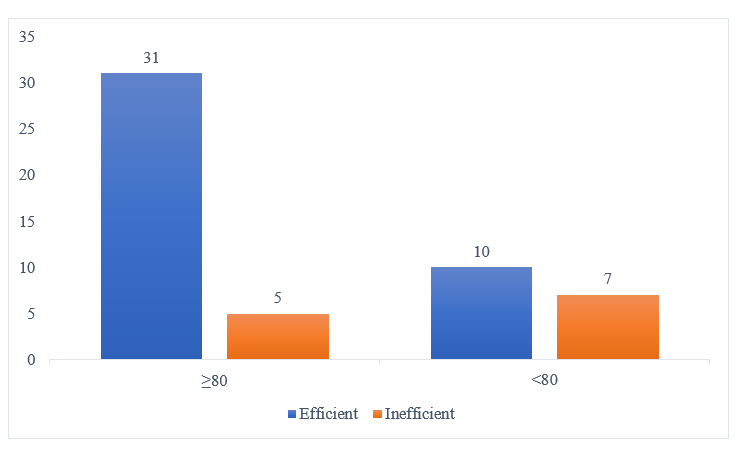
Fig 3: Post-test comparison of percentage predicted PEF between patients with efficient and inefficient inhaler technique.
DISCUSSION:
The current study found that educating patients on inhaler technique through PIL and physical demonstration significantly increased asthma control. The proportion of patients with uncontrolled asthma was relatively higher among inefficient patients as compared to efficient, demonstrating that inappropriate use of the devices is one of the significant predictors of asthma symptom control. Correct performance of critical steps involved in using the devices was one of the factors affecting asthma symptom control. These steps which include, no full expiration before inhalation and no deep inspiration and breath-hold are crucial for fully delivering the drug to the lungs and in the present study, these key steps were the ones with the highest proportion of errors which is similar to results obtained by Vanoverschelde et al. [5] Evidence for the association between poor inhaler technique and poor asthma control exists in previous literature. [12,13] Pharmacists could play an important role in teaching patients how to use their inhaler devices properly and improve asthma control. This insight highlights the critical role of educational interventions in achieving improved inhaler technique and disease control by increasing the inhaler adherence.
CONCLUSION:
The study found a strong correlation between asthma control and inhalation technique. Using the right inhalation technique can improve asthma patients' general health and reduce hospitalizations and asthma flare-ups. Inadequate asthma management and a lack of knowledge about inhalers are powerful indicators of improper inhaler use method. Inadequate technique necessitates emphasizing correct inhaler technique to patients.
ACKNOWLEDGEMENT:
We appreciate the facilities and assistance provided by the management and employees of Srinivas Hospital in Mukka, Mangalore. All study participants have our deepest gratitude for their vital contributions to this investigation.
REFERENCES

Viresh K Chandur, Abhiram U.V. Bhat*, A. R. Shabaraya, A Prospective Study on Relationship of Asthma Control and Inhaler Use Technique among Non-adherent Adult Asthma Patients in Mangalore, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 822-828. https://doi.org/10.5281/zenodo.14309302
 10.5281/zenodo.14309302
10.5281/zenodo.14309302