Department of Pharmaceutics, Bharathi College of Pharmacy, Bharathinagara, Mandya, Karnataka-571422, India.
Oral drug delivery is the most preferred route due to its convenience and patient compliance; however, it faces significant limitations such as enzymatic degradation, first-pass metabolism, gastrointestinal toxicity, and short gastric residence time (GRT), particularly for drugs absorbed in the upper gastrointestinal tract. Gastro-retentive drug delivery systems (GRDDS) have emerged as an effective strategy to overcome these challenges by prolonging gastric retention and enabling controlled, site-specific drug release. Among GRDDS, mucoadhesive in-situ gelling systems offer notable advantages by transforming from a liquid to a gel under physiological conditions, thereby enhancing gastric residence time, bioavailability, and therapeutic efficacy. These systems utilize natural or synthetic polymers that adhere to the gastric mucosa and provide sustained drug release while minimizing dosing frequency and systemic side effects. This review highlights the need, mechanisms, polymers, approaches, applications, and evaluation parameters of mucoadhesive in situ gelling systems as promising platforms for advanced gastro-retentive drug delivery.
Oral delivery of drug molecules is generally preferred when compared to other administration routes; however, it has certain limitations, including primary hepatic metabolism, drug degradation by alimentary canal enzymes, and GI toxicity, which limits oral administration of some drugs, mainly proteins and peptides.[1]
There are several drawbacks to the fact that most pharmaceutical dose forms are designed for quick release. For instance, medications with short half-lives require frequent administration, patient compliance is poor, and adverse effects from drug level variations are more likely, particularly for medications with small therapeutic indices.
Numerous technological advancements have increased the capacity to administer medications in a controlled manner, potentially updating drug therapy. offer several therapeutic benefits and solve the short comings of traditional medication delivery techniques.[2] Limited gastric residence times (GRTs) restrict the oral sustained medication delivery strategy. Since most medications are absorbed in the stomach or upper portion of the small intestine, rapid GI transit can impede full drug release in the absorption zone and lower the effectiveness of the prescribed dose. [3,4]
GASTROINTESTINAL TRACT
Conventional drug delivery methods may encounter issues in the gastrointestinal tract (GIT), such as insufficient drug release, diminished dose efficacy, and frequent dose requirements. Consequently, novel drug delivery methods such as the GRDDS could be created as a due to the incapacity of conventional drug delivery methods to retain drugs in the stomach.
The ability to target distribution in the stomach, enhance drug absorption, and prolong the gastric residence time (GRT) of dose forms in the stomach for several hours are only a few benefits offered by these systems. [5,6]
FACTORS AFFECTING GASTRIC RETENTION
The gastric retention time (GRT) of dosage formulations is influenced by a number of factors. which might delay intestinal transit and gastric emptying. These include the size and density of the dose form, the fed and fasting stomach, and food elements like fat, certain amino acids, and peptides. Position, posture, age, sex, sleep patterns, and health conditions (such as diabetes or gastrointestinal disorders) can all influence motor activity and shorten transit times.[7]
ADVANTAGES
NEED OF GRDSS
PHYSIOLOGY OF STOMACH
Since the stomach is a key component of the GRDDS, developing a good gastro-retentive dose form requires a deep understanding of stomach physiology and anatomy. The stomach is separated anatomically into two sections: the proximal stomach, which is made up of the body and fundus, and the distal stomach, which is made up of the pylorus and the antrum, as seen in the figure below. The main job of the stomach is to crush and temporarily store food before releasing it into the duodenum. The antrum acts as a pump to move food into the stomach, whereas the fundus and body primarily act as storage spaces for undigested food.The migrating myoelectric complex (MMC) is the term used to describe the movement pattern of the stomach. Both fed and fasting states experience gastric emptying, although the patterns are very different. When fasting, an internal digestive Every 90 to 120 minutes, a series of electrical events passes through the small intestine and stomach.
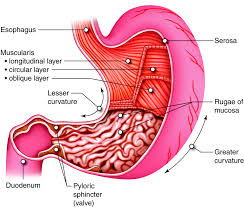
Fig. no. 1: Physiology of Stomach
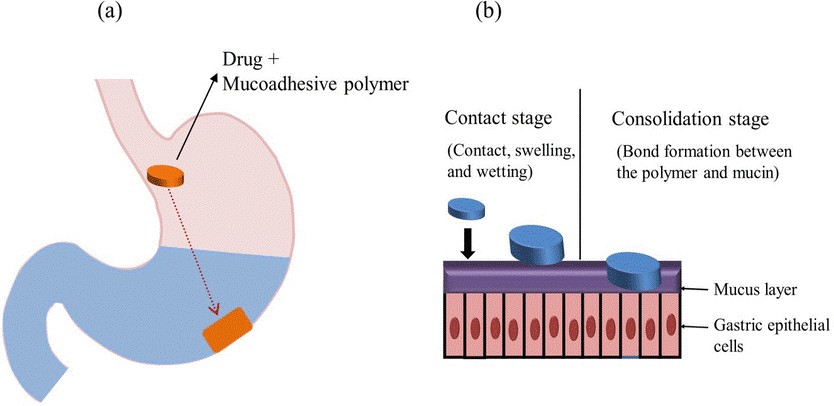
The mucoadhesive/bio-adhesive system was designed to adhere to the gastric epithelial cell surface and prolong the GRT of drug compounds. In this approach, drugs are incorporated into a mucoadhesive agent, which can be natural or synthetic polymers. The bond formed between the polymer and the mucosal surface enhances the mucoadhesion process, which typically consists of two steps.
(a) Contact stage
(b) Consolidation stage.
Carbopol, chitosan, sodium alginate, HPMC, polyethylene glycol, and polyacrylic acid are some of the most often used mucoadhesive polymers. Mucoadhesive polymers help to bind pharmacological compounds to mucosal surfaces, increasing drug residence time at the application site.[11]
MUCOADHESION
Bio-adhesion is a phenomenon in which two materials at least one of which is biological in nature are held together by means of interfacial forces. The term ‘mucoadhesion’ is defined as the adhesion of the polymers with the surface of the mucosal layer.
MUCUS MEMBRANE
Mucus membranes are the moist surfaces lining walls of various body cavities such as the gastrointestinal and respiratory tracts.Mucus is secreted by the goblet cells. Mucus is present either as a gel layer adherent to the mucosal surface or in suspended form or as a luminal soluble. The major components of all mucus gels are mucin glycoprotein, water, lipids, and inorganic salts. The mucus serves as a protective barrier and for lubrication also.[12]
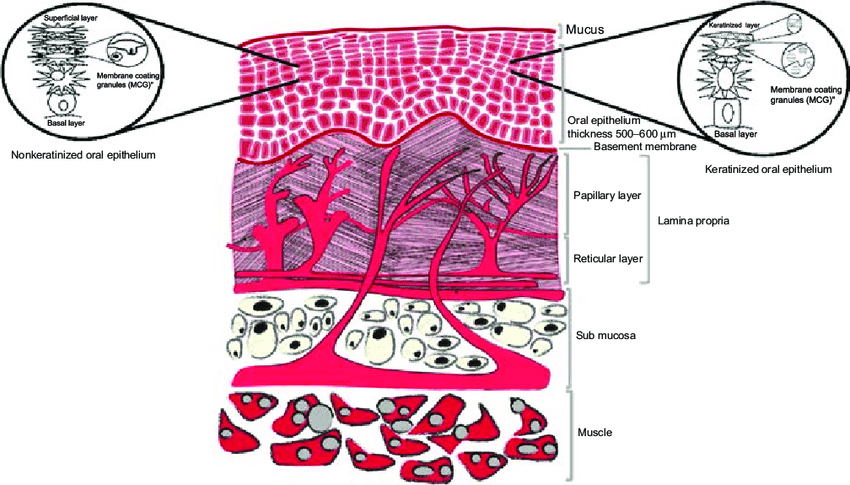
Fig.no.3 Mucus Membrane.
FUNCTION OF MUCUS LAYER
The primary functions of the mucus layer are.
MECHANISM OF MUCOADHESION
The mechanism of muco-adhesion is generally divided in two steps,
Essentially, there are two theories explaining the consolidation step
1. The diffusion theory. 2. The dehydration theory.
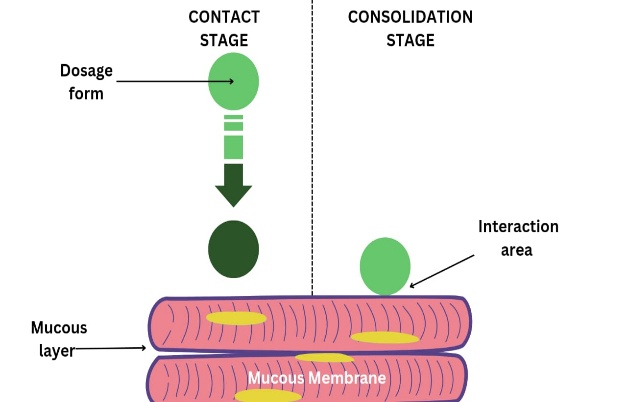
Fig. no. 4: Stages of Muco-adhesion
According to diffusion theory, the mucoadhesive molecules and the glycoproteins of the mucus mutually interact with each other by means of interpenetration of their chains and the building of secondary bonds. For this to take place the mucoadhesive device has features favoring both chemical and mechanical interactions.
According to dehydration theory, materials that may quickly jellify in an aqueous environment, when placed in touch with mucus, might cause its dehydration due to the difference in osmotic pressure.[14]
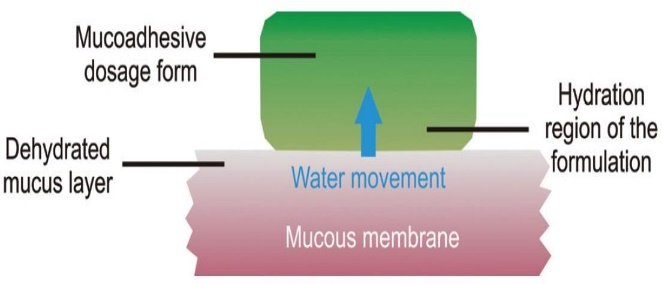
Fig.no.5: Mechanism of Mucus Membrane
THEORIES OF MUCO-ADHESION
Different theories are involved in the muco-adhesion which are as follows
According to this theory an electrical double layer is formed on the transfer of the electrons among the mucoadhesive and mucosal membrane.
This theory is applicable for liquids, postulates that the lower the contact angle of liquid on substrate surface there will be greater affinity for adhesion.
According to this idea, the mucoadhesive is adsorbed on the mucosal surface due to intermolecular forces such hydrogen bonds and Vander Waal's forces.
This theory illustrates the forming of a network structure among the mucoadhesive and the mucosal surface by diffusion of the polymer’s chains present on the mucoadhesive surface.
Explains the production of an interlocking structure by the diffusion of liquid adhesives into the micro-cracks and imperfections present on the mucoadhesive substrate, which results in muco-adhesion.
This theory states that like-molecule interactions are the primary cause of the muco-adhesion phenomenon.[15]
IN-SITU GEL
The term "in-situ gel" describes a polymer solution that, when exposed to a physiological environment, changes from a liquid to a semisolid gel. Temperature, pH changes, ionic changes, UV-induced gelation, and solvent exchange-induced gelation can all cause the gelation.[16]In-situ gel systems are liquid formulations that undergo sol–gel transition upon exposure to physiological conditions such as pH, temperature, or ionic strength. The incorporation of mucoadhesive polymers into these formulations enables the system to adhere to mucosal surfaces, thereby enhancing the residence time and bioavailability of the drug. Upon administration, the system transforms into a gel that remains at the site of application, providing sustained and controlled drug release.[17]This innovative drug delivery system supports the crucial ease and convenience of administration, delivery of an exact dose, and prolongation of the residence period of the drug in contact with mucosa, which are issues often present in semi-solid dosage forms. One or more combinations of several stimuli, such as pH change, temperature modulation, and solvent exchange, result in in situ gel formation.[18]
ADVANTAGES
Administered as a liquid (sol), which is easy to swallow and convenient for patients.
Converts from sol to gel in response to pH, temperature, or ions, ensuring localized drug retention.
Mucoadhesive and/or gel nature helps the formulation stay longer in the stomach.
Gel matrix slows drug diffusion, maintaining therapeutic drug levels for longer periods.
Particularly useful for drugs absorbed mainly in the upper GIT or unstable at intestinal pH
Sustained release minimizes frequent dosing, improving patient compliance.
Polymers like HPMC, sodium alginate, Carbopol adhere to gastric mucosa, enhancing contact time.
Localized gel formation protects the drug from rapid gastric emptying and degradation.
Drug is evenly dispersed within the gel, reducing dose dumping.
Controlled release lowers peak plasma concentrations.
Suitable for oral, ocular, nasal, buccal, vaginal, and rectal drug deliver.[19]
POLYMERS USED IN INSITU GELLING SYSTEM
1.Natural polymer
2.Syntheic polymer
1. Natural polymer
2. Syntheic polymer
APPROCHES
1. In-situ gel formation due to physiological stimuli:
a) Temperature triggered in-situ gel systems
b) pH triggered in situ gelling systems
2. In-situ gel formation due to ion-activated system
3. In-situ gel formation due to physical mechanism
a) Swelling
b) Diffusion
4. In-situ gel formation due to chemical reactions
a) Ionic cross-linking
b) Enzymatically cross linking
c) Photo-polymerization [21]
1. IN SITU GEL FORMATION DUE TO PHYSIOLOGICAL STIMULI:
A. PH TRIGGERED SYSTEMS:
Variations in pH can also trigger in-situ gel formation in response to physiological conditions. pH-sensitive polymers contain pendant acidic or basic functional groups that respond to changes in the surrounding pH by accepting or releasing protons. Polymers with a high density of ionizable groups are known as polyelectrolytes. In polymers containing weakly acidic (anionic) groups, hydrogel swelling increases as the external pH rises, whereas polymers with weakly basic (cationic) groups show reduced swelling with increasing pH.Most anionic pH-sensitive polymers are based on polyacrylic acid (PAA), such as Carbopol® or carbomers and their derivatives. Similarly, low-viscosity solutions of polyvinylacetal diethylaminoacetate (AEA) at pH 4 can form hydrogels under neutral pH conditions. Combinations of poly(methacrylic acid) (PMA) and poly(ethylene glycol) (PEG) have also been used as pH-responsive systems to achieve gelation.[22]
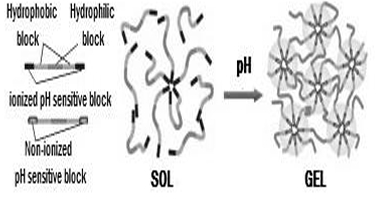
Fig.no.6: Mechanism of pH triggered in situ gel system
B. TEMPERATURE TRIGGERD SYSTEM:
Temperature is the most widely used stimulus in environmentally responsive polymer systems for in-situ gelling formulations because temperature changes are easy to control and can be applied both in vitro and in vivo. In this approach, gelation is triggered by body temperature, eliminating the need for any external heat source. These hydrogels remain in a liquid state at room temperature (20–25 °C) but undergo gelation upon contact with physiological fluids at body temperature (35–37 °C).Temperature-responsive systems are generally classified into three categories and may exhibit either positive or negative thermosensitivity, as seen with polymers such as poly(N-isopropylacrylamide). Common examples of thermoreversible polymers include poloxamers (Pluronics) and tetronics. This technology relies on thermoresponsive polymers that display a sharp and reversible change in physical properties in response to temperature variations. Certain polymers possess an upper or lower critical solution temperature (UCST or LCST), beyond which a miscibility gap appears at either high or low temperatures, leading to gel formation.[23]
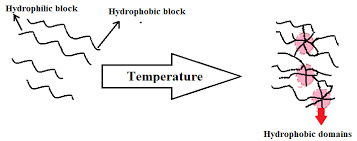
Fig.no.7: Mechanism of temperature triggered system
2. ION ACTIVATED SYSTEM:
In this method, gelling of the solution instilled is triggered by change in the ionic strength. It is assumed that the rate of gelation depend on the osmotic gradient across the surface of the gel. The polymer which shows osmotically induced gelation is Gelrite or Gellan gum, Hyaluronic acid and Alginates etc.[24]
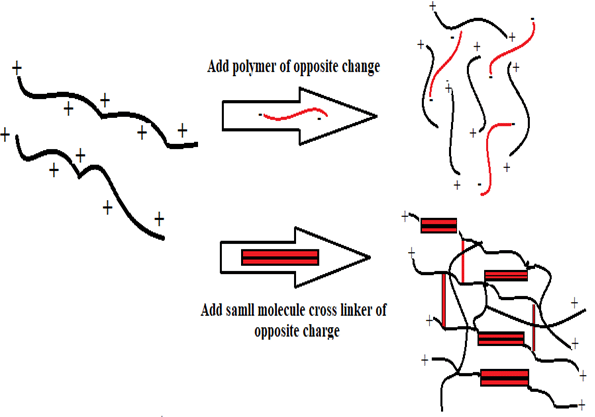
Fig.no.8: Mechanism of temperature triggered system
3. IN SITU GEL FORMATION DUE TO PHYSICAL MECHANISM
A. SWELLING:
In situ formation can also take place when a material absorbs water from the surrounding environment and expands to occupy the desired space. One such material is Myverol® 18-99 (glycerol mono-oleate), a polar lipid that swells in the presence of water to form lyotropic liquid crystalline phase structures. It also exhibits bioadhesive properties and can be degraded in vivo through enzymatic action.
B. DIFFUSION:
This technique is based on the diffusion of solvent from a polymer solution into the surrounding tissue, which leads to precipitation or solidification of the polymer matrix. N-methyl pyrrolidone (NMP) has been demonstrated to be an effective solvent for use in such systems.[25]
4. IN SITU GEL FORMATION DUE TO CHEMICAL REACTIONS
A. IONIC CROSS-LINKING:
Polymers may undergo phase transition in presence of various ions. Some of the polysaccharides fall into the class of ion-sensitive ones. Gelrite (Gellan gum), pectin, sodium alginate, and carrageenan are typical examples of ion pH sensitive poly saccharides. They form a gel in the presence of divalent or polyvalent cations. such as Ca2+, Mg2+ and Na2+. For example, alginic acid gels in the presence of Ca2+.[26]Gellan gum commercially available as Gelrite® is an anionic polysaccharide that undergoes in-situ gelling in the presence of mono- and divalent cations, including Ca2+, Mg2+, K+ and Na+. Gelation of the low-methoxy pectins can be caused by divalent cations, especially Ca2+. Likewise, alginic acid undergoes gelation in presence of divalent/polyvalent cations e. g. Ca2+ due to the interaction with glucuronic acid block in alginate chains.[27]
B. ENZYMATICALLY CROSS LINKING:
C. PHOTO-POLYMERIZATION:
Biomaterials are often formed in situ through photopolymerization. In this approach, a solution containing monomers or reactive macromers along with an initiator is injected into the tissue, followed by exposure to electromagnetic radiation to induce gel formation. Acrylate or similar polymerizable functional groups are commonly used on monomers and macromers because they readily undergo photopolymerization in the presence of a suitable photo-initiator. Typically, long-wavelength radiation in the visible or ultraviolet range is employed, while short-wavelength UV is rarely used due to its biological hazards and limited tissue penetration.When photopolymerizable systems are injected at the target site, they can be photo-cured in situ using fiber-optic cables, enabling prolonged drug release. These photoreactions allow rapid polymerization at physiological temperatures. Additionally, such systems can be easily adapted to complex anatomical shapes, resulting in effective implant formation.[29]
APPLICABILITY OF IN SITU POLYMERIC DRUG DELIVERY SYSTEM:-
1. ORAL DRUG DELIVERY SYSTEM:
pH-sensitive hydrogels can be utilized to deliver drugs to specific regions of the gastrointestinal tract. Hydrogels prepared from varying ratios of polyacrylic acid (PAA) derivatives and cross-linked polyethylene glycol (PEG) enabled the formation of silicone microspheres that either exhibited gastroprotective effects or released prednisolone in gastric media. To develop a potential colon-targeted drug delivery system, cross-linked dextran hydrogels that swell more rapidly at higher pH levels were investigated, along with other polysaccharides such as amidated pectins, guar gum, and inulin. Sodium alginate and Gellan gum formulations contain complexed calcium ions that are liberated in the acidic environment of the stomach, triggering gel formation. Oral delivery of paracetamol using in-situ gel systems has been extensively studied. Natural polymers such as pectin, xyloglucan, and Gellan gum are commonly employed in oral in-situ gel formulations. Sustained-release paracetamol delivery using pectin-based formulations has been reported, with the key advantage of pectin being its water solubility, which eliminates the need for organic solvents.[30]
2. OCULAR DRUG DELIVERY SYSTEM:
Natural polymers such as xyloglucan, Gellan gum, and alginic acid are commonly utilized inocular drug delivery systems. Local ophthalmic formulations used to reduce intraocular pressure in glaucoma include a wide range of agents, such as antimicrobials, anti-inflammatory drugs, and autonomic medications. However, enhanced tear secretion and ocular movement lead to rapid drug elimination from the eye, resulting in poor drug retention. Consequently, conventional delivery systems often exhibit limited therapeutic effectiveness and low bioavailability. Viscosity-enhancing agents such as hydroxypropyl methylcellulose, carboxymethyl cellulose, carbomers, and polyvinyl derivatives are incorporated into formulations to address this issue. Alcohol is added to increase viscosity, thereby improving bioavailability and extending precorneal residence time. In addition, preservatives, chelating agents, and surfactants are included to enhance drug penetration into ocular tissues.[31]
3. NASAL DRUG DELIVERY SYSTEM:
Gellan and xanthan gums are used as in situ gel-forming polymers in nasal in situ gel. The therapeutic efficacy of mometasone furoate for the treatment of allergic rhinitis was evaluated using an animal model of allergic rhinitis. In antigen-sensitised rats, the effect of the in-situ gel on antigen-induced nasal symptoms was investigated. Compared with the marketed preparation Nasonex® (mometasone furoate nasal solution 0.05%), the in-situ gel was shown to significantly inhibit the increase in nasal symptoms.[32]
4. RECTAL DRUG DELIVERY SYSTEM:
In-situ gel systems are widely valued for rectal drug delivery. They are capable of administering medications in liquid form, semisolid preparations such as ointments, creams, and foams, as well as solid dosage forms like suppositories. Traditionally, the use of suppositories has often been linked to discomfort. Moreover, suppositories tend to migrate upward into the colon, making it difficult for them to remain in the rectum and thereby exposing the drug to first-pass metabolism. Choi and co-workers reported the development of a liquid suppository with a gelation temperature ranging from 30 °C to 36 °C, where temperature-dependent gel formation was achieved through the incorporation of Poloxamer 407 and Poloxamer 188.[33]
5. VAGINAL DRUG DELIVERY SYSTEM:
Medications may also be delivered through the vaginal route, which is part of the reproductive system. Thermoplastic graft copolymer–based formulations that undergo in-situ gelation have been developed to provide sustained release of active agents such as progestins, oestrogens, peptides, proteins, and nonoxynol-9 over prolonged periods. In a recent study, a mucoadhesive, thermosensitive gel composed of poloxamers and polycarbophil showed enhanced and longer-lasting clotrimazole effectiveness in fungal infections when compared with conventional PEG-based dosage forms.[34]
6. INJECTABLE DRUG DELIVERY SYSTEM:
In this drug delivery approach, formulations are designed as injectable in-situ gels, which have gained considerable attention over the past decade because they do not require surgical intervention and offer improved patient compliance. Injectable in-situ gels are predominantly formulated using synthetic polymers and block copolymers. An example is the anti-inflammatory drug bupivacaine, which has been developed as an injectable in-situ gel using polymers such as poly(D,L-lactide), poly(D,L-lactide-co-glycolide), and PLGA. These polymer-based gel systems exhibit prolonged drug action under gelled conditions.[35]
7. DERMAL AND TRANSEDERMAL DRUG DELIVERY:
Indomethacin has been delivered percutaneously using a thermoreversible Pluronic F127 gel. In vivo studies indicated that a 20% w/w aqueous gel could serve as an effective base for the topical administration of the drug. Poloxamer 407 gel was also found to be suitable for transdermal delivery of insulin. Furthermore, the combined use of iontophoresis and chemical penetration enhancers produced a synergistic effect, significantly improving insulin permeation through the skin.[36]
EVALUATION AND CHARACTERIZATION OF IN-SITU GELLING SYSTEM:
In-situ gel evaluated & characterized by the following parameters-
1. CLARITY:
The Clarity of formulated solution is determined by visual inspection under black and white background.
2. TEXTURE ANALYSIS:
The firmness, consistency and cohesiveness of hydrogels are assessed using texture analyzer which mainly indicates the syringeability of sol so the formulation can be easily administered in vivo. Higher values of adhesiveness of gels are needed to maintain an intimate contact with surface-like tissues.
3. pH OF GEL:
pH can be determined formulation is taken in beaker & 1ml NaOH added drop wise with continuous stirring. pH is checked by using pH meter.
4. GELLING CAPACITY:
This parameter can be evaluated using a rheometer. Depending on the mechanism of the gelling of gelling agent used, a specified amount of gel is prepared in a beaker, from the sol form. This gel containing beaker is raised at a certain rate, so pushing a probe slowly through the gel. The changes in the load on the probe can be measured as a function of depth of immersion of the probe below the gel surface.
5. RHEOLOGICAL STUDIES:
This is a crucial factor that needs to be assessed for the in-situ gels. The Brookfield rheometer or other viscometers, such Ostwald's viscometer, can be used to measure the viscosity and rheological characteristics of in situ forming drug delivery systems. These formulations' viscosity should be such that the patient has no trouble administering them, particularly when administering them parenterally or intraocularly. Viscosity in the formulation should be between 5 and 1000 mPas.
6. SOL-GEL TRANSITION TEMPERATURE AND GELLING TIME:
For in situ gel forming systems incorporating thermoreversible polymers, the sol-gel transition temperature may be defined as that temperature at which the phase transition of sol meniscus is first noted when kept in a sample tube at a specific temperature and then heated at a specified rate. Gel formation is indicated by a lack of movement of meniscus on tilting the tube. Gelling time is the time for first detection of gelation as defined above.
7. FOURIER TRANSFORMER INFRA RED:
The possibility of drug excipient interaction is investigated by FTIR studies. The FTIR graph of pure drug & combination of drug with excipient are recorded by using KBR pellets.
8. THERMAL ANALYSIS:
Thermo gravimetric analysis can be conducted for in situ forming polymeric system to quantitative the percentage of water in hydrogel. Different scanning calorimetry is used to observed, if there are many changes in thermograms as compared with pure ingredients used thus indicating the interaction.
In this parameter 10 ml of in-situ formulation was added into the 900 ml dissolution vessel containing 0.1N HCl at 37?. The time taken by the formulation to emerge on medium surface (floating lag time) and the time formulation constantly floated on surface of dissolution medium (duration of floating).
10. IN VITRO FLOATING DURATION:
The invitro floating study was carried out by introducing 10ml of formulation into beaker containing 100ml of 0.1N HCl, pH (1.2) at 37? without much disturbance. The time formulation took emerge on the medium surface (floating lag time) and time of formulation constantly floated on the surface of the dissolution medium (duration of floating) were recorded. [37]
11. IN VITRO DRUG RELEASE:
The dissolution studies were performed in triplicate using a type II (paddle method) dissolution apparatus. The dissolution medium used was 900 ml of 0.1 N HCl (pH 1.2), maintained at 37 ºC. The stirring rate was adjusted to 50 rpm. This speed was believed to simulate the in vivo existing mild agitation and was slow enough to avoid the breaking of gelled formulation. At predetermined time intervals, 10 ml samples were withdrawn and replaced by fresh dissolution medium, filtered through Whatman filter paper, diluted, and assayed at maximum absorbance at 278 nm using UV-Visible Spectrophotometer. [38]
12. MUCOSHESION STUDY:
Mucoadhesion study was carried out using modified mucoadhesion apparatus. There was two glass slides, bottom slide was fixed with wooden base while upper slide was attached to nylon thread, and the other end of nylon thread was attached to plastic bowl. Here the weight of glass slide and plastic bowl was equal. Sheep or chicken stomach mucosa was fixed on both glass slides using gum. 1 gm of gel was placed between two slide and put 1 kg weight for removal of air for 5 min. Water was continuously added to plastic bowl till the two slides were just detached. Measure the quantity of water required and mucoadhesive strength was calculated.[39]
13. ACCELERATED STABILITY STUDIES:
The formulation is filled into amber-colored vials and sealed with aluminium foil in compliance with International Conference on Harmonisation (ICH) guidelines for short-term accelerated stability testing at 40 °C and 75% relative humidity. Samples are evaluated monthly for clarity, pH, and gelling capacity, along with in vitro dissolution, rheological properties, and drug content.[40]
CONCLUSION
Novel drug delivery systems have gained significant attention in recent years within modern pharmaceutical formulation research. Mucoadhesive in-situ gels have emerged as a promising approach for site-specific drug delivery in a controlled or sustained manner. By retaining the drug at the target site for an extended period, these systems enhance drug absorption and consequently improve bioavailability. Therefore, mucoadhesive in-situ gels are expected to continue playing an important role in the future development of pharmaceutical products, supported by the use of advanced materials and innovative technologies.
REFERENCES



Mohammad Ali., Kishor S.*, Parthiban S., A Comprehensive Review on Mucoadhesive In-Situ Gel Drug Delivery SystemsInt. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 111-125. https://doi.org/10.5281/zenodo.18454135
 10.5281/zenodo.18454135
10.5281/zenodo.18454135
