Kamalakshi Pandurangan College of Pharmacy, Ayyampalayam, Tiruvannamalai 60603, Tamilnadu, India.
Liver inflammation, or hepatitis, is most frequently brought on by viral infections; the most prevalent forms are hepatitis A, B, C, D, and E. These viruses differ in their modes of transmission, levels of severity, and approaches to prevention and treatment. Some types are acute and resolve on their own, while others can develop into chronic conditions that can cause cancer and liver cirrhosis, among other serious consequences. Hepatitis is a worldwide health concern, although it is still underreported and underdiagnosed. The types, symptoms, diagnosis, treatment, and prevention of hepatitis are examined in this article, which also emphasizes the significance of immunization, public health awareness, and international initiatives to eradicate viral hepatitis by 2030.
An inflammation of the liver, an essential organ that helps in digestion, stores energy, and filters toxins, is referred to as hepatitis. The most common and harmful type of hepatitis in the world is viral, while it can also be caused by medications, alcohol, chemicals, or autoimmune diseases [1]. According to estimates from the World Health Organization (WHO), millions more individuals get acute infections each year, and 354 million people have chronic hepatitis B or C [2]. Viral hepatitis is a leading cause of liver-related morbidity and mortality globally, but because of stigma, lack of knowledge, and limited access to care, it is still underdiagnosed and undertreated [3].
Overview of Hepatitis:
Hepatitis is a medical condition characterized by inflammation of the liver. Viral infections, heavy alcohol use, autoimmune disorders, toxins, and some drugs are some of the causes of this inflammation. Viral hepatitis is the most prevalent and important cause of this worldwide. A, B, C, D, and E are the five primary forms of viral hepatitis, each of which is caused by a distinct virus and has distinct clinical manifestations and mechanisms of transmission. Hepatitis A and E are mainly spread by contaminated food and water through the fecal-oral pathway. They frequently cause acute infections that typically go away without creating long-term problems. Contact with contaminated blood or body fluids is the primary way that Hepatitis B, C, and D are transferred. They can result in persistent infections, which can lead to serious liver disorders like cirrhosis and liver cancer. Hepatitis symptoms range greatly, from mild flu-like symptoms or no symptoms at all to severe liver malfunction, lethargy, jaundice, and abdominal discomfort. Regular screening and early detection are essential for controlling hepatitis and stopping its progression because some forms of the disease can go undiagnosed for years. Prevention strategies include hepatitis A and B vaccinations, sterile needle use, safe blood transfusions, basic cleanliness, and encouraging safe sexual behavior. The kind of hepatitis and the stage of the disease determine the course of treatment, but it has much improved, particularly because hepatitis B and C antiviral drugs are now widely available. Due to its high global burden and impact on public health, hepatitis remains a focus of international health initiatives aiming to eliminate viral hepatitis as a public health threat by 2030.
Types of Hepatitis:
Viral hepatitis is caused by five primary viruses: A, B, C, D, and E. These viruses differ in their methods of transmission, clinical outcomes, and geographic distribution.
Hepatitis A (HAV)
The Picornaviridae family of RNA viruses includes the hepatitis A virus. In places with inadequate sanitation, it is prevalent and spreads by the fecal-oral route, usually through contaminated food or drink [4]. The infection has a 15–50-day incubation period and is acute. Jaundice, tiredness, nausea, and abdominal pain are possible symptoms. The symptoms of hepatitis A typically go away on their own in a few of weeks and do not cause persistent liver disease. For people who work in food handling, travel to endemic areas, or live in crowded living situations, there is a highly efficient vaccine that is advised [5].
Hepatitis B (HBV)
The DNA virus known as Hepatitis B, which belongs to the Hepadnaviridae family, is spread by blood and bodily fluids, especially by sharing needles, unprotected intercourse, and delivery [6]. It takes 30 to 180 days for it to incubate. Many individuals can recover from acute infection, but many people, particularly infants and young children, get chronic hepatitis B, which can cause liver cancer or cirrhosis [7]. There is a safe and efficient vaccine that has greatly decreased the number of new infections worldwide. Tenofovir or entecavir are examples of antiviral drugs that can be used to treat chronic HBV by inhibiting viral replication [8].
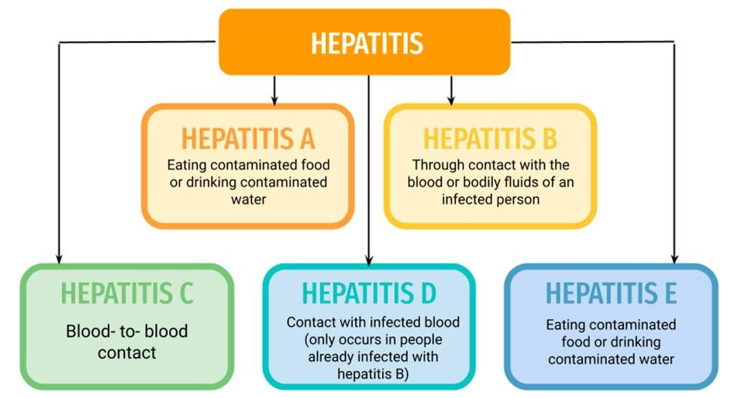
Fig.1 Types of Hepatitis
3.3 Hepatitis C (HCV)
A member of the Flaviviridae family of RNA viruses, hepatitis C is mainly transmitted by blood-to-blood contact. Common causes include unregulated tattoos or piercings, sharing needles, and risky medical practices [9]. Hepatitis C is a persistent virus that can cause long-term liver damage in up to 85% of patients if left untreated. HCV has no vaccination, in contrast to HBV. Nonetheless, the advent of direct-acting antivirals (DAAs) has transformed therapy, as most of the patients now have cure rates above 95% [10].
3.4 Hepatitis D (HDV)
Only those who currently have hepatitis B can get hepatitis D, a special RNA virus. It is spread via the same routes—blood, intercourse, and prenatal exposure—and is dependent on HBV for replication [11]. With HDV, co-infection or superinfection can cause more severe liver disease, raising the possibility of cirrhosis or liver cancer developing quickly. Although hepatitis B immunization indirectly prevents hepatitis D, there is no vaccine for hepatitis D. Pegylated interferon is one of the few available treatments, while more advanced treatments are being developed [12].
3.5 Hepatitis E (HEV)
An RNA virus called hepatitis E is mainly spread by the fecal-oral pathway, particularly through tainted drinking water. It is more prevalent in underdeveloped nations with inadequate sanitation [13]. Although the infection usually resolves on its own, pregnant women may experience severe sickness, especially in the third trimester, when the mortality rate may reach 25% [14]. Although it is not commonly accessible outside of China, a hepatitis E vaccination has a license there. Access to potable water and better sanitation are essential for prevention.
4. Symptoms of Hepatitis:
Symptoms differ according on the infection's stage and type. Symptoms common to all forms include jaundice (yellowing of the skin and eyes), pale feces, dark urine, nausea, exhaustion, loss of appetite, and stomach pain, particularly in the upper right quadrant [1].
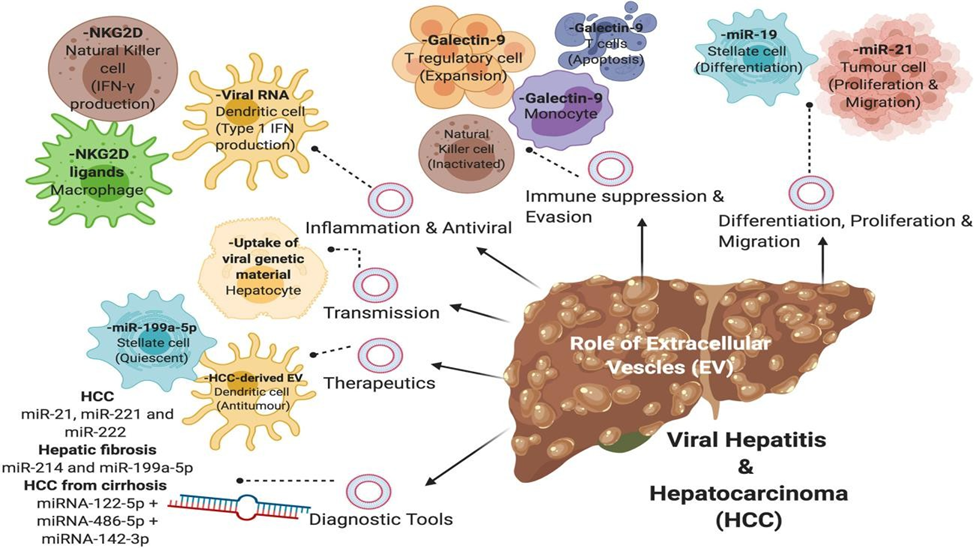
Fig 2. Transmission of Hepatitis
But many people, particularly those with hepatitis B and C, may not show any symptoms for years, which lets the virus harm the liver without anybody noticing.
5. Diagnosis:
Usually, a combination of laboratory tests and clinical assessment is used to make the diagnosis. Elevated liver enzymes, certain viral antigens and antibodies, and viral load can all be found with blood tests. To evaluate liver damage, imaging methods like elastography or ultrasonography may be utilized. Liver biopsies are sometimes done to assess the level of fibrosis or inflammation [5].
6. Treatment for Hepatitis:
The treatment of hepatitis depends largely on the type of hepatitis virus involved and the stage of the disease at diagnosis.
6.1 Hepatitis E and A:
Acute infections caused by hepatitis A and E usually go away on their own without causing long-term liver damage. The basic goals of treatment are relaxing, staying hydrated, and eating a healthy diet. Hospitalization is rarely required and typically only occurs in extreme circumstances, including fulminant hepatitis, which is not common. For these types, prophylaxis by immunization (for hepatitis A) and better sanitation is essential because there is no specific antiviral treatment [1, 13].
6.2 Hepatitis B:
Antiviral treatment for chronic hepatitis B infection is necessary to inhibit the virus's replication and lessen liver inflammation, which stops the development of cirrhosis and hepatocellular cancer. Analogs of nucleos(t)ides, such as entecavir and tenofovir, are first-line treatments because they effectively inhibit viral replication while posing few adverse effects. Depending on how well the patient responds and how severe the liver condition is, treatment may be long-term or lifelong. During therapy, it is crucial to regularly assess the viral load and liver function [6, 8].
6.3 Hepatitis C:
Direct-acting antivirals (DAAs), which target stages of the viral lifecycle, have changed the treatment of hepatitis C. When taken orally, these drugs have cure rates of above 95% after 8–12 weeks. Since DAAs were available, hepatitis C has changed from a chronic, frequently progressing illness to one that is very treatable. Preventing liver injury and transmission requires early diagnosis and treatment beginning [9, 10].
6.4 Hepatitis D:
More severe liver illness is linked to hepatitis D virus infection, which only happens in people who are already infected with hepatitis B. There are few available treatment options, and the main treatment is pegylated interferon-alpha, however its effectiveness varies and is frequently insufficient. There is continuous research into novel therapeutic agents. Vaccination to prevent hepatitis B infection also efficiently protects hepatitis D [11,12].
6.5 Chronic Monitoring for Hepatitis:
To evaluate liver function and identify problems like cirrhosis, fibrosis, or hepatocellular cancer early on, individuals with chronic hepatitis B, C, or D require long-term surveillance. This includes routine blood testing, imaging tests (such as elastography or liver ultrasonography), and occasionally liver biopsies [5].
7. Prevention:
Virus-specific prevention techniques typically consist of:
8. Global Perspective:
A serious worldwide health concern is still hepatitis. Over 1.1 million fatalities per year are attributed to liver illness caused by viral hepatitis, according to WHO [2]. By 2030, the WHO's Global Hepatitis Strategy seeks to eradicate hepatitis B and C as a danger to public health by means of increased immunization, better access to testing and treatment, and raised public awareness [3].
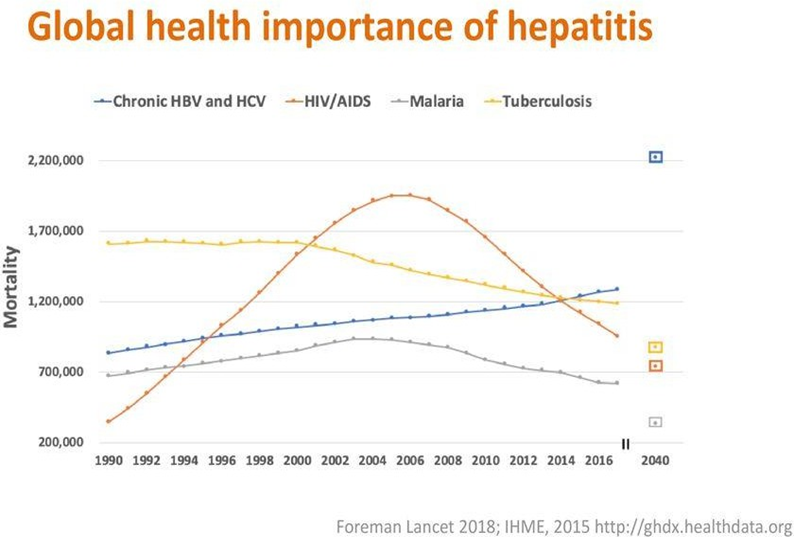
Fig 3. Global Level Health importance of Hepatitis
CONCLUSION
An illness that may be prevented and, in many circumstances, treated, hepatitis still affects millions of people globally. For the benefit of patients, medical professionals, and legislators, it is essential to comprehend the various forms of hepatitis, how they are spread, and available treatments. The global eradication of viral hepatitis and protection of liver health depend on expanded availability to vaccines, early diagnosis, and antiviral treatments as well as public health education. Even with major medical advancements, hepatitis is still underdiagnosed and underreported, particularly in low- and middle-income nations with restricted access to healthcare. Priority must be given to addressing gaps in knowledge, immunization coverage, diagnostic facilities, and treatment affordability. These gaps can be filled by bolstering primary healthcare systems and incorporating hepatitis services into larger public health initiatives.
By 2030, the World Health Organization wants to eradicate viral hepatitis as a public health concern, and this will require sustained investment in research and development for hepatitis D therapy and hepatitis E immunization. We may get closer to a time when millions of lives are not at risk from hepatitis by encouraging cooperation between governments, medical facilities, and neighborhood associations.
REFERENCES

R. V. Sivaprakash, R. Rajesh*, C. Nirmal, B. Rakesh Sharma, D. Rajalingam, R. V. Sivaprakash, R. Rajesh*, C. Nirmal, B. Rakesh Sharma, D. Rajalingam, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 690-696. https://doi.org/10.5281/zenodo.15812762
 10.5281/zenodo.15812762
10.5281/zenodo.15812762
