Department of Pharmaceutics, Late. Adv Dadasaheb Chavan Memorial institute of Pharmacy, Masur, 415106, MS, India
The biological process of wound healing is complex and dynamic, controlled by inflammation, oxidative stress, and the requirement for coordinated tissue regeneration. Complex and chronic wound treatment is still a major therapeutic challenge that calls for cutting-edge materials and creative fabrication techniques. This study focuses on new bioprinting technologies, including 3D and 4D bioprinting, and how they might be combined with innovative biomaterials to produce synthetic tissue structures and next-generation wound dressings. Among these, pectin and hydrogels have attracted interest because of their inherent antibacterial, anti-inflammatory, and biocompatible qualities. The adaptable polysaccharide pectin has shown remarkable promise in 3D-printed hydrogels, films, and scaffolds designed for individualized wound care. Furthermore, Nano clay-reinforced chitosan (CS/HNTs) hydrogels address important issues in the treatment of infected and irregular wounds by providing enhanced mechanical strength, shear-thinning behavior, and hemostatic efficiency. Tissue regeneration is accelerated by the exact spatial organization of cells and bioactive molecules made possible by the combination of smart biomaterials and sophisticated bioprinting. All things considered, these developments demonstrate the revolutionary potential of bioprinting in tissue engineering and regenerative wound care, opening the door for clinically viable, bio functional, and adaptable wound-healing therapies
After an injury, the body repairs damaged tissue and restores anatomical morals through a complex, natural biological process called wound healing. This process involves a number of overlapping cellular, molecular, and humoral events that take place in four main phases: hemostasis, inflammation, proliferation, and remodeling. Wounds that do not heal in three months are frequently classified as chronic, and unlike acute wounds, chronic wounds do not heal in a predictable amount of time or in an organized series of stages, Although many wounds are treated in a standard hospital wound-healing clinic, almost all chronic wounds have a basic cause that can be primarily attributed to one of three clinical groups. Pressure ulcers, also referred to as bed sores, diabetic foot ulcers, and arterial leg ulcers—all of which are commonly caused by arterial deficiencies— In the United Kingdom, leg ulcers are a prevalent chronic wound that affects 0.3% of adult males and 8.3% of males aged 85 and above. However, venous illness, which damages the leg's superficial and/or deep venous systems and results in venous hypertension and decreased blood flow, is present in over 70% of cases.1 The part that infections and oxidative stress play in inadequate tissue regeneration The processes of oxidative stress, infection, and inadequate tissue regeneration are interrelated; infection fuels oxidative stress, which in turn destroys cells and tissues, impairs the body's capacity to heal, and results in chronic, non-healing wounds.2 A sustained excess of reactive oxygen species (ROS) destroys lipids, proteins, and DNA, which hinders the inflammatory response, cell proliferation, and the development of new tissue that is essential for healing, even if modest ROS are required for signaling and battling infection.3
2. An Overview of the Healing Process and Wound Pathophysiology
Wounds can be categorized as either acute or chronic based on how long they take to heal. Acute wounds often heal in a reasonable amount of time, though some circumstances may cause the healing process to take longer. A number of factors, including various diseases, environmental conditions, nutrition, and increased bacterial loads that impair the immune system, can cause chronic wounds to heal very slowly or not at all. Exudation, ongoing infection, and necrosis are physical indicators of chronic wounds, all of which add to the difficulty of treating and controlling these wounds. The four primary stages of the healing process are hemostasis, inflammation, proliferation, and remodeling. Vascular constriction, which decreases blood flow to the wound site, is the initial stage of the healing process.5 Platelet receptors in the blood engage with extracellular matrix proteins and adhere to blood vessel walls during the hemostasis phase. Following attachment, the platelet undergoes activation, which results in a conformational shift and the release of bioactive chemicals that improve coagulation. Coagulation stops bleeding and shields the blood environment from outside pathogens by forming a clot that contains fibrin, fibronectin, vitronectin, and thrombospondin. The inflammatory process starts as soon as the wound is hypostasized. Immune system agents target local microorganisms in an attempt to avoid infection. Vasodilation increases vascular permeability, which permits monocytes and neutrophils to gather in the wound site. In order to control wound closure, matrix deposition, and angiogenesis, keratinocytes, fibroblasts, macrophages, and endothelial cells begin to accumulate during the proliferative phase approximately three days after wound formation.6 Changes in mechanical stress, electrical gradients, hydrogen peroxide, pathogens, growth factors, and cytokines all cause keratinocytes to become activated. Angiogenesis takes place within the granulation tissue as the endothelial cells undergo a phase of fast expansion. Growth factors, cytokines, and chemokines are essential for the wound healing process because they integrate signals in cellular activities within the wound. However, a patient's illnesses may cause a reduction in the quantity of vascularity in the wound area, delaying the healing process. Wound dressings with active ingredients must be used in these situations. The components, microenvironments, and recovery duration of each type of wound might differ, despite the fact that all wounds go through identical healing stages. In order to shorten the time it takes for a wound to heal, a patient-specific wound dressing must be created, taking into account the type of wound.7
2.1. Dressings for Wounds
Traditional dressings like gauze, plasters, and cotton—items that shield the wound area from the elements and absorb excess exudate—are used to cover the wound as part of the conventional healing process. The disruption of both acute and chronic wounds during the removal of conventional bandages is one of the most significant factors that adversely impacts the healing process. Tissue damage and even hemorrhage could occur if the conventional dressing is removed from the wound. Serious side effects, like as potentially fatal infections, could also result from it. Conventional wound dressings are only advised for dry, clean wounds. They essentially work by keeping the wound dry and absorbing the fluid from it. Sadly, compared to contemporary wound dressings, which are capable of preserving the moist environment the wound needs, conventional wound dressings are inadequate.8 Unlike conventional wound dressings, newer ones include antibacterial materials or medicines to lower the bacterial load of the wound while still providing the proper humidity and temperature for the wound site. They also promote cell attachment because of their resemblance to the ECM structure. Additionally, to guarantee the release of active components to the wound region, active compounds including growth hormones, nutritional supplements, antibacterial agents, and other medications may be put into the matrix of the wound dressing. Modern dressings, in contrast to old ones, don't harm the area or cause bleeding when being removed.9
2.2. Bioprinted 3D Dressings for Wounds
Conventional wound dressings absorb exudate and provide physical protection for the wound. Compared to conventional wound dressings, modern ones made with 3D bioprinters contribute more to wound healing. The best wound dressings should give the wound the right temperature and moisture, promote angiogenesis, connective tissue synthesis, and epidermal migration, permit gas exchange, guard against bacteria, offer optimal adhesion to the wound, improve the debridement effect and weep enzyme accumulation, and be biocompatible.10 Composite wound dressings can be printed using a 3D bioprinting technique for these properties. The effectiveness of various bioinks (natural, synthetic, or composite materials) for repairing skin integrity and speeding up wound healing has been the subject of numerous investigations. Because they resemble real tissues, hydrogel-based bioinks are the most popular in the field of 3D-bioprinted wound dressings (Figure 1C). These materials have notable swelling capabilities and are insoluble in water due to a 3D hydrophilic polymer network of hydrogel made of homopolymers or copolymers.11
2.2.1. Wound Dressings Using Bioinks
Because it can print cells and biomaterials on the precise print path, 3D bioprinting has emerged as one of the most effective methods for creating wound dressings in recent years. Three elements determine how well bioink works: form accuracy, printability, and biocompatibility. These factors affect the ensuing tissue development process in addition to determining the bioink's effectiveness. For example, integrated cells release proteases when a material scaffold breaks down, starting a series of processes that eventually result in the creation of extracellular matrix proteins. The complex design of the developing tissue structure is greatly influenced by these proteins. The material's rheological properties, such as its capacity to be extruded at low pressures and to retain the required shape, also determine whether it is suitable for use as a bioink. Because of clinical and regulatory issues, the rheological behavior should also support cell survival if 3D bioprinting uses cells or bioactive substances. Antimicrobial wound dressings are categorized as unclassified items with the designation FRO (dressing, wound, medication) in accordance with FDA standards.12
2.2.2 Scaffold-Based Bioink
Biomimetic and functional tissue structures can be made using a scaffold-based bioink and 3D bioprinting technology. Scaffold-based bioink is a promising technology that has the potential to significantly advance tissue engineering and regenerative medicine due to its robust mechanical properties and ability to work with a variety of biomaterials. The initial cell density and potential for tissue self-assembly are the main drawbacks of scaffold-based bioink. Hydrogels are currently of interest for wound dressings because of their superior swelling and water absorption capabilities, as well as their biocompatibility and biodegradability.13
2.2.3 Bio-ink Free of Scaffolds
The scaffold-free method builds three-dimensional tissue architectures using basic building blocks such cell sheets, spheroids, or tissue strands, which are made up of cells and an extracellular matrix. This process minimizes the importance of cell migration and proliferation by utilizing these building pieces' innate capacity to interlace. As a result, the amount of time needed for tissue creation is significantly decreased. The ability of the scaffold-free technique to handle the complicated architectural complexity of delicate tissues and organs is a noteworthy advantage. The regulated assembly of heterogeneous building pieces that include a variety of cell types is how this accomplishment is made possible. However, this strategy also has certain drawbacks. First of all, the mechanical characteristics of the individual structural units are rather modest, which may make cells vulnerable to injury during manipulation.14
3. Bioactive Molecules and Growth Factors in Bioprinted Wound Dressings
By sending growth hormones and other bioactive compounds straight to the wound site, bioprinted wound dressings can actively influence tissue regeneration, making them more than merely passive coverings. These sophisticated structures, in contrast to conventional dressings, have the ability to regulate the release of therapeutic molecules at specific times and locations, resulting in a microenvironment that promotes all phases of healing, from remodeling to inflammation.15
3.1 VEGF: Constructing Blood Vessels
A steady supply of blood is necessary for new tissue. Vascular endothelial growth factor (VEGF) promotes the development of new blood vessels, which provide regenerated tissue with nutrients and oxygen. Research using diabetic wound models has demonstrated that VEGF-loaded dressings greatly enhance wound closure and speed up capillary development. Researchers can accomplish continuous, localized release of VEGF by incorporating it into hydrogel bioinks, providing tissues with just what they want over days to weeks as opposed to a rapid burst.15
3.2 PDGF: Enhancing Tissue Strength and Attracting Fibroblasts
Fibroblasts, the cells that deposit new extracellular matrix, are drawn to platelet-derived growth factor (PDGF), a naturally occurring signal. It has been demonstrated that PDGF-loaded bioprinted dressings improve granulation tissue production, leading to stronger and more durable repaired tissue. PDGF is progressively released when added to hydrogels, encouraging organized tissue regeneration as opposed to unchecked scar formation.16
3.3 EGF: Accelerating Skin Healing
Re-epithelialization, the last stage of wound closure, is accelerated by epidermal growth factor (EGF), which promotes keratinocyte migration and proliferation. Orderly keratinocyte migration and quicker skin barrier regeneration are supported by bioprinted structures that distribute EGF straight to the borders of wounds. When compared to untreated wounds, EGF-containing hydrogels have shortened healing durations and enhanced epidermal integrity in animal trials.17
Table 1. Key Growth Factors and Bioactive Molecules in Bioprinted Wound Dressings
|
Molecule |
Role in Healing |
Stage of Wound Healing |
How It’s Delivered via Hydrogel |
|
VEGF |
Encourages the growth of new blood vessels, supplying oxygen and nutrients to regenerating tissue |
Proliferation |
Gradually released over time to support continuous angiogenesis |
|
PDGF |
Attracts fibroblasts and promotes extracellular matrix formation, strengthening new tissue |
Proliferation |
Slowly released to provide ongoing support for granulation tissue |
|
EGF |
Stimulates skin cells (keratinocytes) to grow and migrate, aiding in wound closure |
Remodeling |
Targeted delivery at wound edges to accelerate re-epithelialization |
|
Silver |
Acts as a broad-spectrum antimicrobial to prevent infections |
Inflammation |
Steady local release keeps bacteria under control without harming surrounding tissue |
|
Curcumin |
Combines antibacterial, anti-inflammatory, and antioxidant properties to protect the wound |
Inflammation |
Released slowly to continuously reduce inflammation and oxidative stress |
3. Biomaterials and Bioprinting Technologies
3.1 Droplet based bioprinting
Droplet-based bioprinting includes technologies like inkjet and micro-valve printing. The process of creating three-dimensional tissues using inkjet bioprinting (IJP) was first described in 1988. It involved altering commercial inkjet printers to use cell adhesive proteins, swapping out the print ink, and applying cell-laden sheets—three-dimensional biocompatible materials that contain living cells in a gel-like structure. There are three types of inkjet printing: continuous, drop-on-demand, and electrohydrodynamic.15 Thermal, electrostatic, and electrohydrodynamic methods are used to distribute polymer solutions in predetermined patterns on the build platform for inkjet bioprinting. While the printed material is being cured by light, UV, chemical enzymatic, or chemical polymerization, the ink is put into the cartridge that is attached to the print head. IJP has been used to print a variety of biomaterials, such as calcium phosphate, fibrin, gelatin, sodium alginate, poly (ethylene glycol), and dimethacrylate. Commercially available printers can be readily adjusted to provide high speed and good resolution for printed materials, making it an affordable technology. The use of bio inks with modest cell densities to prevent nozzle clogging and maintain cell viability is the main drawback.18
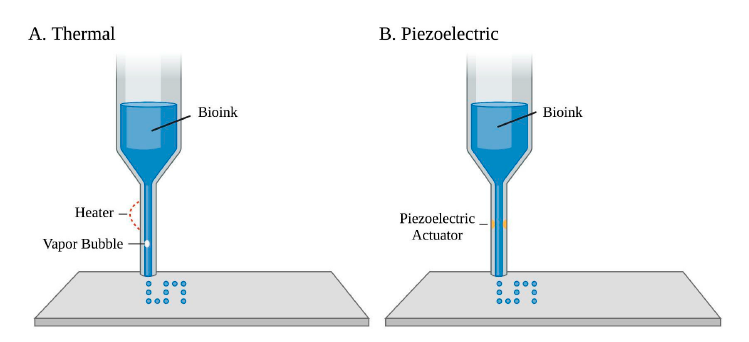
Figure.1: (A) Localized heating is used in thermal-based bioprinting to create vapor bubbles and eject ink droplets. (B) In piezoelectric-based bioprinting, droplets are produced by passing an electric current through a piezoelectric actuator.
3.2. Micro extrusion based bioprinting
Micro extrusion bioprinting controls the dispensed liquid volume and structure shape by depositing the ink using either a solenoid that uses an electrical pulse or a pneumatic device that applies pressured air. While cell viability reaches 80–97%, printed materials are crosslinked using methods similar to those used in inkjet. Better flexibility, scalability, and clinical translation are all made possible by micro extrusion for bio inks with higher viscosities and cell densities. Limited printing resolution and decreased cell viability as a result of applied pressure or nozzle blockage are some disadvantages, though. Furthermore, applying a lot of pressure might harm the integrity of the cells and reduce their vitality. This problem is solved by using polymers that exhibit shear-thinning behavior, which enhance printability and cause a viscus hydrogel to regenerate when shear tension is removed.19
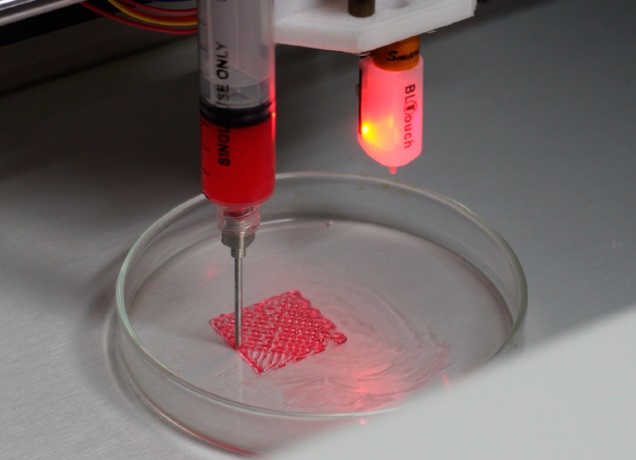
Figure.2: Testing of the 3D bioprinter with hydrogel.
3.3. Stereolithographic bioprinting
Stereolithography is a well-known technology comprises of various vat-photopolymerization techniques where photopolymerized liquid resins are radiated using a single laser beam, digitally projected UV-light source (DLP) or two-photon polymerization. The components of a standard SLA printer are a resin-filled tank, a perforated platform lowered into the tank, a light source, and a computer that controls the platform and glow source. When the resin cures and the laser scans the platform, a thin coating of the photopolymer is created. It is possible to print intricate structures with great resolution by repeating the process. The spot size of the applied laser beam affects resolution. SLA printers employ a top-down method when light exposures are from the bottom of the build platform, or a bottom-up method with light exposures from the top, as seen in figure. Cell-free or cell-laden microstructures have been created using a variety of photocurable polymers, including e-caprolactone, poly(ethylene glycol) diacrylate, poly(2-hydroxyethyl methacrylate), and di methacrylate.20
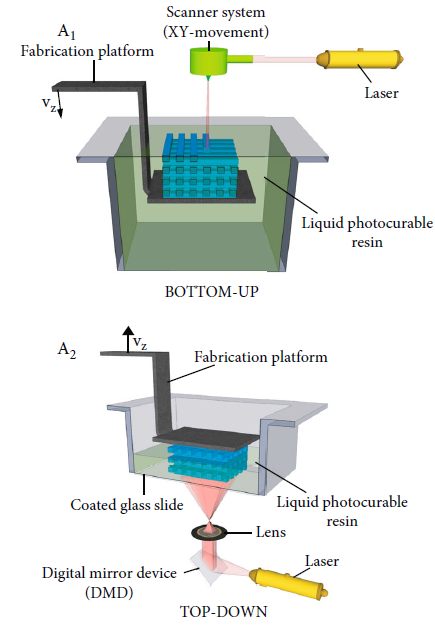
Figure.3: Scheme illustrating top-down and bottom-up approaches in stereolithography
3.4 Microfluidic Methods for 3D Bioprinting
A microfluidic chip contains tiny channels embedded in materials like glass, silicon, or PDMS. These channels connect to external inlets and outlets that allow controlled injection and removal of fluids or gases. Microfluidic chips are widely used in lab-on-a-chip (LOC) systems, cell biology research, and protein crystallization. A new fabrication approach uses simple household tools and a standard desktop 3D printer, making microfluidic chip production cheaper and easier compared to traditional expensive methods.21 This greatly improves accessibility for research, education, and rapid prototyping of point-of-care (POC) diagnostic devices. 3D printing is increasingly transforming microfluidics by reducing cost and complexity. Several breakthroughs have demonstrated its potential:
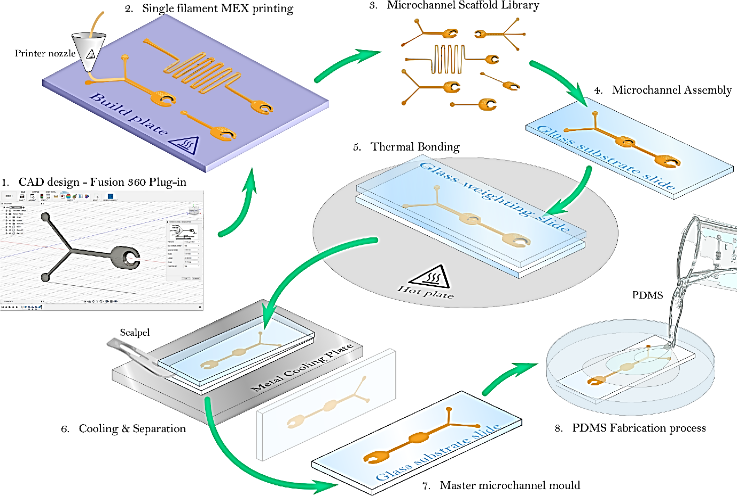
Figure.4: Microfluidic master mould fabrication process.
Table 1. Overview of bioprinting techniques used in wound healing and skin tissue engineering
|
Bio printing Technique |
Printing Resolution |
Cell Viability |
Commonly Used Bioinks / Materials |
Main Strengths |
Key Challenges |
Typical Applications in Wound Healing |
|
Inkjet bioprinting |
High |
Moderate |
Low-viscosity hydrogels such as alginate, gelatin, and collagen |
Simple setup, low cost, rapid and contact-free printing |
Limited to dilute bioinks; risk of nozzle clogging |
Formation of epidermal layers and treatment of superficial wounds |
|
Extrusion-based bioprinting |
Moderate |
High |
Alginate, GelMA, chitosan, and composite hydrogels |
Supports high cell density and a wide range of bioinks |
Lower printing resolution; shear stress may affect cell behavior |
Full-thickness skin constructs and chronic wound repair |
|
Stereolithography (SLA) |
Very high |
Moderate |
Photocurable polymers such as PEGDA and GelMA |
Enables precise and well-defined 3D structures |
Possible UV-related cytotoxicity; limited material choices |
Fabrication of structured skin and micro-architectures |
|
Microfluidic bioprinting |
High |
High |
Multicomponent and gradient-based bioinks |
Excellent control over cell placement and concentration gradients |
Complex device design and operation |
Vascularized and oxygen-gradient wound dressings |
|
Laser-assisted bioprinting |
Very high |
Very high |
Cell suspensions and ECM-based bioinks |
High precision with minimal cell damage; no nozzle blockage |
High equipment cost and limited scalability |
Precise placement of skin cells for advanced wound models |
|
Digital Light Processing (DLP) |
Very high |
Moderate to high |
Photocrosslinkable hydrogels |
Fast printing with high spatial accuracy |
Potential photoinitiator toxicity |
Layered skin and patterned wound scaffolds |
|
Electrospinning-assisted bioprinting |
Nanoscale fiber control |
High |
Synthetic and natural polymers (e.g., PCL, collagen blends) |
Closely mimics native extracellular matrix structure |
Limited control over thick 3D constructs |
ECM-like wound dressings and skin substitutes |
|
In situ bioprinting |
Moderate |
High |
Cell-laden hydrogels printed directly onto wounds |
Personalized treatment and direct wound coverage |
Sterility, portability, and clinical handling challenges |
Burn injuries and irregular wound surfaces |
|
4D bioprinting |
Technique-dependent |
High |
Stimuli-responsive smart bioinks |
Dynamic response to wound environment over time |
Still at an early research stage |
Smart wound dressings with adaptive healing behavior |
4. Cell Sources for Bioprinted Wound Dressings: Translational Aspects and Biological Functions
Tightly controlled interactions between various cell populations that coordinate inflammation, tissue creation, vascularization, and remodeling are necessary for successful wound healing. By allowing the spatially controlled deposition of various cell types within biomimetic bioinks, bioprinting provides a special benefit that replicates the hierarchical architecture of natural skin tissue. Keratinocytes, fibroblasts, endothelial cells, and mesenchymal stem cells (MSCs) are the most commonly used cell sources in bioprinted wound dressings, each of which contributes unique biological activities to the wound healing cascade.23
4.1 Keratinocytes
About 90% of epidermal cells are keratinocytes, which are the main forces behind re-epithelialization during wound healing. Keratinocytes experience phenotypic flipping following damage, which is marked by increased production of integrins and matrix metalloproteinases (MMPs), improved migratory behavior, and cytoskeletal remodeling. These modifications allow keratinocytes to re-establish the epidermal layer by migrating over temporary matrices.To maintain cell viability and encourage quick surface coverage, keratinocytes are frequently printed as the top epidermal layer in bioprinted wound dressings utilizing low-viscosity bioinks. Their incorporation limits microbial invasion, decreases transepidermal water loss, and speeds up barrier regeneration. However, during extrusion-based printing, keratinocytes are extremely sensitive to mechanical stress and shear pressures, therefore printing parameters and bioink rheology must be carefully optimized.24
4.2 Fibroblasts.
By generating extracellular matrix elements such collagen type I and III, elastin, fibronectin, and proteoglycans, fibroblasts are essential to skin regeneration. By differentiating into myofibroblasts under the influence of transforming growth factor-β (TGF-β), they are also in charge of wound contraction. Fibroblasts are usually incorporated in hydrogel matrices that replicate the natural skin milieu in bioprinted constructions. Epidermal stratification and maturation are greatly improved by their paracrine signaling contact with keratinocytes. Additionally, fibroblast-rich bioinks enhance long-term tissue remodeling and aid in the mechanical strengthening of the wound dressing. However, fibrosis and hypertrophic scarring can result from excessive fibroblast activity, underscoring the significance of regulated cell density and spatial organization.25
4.3 Endothelial Cells
Angiogenesis is a crucial factor in determining the effectiveness of wound healing, especially in chronic wounds with reduced perfusion and hypoxia. In the wound bed, endothelial cells migrate, multiply, and assemble into capillary-like structures to start the development of new blood vessels.The creation of pre-vascularized networks is made easier by the structured deposition of endothelial cells into hydrogels made possible by bioprinting. These networks improve graft life after implantation, speed up tissue integration, and facilitate the diffusion of nutrients and oxygen. Through synergistic signaling involving angiopoietins and vascular endothelial growth factor (VEGF), co-printing endothelial cells with fibroblasts or MSCs has been demonstrated to further solidify vascular architecture. Despite these benefits, inadequate perfusion during the early phases of healing makes it difficult to maintain long-term endothelial cell activity in printed structures.26
4.4 Mesenchymal stem cells
Mesenchymal stem cells' capacity for multipotent differentiation and potent immunomodulatory effects have made them one of the most attractive cell sources for bioprinted wound dressings. MSCs secret a wide range of cytokines, chemokines, and growth factors, including VEGF, hepatocyte growth factor (HGF), and fibroblast growth factor (FGF), and they predominantly affect wound healing by paracrine signaling rather than direct differentiation. MSCs regulate the inflammatory response, encourage angiogenesis, boost fibroblast proliferation, and improve epithelial regeneration when added to bioprinted hydrogels. MSCs are especially beneficial for chronic and non-healing wounds because they also inhibit excessive scar formation and minimize oxidative stress. However, problems with cell procurement, expansion, donor variability, and regulatory licensing still prevent them from being widely used in clinical settings.27,28
Table 2. Key cell types used in bioprinted wound dressings and their roles in skin repair
|
Cell Type |
Role in the Wound Healing Process |
Contribution to Bioprinted Constructs |
Practical Considerations |
|
Keratinocytes |
Restore the epidermal layer and re-establish the skin barrier |
Enable rapid surface coverage and promote re-epithelialization |
Sensitive to shear stress during printing; require gentle printing conditions |
|
Fibroblasts |
Produce extracellular matrix and support wound contraction |
Strengthen the dermal layer and improve structural stability |
Excessive activity may lead to fibrosis or scarring |
|
Endothelial cells |
Drive angiogenesis and improve blood supply |
Support formation of microvascular networks within the construct |
Maintaining long-term vascular function remains challenging |
|
Mesenchymal stem cells (MSCs) |
Regulate inflammation and stimulate tissue regeneration |
Enhance healing through paracrine signaling and reduced scarring |
Issues related to sourcing, expansion, and regulatory approval |
5. Bioprinted Wound Dressings' Clinical Translation: Linking Research and Practice
The use of bioprinting in ordinary clinical practice is still in its infancy, despite its impressive potential for wound healing in lab settings. Only a small number of research have advanced to human use, with the majority of bioprinted wound dressings being assessed in preclinical animal models or in vitro systems until now.29
5.1 Current Research in Clinical and Translational Settings
The requirement for quick and efficient skin regeneration is greater in burn injuries and full-thickness skin wounds, which have been the main focus of early translational efforts. In situ bioprinting, which prints autologous keratinocytes and fibroblasts directly onto wound surfaces, is one of the most noteworthy developments.29 when compared to traditional therapies, preclinical research employing pig wound models showed enhanced collagen structure, decreased scar formation, and quicker wound closure. Strong proof-of-concept for clinical feasibility was shown by these results.30
The feasibility and safety of printing cell-laden structures directly onto human wounds have been further validated by early pilot clinical investigations employing portable or handheld bioprinters. However, small patient numbers, brief follow-up periods, and wound type diversity typically restrict these investigations. Because of this, even while the results are promising, there is still not enough solid clinical data to encourage widespread adoption.31
5.2 The difference between in vitro and in vivo success
The disparity between the diverse biological environment of human wounds and controlled laboratory conditions is a significant barrier to clinical translation. High cell vitality, outstanding structural integrity, and potential regeneration indicators are frequently reported in vitro. On the other hand, a variety of factors, including inflammation, infection, decreased blood flow, mechanical stress, and patient-specific disorders including diabetes and vascular disease, affect actual wounds. Furthermore, the chronic and complex character of human wounds cannot be accurately replicated by widely used animal wound models. This disparity restricts the straightforward application of preclinical results and emphasizes the critical necessity for well-planned human clinical studies that more closely resemble actual clinical situations.31, 32
5.3 Regulatory and Ethical Issues
When using bioprinted wound dressings in therapeutic settings, ethical issues are crucial, especially when stem cells or genetically modified cells are involved. Long-term safety, donor permission, and cell sourcing concerns need to be carefully considered. Although therapeutically appealing, personalized bioprinted constructions nevertheless present issues with reproducibility, uniformity, and fair access.33 Because bioprinted items frequently incorporate living cells, biomaterials, and bioactive chemicals, they fall under the advanced therapy or combination product classifications, making them extremely difficult to regulate. Approval procedures are made more difficult by the absence of uniform regulatory frameworks created especially for bioprinting. Guidelines for sterility, quality control, and long-term safety evaluation are still being developed.34
5.4 Practical Considerations and Cost-Benefit Analysis
One major obstacle to clinical translation is still cost. Production costs for bioprinted wound dressings are increased by the need for specialized tools, knowledgeable workers, and lengthy cell culture processes. Personalized bioprinting has obvious therapeutic benefits, but its viability from an economic standpoint in comparison to current wound care techniques needs to be carefully considered.34 However, by reducing reliance on laboratories and facilitating point-of-care care, new technologies like automated printing systems and portable in situ bioprinters may contribute to cost savings. Bioprinting may eventually provide a good cost-benefit ratio if scalability and manufacturing efficiency can be increased, especially for complicated or non-healing wounds.35
5. Industry Adaptability of 3D Bioprinting
5.1. Sustainability
Materials can be recycled and repurposed thanks to three-dimensional bioprinting. In order to promote environmental sustainability, renewable resources are essential. Sustainable materials made from these resources have remarkably low energy and carbon footprints.39 by providing ecologically friendly production options, biopolymers play a crucial role in creating a connection between biomaterials and renewable reservoirs, which greatly enhances the sustainability of 3D bio printing. The materials used in 3D-bioprinted hydrogel dressings are intelligent and efficient biomaterials that can be synthetic (like synthetic fibers, peptides, and elastomers) or natural (like collagen, ALG, and gelatin). Synthetic hydrogels are more widely used in 3D bioprinting because of their better mechanical qualities, biocompatibility, and lower batch-to-batch variation, even though hydrogels of natural origin offer benefits like easy recognition of cellular growth factors and biomolecules as well as their natural degradation by the body.37 In addition to their intrinsic biocompatibility, which promotes and enhances cellular differentiation and proliferation, hydrogels have become increasingly popular in the field of tissue engineering. Conversely, conventional 3D printing frameworks make use of well-known hydrogel-based scaffold materials like ALG, GelMA, and ultra-short peptides, which allows for the creation of softer and more delicate tissue or even harder tissue structures. These essential characteristics characterize hydrogels as intelligent biomaterials that offer appropriate microenvironments for a wide range of cells that need specialized culture media, including neurons, chondrocytes, osteoblasts, and stem cells.38
5.2. Advancing
To ensure excellent quality, safety, and efficacy, therapeutic items need to be approved by regulatory bodies including Australia's Therapeutic Goods Administrative (TGA) agency, the US FDA, and the European Medicines Agency (EMA). Product usage without a license or consent from these authorities can result in major, potentially fatal risks. Even though 3D bioprinting technology has been thoroughly studied in recent years, it is still not fully developed due to a number of obstacles and limitations. These include the difficulty of developing a microvascular network in wound dressings during 3D bioprinting to supply nutrition to the wound area, as well as the difficulty of selecting a material and crosslinking mode appropriate for wounds in terms of physical, mechanical, and biological requirements.39 Good Manufacturing Practice (cGMP) guidelines must be followed when producing altered bioprinting goods, and sterility assurance requirements for microbiological testing must be included. It takes a long time, a lot of labor, and significant initial capital expenditures to produce a product that is clinically tested, ethically acceptable, and ready for the market. Due to the complexity of the process and strict regulations, these high initial capital expenditures can make it challenging to commercialize pricey bioprinting items. However, the cost of such bioprinting items must be evaluated indirectly, taking into account things like the total decrease in hospital expenses, length of stay, and number of reconstructive surgeries following severe burns, in addition to the cost per unit of manufacture. Until fundamental standards of care are met in the early phases of treatment, experienced.40
5.3 Durability and Lifespan
Dressings made of three-dimensional bioprinting are incredibly adaptable and may be tailored to meet the needs of wounds. However, the composition and structure of traditional dressings may not always precisely match the needs of the wound. The content, structure, and mechanical characteristics of the dressing can be accurately regulated using bioprinting.41 Dressings that are suited to particular wound types and healing stages can be created because of the technologies' versatility in utilizing various materials both separately and in combination as bioink. Because of their mechanical and physical resilience, dressings also serve the crucial role of adapting to the changing environment of a healing wound. The degradation of the dressing must coincide with the formation of new tissue in order to provide an efficient wound dressing. For example, before being applied in vivo, the hydrogels particularly selected for use in wound healing models must retain their structure for at least 14 days.42
5.4 Large-Scale Production
High material costs and technology constraints are the main things preventing 3D printing from being widely used. Additionally, this technique is only applicable in certain situations due to issues including the print's lack of accuracy, color, and surface quality. Nevertheless, the literature now in publication has listed a number of 3D printing's financial advantages in spite of these drawbacks. The research notes that energy consumption can be reduced for complicated parts, even while 3D printing technology lowers device needs by making the production stage more accessible. Additionally, this technology makes it possible to establish new supply chains for the creation of novel items. With 3D printing, configurations that are challenging or unfeasible with conventional manufacturing techniques become feasible. Additionally, 3D printing changes the battle for quality by basing the final product's quality on the viewpoint of the computer-based CAD file rather than the manufacturing method.43 In contrast to conventional manufacturing techniques, 3D printing reduces lead times through rapid output while optimizing economies of scale and scope. This strategy shortens supply chain times and further decentralizes production activity. According to this concept, the limitations and financial benefits of 3D printing technology combine to change production processes, and the commoditization of production infrastructure leads to the development of a larger ecosystem and greater production flexibility.44
6. CONCLUSIONS AND FUTURE POSSIBILITIES
The multiple signaling pathways and the synergistic interaction of numerous variables are essential to the complex process of wound healing. Hydrogel-based wound dressings have recently surfaced as viable options, offering the following advantages: creating an ideal environment for wound healing and accelerating the healing process. The capacity to create complex structures using medicinal chemicals, living cells, and personalized hydrogels allows bioprinting to precisely meet patient-specific requirements. Numerous studies have shown that current advancements in hydrogel-based dressings and the development of 3D bioprinting techniques can be used to improve wound closure, re-epithelialization, and angiogenesis without raising cytotoxicity issues. The development of specialized 3D printer configurations that are painstakingly calibrated to satisfy the particular requirements of specific patients has been the focus of recent advancements in 3D printing technology. These technological developments have led to the development of numerous novel techniques, such as advanced scanning systems, robotic mechanisms incorporated into 3D bioprinting applications, the smooth integration of artificial intelligence paradigms, and the groundbreaking use of bioinks for in situ bioprinting, which speeds up wound healing processes. Bioprinting methods with four, five, and six axes of motion suggest that complex three-dimensional structures might be easily created, requiring sophisticated treatment choices for wounds of various depths. The following issues need to be resolved before 3D-bioprinted dressings can be used in clinical settings:
REFERENCES


Pranali P. Yadav*, Omkar S. Jadhav, Prathamesh G. Aughade, Shreyas A. Shete, Alfiya A. Mulani, Bioprinting Innovations: A Review of Emerging Techniques for Tissue Regeneration and Wound Healing, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1956-1972. https://doi.org/10.5281/zenodo.18315467
 10.5281/zenodo.18315467
10.5281/zenodo.18315467
