Valmik Naik Collage of Pharmacy Telwadi.
Vitiligo is a chronic depigmentation disorder caused by autoimmune, genetic, oxidative, and environmental factors, leading to selective melanocyte destruction. This review highlights modern treatment approaches—including corticosteroids, calcineurin inhibitors, phototherapy, and surgical grafting—along with their benefits and limitations. Growing evidence supports the role of herbal therapies such as Psoralea corylifolia, Ginkgo biloba, and traditional remedies in promoting repigmentation through antioxidant and melanogenic effects. Complementary modalities like Siddha medicine, homeopathy, and yoga further enhance management. An integrative approach combining modern, herbal, and traditional treatments may improve therapeutic outcomes and quality of life in vitiligo patients.
Vitiligo is a chronic depigmentation disorder that affects approximately 0.5–2% of the global population, characterized by the selective destruction of melanocytes, leading to well defined white macules on the skin (Moreira et al., 2015). The condition, first described over 3,000 years ago in ancient Vedic and Egyptian texts, has been referenced across various religious traditions (Millington & Levell, 2007). Its prevalence varies worldwide, reaching up to 4% in some South Asian, Mexican, and American populations (Parsad et al., 2003). Vitiligo results from a complex interplay of genetic, autoimmune, oxidative, and environmental factors, often influenced by psychological stress and biochemical imbalances (Zhou et al., 2022).
The disease manifests as smooth, depigmented patches that commonly appear on the face, hands, axillae, umbilicus, and genital areas (Ezzedine et al., 2015). It can occur at any age, with nearly half of cases appearing before age 20. Clinical diagnosis is supported by tests for autoimmune disorders, such as thyroid-stimulating hormone and antinuclear antibody assessments, as well as Wood’s lamp examination, which aids in evaluating disease activity and treatment response (Halder & Chappell, 2009; Wang et al., 2017).
Conventional treatments include topical corticosteroids, calcineurin inhibitors, vitamin D analogs, phototherapy, excimer laser, depigmentation, and surgical grafting, yet these methods often produce incomplete or temporary repigmentation and can cause side effects (Halder & Chappell, 2009). This has led to growing interest in herbal and alternative therapies as safer, complementary options. Herbal agents such as Psoralea corylifolia (Babchi), Ginkgo biloba, khellin, and capsaicin have shown antioxidant, anti-inflammatory, and melanogenic effects that may stimulate melanocyte regeneration and pigment restoration (Pekmezci, 2019).
Recent research increasingly supports the potential of herbal medicines in vitiligo management. Integrating these natural therapies with modern clinical approaches may offer a more holistic, effective, and safer strategy to improve both repigmentation outcomes and quality of life for vitiligo patients.

(Figure no:1)
ETIOLOGY
The exact etiology of vitiligo remains unclear, but it is recognized as a multifactorial and polygenic autoimmune disorder. Several interrelated mechanisms are believed to contribute to melanocyte destruction. The autoimmune theory suggests that the body’s immune system attacks melanocytes, supported by links with diseases like thyroiditis and diabetes mellitus. The cytotoxic theory proposes that toxic by-products of melanin synthesis damage pigment cells. The neural theory indicates that nerve chemicals may inhibit melanin formation. In the oxidative stress theory, excessive free radicals harm melanocytes. The genetic theory shows involvement of susceptibility genes such as NALP1, with nonMendelian inheritance. Environmental and triggering factors— like sunburn, trauma, or stress—may initiate the process. Thus, vitiligo results from a complex interaction of genetic, immune, and environmental elements.
PATHOPHYSIOLOGY
The pathophysiological mechanism of vitiligo is complex and multifactorial, involving both autoimmune and intrinsic cellular factors that affect melanocyte survival, ultimately leading to their destruction and the loss of skin pigmentation. The most widely accepted theory is the autoimmune hypothesis, which suggests that the body’s immune system mistakenly targets and destroys melanocytes. This concept is supported by the presence of melanocyte-specific antibodies and cytotoxic T lymphocytes that attack these pigmentproducing cells. Moreover, vitiligo is frequently associated with other autoimmune disorders such as ; thyroid disease, diabetes, and alopecia areata, further reinforcing the immunemediated mechanism.
In addition to autoimmunity, genetic susceptibility plays an important role. Several genes linked to immune regulation and melanocyte function have been identified, predisposing individuals to vitiligo. Environmental triggers such as trauma, stress, or chemical exposure may further initiate melanocyte destruction in genetically predisposed individuals.
Another major contributing factor is oxidative stress, particularly due to the accumulation of hydrogen peroxide (H?O?) in the skin. This imbalance between oxidants and antioxidants impairs cellular defense mechanisms, resulting in melanocyte damage and apoptosis.
Intrinsic melanocyte defects also contribute to disease progression. Some melanocytes exhibit functional abnormalities, making them more vulnerable to oxidative injury and immune attack. Apoptotic dysregulation further accelerates cell loss by disturbing the balance between cell survival and programmed death.
Additionally, neurogenic mechanisms have been proposed, where toxic neurochemical mediators released from nerve endings adversely affect melanocytes. Viral infections, such as cytomegalovirus (CMV), may also act as external triggers in certain cases.
Autoimmune Mechanism
The body’s immune system mistakenly attacks melanocytes.
Presence of anti-melanocyte antibodies and T-cell mediated destruction.
Commonly associated with other autoimmune diseases (e.g., thyroid disease, Type 1 diabetes). Increased inflammatory cytokines (IL-6, TNF-α) are found in patients.
Oxidative Stress Theory
Excess production of reactive oxygen species (ROS) damages melanocytes.
Reduced antioxidant defense makes melanocytes more vulnerable.
Leads to cellular injury and apoptosis (cell death).
Neural Factors
Neurochemicals like catecholamines and neuropeptides from nerve endings may harm melanocytes.
This theory explains cases where vitiligo appears after emotional stress.
Genetic Predisposition
Family history and certain genes increase susceptibility.
GWAS studies show involvement of genes related to immune regulation and melanocyte function.
CLASSIFICATION OF VITILIGO
Vitiligo is mainly classified into Non-Segmental Vitiligo (NSV) and Segmental Vitiligo (SV).
This classification is based on pattern of distribution, progression, prognosis, and response to therapy.
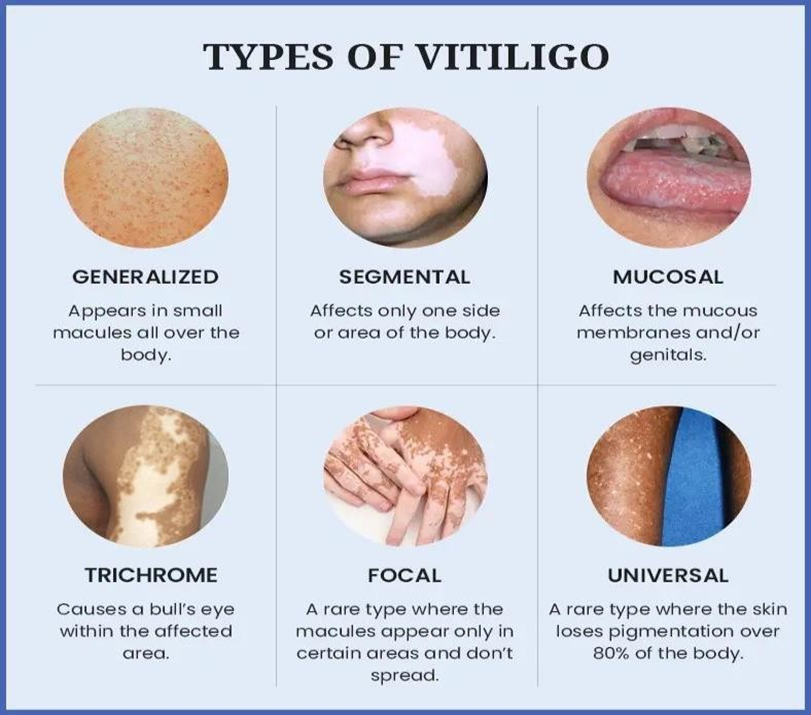
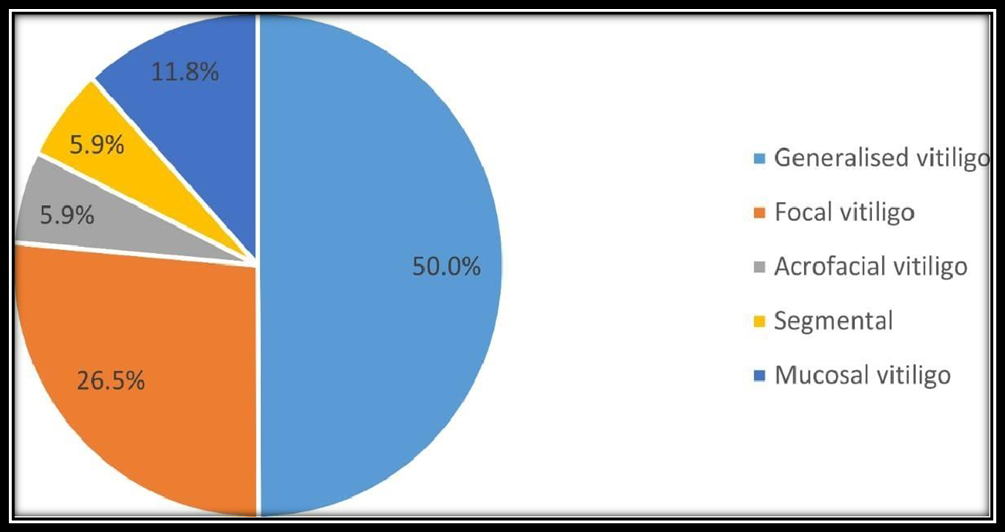
(Figure No:2)
Non-Segmental Vitiligo (NSV) Most common type. Symmetrical and bilateral distribution of white patches. Slow, progressive course, may worsen over time.
Generally, responds better to treatment than SV.
Subtypes of NSV:
Focal: One or few small patches in one area (may progress to generalized). Mucosal : Involves one or more mucosal sites (e.g., oral, genital).
Acrofacial: Affects face and distal extremities (hands/feet).
Generalized: Widespread patches over body surface.
Universal: >80% body pigmentation loss.
Segmental vitiligo (SV)
Less common, but more distinct.
Occurs in a single segment or along dermatome-like patterns. Usually unilateral and does not cross the midline.
Rapid onset (progresses for 6 months–2 years) and then stabilizes. Frequently associated with leukotrichia (white hair within patches). Responds less well to conventional treatments.
(Figure no :3)
PSYCHOLOGICAL IMPACT AND SOCIAL CONSEQUENCES
Vitiligo often affects self-image due to visible skin patches. Patients may experience emotional distress, including shame, insecurity, anxiety, and depression. Quality of life is reduced, especially when lesions occur on the face and hands. Many patients report social stigma, such as staring, rude remarks, and even workplace discrimination, contributing to low confidence and social withdrawal.
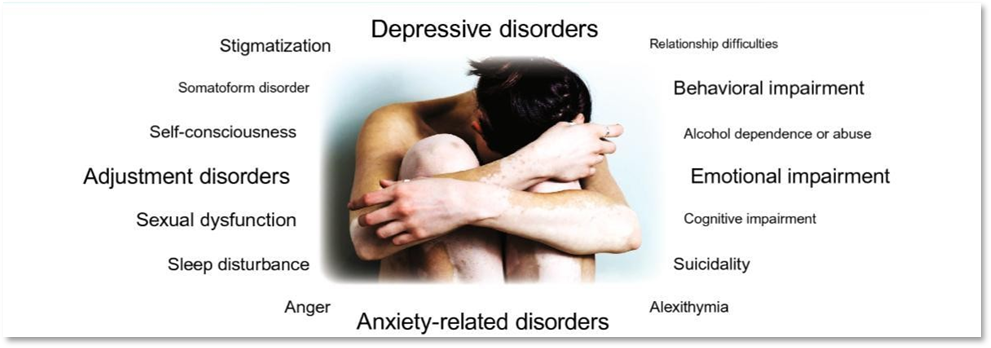
(Figure no: 4)
Associated Medical Conditions Thyroid Dysfunction
Thyroid abnormalities, particularly autoimmune thyroid disorders, are commonly linked with vitiligo. People with vitiligo have a higher likelihood of developing both obvious (clinical) and hidden (subclinical) thyroid conditions than the general population. The two thyroid diseases most frequently associated with vitiligo are Hashimoto’s thyroiditis and Graves’ disease. In a study from 1994 involving 35 vitiligo patients, 43% showed indications of thyroid involvement, with 22.8% having thyroid dysfunction (including 17.1% with hyperthyroidism and 5.7% with hypothyroidism). Individuals with autoimmune thyroid disease are more likely to develop vitiligo than those with non-autoimmune thyroid issues. This relationship is particularly strong in patients with generalized (non-segmental) vitiligo, especially when there is a family history of autoimmune disorders.
Other Autoimmune Disorders
Research indicates that vitiligo is often linked with several other autoimmune disorders, such as pernicious anemia, diabetes mellitus, systemic lupus erythematosus, rheumatoid arthritis, psoriasis, alopecia areata, and Addison’s disease. A study carried out between 2001 and 2006 in a Romanian population with strong family ties found that among 51 individuals with vitiligo, 22 also had at least one additional autoimmune condition. Of those with both vitiligo and another autoimmune disorder, about 82% exhibited generalized vitiligo. Within this group, 31% had autoimmune thyroid disease, 14% had rheumatoid arthritis, and 12% had adult-onset type 1
diabetes. Furthermore, these autoimmune diseases were more frequently observed in first-degree relatives of vitiligo patients, suggesting a hereditary susceptibility to autoimmune and autoinflammatory conditions within certain families.
DIFFERENTIAL DIAGNOSIS
For diagnosing vitiligo, it is essential to distinguish between complete loss of pigment, partial hypopigmentation, and normally pigmented skin. This distinction becomes more challenging in individuals with fair skin. When vitiligo appears in its typical symmetrical form, the diagnosis is usually clear and can be confidently established in primary care settings. Wood’s light can assist in confirming the diagnosis and in identifying the extent and activity of the lesions, especially in people with skin types I and II. It is also useful for monitoring the response to treatment. Additionally, due to the high association of vitiligo with autoimmune thyroid disorders, thyroid function tests should be considered in adult patients.
Equipment Used in the Diagnosis of Vitiligo
Pure tone and speech audiometer Sound-treated examination room
Cochlear emission analyzer (Madsen) Immittance meter
Evoked response audiometer (Nicolet Compact Four) Wood’s lamp (Wood’s light)
MEDICAL MANAGEMENT OF VITILIGO
Topical Corticosteroids
Topical corticosteroids are among the most commonly prescribed medications for vitiligo.
A 1998 meta-analysis revealed that class III and IV corticosteroids produced over 75% repigmentation in 56% of segmental and 55% of generalized vitiligo patients.
Further research in 1999 established evidence-based guidelines for their use in both adults and children.
Overall, class III corticosteroids were identified as the most effective and safest option, especially for segmental vitiligo.
Topical Immunomodulators
Topical immunomodulators such as tacrolimus and pimecrolimus were developed to minimize side effects associated with corticosteroids.
Studies have demonstrated comparable efficacy to corticosteroids but without adverse effects like skin atrophy.
However, due to concerns regarding long-term safety, these agents are best suited for localized or sensitive areas (e.g., eyelids).
A notable observation includes a case of localized hypertrichosis (excess hair growth) in a child treated with tacrolimus.
Systemic PUVA (Psoralen + UVA Therapy)
PUVA therapy was first introduced in the 1940s for vitiligo treatment. It involves administering psoralen followed by UVA exposure.
Although effective, complete repigmentation is rare, and treatment duration (1–3 years) is long. Darker skin tones generally respond better than lighter ones.
Common adverse effects include nausea, vomiting, phototoxicity, and a potential risk of skin cancer.
Due to these limitations, PUVA use has declined, especially in the United States.
Topical PUVA
Topical PUVA was designed to target smaller affected areas, reducing systemic exposure to psoralen.
While effective, it can cause erythema, blistering, and hyperpigmentation of nearby normal skin.
When compared to narrowband UVB (NB-UVB) therapy, both showed similar efficacy, but NB- UVB had fewer side effects and a lower cumulative UV dose.
Narrowband UVB (NB-UVB) Therapy
NB-UVB phototherapy has emerged as a safe and effective treatment, particularly for generalized vitiligo in children.
A 1999 meta-analysis identified it as the most effective and safest method.
Best responses occur on the face and neck, while hands and feet respond poorly. Treatment three times per week yields better results than twice-weekly sessions.
Microphototherapy (Targeted UVB)
Microphototherapy is a localized form of NB-UVB, delivering UV light only to depigmented areas. In clinical trials, 70% of patients achieved over 75% repigmentation.
This method is ideal for individuals with <30% body surface area (BSA) involvement and is particularly suitable for children, as it minimizes radiation exposure to normal skin.
Monochromatic Excimer Light (MEL)
MEL therapy uses focused light to stimulate repigmentation in segmental and generalized vitiligo.
Studies show that 95% of patients achieved some repigmentation, and 50% showed >75% repigmentation.
Notably, some patients unresponsive to NB-UVB improved with MEL.
Compared to excimer lasers, MEL offers lower risk of overexposure, ability to treat larger areas, and shorter treatment durations.
However, its safety and efficacy in children (<15 years) remain under investigation.
SURGICAL MANAGEMENT OF VITILIGO
1. Epidermal Grafting Techniques Surgical grafting is particularly effective for stable segmental vitiligo.
Methods include mini-punch grafting and suction blister (blister roof) grafting.
Studies have shown best outcomes in segmental cases and patients below 20 years of age. In contrast to medical therapies, site of vitiligo does not significantly affect results.
Among surgical methods, split-skin grafting has shown superior results, especially for face and limbs.
Epidermal Cell Transplantation
This advanced approach involves applying a melanocyte-rich cell suspension to depigmented areas.
It minimizes complications like cobblestoning and allows larger area coverage. Best results are seen in segmental vitiligo or patients with localized involvement. If successful, it usually requires only a single treatment session.
COSMETIC AND SUPPORTIVE MANAGEMENT
Cosmetic Camouflage
Cosmetic camouflage products help mask depigmented patches, improving selfconfidence and quality of life.
Brands such as Dermablend, Covermark, Derma Color, Dermage, and Elizabeth Arden Concealing Cream are commonly used.
Studies show that camouflage improves self-esteem, reduces embarrassment, and enhances clothing choices—especially for facial lesions.
Skin Bleaching (Depigmentation Therapy)
In adults with extensive vitiligo, depigmentation of the remaining pigmented skin may be considered to achieve uniformity.
Agents include monobenzyl ether of hydroquinone (monobenzone) and Q-switched ruby laser.
However, this is not recommended in children, as the process is permanent and may be psychologically distressing.
TRADITIONAL REMEDIES FOR THE MANAGEMENT OF VITILIGO
In traditional medicine, several herbal and natural preparations have been used in the treatment of vitiligo and leucoderma. One well-known remedy involves Psoralea corylifolia (Babchi) seeds. The seeds are traditionally soaked in ginger juice or cow’s urine for approximately three days, with the liquid being replaced daily. After soaking, the seeds are rubbed between the hands to remove the outer husk, dried away from direct sunlight, and ground into a fine powder. About one gram of this powder is recommended to be taken daily with fresh milk for a period of 40 days. Additionally, the powdered form of the seeds can be externally applied to depigmented patches to help stimulate repigmentation.
A combination of Babchi seeds and Tamarind seeds is also commonly utilized. Equal portions of both seeds are soaked in water for three to four days. Once softened, they are peeled, dried in shade, and ground into a paste. This paste is applied over affected skin areas for one week. If symptoms such as redness, itching, or oozing occur, the application should be stopped immediately. However, if no irritation develops, the oral use of Babchi seeds may be continued for another 40 days.
Red clay found near riverbanks or hill slopes is also used traditionally for leucoderma. When mixed with ginger juice and applied to white patches, the copper content in the clay is believed to assist in restoring pigmentation, while the ginger increases local blood circulation.
Another traditional preparation uses radish seeds. Approximately 35 g of radish seeds are ground using vinegar and applied to the affected areas. Enhanced effect is claimed when the seeds are mixed with a small amount of white arsenic and soaked overnight in vinegar before application.
A widely practiced remedy is the use of turmeric combined with mustard oil. About 500 g of turmeric is boiled overnight in eight liters of water until the volume reduces to one liter. The strained solution is then mixed with 500 g of mustard oil and reheated until only the oil remains. This oil mixture is applied to the affected areas twice daily for several months.
SIDDHA SYSTEM APPROACH
Vitiligo is considered a significant condition in Siddha medicine, particularly in tropical regions. Siddha practitioners note that individuals such as professional hairdressers, agricultural workers exposed to pesticides, frequent users of hair dyes, and those wearing footwear made from low- quality rubber may show increased susceptibility.
Several Siddha classical texts reference formulations for vitiligo. Some of the most commonly cited herbs include:
Aristolochia indica (Aristolochiaceae)
Traditionally used for disorders such as malaria, anemia, allergies, joint pain, and certain toxic states. The root is specifically noted to be beneficial in vitiligo therapy.
Tribulus terrestris (Zygophyllaceae)
Known in classical Tamil literature for possessing “photo-helium” properties that are believed to assist in pigment restoration. It is described as useful in various “Megha” (skin discoloration) conditions, including vitiligo.
Thespesia populnea (Malvaceae)
The root of mature plants is considered valuable for long-standing skin diseases including vitiligo and leprosy. Its inner bark is traditionally chewed to restore pigmentation, especially around the lips.
Siddha preparations in powder (Chooranam) form are also commonly used to restore natural skin coloration.
HOMEOPATHIC MANAGEMENT
Homeopathic treatment emphasizes a holistic approach, focusing not only on the physical presentation of vitiligo but also on the individual’s mental and constitutional tendencies. Detailed case history, emotional profile, and genetic predisposition are considered before selecting medicines. Commonly used remedies include Arsenicum album, Arsenicum sulphuratum flavum, Bacillinum, Graphites, Mercurius solubilis, Natrum muriaticum, Nitric acid, Nux vomica, Phosphorus, Sepia, Silicea, Sulphur, and Thuja, although specific remedy selection varies from patient to patient.
YOGA THERAPY
Among yogic practices, Kapalbhati Pranayama is specifically recommended. Performed in the morning on an empty stomach, this breathing exercise enhances blood oxygenation and circulation. Its consistent practice is reported to support improvement in skin health and is traditionally believed to help in conditions such as vitiligo, eczema, psoriasis, and certain anxiety-related disorders.
AYURVEDIC PERSPECTIVE AND MANAGEMENT
In Ayurveda, vitiligo (referred to as Kilas, Darun, Charun, or Switra) is considered a tridoshaja disorder where improper dietary habits lead to imbalance of Vata, Pitta, and Kapha doshas. These imbalances affect deeper tissues such as blood (rakta), muscle (mamsa), and adipose (meda).
Ayurvedic treatment focuses on:
Selecting appropriate herbal medicines that target the root cause. Maintaining patience and a positive mental attitude.
Strict adherence to dietary and lifestyle restrictions. Developing faith in the treatment process.
Ayurvedic therapy strengthens the immune system and improves metabolic activity to counter the autoimmune tendencies associated with vitiligo.
Herbal Drugs and Their Active Constituents
The use of herbal remedies in treating skin conditions has deep roots in traditional medicine. Modern research has increasingly focused on identifying and understanding the active phytochemicals responsible for their therapeutic effects. The following herbal agents have shown promising outcomes in the management of hypopigmented skin lesions, including vitiligo.
Psoralea corylifolia (Babchi)
Psoralea corylifolia, commonly called Babchi, is one of the most thoroughly researched herbs for vitiligo. Its seeds contain psoralen and isopsoralen—furocoumarin compounds that stimulate melanin production when activated by UV-A light. Psoralen has been found to enhance tyrosinase activity, a key enzyme involved in melanin synthesis. Clinical evidence shows that topical Babchi preparations used in combination with narrowband UVB (NBUVB) phototherapy can lead to notable repigmentation. Additionally, laboratory studies suggest that psoralen may also help regulate immune responses and reduce local skin inflammation.
Ginkgo biloba
Ginkgo biloba extracts are rich in terpenoids and flavonoids, which have strong antioxidant effects. Since oxidative stress plays a major role in melanocyte damage in vitiligo, the free radical– scavenging properties of Ginkgo are particularly beneficial. Clinical trials have shown that oral supplementation with Ginkgo biloba may help slow disease progression and promote repigmentation in some patients. Its ability to improve microcirculation and protect nerve cells may also contribute to maintaining melanocyte function.
Curcumin (from Curcuma longa)
Curcumin, the primary active compound in turmeric, is known for its anti-inflammatory and antioxidant activities. Although its direct role in melanin formation is still debated, curcumin’s ability to reduce inflammatory cytokines and protect melanocytes from oxidative stress makes it a useful supportive therapy. Experimental studies indicate that curcumin boosts the skin’s natural antioxidant defenses, though more clinical research is needed to determine ideal dosing for vitiligo treatment.
Nigella sativa (Black Seed)
Black seed oil, derived from Nigella sativa, contains thymoquinone, a molecule with strong anti- inflammatory and antioxidant effects. Preclinical studies show that thymoquinone can lower reactive oxygen species (ROS) levels and help prevent melanocyte cell death. Early clinical reports suggest that topical preparations of Nigella sativa may improve repigmentation when used alongside standard therapies.
Additional Herbal Candidates
Several other plant-derived agents also show potential benefits in vitiligo care: Aloe vera: Known for reducing inflammation and promoting skin repair.
Milk Thistle (Silybum marianum): Its active compound, silymarin, offers antioxidant protection that may help minimize systemic oxidative stress.
Green Tea (Camellia sinensis): Catechins in green tea provide strong antioxidant support and may help protect melanocytes from UV-related damage.
Ashwagandha (Withania somnifera): Traditionally used for immune balancing and stress regulation, which may aid in autoimmune aspects of vitiligo.
Herbal drugs list which affected on white skin patch
|
Sr.no |
Herbal (biological name) |
Common name |
Part used |
Treatment support |
|
1. |
Plumbago indica (Plumbaginaceae) |
Chitraka |
Root and bark |
Used for vitiligo skin |
|
2. |
Psoralea corylifolia (Fabaceae) |
Bakuchi |
Seeds, root, leaves |
Alleviates vitiligo |
|
3. |
Semecarpus anacardium (Anacardiaceae) |
Bhallataka |
Nuts, oil, flowers |
Nuts crushed with cow urine |
|
4. |
Terminalia bellerica (Combretaceae) |
Bibhitaka |
Fruit and seed |
Used for vitiligo skin |
|
5. |
Nigella sativa (Ranunculaceae) |
Kalonji |
Seeds and oil |
Used for vitiligo skin |
|
6. |
Ginkgo biloba (Ginkgoaceae) |
Ginkgo |
Extract (40 mg, three times/day for six months) |
Promotes repigmentation |
|
7. |
Picrorhiza kurroa (Plantaginaceae) |
Kutki / Gentian |
400–1500 mg as powder encapsulated/ day |
Promotes repigmentation |
|
8. |
Zingiber officinale (Zingiberaceae) |
Ginger |
Tincture, tea, tablet, capsule |
Bowel strengthening |
|
9. |
Ammi visnaga (Apiaceae) |
Khella |
Tincture (internal and external) |
Enhances pigmentation |
|
10. |
Silybum marianum (Asteraceae) |
Milk Thistle |
tincture, capsule |
Liver protectant, tonic |
|
11. |
Tribulus terrestris (Zygophyllaceae) |
Gokhru |
Fruit powder |
Promotes repigmentation |
|
12. |
Azadirachta indica (Meliaceae) |
Neem |
Leaves |
Promotes repigmentation |
|
13. |
Picrorhiza kurroa (Plantaginaceae) |
Picrolex |
Root extract |
Promotes repigmentation |
|
14. |
Ammi majus (Apiaceae) |
Bishop’s Weed |
Fruits |
Promotes repigmentation |
CONCLUSION
Vitiligo is a complex, multifactorial skin disorder influenced by autoimmune, genetic, oxidative, and environmental factors. Although modern medical treatments—such as corticosteroids, calcineurin inhibitors, phototherapy, and surgical grafting—offer significant benefits, they often provide incomplete or temporary repigmentation. This has increased interest in herbal, traditional, and holistic approaches like Psoralea corylifolia, red clay, Siddha formulations, and yoga practices, which may support melanocyte regeneration and improve treatment outcomes. Integrating modern therapies with safe, evidence-supported herbal and traditional remedies can provide a more comprehensive and patient-centered strategy. A multimodal approach not only enhances repigmentation but also supports psychological well-being, offering improved quality of life for vitiligo patients.
REFERENCES

Muni Chandragade*, Renuka Sagane, Vitiligo Management Through Modern, Herbal and Traditional Modalities: A Detailed Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 404-419 https://doi.org/10.5281/zenodo.17797773
 10.5281/zenodo.17797773
10.5281/zenodo.17797773
