Govindrao Nikam College of Pharmacy, Sawarde
Diabetes Mellitus (DM) is a rapidly escalating global health crisis affecting hundreds of millions, requiring complex, self-managed care that is highly susceptible in response. This project provides a comprehensive overview of the current landscape of antidiabetes disease management, focusing specifically on the critical interplay between therapeutic efficacy and the inevitability of human-centric failures. While significant research effort is directed toward novel pharmacotherapies (e.g., GLP-1 agonists, SGLT2 inhibitors), the realized effectiveness of these treatments is often dramatically reduced by errors in prescription, patient adherence, self-monitoring, and device use (e.g., insulin pens and pumps). This review synthesizes current knowledge on the most frequent and impactful categories of human error including slips, lapses, and mistakes within the context of DM care. Ultimately, this project establishes a critical need for a paradigm shift in diabetes research, arguing that future antidiabetes strategies must move beyond solely targeting biological pathways to incorporate human-factors engineering and error-reduction design to create more robust, safer, and inherently user-friendly management systems.
Diabetes Mellitus, often called just Diabetes, is a long-lasting health problem where blood sugar levels stay high because the body either doesn't produce enough insulin, can't use insulin properly, or a combination of both. It's a complex disease with different forms, causes, and health risks, making it a major health issue worldwide. Research on how to treat diabetes is getting more attention because the number of people with diabetes is increasing every year. By 2030, it's expected that there will be around 439 million adults with the condition. As awareness about the problem grows, researchers are finding lots of new medicines and also natural products from herbal plants to help manage it. Because of that, a study has been done on plant extracts that have anti-diabetes properties. The study looks at where these plants are found around the world, which parts of the plants contain the healing ingredients, and also how these parts work to help treat diabetes.[1] Diabetes mellitus is a kind of metabolic problem that affects the endocrine system. [2]
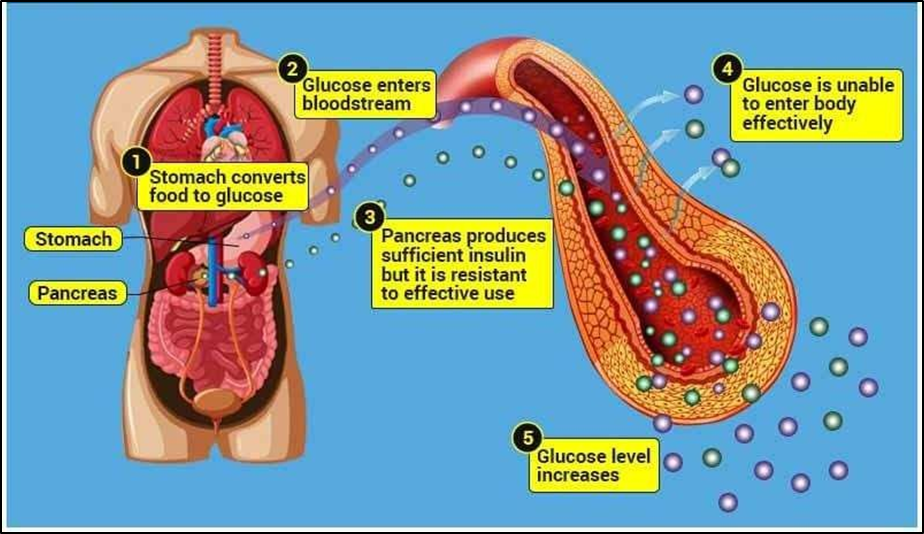
Fig No:1 Increase in the Glucose level.
Defects in insulin action, secretion, or both can lead to persistent hyperglycemia, which is a hallmark of diabetes mellitus (DM), a chronic metabolic disease.[3] A severe public health and socioeconomic burden, it is one of the most prevalent non-communicable illnesses in the world, impacting hundreds of millions of people.[4] The illness results from the body's incapacity to use insulin efficiently at target tissues, including muscle, adipose tissue, and the liver, or to manufacture enough of it from pancreatic β-cells.[5] The two main types of diabetes are Type 1 Diabetes Mellitus (T1DM), which is caused by the autoimmune destruction of β-cells, and Type 2 Diabetes Mellitus (T2DM), which is characterised by relative insulin insufficiency and insulin resistance.[6] Pregnancy-related Gestational Diabetes Mellitus (GDM) raises the chance of developing type 2 diabetes in later life.[7] Furthermore, secondary diabetes brought on by pancreatic or endocrine diseases and monogenic diabetes are further distinct types.[8]Over the past few decades, urbanisation, sedentary lifestyles, and rising obesity rates have all contributed significantly to the sharp increase in the prevalence of diabetes.[9]Diabetes-related chronic hyperglycemia is linked to long- term harm, malfunction, and failure of many organs, particularly the heart, blood vessels, kidneys, eyes, and nerves.[10] Effective management techniques, lifestyle changes, and early diagnosis are crucial for preventing problems and enhancing the lives of those who are impacted.[11] The exact cause of diabetes isn't fully understood, but it seems that both genetic factors and environmental ones like obesity and not getting enough exercise are involved. According to the World Health Organization, the number of people with diabetes is expected to rise to over 300 million by the year 2025.Right now, treatments for diabetes include insulin and different kinds of pills like sulfonylureas, biguanides, alpha-glucosidase inhibitors, and glinides. These can be used alone or together to try to keep blood sugar levels in check. But, a lot of these medicines can cause serious side effects, so managing diabetes without any side effects is still pretty tough.
People have been trying to find better and safer medicines to lower blood sugar for a while now. The drugs that work best to control blood sugar after meals include insulin lispro, amylin analogues, and alpha- glucosidase inhibitors. In cases where high blood sugar is linked to diabetes, some reports say that aldose reductase inhibitors might be used as a treatment. Aldose reductase is an important enzyme in the polyol pathway, and it helps convert glucose into sorbitol. Sorbitol doesn’t easily pass through cell membranes, so it tends to build up inside cells. This build-up of sorbitol inside cells has been linked to long-term problems of diabetes, like nerve damage (neuropathy), eye issues (retinopathy), and cataracts. The blood sugar-lowering effects of various plants used as natural remedies for diabetes have been confirmed, and scientists are currently studying how these plants actually work to lower blood sugar. Recently, two reviews about the chemical makeup of medicinal plants that might help with diabetes were published by Li and Shapiro.This review also looks at how traditional treatments and natural medicines from common medicinal plants can help with diabetes. Traditional medicines made from easily available plants have a lot of promise for finding new drugs to treat diabetes. [12]
The term ‘diabetes mellitus’ basically means ‘excessive urination with sweet-smelling urine’. It’s a group of metabolic disorders where high blood sugar levels happen because of problems with insulin, either not enough insulin being produced or it not working properly Long-term high blood sugar from diabetes can cause damage and dysfunction in many organs, especially the eyes, kidneys, nerves, heart, and blood vessels. When insulin isn’t made enough or doesn’t work well, it leads to high blood sugar levels.When blood sugar levels get really high in hyperglycemia, the excess glucose starts to spill into the urine. But at the same time, the cells don’t get enough glucose because its entry into the cells is messed up. This can make a person feel very thirsty and need to urinate often. If high blood sugar sticks around for a long time, it can cause damage to things like the eyes, kidneys, nerves, heart, and blood vessels.[13]
Diabetes is a kind of metabolic problem that involves both carbs and proteins, and it affects a lot of people, especially those with certain genetic backgrounds. Basically, in diabetes, the way the body handles sugar gets all messed up because of issues with insulin. This can lead to things like high sugar in the urine, ketone buildup in the blood, and problems with blood vessels and organs. The symptoms can include things like abnormal thirst, frequent urination, and weight loss. If it’s not managed well, it can cause other health issues like nerve damage, kidney problems, eye issues like retinopathy, and problems with the heart and blood vessels. So, overall, diabetes can lead to serious health complications if not treated properly.
Diabetes is mainly caused by people leading unhealthy lifestyles, urban living, and getting older. It’s known that the rise in diabetes is linked to things like rapid lifestyle changes. In diabetes, there’s a lot of stress on the body’s cells because of lipid peroxidation and damage to cell membranes, which play a big role in causing secondary complications like cataracts and other issues. Managing these factors can help prevent or delay some of the long-term problems of diabetes. Also, inflammation is involved, with certain enzymes that promote inflammation and reduce antioxidant levels, which worsens complications. Overall, oxidative stress and inflammation contribute a lot to the chronic problems seen in people with diabetes
Researchers are looking into how these plants can help control blood sugar levels, support the immune system, and protect the body from damage caused by diabetes. Some evidence suggests that plant materials tested in labs could be useful in treating or preventing complications of diabetes. These studies also show that certain plant compounds might help reduce inflammation and oxidative stress, which are common in diabetes. Overall, exploring these natural options might provide additional ways to manage diabetes better and reduce the risk of related health issues.[14] Diabetes, with its fast growing spread all over the globe, has now become one of the biggest and toughest health problem that people are facing in today’s world. The rise of diabetes cases in many countries is running side by side with quick economic growth, more urbanisation and shifting of people towards modern lifestyle habits.[15]
CAUSES AND SYMPTOMS OF DIABETES MELLITUS:
Diabetes mellitus is caused by lifestyle, environmental, and hereditary factors.
Type 1 Diabetes is caused by the frequent HLA gene variation, which is caused by the autoimmune destruction of pancreatic β-cells.
Obesity, inactivity, and a poor diet all contribute to insulin resistance and β-cell malfunction, which lead to type 2 diabetes.
Risk factors include aging, family history, genetic predisposition, and some ethnicities. Pregnancy- related hormonal changes (gestational diabetes), medicines, and pancreatitis are examples of secondary causes. Disease onset can also be triggered by poisons and viruses.
Rising blood sugar is the cause of diabetes symptoms.
Overall Symptoms are Increased thirst and appetite, as well as weight loss, Hazy eyesight and frequent urination, extreme exhaustion, non-healing sores are common signs of diabetes.
Men with diabetes may experience erectile dysfunction (ED), diminished sex drive, and weak muscles in addition to the typical symptoms of the disease.
Women with diabetes may also experience symptoms like dry, itchy skin, yeast infections, and urinary tract infections.
Extreme hunger is one of the symptoms of type 1 diabetes. Increased hunger and inadvertent weight loss frequent urination, fatigue, and blurred vision.
Heightened appetite increased thirst, increased urination, fatigue, and blurred vision Slow-healing sores can be caused. Additionally, it might result in recurrent infections. This is because the body finds it more difficult to heal when glucose levels are high.
Since many of the changes can be comparable to those that happen during pregnancy, gestational diabetes may not show any clear signs or symptoms. However, potential symptoms and indicators include Anxiety, Vision blurring, Prolonged thirst, Anxiety, Frequent skin, vaginal, or bladder infections, Urinating frequently, Urine with sugar. When a pregnant woman experiences new or unexpected symptoms, she should consult her physician.
PATHOPHYSIOLOGY OF DIABETES MELLITUS:
Diabetes mellitus (DM) has a very complex cause and different ways of showing in patients, so any kind of classification made is not perfect, but still it is helpful. The way DM is classified usually depends on the physiological state of the person when the diagnosis is done. The system which is mostly used today is based on both the reason (etiology) and the mechanism (pathogenesis) of the disease. This makes it useful for understanding the disease better and also helps doctors to choose proper therapy.
Based on this classification, diabetes is generally divided into four main types: type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM), gestational diabetes mellitus (GDM), and diabetes which is caused or linked with some other specific health problems or disorders.[15]
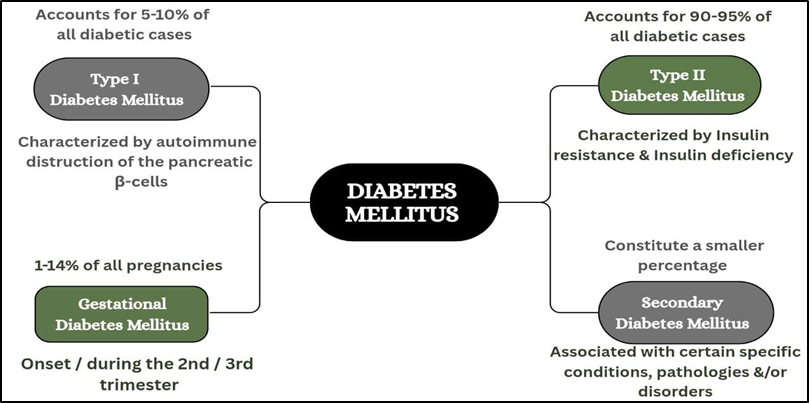
Fig No: 2 Types of Diabetes Mellitus.
Type 1 Diabetes Mellitus:
T1DM is also called type 1A DM, and earlier it was known by other names like insulin-dependent diabetes mellitus (IDDM) or juvenile-onset diabetes. It makes up about 5–10% of all diabetes cases. This is mainly an autoimmune disease where T-cells of the body’s immune system attack and destroy the β-cells of pancreas. Because of this destruction, insulin production goes down, which leads to insulin deficiency and finally high blood sugar (hyperglycemia) occurs . The exact process behind this autoimmune reaction is still not fully clear, but it is considered as the key reason for type 1 diabetes.
The speed at which the immune system destroys the pancreatic β-cells is not always the same, and this difference usually decides how fast the disease develops. In some children and teenagers, the β-cell damage happens very fast and suddenly, leading to complete failure and diabetic ketoacidosis (DKA), which is often the first clear sign of the disease. In other cases, the disease goes on very slowly, with only small rise in fasting blood sugar at first, and it only turns into serious hyperglycemia (with or without ketoacidosis) when the body is under stress like severe infections or other illness.
In certain adults, the β-cells may still keep working partly, making just enough insulin to stop ketoacidosis for many years. But, as insulin keeps reducing with time, these people finally become insulin-dependent when high blood sugar and ketoacidosis start appearing. So, even though the progress of this type of diabetes is not the same for everyone, patients at early, middle, or later stages end up with serious or almost complete insulin deficiency and they must take insulin for survival. This strong lack of insulin at any age is usually shown by very low or sometimes absent plasma C-peptide levels.[15]
Type 1 diabetes mellitus (T1DM) is an autoimmune condition that is marked by different immune markers, mainly autoantibodies. These antibodies are connected to the immune system–driven destruction of β-cells, which is the key feature of this disease.
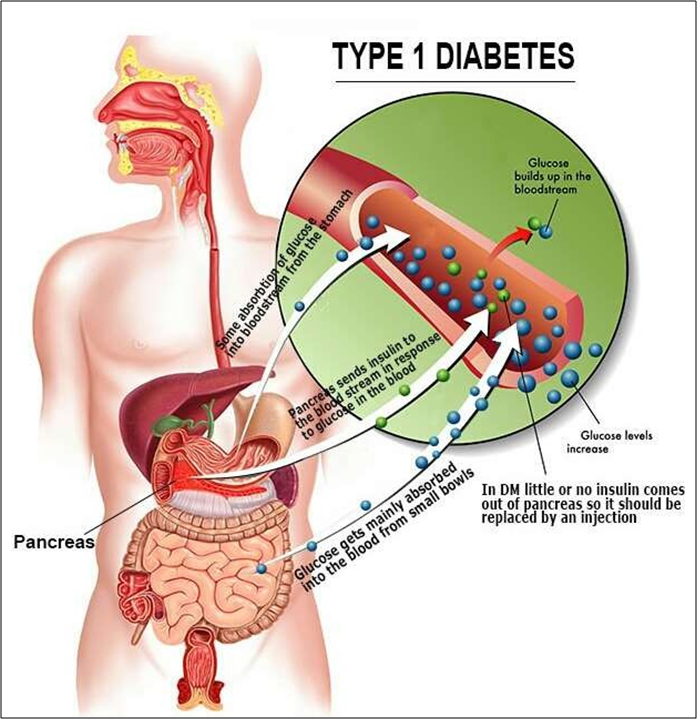
Fig No: 3 Type I Diabetes.
The common autoantibodies are glutamic acid decarboxylase antibodies (GADAs) like GAD65, islet cell antibodies (ICAs) that target β-cell cytoplasmic proteins, antibodies to islet cell antigen 512 (ICA512), antibodies to the tyrosine phosphatases (IA-2 and IA-2α), insulin autoantibodies (IAAs), and antibodies against the zinc transporter isoform 8 (ZnT8) which is specific to islets. For clinical diagnosis, even one of these antibodies can be useful, but in most cases more than one marker is found. Around 85–90% of newly diagnosed T1DM patients show at least one or more of these antibodies. Among them, GAD65 is seen as the most significant ,as it is detected in almost 80% of T1DM cases at the time of diagnosis. After that, ICAs are found in 69–90% of cases, while IA-2α is present in about 54–75% of the patients when they first show the disease.[15]
Type 2 Diabetes Mellitus
Type 2 diabetes mellitus (T2DM), earlier called non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes, makes up about 90–95% of all diabetes cases. This type mainly involves two insulin problems: insulin resistance and dysfunction of β-cells Insulin resistance happens because of disturbances in different cellular pathways, which lowers the sensitivity of body tissues—especially muscle, liver and fat tissue—to insulin. In the beginning stages, when insulin sensitivity drops, the β-cells try to overwork and release more insulin to keep blood sugar normal (normoglycemia). This leads to higher circulating insulin levels (hyperinsulinemia), which for a while can stop hyperglycemia from showing up. But with time, the β-cells can’t keep up. Their function starts going down, and they cannot release enough insulin to match the resistance. This ends up in insulin deficiency, and normal glucose balance cannot be maintained anymore, so hyperglycemia develops. Even though insulin secretion is reduced, in most patients it is still just enough to prevent diabetic ketoacidosis (DKA). Still, DKA may happen under certain stress conditions like severe infections or other health problems. It can also be triggered by some medicines, such as SGLT2 inhibitors, corticosteroids, and second-generation antipsychotic drugs. In the absence of serious physiological stress, most people with T2DM usually don’t need insulin treatment at the beginning of the disease, and sometimes even later in their whole life.
The disease goes forward very slowly and without clear signs, with mild hyperglycemia staying unnoticed for many years. Because of this, T2DM often remains undiagnosed until the typical symptoms of severe hyperglycemia appear, like weight loss, blurry vision, growth problems, polyuria, and polydipsia, usually in the advanced stage. The cause and development of this type of diabetes is quite complicated. It is not only one reason but a mix of many factors—some genetic (polygenic) and others environmental. Generally, T2DM is linked with older age, obesity, family history of diabetes, less physical activity, and modern lifestyle habits. In women, it can also happen if they had gestational diabetes before. It is also commonly connected with health problems like hypertension.[15]
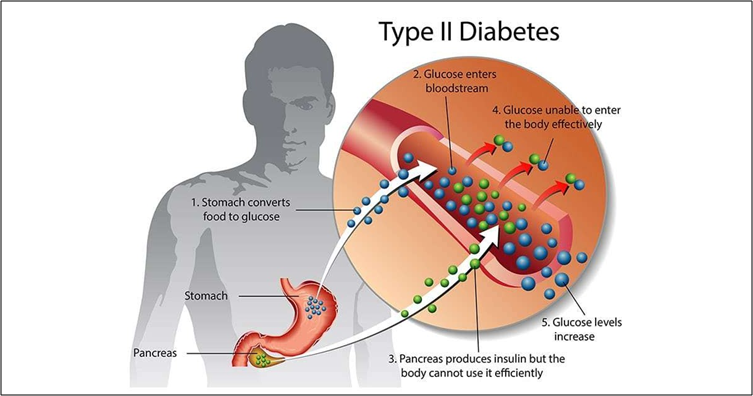
Fig No: 4 Type II Diabetes.
People with T2DM are often linked more with abdominal fat or visceral obesity rather than fat around the hips or under the skin (peripheral obesity) . Because of this strong connection with excess body fat, patients commonly show other cardiovascular risk factors too, like high blood pressure and lipid problems such as high triglycerides and low HDL (good cholesterol). Since T2DM lasts lifelong and is marked by constant metabolic problems caused by hyperglycemia, it usually leads to different complications, both microvascular and macrovascular, especially when the disease advances in middle or older age.Peripheral insulin resistance and insufficient insulin production by pancreatic beta cells are the hallmarks of type 2 diabetes. Reduced glucose transport into muscle cells, increased hepatic glucose synthesis, and accelerated fat breakdown are all consequences of insulin resistance, which has been linked to raised levels of proinflammatory cytokines and free fatty acids in plasma.
Type 2 diabetes is an islet paracrinopathy in which the reciprocal link between the glucagon-secreting alpha cell and the insulin-secreting beta cell is lost, resulting in hyperglucagonemia and, consequently hyperglycemia. Therefore, the function of excess glucagon cannot be understated.
Insulin resistance and insufficient insulin production are both necessary for type 2 diabetes mellitus to develop. The pancreas may atrophy as a result of chronic diabetes. A study by Philippe et al. confirmed decreased pancreatic volume in people with a median 15-year history of diabetes mellitus (range, 5-26 years) using computed tomography (CT) scan results, glucagon stimulation test results, and faecal elastase-1 assays. The exocrine deficit linked to chronic diabetes may also be explained by this.[15]
DIFFERENCE BETWEEN TYPE 1 AND TYPE 2 DIABETES MELLITUS
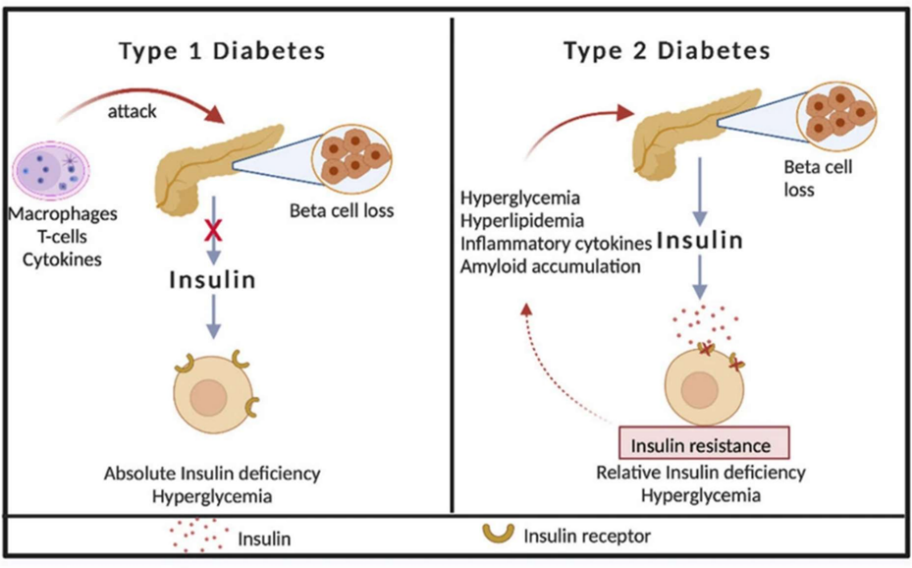
Fig No: 5 Difference between Type I Diabetes and Type II Diabetes.
Gestational Diabetes Mellitus
Pregnancy-related diabetes
Any level of diabetes or glucose intolerance identified at the beginning or throughout pregnancy diabetes mellitus (GDM).the second or third trimester, often. This earlier definition also covered any undiagnosed type 2 diabetes that might start before or at the outset of pregnancy. Nonetheless, the most recent suggestions made by the International Association. Both fasting and postprandial blood glucose levels are typically lower than normal in the first trimester of pregnancy, but they rise in the third trimester. When this blood glucose level approaches diabetic levels, the condition is known as gestational diabetes mellitus (GDM). GDM is responsible for almost 90% of all cases of diabetes and related complications that arise during pregnancy. The prevalence of GDM is significantly impacted by the populations being studied, and its incidence ranges from 1% to 14% of all pregnancies. Certain racial or ethnic groups are more likely than others to develop GDM, and this relationship between ethnicity and GDM risk is significant and well- established.[15]
GDM is most common among Asian Indians, Middle Easterners (Lebanese, Syrian, Iranian, Iraqi, or Afghan), Pacific Islanders, Chinese, Japanese, Korean, and Mexican women, and Aboriginal Australians. The frequency is lowest among non-Hispanic white women and lower among Black women. The risk of GDM increases with age, obesity, previous pregnancy with large babies, and any previous history of impaired glucose tolerance or GDM. Moreover, a higher lifetime risk of developing type 2 diabetes has been linked to GDM. The regular and lifetime screening for any kind of glucose impairment is, therefore, highly recommended in order to ensure early diagnosis of T2DM. Diabetes brought on by monogenic abnormalities in β-cell function Diabetes resulting from monogenic defects in β-cell function constitutes only 0.6–2% of all the cases of diabetes and includes maturity-onset diabetes of the young (MODY) and neonatal diabetes, besides other but rare types.[15]
OTHER TYPES OF DIABETES
Different forms of diabetes:
In addition to T1DM, T2DM, and GDM, diabetes in a number of additional forms has been linked to a number of specific illnesses, such as different pathologies and/or multiple disorders, but in smaller percentages relative to the overall diabetic incidence scenario. Diabetes caused by genetic anomalies in insulin action, endocrinopathies, exocrine pancreatic diseases, and monogenic deficiencies in β-cell activity are the most common kinds of diabetes among these.[15]
Maturity-onset diabetes of the young:
MODY is a genetically, metabolically, and clinically heterogeneous group of mostly non-insulin- dependent diabetes, resulting from mutations in several specific genes involved in pancreatic β-cell function, which affects glucose sensing and subsequent insulin secretion with no or minimal defects, if any, in insulin action. MODY, as the name suggests, has an early onset with glucose tolerance impairment and hyperglycemia occurring usually before the age of 25 years and is often misdiagnosed as T1DM or T2DM MODY2 (GCK MODY). 15–25% of all cases of MODY are caused by MODY2, which is caused by one or more of the more than 200 loss-of-function mutations in the glucokinase (GCK) gene on chromosome 7p13. The initial and rate-limiting step of glycolytic phosphorylation of glucose to glucose- 6-phosphate is catalysed by the GCK enzyme, which is encoded by the GCK gene and acts proportionately to the concentration of glucose. Because of its special catalytic characteristic, the GCK enzyme can act as a kind of glucose sensor and the β-cells can trigger an insulin secretion response that is suitable for the current glucose concentration. The loss-of-function mutations characteristic of MODY2 disrupt this glucose-sensing function of the GCK enzyme such that only hyperglycemic but not normoglycemic levels can elicit a normal insulin secretion response from β-cells[15]
Diabetes mellitus in neonates :
Diabetes diagnosed within the first six months of life is referred to as neonatal diabetes mellitus (NDM), earlyonset diabetes, or congenital diabetes. It is an uncommon condition that affects 1 in 500,000–300,000 (1:500,000–1:300,000) live births worldwide [88,89], while an Italian research found a higher frequency of 1 in 90,000. With 80–85% of cases resulting from monogenic abnormalities, NDM is primarily of genetic origin. It is characterized by severe uncontrolled hyperglycemia and hypoinsulinemia, necessitating insulin replacement treatment. Due to increased apoptotic or non-apoptotic β-cell death, the genetic defects cause β-cell malfunction and decreased β-cell bulk. The pancreas and/or its islets may develop abnormally as a result of these flaws, or in extremely rare instances, they may completely disappear, which would result in hypoinsulinemia, or reduced insulin production and secretion, and in the latter scenario, a full insulin deficit. Neonatal diabetes, which often develops within the first six months of life, is very different from early-onset type 1 diabetes and differs from it in both the aetiology and pattern of inborn pancreatic dysfunction.DM is caused by a number of monogenic abnormalities in β-cell function in addition to MODY and NDM. These include autosomal dominant mutations, which cause an abnormal conversion of proinsulin to insulin or complete incapacity to convert proinsulin to insulin, and point mutations in mitochondrial DNA, such as the 3243AG mutation in the mitochondrial transfer RNA leucine-1 (MTTL1) gene, which causes diabetes and deafness Moreover, it encompasses the mutations that result in the synthesis of insulin molecules with aberrant structures and poor receptor binding.[15]
Diabetes brought on by Inherited Variations in Insulin Activity:
Mutations in the insulin receptor (INSR) gene, which is found on chromosome 19, are primarily responsible for a multitude of genetic abnormalities in insulin action that arise from either a reduction in the number of insulin receptors or functional impairment of insulin receptors. These insulin action anomalies result in insulin resistance or hyperinsulinemia, which in turn causes mild to moderate hyperglycemia or possibly severe hyperglycemia. a sign of diabetes mellitus. Type A insulin resistance syndrome, lipoatrophic diabetes, Donohue syndrome (leprechaunism), and Rabson–Mendenhall syndrome (RMS) are among the different types of diabetes caused by anomalies in insulin action, which are frequently referred to as inherited severe insulin resistance syndromes.
Mutations in the INSR gene cause type A insulin resistance syndrome. Menstrual disorders (primary amenorrhoea or oligomenorrhea) and certain types of polycystic ovarian syndrome are linked to this syndrome. In females, it is characterised by hirsutism brought on by hyperandrogenism and multiple enlarged cysts on the ovaries . In males, it is more common than in females to have acanthosis nigricans, a skin pigmentation disorder, and obesity . It is also linked to severe insulin resistance.[15]
PREVENTION OF DIABETES MELLITUS
Recently, there has been an exponential rise in the prevalence of obesity in particular, which is linked to an increase in the risk of diabetes. It is commonly known that obesity increases the chance of developing diabetes. Because central obesity raises the risk of type 2 diabetes, it has a particularly strong correlation with insulin resistance. The portal vein allows free fatty acids to enter the liver directly. The liver is exposed to a high concentration of free fatty acids due to the accelerated rate of lipid decomposition in visceral fat, which raises the risk of insulin resistance and hepatogenesis. Therefore, in patients with reduced glucose tolerance, reducing visceral fat and the resulting weight can stop the development of diabetes. It is commonly known that obesity and a decrease in physical activity are related. For example, people who work in physically demanding occupations typically have low prevalences of T2D. Diabetes became more common as a result of these individuals' tendency to abandon their traditional way of life and quickly adopt an urbanised one. There is a worldwide trend of people leading modern lives engaging in less physical activity as a result of spending more time on their smartphones or watching television. Exercise improves insulin resistance by directly increasing the skeletal muscle's insulin-mediated glucose absorption. Regardless of age or weight, a study conducted on Caucasian men revealed that increasing exercise intensity decreased the incidence of diabetes.[16]
Dietary Intervention:
Cutting back on calories is the most crucial step in preventing type 2 diabetes. Rather than emphasising the consumption of certain nutrients, nutritional counselling should concentrate on developing healthy eating habits. Certain food intakes have an impact on the risk of diabetes. Numerous studies have consistently shown that eating refined grains, processed red meat (ham), and beverages with simple sugars increases the risk of developing new-onset diabetes, while eating vegetables, fermented yoghurts, nuts, berries, and coffee lowers the risk. According to a prior randomised controlled study, customised medical nutritional therapy successfully lowered the amount of glycated haemoglobin. Education on diet treatment should take into account social, cultural, and personal aspects in addition to being tailored to each individual.
Fat
According to recent research, the kind of fat consumed is more significant than its quantity. 9,200 people in Jacobs' study, which followed 166,550 multiracial cohorts (Caucasian, African-American, Hawaiian, Japanese, and Hispanic) for ten years, developed new-onset diabetes. Low incidence of diabetes (13–28%) was associated with the food quality indicators. A prospective cohort study's meta-analysis revealed that a Mediterranean diet high in monosaturated fat prevented.
Omega-3
Docosahexaenoic acid and eicosapentaenoic acid consumption reduced the risk of developing new diabetes in a meta-analysis of 18 cohort studies involving 540,184 people (risk ratio, 1.04 for the intake of 250 mg/day; 95% CI, 0.97, 1.10) However, in western countries, eating fish increased the intake of omega-3 fatty acids, whereas in eastern countries, the risk was found to have decreased. The additional consumption of omega-3 fatty acids did not lower the level of glycated haemoglobin, according to a meta- analysis of 20 randomised controlled trials on T2D patients.Fruits have not been linked to an increased risk of diabetes, according to numerous research. A meta-analysis of three prospective cohort studies found that eating apples, blueberries, and grapes decreased the incidence of diabetes. The relative risk ratio for apples was 0.82 (0.73–0.92), for grapes it was 0.77 (0.64–0.92), and for blueberries it was 0.82 (0.69–0.98). This was in contrast to those who had fewer than four servings of these fruits each week. On the other hand, eating peaches, bananas, oranges, and strawberries did not appear to have any protective effects.
Vitamin D (Vit D)
Unless the patient has a vitamin or mineral shortage, it is not advised for patients with type 2 diabetes to take additional vitamins or minerals. Nonetheless, to guarantee sufficient vitamin intake, a balanced diet is to be advised. The incidence of new-onset diabetes was found to be inversely correlated with the plasma level of 25-hydroxy vitamin D in a meta-analysis that included a prospective study24; however, this does not prove that a low vitamin D level is the reason for elevated blood glucose. Without lowering the amount of glycated haemoglobin, a meta-analysis of 20 small-scale randomised controlled experiments on vitamin D supplementation revealed that vitamin D enhanced the insulin resistance indicator (homeostasis model assessment-insulin resistance).
Dairy goods
It has been demonstrated that several dairy products can lower the risk of developing diabetes. Fermented yoghurts demonstrated the most significant benefit on diabetes prevention (related risk ratio, 0.83 [95% CI, 0.74, 0.90]), but common plain milk had no preventative effect (relative risk ratio, 0.95 after adjustment [95% CI, 0.86, 1.05] in a meta-analysis that included seven cohort studies. Low-fat dairy products demonstrated greater preventative benefits than high-fat ones (relative risk ratio, 0.82 vs. 1.00). Nevertheless, simple sugars are included in a lot of fermented yoghurts that are sold commercially.
A Study on The Prevention of Diabetes in Korea
In order to prevent diabetes, the American Diabetes Association currently advises prediabetic patients to lose 7% of their body weight. The 7% weight loss is not applicable to all patients in Korea because many prediabetic individuals are thin. The pathophysiology of type 2 diabetes is different in Koreans than in Caucasians. In the Korean investigation, prediabetic patients did not exhibit compensatory hypersecretion of insulin in response to the rise in insulin resistance. The proportion of obese Korean patients is lower than that of Caucasians, and multiple investigations have shown that insulin insufficiency is frequently detected as early as possible.[16]
PHARMACOLOGICAL INTERVENTIONS
Suggestions
A . Adults with pre-diabetes, as defined by the Diabetes Prevention Program, who have a BMI of 35 kg/m2, higher fasting plasma glucose (e.g., 110 mg/dL), higher A1C (e.g., 6.0%), and women who have previously had gestational diabetes mellitus should be evaluated for metformin therapy as a preventative measure for type 2 diabetes.
B. Prolonged use of metformin may result in biochemical vitamin B12 deficiency; patients taking metformin should have their vitamin B12 levels checked on a regular basis, particularly if they have peripheral neuropathy or anaemia.
People undergoing weight loss therapy may benefit from support and additional pharmacotherapeutic alternatives, if necessary, as weight loss through dietary and exercise changes alone can be challenging to maintain over the long term In certain populations, it has been demonstrated that metformin, a-glucosidase inhibitors, liraglutide, thiazolidinediones, testosterone , and insulin reduce the risk of diabetes however, nateglinide did not prevent diabetes . Furthermore, studies have demonstrated that a number of weight- loss drugs, including orlistat and phentermine topiramate, can reduce the prevalence of diabetes in people with prediabetes to varied degrees . Research on various pharmaceutical treatments has demonstrated that valsartan is somewhat effective at preventing diabetes, while ramipril and anti-inflammatory medications are ineffective at doing so. Although post hoc analyses and meta-analyses indicate a possible benefit in particular populations, the Vitamin D and Type 2 Diabetes (D2d) prospective randomised controlled trial found no significant benefit of vitamin D versus placebo on the progression to type 2 diabetes in high-risk individuals . To identify patient characteristics and clinical signs where vitamin D treatment may be beneficial, more research is required.[17]
DIAGNOSIS
Diagnosis and Treatment of Diabetes Mellitus (DM)
Diagnosing and managing diabetes is a key step toward controlling the disease and preventing long-term complications.
Diagnosis
Diabetes is usually diagnosed through standard blood tests such as:
Fasting Plasma Glucose (FPG): Checks blood sugar after fasting for at least 8 hours. Levels of 126 mg/dL or higher suggest diabetes.
Oral Glucose Tolerance Test (OGTT): Measures blood sugar two hours after consuming a glucose drink. Readings of 200 mg/dL or more indicate diabetes.
Hemoglobin A1c (HbA1c): Shows average blood sugar levels over the past few months, with 6.5% or above confirming diabetes.
Although accurate, these tests require drawing blood, which can be painful and inconvenient for regular monitoring. Factors like age, time of day, and body condition can also affect results.
Advances in Diagnosis
New technologies, especially nanotechnology-based tools, are being developed to make diagnosis easier and less invasive.
Examples include:
Nanobiosensors: These devices can detect glucose from body fluids like saliva, sweat, or tears.
Theranostic Nanoparticles: These systems can both detect and treat diabetes, allowing earlier intervention even before symptoms become obvious.
Such innovations aim for faster, painless, and continuous glucose monitoring for better disease control.[16]
TREATMENT
Insulin Therapy
For people with type 1 diabetes and those with advanced type 2 diabetes, insulin remains essential to control blood sugar levels. Traditional insulin injections, however, are associated with discomfort, risk of low blood sugar, weight gain, and other side effects.
Researchers are now exploring alternative ways to deliver insulin, such as:
Oral delivery: Challenging due to stomach acid and intestinal barriers that break down insulin.
Inhalable (pulmonary) delivery: A non-invasive option, though it faces issues with drug stability and absorption.
Other strategies to improve insulin delivery include using enzyme inhibitors, absorption enhancers, molecular modifications (like PEGylation), and target-specific ligands such as vitamin B12 or transferrin. However, issues like long-term safety and nutrient absorption still need attention.
Oral Medications for Type 2 Diabetes
In addition to insulin, there are several drug classes available for managing type 2 diabetes when diet and exercise aren’t enough:
Sulfonylureas – stimulate insulin release from the pancreas.
Biguanides (Metformin) – reduce glucose production in the liver and increase insulin sensitivity.
Meglitinides – prompt short-term insulin release around meals.
Thiazolidinediones – help muscles and fat tissues use glucose more efficiently.
Alpha-glucosidase inhibitors – slow down carbohydrate absorption in the intestine.
Many of these drugs have poor water solubility, meaning their absorption and effectiveness can vary between individuals. To maintain stable blood sugar levels, sustained and controlled release drug formulations are being developed.
Emerging Drug Delivery Technologies
To improve results and patient comfort, advanced drug delivery systems are now under study: Nanocarriers such as liposomes and polymeric nanoparticles boost the stability and absorption of drugs. Controlled-release formulations help maintain steady blood sugar throughout the day.
Hybrid systems combine immediate and sustained release patterns to better mimic the body’s natural insulin rhythm.[16]
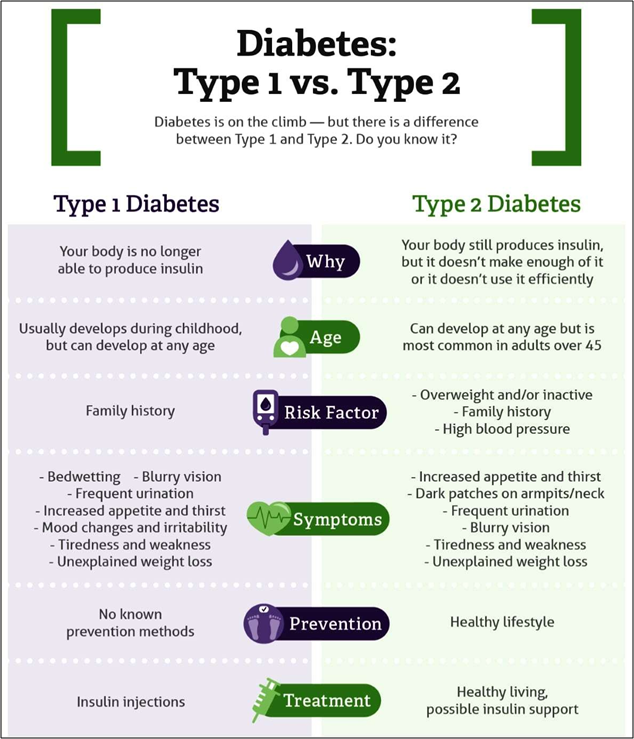
Fig No: 6 Type I and Type II Diabetes.
Around 5–10% of all diabetes cases.
Caused mainly due to autoimmune attack on the pancreatic β-cells.
Makes up almost 90–95% of diabetic patients.
Mostly due to insulin resistance along with not enough insulin production.
Seen in about 1–14% of pregnancies.
Usually starts during 2nd or 3rd trimester of pregnancy.
A smaller fraction of diabetes cases.
Linked with other health issues, disorders or specific pathological conditions.[18]
DIABETES DEVICES
Insulin Pens
Regardless of whether a patient has type 1 or type 2 diabetes, the aim of insulin therapy is to return blood glucose levels to normal. It has been demonstrated that restoring normal glucose levels lowers the risk of microvascular problems in individuals with type 1 or type 2 diabetes as well as the risk of macrovascular consequences in those with type 1 diabetes. In the past, a syringe filled with insulin from a vial has been used to inject insulin. Prefilled disposable pens and refillable injectable devices that resemble pens have lately been made available as substitutes. More recently, inhaled products and formulations that are forced subcutaneously by a burst of air have been added to the list of alternatives for administering insulin. However, these methods are not as commonly employed, and there isn’t a commercially accessible inhaled insulin product at the moment. In either basal-only, split-mixed (often requiring two daily injections of long-acting and short-acting insulin mixes), or basal-bolus insulin regimens, patients commonly utilise insulin pens to provide both long-acting and short-acting insulin.[19] Cost is the main drawback of utilising insulin pens, as it is with other new diabetes technologies. When bought as prefilled or refillable pens, insulin analogues cost about 30% more per unit than when bought in vials. Insurance companies might therefore be hesitant to pay for the extra expense of administering insulin using pen devices unless there are exceptional circumstances, such tremor or vision impairment.[20]

Fig No: 7 Insulin Pen
Monitoring Glucose
The creation of self-monitoring blood glucose (SMBG) may be the most significant advancement in the treatment of diabetes, aside from the discovery of insulin. Prior to blood glucose meters becoming commercially available, patients used urine glucose concentration estimation to track how well they were responding to treatment. In essence, patients used an imprecise assessment of glucose control to modify the dosages of drugs like insulin. Patients may now measure their glycaemic control with much more accuracy thanks to SMBG, which enables more intelligent medication titration. Patients with type 1 diabetes have been shown to benefit from glucose monitoring. It has been linked to better glycaemic control when done at least once a day in patients with type 2 diabetes receiving medication. While some research has indicated that patients undergoing SMBG have better glycaemic control, not all investigations have come to the same result. For patients receiving several daily doses of insulin or insulin pump therapy, the American Diabetes Association (ADA) advises that SMBG be carried out three or more times per day. SMBG may still be helpful in helping patients on different regimens, like oral medications or basal insulin treatment, achieve appropriate glycaemic control, particularly postprandially.[20]
Fig No: 8 Monitoring Glucose.
Insulin Pumps :
Since the 1970s, insulin pumps have been sold commercially to help patients with type 1 diabetes manage their blood sugar levels. Patients who use an insulin pump receive a continuous subcutaneous infusion of short-acting insulin instead of several daily subcutaneous injections of short-acting insulin and either long- acting or intermediate-acting insulin. These devices contain an insulin reservoir and deliver insulin to subcutaneous tissue through a plastic tube. Typically, the tube is replaced every three days. There are numerous pumps that differ in size and cost. Compared to numerous daily injection therapy, insulin pump therapy has a number of benefits. Compared to insulin pens or syringes, pumps can provide insulin doses more accurately.Both patients and carers must be very committed to using insulin pumps. When a pump breaks down and needs to be replaced, a patient must quickly resume insulin doses while they wait for a replacement. Catheter occlusions can occur in patients, stopping the insulin flow. In order to treat persistent, unexplained hyperglycemia, patients need to be particularly aware of their blood sugar levels and ready to adjust their insulin infusion schedule. One of the most crucial components of effective pump therapy is careful patient selection because insulin pumps can be both labour-intensive and technically complex.[20]

Fig No: 9 Insulin Pumps.
CLASSIFICATION ON ANTIDIABETIC DRUGS
Table no 1: Classification of Antidiabetic Drugs.
|
Class (Route) |
Representative Agents |
Mechanism of Action |
Metabolic Alterations |
Cardiovascular Benefit/ Risk |
|
Biguanide (oral) |
Metformin |
Insulin sensitizer; inhibits hepatic glucose production |
Can cause lactic acidosis (rare); mayalter electrolytes /pH |
Reduces MI by 39% and coronary deaths by 50% (UKPDS) |
|
DPP-4 inhibitors (oral) |
Sitagliptin, Saxagliptin, Vildagliptin, Linagliptin, Alogliptin |
Inhibit DPP-4 enzyme → ↑ GLP-1 activity |
Decreases postprandial lipemia |
May increase CHF risk (esp. Saxagliptin) |
|
SGLT2 inhibitors (oral) |
Canagliflozin, Dapagliflozin, Empagliflozin |
Block glucose reabsorption in PCT (90%) → glucosuria (insulin-independent) |
May increase LDL-C; mild ketoacidosis risk |
CV benefit (↓ BP, ↓ uric acid, ↓ hospitalization for HF) |
|
Insulin (parenteral) |
Regular, NPH, Lispro, Aspart, Glulisine, Glargine, Detemir, Degludec, Premixes |
Activates insulin receptors → glucose uptake in target tissues |
Possible electrolyte imbalance |
May cause HF with TZDs |
|
GLP-1 receptor agonists (parenteral) |
Liraglutide, Exenatide, Dulaglutide |
GLP-1 agonist → ↑ insulin, ↓ glucagon, delayed gastric emptying, ↑ satiety |
Improves postprandial metabolism |
Reduces CV risk |
|
Sulfonylureas (oral) |
Glimepiride, Glipizide, Glyburide |
Stimulate pancreatic insulin secretion |
— |
May increase CV risk due to hypoglycemia |
|
Thiazolidinediones (TZD) (oral) |
Rosiglitazone, Pioglitazone |
PPAR-γ agonist → improves insulin sensitivity |
Improves HDL; may cause fluid retention |
Risk of HF (esp. with insulin) |
Table no 2: Classification of Antidiabetic depending on onset, peak and duration.
|
Type |
Examples |
Onset |
Peak |
Duration |
|
Short-acting |
Regular (Humulin R, Novolin R) |
30 min– 1 h |
2–5 h |
8 h |
|
Intermediate |
NPH (Humulin N) |
1.5–4 h |
4–12 h |
24 h |
|
Long-acting |
Glargine, Detemir, Degludec |
0.8–4 h |
Minimal |
24 h+ |
|
Rapid-acting |
Lispro, Aspart, Glulisine |
10–30 min |
30 min–3 h |
3–5 h |
|
Premixed |
Lispro/Protamine, Aspart/ Protamine, NPH/ Regular |
5–60 min |
Dual |
10–16 h |
AYURVEDIC HISTORY ON ANTI DIABETES
Ayurvedic medicine has been used for a really long time to treat diabetes, which they call "Madhumeha." The ancient texts like Charaka Samhita and Sushruta Samhita talk about different herbs and therapies to help keep blood sugar levels normal and improve overall health. In Ayurveda, diabetes is seen as a problem with the body's doshas, mainly Kapha, and it's linked to issues in digestion and metabolism. The treatments usually include herbal remedies, diet changes, lifestyle adjustments, and detox therapies called Panchakarma
Some of the most common herbs used for diabetes in Ayurveda are Gymnema sylvestre (Gurmar), Fenugreek (Methi), Bitter Melon (Karela), Indian Gooseberry (Amla), and Turmeric (Haridra). These herbs are thought to help control blood sugar, boost insulin sensitivity, and support the pancreas. Over the years, Ayurvedic doctors have recorded many herbal mixes and treatment plans for diabetes, focusing on a complete approach that combines herbs, diet, and lifestyle. Even today, scientists are studying these traditional herbs to see how they might help manage diabetes safely and effectively.
Here is a list of some common Ayurvedic herbs and medicines used for treating diabetes (Madhumeha):
Table No 3: Detailed uses parts used name and the family of the drug used in treating Antidiabetes.
|
Botanical Name |
Family |
Parts Used |
Method of Extraction |
Key Phytoconstituents |
Pharmacological Process/ Mechanism |
|
Gymnema sylvestre |
Apocyna-ceae |
Leaves |
Hydroalcoholic / Aqueous extraction |
Gymnemic acids, Gurmarin |
Stimulates insulin secretion, regenerates β- cells, reduces intestinal glucose absorption |
|
Momordica charantia |
Cucurbit-aceae |
Fruit, Seeds |
Methanolic / Aqueous extraction |
Charantin, Polypeptide-p, Momordicosides |
Mimics insulin action, improves glucose uptake, decreases hepatic gluconeogenesis |
|
Trigonella foenum- graecum |
Fabace-ae |
Seeds |
Soxhlet extraction (alcohol/water) |
Trigonelline, Diosgenin, Galactomannan |
Slows carbohydrate digestion, enhances insulin sensitivity, lowers postprandial glucose |
|
Tinospora cordifolia |
Menispe- rmaceae |
Stem, Leaves |
Aqueous / Ethanol extraction |
Berberine, Tinosporaside, Cordifolioside |
Enhances glucose utilization, modulates oxidative stress, protects pancreatic cells |
|
Syzygium cumini |
Myrtaceae |
Seeds, Bark |
Aqueous / Hydroalcoholic extraction |
Jamboline, Ellagic acid, Flavonoids |
Delays starch digestion, promotes insulin secretion, reduces oxidative damage |
|
Aloe vera |
Asphod- elaceae |
Leaf gel, Latex |
Gel extraction / Alcoholic methods |
Aloin, Aloesin, Polysaccharides |
Improves β-cell activity, enhances glucose uptake, shows antioxidant and lipid-lowering effects |
|
Ocimum sanctum (Tulsi) |
Lamiaceae |
Leaves |
Hydroalcoholic extraction |
Eugenol, Rosmarinic acid, Flavonoids |
Reduces oxidative stress, improves insulin function, lowers fasting blood glucose |
|
Pterocarpus marsupium |
Fabaceae |
Heart wood |
Methanolic extraction |
Pterostilbene, Marsupsin, Epicatechin |
Stimulates insulin secretion, protects pancreatic β-cells, decreases blood glucose levels |
|
Allium sativum (Garlic) |
Amaryll- idaceae |
Bulb |
Steam distillation / Ethanol extract |
Allicin, S-allyl cysteine, Sulfur compounds |
Enhances insulin sensitivity, reduces lipid peroxidation, lowers fasting glucose |
MARKET ANALYSIS OF ANTIDIABETIC DRUGS
The cost of medications marketed in India and other nations varies greatly from one another. There aren't many studies that show these kinds of open-market pricing fluctuations. The price of a certain medication produced by other businesses in the same dose form, strength, and quantity was compared. The percentage price variation as well as the difference between the maximum and minimum prices of the identical medication produced by various pharmaceutical businesses were computed.[22]
Patients are burdened by the high cost of medications, particularly when treating chronic conditions like diabetes. One of the main causes of patient noncompliance is the high cost of medications, which results in inadequate blood sugar management and an increase in the morbidity linked to diabetes. Therefore, while choosing an antidiabetic medication therapy, the cost of the treatment should be a key factor. According to the bioequivalence statistics, prescribing a less expensive brand of antidiabetic medication will be a financially feasible option for the patient and boost adherence to therapy in the long-term treatment of diabetes.[23]
People with diabetes usually have medical expenses that are 2.3 times greater than they would be if they did not have the condition. People with diabetes usually spend USD 16,750 a year on medical bills, of which USD 9,600 are directly associated with the condition. In India, the estimated median yearly direct and indirect expenses of treating diabetes were ?4,970 and ?25,391, respectively. The total anticipated lifetime cost of all diabetic drugs is ?19,45,135. The average monthly cost per patient (ppm) was 1,265 naira, of which 993 naira was spent on medical bills and 271 naira on nonmedical ones. Patients with diabetes had an annual total cost of care (COI) of ?22,456.[24]
18. Between 2006 and 2016, 14 novel active ingredients were released, including three SGLT-2 inhibitors, five DPP-4 inhibitors, and five GLP-1 receptor agonists. Degludec was regarded as a novel kind of insulin. Fig no 10. shows the availability of novel antidiabetic drugs in the participating nations. Available in France, Hungary, Germany, Austria, Sweden, and the UK, the new antidiabetic medications also included a combination of two novel active ingredients: insulin degludec and the GLP-1 receptor agonist liraglutide. Liraglutide and degludec together were considered in the group of GLP-1 analogues in subsequent analyses.[25]
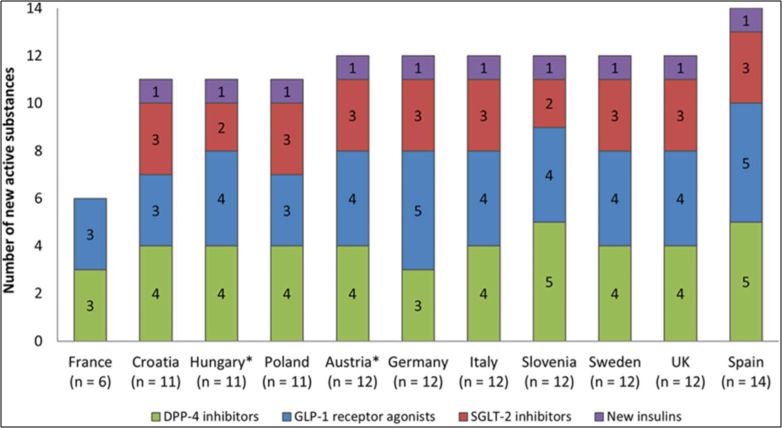
Fig No: 10 Graph based on Marketing Analysis based on Antidiabetes
Diabetes affects over 171 million people globally, and by 2030, its incidence is predicted to increase. Heart failure is more likely to occur in people with diabetes; the relative risk rises by 10% to 15% for every unit increase in glycated haemoglobin. On the other hand, 25–40% of persons with diabetes have heart failure. It has also been proposed that any degree of hyperglycemia is linked to higher rates of hospitalisation, even in patients without obvious diabetes, and that individuals with heart failure fare worse if they also have diabetes.[26]
In 2024, Novo Nordisk will have the largest market share in the world market for antidiabetic drugs. Market Share and Growth for Diabetes Drugs | Global Report [2032]. The Danish pharmaceutical company's extensive product line and substantial R&D expenditures are responsible for its dominance.With projected sales of $6.2 billion and $6.6 billion in 2024, respectively, Novo Nordisk's GLP-1 receptor agonist Ozempic (semaglutide) and Eli Lilly's Trulicity (dulaglutide) are two of the best- selling antidiabetic medications. Trends in Antidiabetic Drug Discovery: New Drugs in Clinical Trials, FDA-Approved Drugs, and Worldwide Sales - PMC. These more recent GLP-1 drugs have grown in popularity and are significant sources of income for the market for diabetic treatments.
CONCLUSION
By the end of the sudy based on Antidiabetic it is concluded that Diabetes Mellitus is a chronic, multifactorial metabolic disorder that has emerged as one of the most challenging global health problems. It results from either insulin deficiency, insulin resistance, or both, leading to persistent hyperglycemia and multiple long-term complications affecting vital organs such as the heart, kidneys, eyes, and nerves. The review highlights the growing prevalence of diabetes worldwide due to rapid urbanization, sedentary lifestyle, and dietary changes.
Conventional treatment options such as insulin and oral hypoglycemic agents remain the mainstay of therapy, yet they often present limitations including side effects, high cost, and patient non- compliance. Recent advances, including nanotechnology-based diagnostic tools and innovative drug delivery systems, have improved the accuracy of glucose monitoring and therapeutic efficacy.
In addition, herbal and Ayurvedic medicines — such as Gymnema sylvestre, Momordica charantia, Trigonella foenum-graecum, Tinospora cordifolia, and Syzygium cumini — have shown significant antidiabetic potential through mechanisms like β-cell regeneration, improved insulin sensitivity, and antioxidant effects. Integrating such traditional knowledge with modern pharmacology could lead to safer and more sustainable treatment approaches.
Ultimately, prevention through healthy diet, regular physical activity, and early diagnosis remains the cornerstone in combating diabetes. Continuous research into novel synthetic and plant-derived antidiabetic agents, along with effective public awareness, is essential to reduce the global burden of this disease.
REFERENCES


Mohammed Zakee Muazzam Malgundkar, Sumedha Bane, An Overview on Antidiabetic Disease, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1597-1617. https://doi.org/10.5281/zenodo.18269433
 10.5281/zenodo.18269433
10.5281/zenodo.18269433
