Dr. DY Patil College of Pharmacy, Akurdi, Pune, 411044
Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Among the various transmucosal routes, buccal mucosa has excellent accessibility and relatively immobile mucosa, hence suitable for administration of retentive dosage form. The objective of this paper is to review the works done so far in the field of mucoadhesive buccal drug delivery systems (MBDDS), with a clinical perspective. Starting with a brief introduction of the mucoadhesive drug delivery systems, oral mucosa, and the theories of mucoadhesion, this article then proceeds to cover the works done so far in the field of MBDDS, categorizing them on the basis of ailments they are meant to cure. Additionally, we focus on the various patents, recent advancements, and challenges as well as the future prospects for mucoadhesive buccal drug delivery systems.
The field of drug delivery has witnessed significant advancements over the years, aiming to improve therapeutic efficacy, reduce side effects, and enhance patient compliance. One such promising area of research is the development of mucoadhesive drug delivery systems. These specialized formulations have garnered considerable attention for their ability to adhere to the mucosal surfaces of various tissues, offering a unique and targeted approach to drug administration . In recent years, significant strides have been made in understanding the intricate interactions between mucoadhesive polymers and mucosal tissues, leading to the design of more efficient and effective drug delivery systems. Researchers have explored various routes of administration, such as buccal, nasal, vaginal, and ocular, each offering unique advantages for specific therapeutic applications .
Since the early 1980s, the concept of mucoadhesion has gained considerable interest in pharmaceutical technology. Adhesion can be defined as the bond produced by contact between a pressure -sensitive adhesive and a surface1. The American society of testing and materials has defined it as the state in which two surfaces are held together by interfacial forces, which may consist of valence forces, interlocking action or both. The adhesion processes have demonstrated important purposes in nature and consequently, have diverse healthcare and non-biomedical implications, such as bacterial adhesion or water purification. In pharmaceutical sciences, bioadhesion is described as the ability of a dosage form to come into close contact, by attractive interactions with a biological surface (epithelial tissue or mucus coat). If the biological environment is the mucosal surface or mucous coat, this process is termed mucoadhesion . Bio-adhesion (or mucoadhesion) is generally understood to define the ability of a biological or synthetic material to “stick” to a mucous membrane, resulting in adhesion of the material to the tissue for a protracted period of time.
Structure and Composition of Mucous and Mucus Layers
The mucous membrane (mucosae) is characterized as a moist layer of connective tissue (thelamina propria), with an epithelial layer covered by mucus. According to the body cavity, these epithelia can be multilayered/stratified, such as in the vagina, cornea and esophagus, or single layered, like the small and large intestine. Moreover, this membrane has demonstrated a great ability for the absorption of active substances, since it is relatively permeable, enabling the quick absorption of drugs14-16. Mucus is a complex and viscous fluid synthesized by goblet cells. These glandular cells are present in every epithelium layer exposed to the external environment. Mucus is found as a gel layer which adheres to surfaces, as a soluble form, or suspended within the channels, creating a fully hydrated viscoelastic gel layer. This is composed of glycoproteins, including mucin, which is responsible for the gel structure and appearance, lipids, inorganic salts, proteins, mucopolysaccharides, IgA, lysozyme and 95% water. Mucin can be bound to the mucous membrane or secreted.
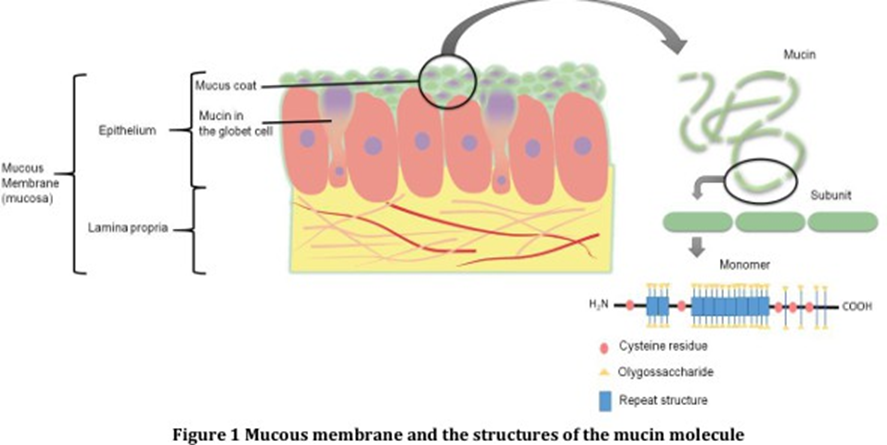
The latter entangles and adhesively crosslinks reversibly in order to make up the viscoelastic, shear- thinning gel, by physiological mechanisms. Although mucin is the main factor responsible for the mucus gel properties, the viscoelastic behavior is also governed by water content, and lipids and ions from the mucus, being crucial for protection and lubrication. Furthermore, mucin (Figure 1) behaves as an anionic polyelectrolyte at neutral pH due to sialic acid, which is believed to be responsible for the bacteriostatic action observed in mucus. Mucus exhibits many functions such as protection and lubrication of the epithelium, in order to impair the absorption of microorganisms and other substances. In addition, mucus allows the passage of objects and preservation of the hydrated mucous layer, while other supplementary functions depend on the epithelium being covered. Although mucus has demonstrated numerous functions, it is a dynamic system, being continuously removed from the epithelial layer and can reduce the residence time, as well as decrease the drug delivery rate at the site of administration.
Additionally, their properties, composition and thickness can be influenced by pathologies. In this context, gastrointestinal, nasal, ocular, buccal, vaginal, rectal and periodontal areas are covered by a mucous membrane and can be employed for the administration of mucoadhesive drug delivery systems. According to the site of secretion, the pH and the thickness of the mucous layer are variable. The mucus pH in the eye is slightly basic, close to 7.8. However, for the lung and nasal cavity, the pH is 5.5-6.5. Also, the balance between the rate of mucus secretion and its rate of degradation and shedding regulate the thickness of the mucus layer.
Mucoadhesion Theories
Mucoadhesion is a complex process and numerous theories have been proposed to explain the mechanisms involved. These theories include mechanical interlocking, electrostatic, diffusion interpenetration, adsorption and fracture processes.
Wetting Theory
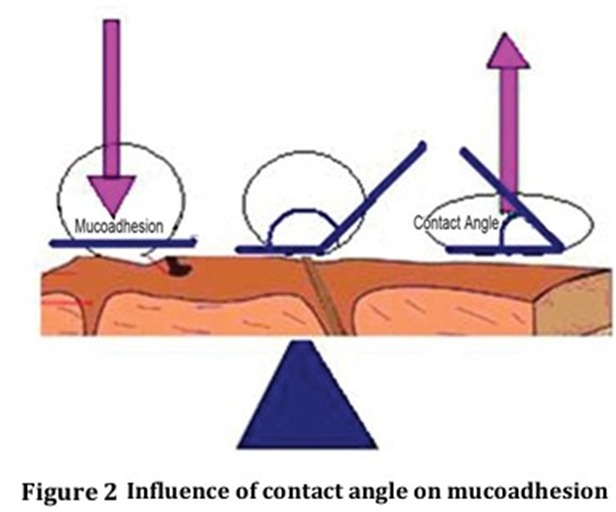
The wetting theory applies to liquid systems which present affinity to the surface in order to spread over it. This affinity can be found by using measuring techniques such as the contact angle. The general rule states that the lower the contact angle, the greater is the affinity [Figure 2]. The contact angle should be equal or close to zero to provide adequate spreadability. The spreadability coefficient, SAB, can be calculated from the difference between the surface energies γB and γA and the interfacial energy γAB, as indicated in the equation given below15. This theory explains the importance of contact angle and reduction of surface and interfacial energies to achieve good amount of mucoadhesion.
SAB = γB ? γA ? γAB
Diffusion Theory
Diffusion theory describes the interpenetration of both polymer and mucin chains to a sufficient depth to create a semi-permanent adhesive bond . It is believed that the adhesion force increases with the degree of penetration of the polymer chains. This penetration rate depends on the diffusion coefficient, flexibility and nature of the mucoadhesive chains, mobility and contact time. According to the literature, the depth of interpenetration required to produce an efficient bioadhesive bond lies in the range 0.2 - 0.5 μm. This interpenetration depth of polymer and mucin chains can be estimated by the following equation:
l = (tDb)½
Where t is the contact time and Db is the diffusion coefficient of the mucoadhesive material in the mucus. The adhesion strength for a polymer is reached when the depth of penetration is approximately equivalent to the polymer chain size. In order for diffusion to occur, it is important that the components involved have good mutual solubility, that is, both the bioadhesive and the mucus have similar chemical structures. The greater the structural similarity, the better is the mucoadhesive bond.
Fracture Theory
This is perhaps the most used theory in studies on the mechanical measurement of mucoadhesion. It analyzes the force required to separate two surfaces after adhesion is established. This force, sm, is frequently calculated in tests of resistance to rupture by the ratio of the maximal detachment force, Fm, and the total surface area, A0, involved in the adhesive interaction
Sm= Fm/ A0
Since the fracture theory [Figure 3] is concerned only with the force required to separate the parts, it does not take into account the interpenetration or diffusion of polymer chains. Consequently, it is appropriate for use in the calculations for rigid or semi-rigid bioadhesive materials, in which the polymer chains do not penetrate into the mucus layer.

The Electronic Theory
This theory describes adhesion occurring by means of electron transfer between the mucus and the mucoadhesive system, arising through differences in their electronic structures. The electron transfer between the mucus and the mucoadhesive results in the formation of double layer of electrical charges at the mucus and mucoadhesive interface. The net result of such a process is the formation of attractive forces within this double layer.
The Adsorption Theory
In this instance, adhesion is the result of various surface interactions (primary and secondary bonding) between the adhesive polymer and mucus substrate. Primary bonds due to chemisorptions result in adhesion due to ionic, covalent and metallic bonding, which is generally undesirable due to their permanency.
Secondary bonds arise mainly due to van der Waals forces, hydrophobic interactions and hydrogen bonding. Whilst these interactions require less energy to “break”, they are the most prominent form of surface interaction in mucoadhesion processes as they have the advantage of being semi-permanent bonds.
Mechanical Theory
This theory considers the adhesion of mucoadhesive liquids systems (mucoadhesive liquids or particulate systems) which happens when the liquid fills the irregularities of a rough surface, since the adhesion is facilitated due to roughness on the substrate surface. These irregularities increase the area available to interact and improve the humectant characteristics. In this way, the mechanical theory has a close contact with the wetting theory, described previously, since both are adequate and complementary with regard to describing the adhesion of liquid systems. Moreover, with increased roughness there is higher viscoelasticity and plastic dissipation of the energy at the interface.
Factors Affecting Mucoadhesion
Mucoadhesion may be affected by a number of factors, including:
Hydrophilicity
Bioadhesive polymers possess numerous hydrophilic functional groups, such as hydroxyl and carboxyl. These groups allow hydrogen bonding with the substrate, swelling in aqueous media, thereby allowing maximal exposure of potential anchor sites. In addition, swollen polymers have the maximum distance between their chains leading to increased chain flexibility and efficient penetration of the substrate.
Molecular Weight
The interpenetration of polymer molecules is favored by low molecular-weight polymers, whereas entanglements are favored at higher molecular weights. The optimum molecular weight for the maximum mucoadhesion depends on the type of polymer, with bioadhesive forces increasing with the molecular weight of the polymer up to 100,000. Beyond this level, there is no further gain.
Cross-linking and Swelling
Cross-link density is inversely proportional to the degree of swelling. The lower the cross-link density, the higher the flexibility and hydration rate; the larger the surface area of the polymer, the better the mucoadhesion. To achieve a high degree of swelling, a lightly cross-linked polymer is favored. However, if too much moisture is present and the degree of swelling is too great, a slippy mucilage results and this can be easily removed from the substrate50. The mucoadhesion of cross-linked polymers can be enhanced by the inclusion in the formulation of adhesion promoters, such as free polymer chains and polymers grafted onto the preformed network.
Spatial Conformation
Besides molecular weight or chain length, spatial conformation of a polymer is also important. Despite a high molecular weight of 19,500,000 for dextrans, they have adhesive strength similar to that of polyethylene glycol (PEG), with a molecular weight of 200,000. The helical conformation of dextran may shield many adhesively active groups, primarily responsible for adhesion, unlike PEG polymers, which have a linear conformation.
pH
The pH at the bioadhesive to substrate interface can influence the adhesion of bioadhesives possessing ionizable groups. Many bioadhesives used in drug delivery are polyanions possessing carboxylic acid functionalities. If the local pH is above the pK of the polymer, it will be largely ionized; if the pH is below the pK of the polymer, it will be largely unionized. The approximate pKa for the poly(acrylic acid) family of polymers is between 4 and 5. The maximum adhesive strength of these polymers is observed around pH 4-5 and decreases gradually above a pH of 6. A systematic investigation of the mechanisms of mucoadhesion clearly showed that the protonated carboxyl groups, rather than the ionized carboxyl groups, react with mucin molecules, presumably by the simultaneous formation of numerous hydrogen bonds.
Concentration of Active Polymer
Ahuja stated that there is an optimum concentration of polymer corresponding to the best mucoadhesion. In highly concentrated systems, beyond the optimum concentration the adhesive strength drops significantly. In concentrated solutions, the coiled molecules become solvent-poor and the chains available for interpenetration are not numerous. This result seems to be of interest only for more or less liquid mucoadhesive formulations. It was shown by Duchêne55 that, for solid dosage forms such as tablets, the higher the polymer concentration, the stronger the mucoadhesion.
Drug/ Excipient Concentration
Drug/ excipient concentration may influence the mucoadhesion. Blanco Fuente studied the effect of propranolol hydrochloride to Carbopol (a lightly cross-linked poly(acrylic acid) polymer) hydrogels adhesion. Author demonstrated increased adhesion when water was limited in the system due to an increase in the elasticity, caused by the complex formation between drug and the polymer. While in the presence of large quantities of water, the complex precipitated out, leading to a slight decrease in the adhesive character.
Increasing toluidine blue O (TBO) concentration in mucoadhesive patches based on Gantrez (poly(methylvinylether/maleic acid) significantly increased mucoadhesion to porcine cheek tissue This was attributed to increased internal cohesion within the patches due to electrostatic interactions between the cationic drug and anionic copolymer.
Other factors affecting mucoadhesion
Mucoadhesion may be affected by the initial force of application. Higher forces lead to enhanced interpenetration and high bioadhesive strength59. In addition, the greater the initial contact time between bioadhesive and substrate, the greater the swelling and interpenetration of polymer Physiological variables can also affect mucoadhesion. The rate of mucus turnover can be affected by disease states and also by the presence of a bioadhesive device. In addition, the nature of the surface presented to the bioadhesive formulation canvary significantly depending on the body site and the presence of local or systemic disease.
Ideal properties of implantable devices:
Advantages of the implantable drug delivery system:
Disadvantages of implantable drug delivery system:
Mucoadhesive polymers
Different polymers have been explained by the researchers for the drug delivery. However, polymers having mucoadhesive nature should possess same specific characteristics and act as drug delivery system. An ideal mucoadhesive polymer has the following characteristics :
Effect of polymer properties on mucoadhesive drug delivery system
Different polymers exhibit different mucoadhesive properties depending on their physical and chemical strength. For example, a more flexible polymer exhibits higher degree of mucoadhesive property.
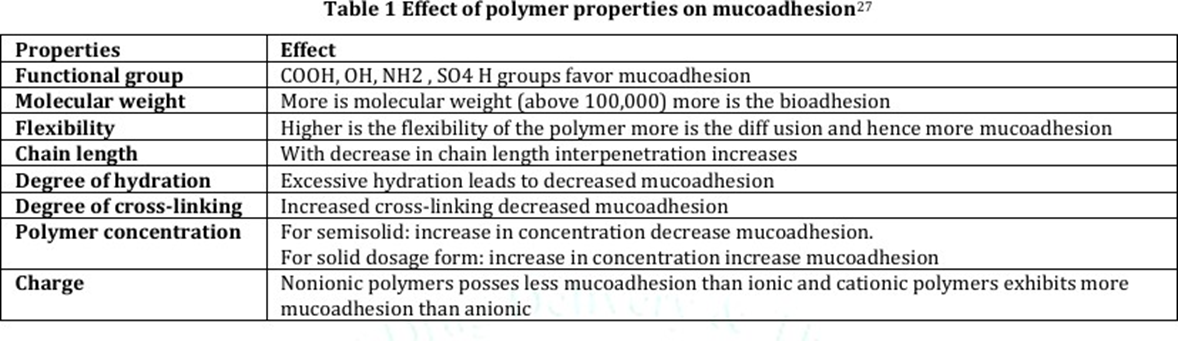
Mucoadhesive polymers possessing hydrophilic functional groups such as COOH, OH, NH2 and SO4H are more favorable candidates for the formulation of targeted drug delivery. These polymers bearing the desired functional group interact with mucus through physical entanglement as well as through chemical bonds resulting in formation of cross-linked network. For example, urea is a well-accepted hydrogen-bonding disruptor which decreases mucoadhesion of mucin/pectin samples. Other properties which may affect the mucoadhesive nature of the polymer include chain length, degree of hydration, degree of cross-linking, polymer concentration, charge, etc. (Table 1).
Polymers used for mucoadhesive drug delivery
The rheology of the mucoadhesion is a typical topic and it deals with a number of forces, factors of the components, state of the material and its derived properties. Different polymers and their mucoadhesive strength are listed in Table 2.

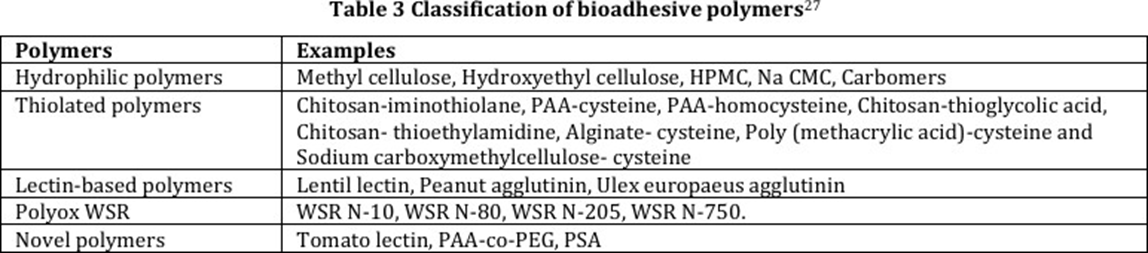
Based on the rheological aspects, we can categorize the mucoadhesive polymers into two broad categories: materials which undergo matrix formation or hydrogel formation by either a water swellable material or a water soluble material. These carriers are generally polymers and classified as given in Table 3.
Natural polymers
The polymers within this category are soluble in water. Matrices developed with these polymers swell when they come in contact an aqueous media with subsequent dissolution of the matrix. The polyelectrolytes widen greater mucoadhesive property such as. poloxamer, hydroxypropyl methyl cellulose, methyl cellulose, poly (vinyl alcohol) and poly (vinyl pyrrolidone), have been used for mucoadhesive properties. The natural polysaccharides and its derivatives like chitosan, methyl cellulose, hyaluronic acid, hydroxy propyl methylcellulose, hydroxy propyl cellulose, Xanthan gum, gellan gum, guar gum, and Carrageenan have been utilized in development of ocular drug delivery systems. Cellulose and its derivates have been reported to have surface active property in addition to its film forming capability. Cellulose derivatives with lower surface acting property are normally preferred in ocular delivery systems as they cause reduced eye irritation. Cationic cellulose derivatives (e.g. cationic hydroxyethyl celluloses) have been used in conjunction with various anionic polymers for the development of sustained delivery systems.
List of Natural Polymers
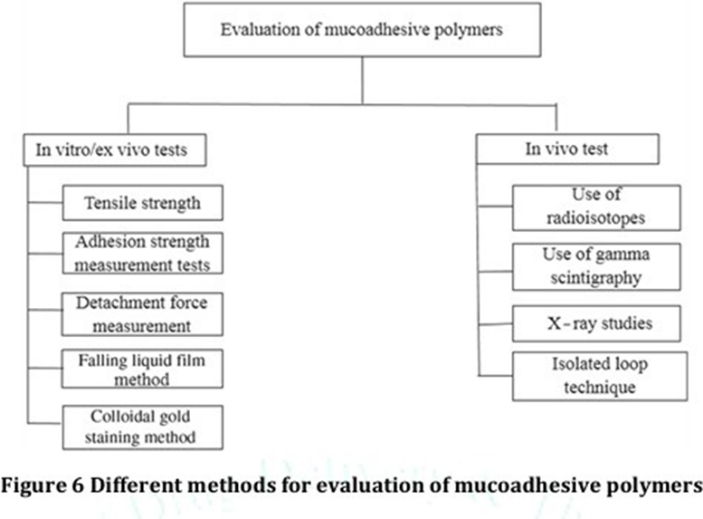
Evaluation of mucoadhesive drug delivery systems
Mucoadhesive drug delivery systems can be evaluated by testing their adhesion strength. Various in vitro and in vivo tests (Figure 4) are available to determine the adhesion strength of the mucoadhesive polymers.
Applications of mucoadhesive implants in modern treatments :
Periodontitis Management – Local delivery of antimicrobials (e.g., doxycycline, metronidazole, chlorhexidine) through biodegradable mucoadhesive implants placed in periodontal pockets for sustained infection control.
Peri-implantitis Therapy – Mucoadhesive silver nanoparticle-based implants provide long-lasting antimicrobial action against peri-implant pathogens around dental implants.
Post-surgical Oral Care – Mucoadhesive antibiotic implants prevent microbial colonisation and reduce inflammation following oral surgeries or extractions.
Oral Cancer Treatment – Localised delivery of chemotherapeutics (e.g., 5-FU, cisplatin) using mucoadhesive implants reduces systemic toxicity and improves drug concentration at tumour sites.
Chronic Pain Relief – Buccal mucoadhesive fentanyl implants provide controlled systemic analgesia in cancer-related or neuropathic pain.
Nicotine Replacement Therapy – Nicotine-loaded buccal mucoadhesive implants help in smoking cessation by offering sustained drug release and reducing withdrawal symptoms.
Hormone Replacement – Vaginal mucoadhesive implants for progesterone or oestrogen support infertility treatment and hormone deficiencies with prolonged release.
HIV Prevention – Vaginal or rectal mucoadhesive implants delivering antiretrovirals (e.g., tenofovir) provide localised protection and reduce systemic exposure.
Contraception – Vaginal mucoadhesive implants designed for long-term release of hormones like levonorgestrel act as non-invasive contraceptives.
Glaucoma Therapy – Ocular mucoadhesive inserts containing pilocarpine or timolol offer prolonged reduction of intraocular pressure compared to eye drops.
Ocular Infections – Antibiotic-loaded mucoadhesive ocular implants enhance residence time in conjunctival sac, improving treatment efficacy for conjunctivitis or keratitis.
Diabetes Management – Experimental buccal mucoadhesive insulin implants deliver peptides via mucosal absorption, bypassing enzymatic degradation in the gut.
Peptide and Protein Delivery – Mucoadhesive implants with stabilised formulations of peptides (e.g., calcitonin, vaccines) offer systemic delivery through mucosal tissues.
Wound Healing – Mucoadhesive implants incorporating growth factors or phytochemicals (e.g., EGCG) promote gingival or mucosal regeneration.
Local Antifungal Therapy – Mucoadhesive implants releasing antifungals like clotrimazole or nystatin are used in chronic oral or vaginal candidiasis.
Anti-inflammatory Therapy – Implants loaded with NSAIDs or corticosteroids reduce local inflammation in oral mucosal lesions or post-surgical conditions.
Targeted Periodontal Bone Regeneration – Mucoadhesive implants with bone morphogenetic proteins (BMPs) stimulate alveolar bone regeneration in periodontal defects.
CONCLUSION
Today, drug delivery systems designed with the aim to improve patient compliance and convenience is more important than ever. Therefore, huge work is going on to develop novel dosage forms to satisfy increased patient demands of more convenient dosage forms. This overview about the mucoadhesive dosage forms might be a useful tool for the efficient design of novel mucoadhesive drug delivery systems. Mucoadhesive drug delivery systems have applications from different angles, including development of novel mucoadhesive, design of the device, mechanisms of mucoadhesion and permeation enhancement. With the influx of a large number of new drug molecules due to drug discovery, mucoadhesive drug delivery will play an even more important role in delivering these molecules. The mucoadhesive dosage forms offer prolonged contact at the site of administration, low enzymatic activity, and patient compliance. However, these novel mucoadhesive formulations require much more work, to deliver clinically for the treatment of both topical and systemic diseases.
REFERENCES




Swaraj Barne, Swarup Dhore, Yashad Chavan, Yashodeep Gore, A Clinical Perspective on Mucoadhesive Implants, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 3407-3418. https://doi.org/10.5281/zenodo.17226417
 10.5281/zenodo.17226417
10.5281/zenodo.17226417
