
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Vijayrao Naik College of Pharmacy, Kankavli, India
The fourth most prevalent neurological condition, epilepsy, is characterized by prominent comorbidities that affect quality of life and frequent convulsions. Although they have improved seizure control, conventional therapies such as oral, parenteral, rectal, buccal, nasal, transdermal, and nanotechnology-based drug delivery systems face difficulties such poor adherence, medication resistance, and limited blood-brain barrier penetration. New possibilities for managing epilepsy have been made possible by recent developments in artificial intelligence (AI) and machine learning (ML). These include seizure detection, prediction, individualized treatment planning, medication delivery optimization, surgical support, and caregiver aid. EEG-based prediction models, wearable technology driven by AI, and neuroimaging techniques improve therapy outcomes, monitoring, and diagnostics while lowering side effects and enhancing patient safety. However, it is necessary to overcome the constraints pertaining to cost, openness, data requirements, and ethical considerations. This paper emphasizes how AI might be used to diagnose epilepsy and distribute medications, highlighting its revolutionary potential while acknowledging present obstacles and prospective future research areas.,
Although epilepsy affects millions of people worldwide, little is known about this fourth most frequent neurological disorder compared to less common conditions like multiple sclerosis and Parkinson's disease. Not all seizures are caused by epilepsy, and seizures associated with epilepsy can differ greatly in severity and the areas of the brain that are impacted. Epilepsy is a complicated medical condition. Furthermore, many individuals with epilepsy also have other comorbid medical disorders that can have a substantial impact on their overall health and well-being. Epilepsy is more than just seizures. Epilepsy-related health care and community resources are frequently dispersed, disorganized, and difficult to reach. The groups with newly diagnosed epilepsy that are expanding the fastest are children and older individuals. People with epilepsy may have varied degrees of impairment in their quality of life; this may include limitations on their driving and work abilities, as well as consequences on their social connections and family dynamics. For people, their families, and society as a whole, these difficulties have a substantial indirect cost in the form of lost production due to underemployment, unemployment, and early death. Misconceptions regarding epilepsy have grown and been reinforced in popular culture over the ages, leading to social exclusion and stigma that can worsen quality of life and have an impact on health. It has proven challenging to undo this history of stigma and discrimination. There are numerous ongoing initiatives to enhance the lives of individuals with epilepsy and their families in spite of these obstacles; these initiatives must go on and be reinforced in order for all individuals with epilepsy to eventually have access to the entire spectrum of coordinated health and community services that they require. Many patients with epilepsy are able to have fewer or no seizures thanks to access to modern drugs, medical gadgets, surgery, and other treatments. For those with epilepsy who do not react to current medications or who experience intolerable side effects from existing treatments, new therapy choices are required. Depending on the audience, different kinds of information and differing degrees of depth are needed for educating individuals with epilepsy, their families, medical professionals, and the general public on the condition. To enable individuals with epilepsy and their families to actively participate in patient-centered epilepsy treatment and management, educational materials and techniques that support optimal self-management must be assessed and extensively distributed. Furthermore, more information is required regarding the prevalence and effects of epilepsy, as well as prevention and early detection chances, in order to better target initiatives and make them more sustainable during these resource-constrained times. Planning and policy initiatives to improve the lives of individuals with epilepsy can be guided by data from improved research and surveillance. [1,2]
Classification of seizures [3-5]
A. Focal seizures
i. Motor onset
1. Focal automatism seizures
Often misdiagnosed and ignored as seizures, focal automatism seizures are characterized by repeated motor activity, typically under impaired awareness, and occasionally followed by amnesia. Such actions include lip-smacking, rubbing, wandering, and repeating words.
2. Focal atonic seizures
These are abrupt, brief seizures characterized by a loss of muscular tone that can affect one limb or one side of the body. Usually, awareness is maintained.
3. Focal tonic seizures
Which manifest clinically as stiffness of the neck or limb, are seizures characterized by a prolonged increase in muscle contraction that lasts for a few seconds or minutes.
4. Localized colonic convulsions
Steady, rhythmic jerking of a muscle group that might be symmetrical or asymmetrical.
5. Localized epileptic attacks
Children frequently experience sudden, uncontrollable, and occasionally painful muscular contractions. clinically manifest as abrupt waist flexion and arm and leg flexion or extension, which can be focal, widespread, or have an unclear beginning. It can also happen in clusters. Video-EEG is typically used to diagnose it. Infantile spasm is the term for it when it happens to babies. Usually, awareness is maintained.
6. Hyperkinetic focal seizures
Seizures that include frenzied kicking, thrashing, and pedaling, among other excessive and frequently uncontrollable muscle movements.
7. Myoclonic focal seizures
Though they are typically short, unsustained muscle spasms that happen suddenly and persist for a few seconds or even less than a second, or only an erratic jerking in one portion of the face or body, they may resemble clonic seizures. Usually, awareness is maintained.
ii. Non-motor onset
1. Focal autonomic seizures without movement
The autonomic nervous system is affected by these seizures, which manifest as symptoms like a rising stomach sensation, heat and cold sensations, an odd taste or smell, etc.
2. Arrest seizures of focal non-motor behavior
These seizures manifest by stopping all activity and remaining unresponsive for the duration of the episode.
3. Focal cognitive seizures without movement
A patient is considered to have experienced cognitive seizures if they experienced hallucinations, illusions, or verbal impairments during the seizure occurrence.
4. Emotional focal non-motor seizures
Emotions such as panic, worry, fear, excitement, sobbing, melancholy, or any other emotion can trigger these non-motor seizures.
5. Focal sensory seizures without motor action
Visual, olfactory, auditory, gustatory, somatic hallucinations, or vertigo are some of the aberrant experiences that accompany these seizures.
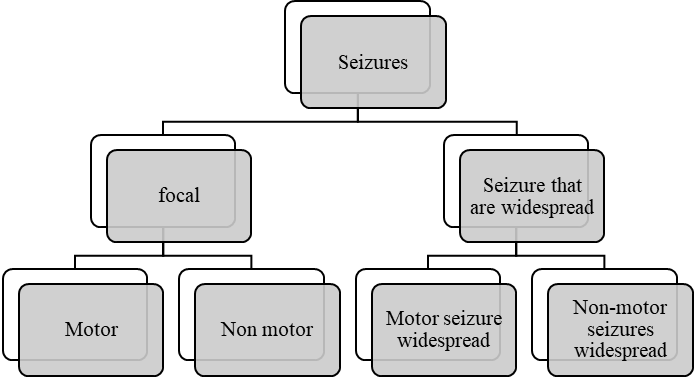
Figure 1 Classification of seizures
B. Seizures that are widespread
There are two types of generalized seizures: motor and non-motor. Tonic-clonic, clonic, tonic, myoclonic, myoclonic-tonic-clonic, myoclonic-atonic, atonic, or epileptic spasms are examples of motor seizures, while normal or atypical absence seizures, seizures involving myoclonic activity, or seizures involving eyelid myoclonia are examples of non-motor seizures. Since the majority of generalized seizures are linked to awareness impairment, the awareness-based classification is purposefully left out.
i. Motor seizure that is widespread
1. Seizures that are myoclonic-clonic
Usually, people with juvenile myoclonic epilepsy exhibit this seizure. Arms jerking, tonic stiffening, and finally clonic rhythmical jerking are its defining characteristics.
2. Seizures that are myoclonic atonic
Previously known as myoclonic astatic seizures, this seizure is frequently observed in people with Doose syndrome. It is characterized by a limp drop after a transient shaking of the trunk or limbs.
ii. Non-motor seizures that are widespread
1. Common seizures of absence
These seizures are typified by abrupt interruptions of activities, followed by a blank look. Occasionally, there is eye deviation that lasts anywhere from a few seconds to half a minute, followed by a quick recovery.
2. Unusual absence convulsions
It starts slowly and causes noticeable changes in muscular tone that are more noticeable than in normal absence. At EEG, it exhibits modest spike waves, often less than three per second.
3. A seizure with myoclonic absence
A brief period of rhythmic jerking precedes the staring phase that follows this seizure.
4. Myoclonia of the eyelids
The gazing spell (absence seizure) may be linked to the abrupt, powerful upward jerking of the eyelids that occurs during this seizure. Usually, closing the eyes stimulates it.
C. Unidentified seizures
Unknown onset seizures are those that happen while you're sleeping or in a situation that's difficult to define since the patient is by themselves or the witness is unable to do so. Additionally, it is considered an unclassified seizure when the doctor is positive that the information provided is a seizure episode but is unable to characterize it because of insufficient details. Thus, "unknown onset" is merely a nickname and does not refer to the seizure's nature.
The pathophysiology of epilepsy is characterized by significant alterations in astrocytes that impair their homeostatic capabilities, which results in a compromised ability to regulate neuronal excitability via processes like glutamate clearance and K+ buffering. One of the main characteristics of the illness is the functional asthenia of astrocytes.
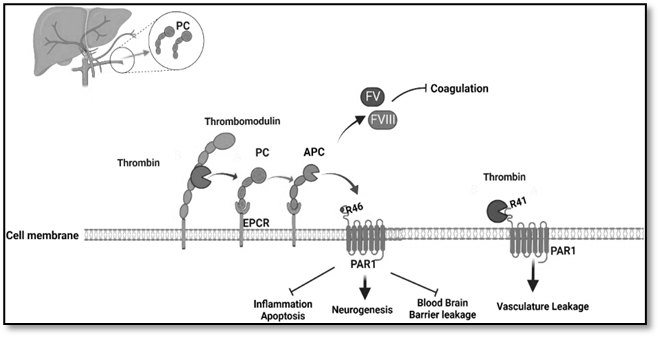
Figure 2 Pathophysiology of epilepsy [7]
ML and DL models, which allow computers to analyse data, make decisions, make predictions, and learn from the data they encounter, are frequently grouped together under the umbrella term artificial intelligence (AI). Numerous studies have tried various machine learning techniques, including logistic regression, linear discriminant analysis, and support vector machines, in the context of epilepsy imaging research. Neural networks, the foundation of deep learning, have progressed from single-layer to dual-layer and multi-layer neural networks to more intricate designs like deep neural networks, which are being used more and more in imaging studies for epilepsy. EEG data was used to test automatic seizure detection using supervised machine learning algorithms such k NN, SVM, and deep ML.Better epilepsy diagnostic models are produced when state-of-the-art AI algorithms are combined with superior clinical EEG data. The fields of artificial intelligence (AI) and machine learning (ML) are expanding quickly, and there is increasing interest in combining and using these technologies to help doctors deal with diagnostic uncertainty. Wearable data, neuroimaging, seizure movies, and electroencephalograms (EEG) are all increasingly being interpreted using machine learning (ML) methods, especially deep neural networks. [8,9]
V. CONVENTIONAL DRUG DELIVERY SYSTEM [10-17]
1. Parenteral, Intravenous (IV) and Intramuscular (IM)
When oral delivery is not feasible, intravenous and intramuscular antiseizure medications (ASDs) are crucial for both replacement therapy and the treatment of clinical seizure situations. The parenteral formulations offer complete (intravenous) or almost complete (intramuscular) bioavailability along with quick administration. Intravenous preparations of the ASD allow for controlled delivery, but not intramuscular forms. In seizure situations, the first line of treatment is usually an intravenous or intramuscular formulation of lorazepam, diazepam, midazolam, or clonazepam. In the pre-hospital context, recent research also supports the use of intramuscular midazolam as being simpler than intravenous lorazepam delivery. Intravenous forms of valproic acid, levetiracetam, and lacosamide are other medications used for acute seizure situations. Status epilepticus's (SE) relative efficacy hasn't been sufficiently assessed, though.
2. Rectal administration:
Since it avoids first-pass metabolism and distribution, rectal drug delivery is a good substitute for oral and parenteral modes of administration for protein-peptide medications. Drug therapy can be administered both locally and systemically thanks to rectal delivery. For patients who are unconscious or unable to swallow, the rectal drug delivery device is a helpful substitute for the oral route of administration. When pharmaceuticals or treatments are administered through the rectum for either local or systemic effects, this is referred to as rectal drug delivery. Rectal medication delivery systems are one kind of mucosal adhesive drug delivery method. These methods offer both an efficient carrier and mucoadhesion, or the drug's attachment to the mucosal membrane.
3. Buccal administration- buccal midazolam (pediatric)
Buccal delivery is the process of administering a medication through the oral cavity's buccal mucosal membrane lining. Because the buccal region of the oral cavity has some distinct benefits over all other routes, it is a compelling target for the drug of choice's administration. But for medications that must pass through a strict first-pass metabolism in the mucosal lining of the mouth cavity, the buccal route works well. Buccal drug delivery is an intriguing and viable alternative for the non-invasive delivery of powerful peptide and protein therapeutic molecules. It is also a promising field for future research aimed at systemic distribution of oral ineffective medications. Buccal formulations are used to treat both local and systemic disorders. They are placed in the mouth between the cheek and upper gingival (gums). A benzodiazepine called oromucosal midazolam (BuccolamTM) is authorised for the treatment of paediatric patients experiencing acute, protracted convulsive seizures. In order to produce neuronal inhibition, midazolam increases the effects of γ-aminobutyric acid (GABA) on GABA(A) receptors. Because of its quick absorption via the buccal membrane and high lipophilicity, oromucosal midazolam has a quick start (less than 10 minutes) and a brief duration of action (defined by the short elimination half-life of midazolam and its active metabolite). Compared to oral midazolam, the drug's bioavailability is better when administered orally because it avoids first-pass hepatic metabolism. In paediatric patients with acute convulsive seizures, oromucosal midazolam appears to be as well tolerated as rectal or intravenous diazepam formulations and is at least as effective in stopping seizures.
4. Nano therapy
Millions of individuals worldwide suffer with epilepsy, a complicated neurological condition marked by frequent seizures. Due to issues like blood-brain barrier (BBB) impermeability, multidrug resistance, and complex epileptogenesis, a considerable percentage of patients continue to be resistant to traditional antiepileptic medications (AEDs) despite advancements in medication therapy. By increasing drug delivery across the blood-brain barrier, improving target specificity, and reducing systemic adverse effects, nanotechnology presents viable ways to get over these obstacles. In addition to discussing the design principles, mechanisms of action, and treatment efficacy of these nanodelivery systems, this review examines current developments in many novel approaches to epilepsy therapy. We also go over the obstacles and restrictions that prevent the clinical application of treatments for epilepsy based on nanomedicine.
5. Extended release:
Many antiepileptic drugs (AEDs) have short half-lives with large fluctuations in peak-to-trough plasma concentrations. Consequences of these pharmacokinetic (PK) properties may include adverse events (AEs) and breakthrough seizures, potentially leading to poor adherence. To address these challenges, newer formulations of these AEDs have been developed using unique extended-release (ER) technologies. These technologies extend the dosing interval such that dosing frequency can be minimized, which may improve patient adherence.
6. Nasal Diazepam nasal spray
The use of benzodiazepines as rescue medication in the management of ARS can help reduce healthcare-related expenses in patients due to decreased emergency room visits. Once delivered into the central nervous system, benzodiazepines are shown to be e ective against a wide range of seizures with a rapid onset of action and thus can reduce emergency room visits. Intranasal diazepam has found a niche in alternate out-of-hospital rescue therapies of ARS, as several studies have demonstrated its undeniable positive e ect on ARS. Diazepam nasal spray demonstrated an acceptable safety profile with less variation in the bioavailability compared with the rectal route. Onthe basis of pharmacokinetic results, tolerability and safety, diazepam nasal spray has the potential to be a game-changing treatment in acute radiaton syndrome (ARS).
7. Transdermal / Topical drug delivery
Transdermal method of medication administration circumvents the drawbacks of oral drug delivery, it is beneficial. Painlessness, avoiding first-pass metabolism and irregular absorption, controlling drug release rate, facilitating therapy termination, and enabling self-administration and sustained drug release with a single application are some of the benefits of the percutaneous method. benefits of this drug delivery method, only 20 active pharmaceutical compounds are utilized in transdermal patches for clinical application. This is due to the skin's very robust barrier that prevents drugs from penetrating the body. The structure and components of the skin make it difficult for medication molecules to be transported percutaneously through the skin. In addition to protecting internal organs, the human skin allows for minimal medication absorption through its surface.
VI. UTILIZATION OF AI IN EPILEPSY MANAGEMENT
1. Epilepsy detection and prediction
Seizures alter the rhythm and frequency of brain activity, and these signal records are reasonably priced. As a result, EEG is commonly used as the main signal to detect epileptic seizures . Therefore, this research solely focuses on the EEG approach for collecting brain signals because of its immense popularity and widespread application. Electrodes on a head-mounted headset are in charge of detecting brainwaves, allowing EEG signals to be recorded. EEG data is analyzed and transformed into commands for an output device for the intended action using a computer-oriented system called Brain-Computer Interface (BCI). We can quickly identify and anticipate seizures by gathering EEG data and translating it into commands. Over the years, a number of researchers have addressed seizures using ML-based prediction and detection techniques. [18]
2. Personalized treatment plans
More precise detection, prognosis, and individualized treatment regimens are made possible by AI technologies. algorithms for seizure detection powered by AI. ML is particularly useful in the healthcare industry for data analysis, including seizure prediction and EEG signal pattern recognition, which enables proactive management and improves patient safety. As ML models are exposed to additional data, their accuracy increases, in contrast to classical AI, which could rely on rule-based systems. DL has the potential to revolutionize personalized medicine by enabling AI to more precisely customize treatment regimens by utilizing patient-specific data, such as clinical profiles, genetic markers, and prior treatment outcomes. This individualized method can minimize adverse effects and enhance patient results by reducing the trial-and-error procedure usually involved in choosing anti-seizure medications (ASMs), particularly in cases that are refractory.
3. Optimizing of drug delivery system
Precision or personalised medicine aims to customise the best treatment approach for each individual with epilepsy. Medical decision-making about epilepsy has also made use of AI and machine learning approaches. Additionally, machine learning algorithms have been tried to anticipate how each patient will react to a particular prescription by using information from genetic profiles, EEG profiles, and drug dispensing databases. The application of AI to enhance EEG-guided management is the subject of ongoing study. ASMs have varied pharmacokinetics and pharmacodynamics as well as restricted therapeutic indices and substantial hazards. Population-level analyses are used to generate guidelines for the use of ASM in epilepsy and seizures Individualised therapy is known to be important, but it can be difficult to implement in practice, especially for critically sick patients with altered physiology. Additionally, despite the lack of clear benefits, intensive management of electrographic seizures and periodic and rhythmic patterns is frequently used. [19,20]
4. Monitoring and managing side effects
Epilepsy seizures can significantly impact an individual's daily life, relationships, and overall well-being. Hence, recognizing the nature of these seizures, their triggers, and available management strategies to provide appropriate support and care for individuals living with epilepsy are essential. However, the challenges of epileptic prediction and seizure detection based on EEG dataset remain. Adding remote monitoring in digital care pathways for epilepsy allows for continuous observation of patients in their natural environments, providing a more comprehensive understanding of seizure patterns compared to traditional in-hospital visits. This can lead to more timely and accurate adjustments in treatment plans, improving seizure control and quality of life for patients. The primary benefits of remote monitoring include improved seizure management, enhanced patient safety, and increased patient autonomy. Remote monitoring systems can alert caregivers and medical professionals to seizure events in real time, potentially reducing the response time during emergencies. [21]
5. Enhancing patient adherence
AI tools, including machine learning algorithms and neural networks, have demonstrated significant promise in enhancing diagnostic accuracy and identifying epileptic patterns. This study explores various AI-driven educational platforms designed to improve the knowledge and skills of healthcare professionals, patients, and caregivers in managing epilepsy. Moreover, AI applications in wearable devices and mobile health platforms facilitate real-time monitoring and patient engagement, ultimately improving quality of life. However, integrating AI into clinical practice presents several challenges, including the need for large and high-quality datasets, interdisciplinary collaboration, data privacy, and ethical considerations. Mobile applications are well-recognized and popular modes of enhancing self-management in PWE. [22]
6. Predicting Treatment outcomes:
Combinations of prognostic variables are called prediction models, and they are used to calculate the likelihood of a particular outcome. Prediction models, which have been developed with and verified on large cohorts, enable the estimation of individual patient outcomes using a rigorous statistical framework. Prognostic and diagnostic models are frequently used in the treatment of epilepsy, and given the complexity of epileptic processes, the main advantage of multivariable models (as opposed to using univariable factors for prediction) is accuracy. In epilepsy, single biomarkers—quantifiable characteristics that indicate regular biological processes—are believed to be insufficiently robust and granular to enable clinical use. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) recommendations provide a systematic approach to the creation and reporting of prediction models. [23]
7. Supporting surgical planning
When a clearly defined epileptogenic zone can be successfully excised or detached, surgery is the most economical choice for individuals with drug-resistant focal epilepsy. For epilepsy surgery to be successful, the Seizure Onset Zone (SOZ) evaluation is essential. Computer-assisted techniques are being used more and more to improve accuracy. Artificial intelligence plays a significant role in EEG for epilepsy surgery, helping to pinpoint seizure foci with greater precision, safety margin, and surgical efficiency. Better epilepsy localization using sophisticated imaging and electrophysiological has been the main focus of efforts to enhance results. The scope and depth of presurgical tests have increased dramatically. Due to the lack of available data, machine learning approaches have been used primarily to detect SOZ in iEEG or Stereo electroencephalography (SEEG, a kind of iEEG). By integrating IEEG or SEEG with robotic devices and multimodal planning tools, epilepsy surgery teams can improve surgical accuracy, efficiency, and safety margins. [24]
8. Enhancing caregiver support
By enhancing seizure safety, lowering caregiver hypervigilance, and lowering seizure fear, seizure detection systems may enhance HR-QOL. The aspects that make detection devices more acceptable to individuals with epilepsy and their caretakers have been better understood as a result of emerging data. These gadgets aim to improve health-related quality of life (HR-QOL) and lessen the unpredictability associated with epilepsy by automating seizure detection. By allowing caregivers to assist the individual during and after the seizure—for example, by giving rescue medication—or to call for assistance if the seizure progresses into status epilepticus or a seizure cluster, devices that notify caregivers when seizures are occurring may also help to promote seizure safety. Patients and caregivers utilize SeizureTracker.com, one of the biggest seizure diary databases in the world, to document clinical seizures in their patients. [25]
VII. Advantages [26]
1. Improved classification and diagnosis of seizures: Electroencephalogram (EEG) data can be analysed by AI algorithms, especially deep learning models, to find minor patterns that could be signs of seizures. These models have a high degree of accuracy in classifying different kinds of seizures, even complex and uncommon ones. For example, using stereo EEG data, a study created a Graph Neural Network (GNN) model that predicted seizure freedom outcomes with 92.4% accuracy.
2. Real-Time monitoring and wearable device: Wearable technology driven by AI is able to track physiological data continuously and identify seizure activity in real time. These gadgets can improve patient safety and quality of life by instantly alerting caregivers.
3. Personalized treatment planning: Through the analysis of enormous volumes of patient data, such as pharmaceutical responses, genetic factors, and lifestyle variables, AI can help clinicians create individualized treatment plans. This strategy makes customized treatments possible, enhancing seizure control and reducing adverse effects.
4. Forecasting and predicting seizures: By examining patterns in EEG data, AI systems are able to anticipate upcoming seizures.
5. Educational tools and awareness: AI-driven apps, like the Tele-ESSI app created by AIIMS Nagpur, teach educators, parents, and medical professionals how to recognize and treat seizures through animated movies. The goal of this project is to make schools safer and more welcoming for kids with epilepsy.
VIII. Disadvantages [27]
1. Transparency and Interpretability: Many AI systems, particularly deep learning models, behave like "black boxes," making it challenging for medical professionals to comprehend the decision-making process. Clinical adoption and trust may suffer as a result of this lack of openness.
2. Insufficient Medical Compassion: Empathy, which is essential for patient care and fostering trust in the doctor-patient connection, cannot be expressed by AI. Compassionate, comprehensive care may be hampered by this absence.
3. Expensive and Requiring Training: The cost of purchasing and maintaining AI tools is high. Additionally, using them necessitates specialized training for medical personnel, which can put a burden on resources.
IX. FUTURE SCOPE
There are several opportunities for future study and clinical innovation due to the development of EEG in the treatment of juvenile epilepsy. The potential to anticipate the onset of epilepsy in high-risk populations is presented by the continuous improvement of scalp EEG techniques. Clinicians may soon be able to recognize epileptogenic patterns earlier thanks to quantitative and AI-driven algorithms that are increasingly parsing complex EEG data in real time. This would allow for the development of individualized treatment plans based on each child's particular electroclinical profile and preventative therapeutic interventions. To create a thorough framework for comprehending juvenile epilepsy disorders, future studies should also investigate the integration of multimodal diagnostic techniques, which combine EEG results with genetic, imaging, and neurodevelopmental data. The significant new field that AI is revealing is neurogenetics. Opportunities for AI discovery and related targeted neurogenetic therapeutic interventions are made possible by recent developments in the field of genomics and the growing amounts of genetic data that are now available. [28,29]
CONCLUSION
The use of AI in the treatment of epilepsy represents a paradigm change in both diagnosis and treatment. AI improves patient safety, treatment compliance, and general quality of life by facilitating accurate seizure detection, predictive modeling, and customized medication delivery. The range of individualized care is further expanded by wearable technology, smartphone health apps, and AI-assisted surgical planning, while caregiver support platforms enhance real-time seizure response. Not withstanding these encouraging developments, there are still many obstacles to overcome, including the interpretability of AI models, high implementation costs, a lack of high-quality datasets, and ethical issues. It is crucial to address these problems through patient-centered research, policy support, and interdisciplinary collaboration. AI-driven tactics have the potential to transcend the drawbacks of traditional therapeutic modalities and usher in a new era of precision medicine in the treatment of epilepsy, provided that they are further developed.
Author’s Conflicts: No conflicts of interest.
REFERENCES




Shardul Kalyankar, Rutika Raghav, Rushikesh Powar, Shrirang Patil, Sohil Shaikh, Artificial Intelligence in Neurology: Emerging Applications for Epilepsy Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2485-2496. https://doi.org/10.5281/zenodo.18667521
 10.5281/zenodo.18667521
10.5281/zenodo.18667521