
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,4 Sardar Patel College of Pharmacy, Vidyanagar Vadtal Road, Bakrol , Anand, Gujarat.
2,3 Sal Institute of Pharmacy, Ahmedabad, Gujarat
The COVID-19 pandemic, caused by SARS-CoV-2, affects virtually all organ systems, manifesting with respiratory symptoms (fever, cough, dyspnoea) as well as cardiovascular (myocarditis, arrhythmias), gastrointestinal (diarrhea, nausea), neurological (headache, anosmia, stroke), renal (acute injury, proteinuria), dermatological (rash, “COVID toes”) and other systemic features. Prevention efforts varied by setting: studies indicate that rural populations were significantly less likely than urban residents to adopt several key protective behaviours (e.g. mask use, disinfection, working from home). Vaccines have dramatically altered the course of the pandemic: mRNA (Pfizer–Biotech, Moderns), adenovirus-vectored (AstraZeneca, J&J) and inactivated (Sino vac, Sino pharm) vaccines were deployed globally, with initial efficacies of ~60–95% against early strains. However, immunity waned and viral variants (especially Omicron lineages) partially evaded protection, making booster doses (including updated bivalent vaccines) necessary to sustain defence. Diagnostic approaches evolved from early RT-PCR (gold standard) to rapid antigen tests and advanced point-of-care methods (CRISPR-based assays, biosensors) that offer rapid, sensitive detection. A subset of survivors (~6% globally) develops “long COVID” – a constellation of chronic symptoms (fatigue, cognitive impairment, dyspnea, etc.) lasting months, with risk factors including female sex, older age, obesity, and severe initial illness. Active variant surveillance remains crucial: major variants (Alpha, Beta, Delta, Omicron and its subline ages) have impacted transmissibility and vaccine/diagnostic performance. Finally, special populations such as children and pregnant women often exhibit distinct clinical courses: most pediatric cases are mild, but Multisystem Inflammatory Syndrome in Children (MIS-C) can be severe; pregnant patients face higher risks of severe COVID-19 but rare vertical transmission. This comprehensive review collates the latest evidence on these topics, integrating clinical studies, public health data, and authoritative guidelines to support pharmaceutical and clinical research.
SARS-CoV-2, a novel β-coronavirus identified in Wuhan, China in late 2019, has caused a global pandemic of unprecedented scale[3,9]. The virus primarily targets the respiratory tract (via ACE2 receptor binding) but can trigger systemic inflammation affecting multiple organ systems[3]. By mid-2025, over 770 million cases and >7 million deaths have been reported worldwide[12]. In response, enormous scientific effort has focused on understanding the virus’s pathogenesis, improving prevention, and developing diagnostics and therapies. Vaccines against SARS-CoV-2 were developed and authorized at record speed, transforming the epidemiology of COVID-19[4]. At the same time, nonpharmaceutical interventions (NPIs) like masking and distancing were implemented unevenly across different communities. Health behaviours varied between urban and rural areas; for example, rural residents in the United States were much less likely to wear masks or work from home compared to urban counterparts[3]. Meanwhile, testing technology rapidly advanced: initial reliance on laboratory RT-PCR tests evolved to include rapid antigen kits and novel CRISPR-based and biosensor diagnostics[9]. The pandemic also spurred intense genomic surveillance: multiple SARS-CoV-2 variants (designated by WHO as Variants of Concern such as Alpha, Delta, Omicron) emerged, challenging vaccines and diagnostics. Furthermore, awareness grew of “long COVID” – persistent symptoms long after acute illness – which affects a substantial minority of patients. Finally, it became clear that special populations (children and pregnant women) might experience COVID-19 differently, necessitating focused study.
This review systematically covers the clinical manifestations of COVID-19 by organ system; explores differences in prevention behaviours between rural and urban communities; analyses the impact and development of vaccines (including booster doses) on the pandemic; summarizes diagnostic strategies from RT-PCR to cutting-edge point-of-care tests; examines the emerging understanding of long COVID (its prevalence, symptomatology and risk factors); surveys variant surveillance efforts and the implications of major viral mutations; and highlights the clinical characteristics of COVID-19 in pediatric and pregnant populations. We draw on the latest peer-reviewed literature and public health reports (WHO, CDC, etc.) through 2025 to provide a comprehensive, up-to-date synthesis suitable for pharmaceutical and clinical researchers[10].
Clinical Manifestations by Organ System
Respiratory system: COVID-19 most often presents with fever, cough, and dyspnea. These reflect viral pneumonia and lower respiratory tract infection. Radio logically, chest CT frequently shows bilateral ground-glass opacities and consolidation. In severe cases, acute respiratory distress syndrome (ARDS) can develop. The respiratory epithelium is a primary target due to high ACE2 expression. Importantly, some patients develop “silent hypoxemia” with severe lung involvement but relatively mild subjective dyspnea. Imaging is used to assess severity: while not diagnostic of SARS-CoV-2 per se, chest CT findings support clinical assessment when RT-PCR is pending.
Cardiovascular: SARS-CoV-2 can affect the heart and circulation via direct viral injury, systemic inflammation, or hypoxemia. Myocardial injury (elevated troponin) and arrhythmias are reported in up to 20–30% of hospitalized patients[15,16]. Cases of acute myocarditis and heart failure have been described. Patients with pre-existing cardiovascular disease face higher risk of severe COVID-19. In addition, COVID-19 is associated with a hypercoagulable state: thrombotic events (pulmonary embolism, stroke, arterial clots) can complicate infection. These arise from endothelial dysfunction, inflammation and immobilization. Clinically, chest pain and palpitations may occur; echocardiography in severe cases can show ventricular dysfunction. Hence, cardiac biomarkers and monitoring are often indicated in moderate-to severe cases[6].
Gastrointestinal (GI): GI symptoms are common, reflecting ACE2 expression in the gut. Up to 20–30% of patients report anorexia, nausea, diarrhea, or abdominal pain. In some cohorts, GI symptoms preceded respiratory ones or were the only manifestations in a minority. Viral RNA has been detected in stool, raising the possibility of fecal-oral spread. Liver enzyme elevations (AST/ALT) occur in many hospitalized patients, possibly from viral hepatitis, systemic inflammation, or drug toxicity. Endoscopy units have adopted precautions given reports of viral RNA in GI secretions[12].
Neurological: COVID-19 impacts the nervous system in multiple ways. Common symptoms include headache, anosmia (loss of smell), ageusia (loss of taste), dizziness, and confusion. More severe neurologic complications have been reported: encephalopathy, seizures, stroke (ischemic and hemorrhagic) due to coagulopathy, and peripheral neuropathies. A peculiar feature is the frequency of anosmia/ageusia, often early in disease. The virus may enter the CNS via olfactory nerves or through blood. Post infectious immune-mediated syndromes (Guillain–Barré syndrome, acute disseminated encephalomyelitis) have been described. MRI sometimes shows changes consistent with viral encephalitis. Overall, neuro-COVID manifestations underscore the broad organotropism of SARS-CoV-2[12].
Renal: Kidney involvement is common in hospitalized COVID-19. Acute kidney injury (AKI) occurs in 20–30% of severe cases, driven by direct viral cytotoxicity of tubular cells (rich in ACE2), systemic hypoxia, hypotension, and cytokine storm. Proteinuria and hematuria at presentation predict worse outcome. Some patients require renal replacement therapy. Autopsy studies have found viral particles in podocytes and proximal tubule cells, as well as evidence of microthrombosis in renal vessels. Thus, routine monitoring of renal function is advised in moderate/severe illness[11].
Dermatological: While less common than other manifestations, various skin findings are reported. These include maculopapular rash, urticaria, and the so-called “COVID toes” (chilblain-like lesions on acral surfaces). The latter are especially seen in younger patients or as a late phenomenon, possibly representing immune-mediated vasculopathy. Vascular skin lesions (livedo reticularis, acral ischemia) occur in severe disease and may indicate coagulopathy. Overall, cutaneous signs are non-specific but can alert clinicians to COVID-19 in absence of respiratory symptoms[10].
Other systems: COVID-19 can also cause hematologic abnormalities (lymphopenia, neutrophilia, elevated D-dimer), and endocrine dysfunction (new-onset diabetes, thyroiditis). Musculoskeletal pain and arthralgias are frequent. Importantly, multisystem inflammatory syndromes (MIS) occur post-infection: MIS in adults (MIS-A) and children (MIS-C) feature fever, hyper inflammation, shock and multi-organ involvement (often cardiovascular, GI, skin) several weeks after acute infection. In children, MIS-C resembles Kawasaki disease and is often severe (abdominal pain, rash, myocardial dysfunction), with elevated inflammatory markers[10].
Table 1. Reported prevalence of key symptoms in COVID-19 by organ system (composite from clinical studies) [11-12].
|
System |
Common Symptoms/ Findings |
References |
|
Respiratory |
Fever, cough, dyspnea, pneumonia (GGO on CT) |
Mehta et al. (2021) |
|
Cardiovascular |
Chest pain, palpitations, myocarditis, clots |
Mehta et al. (2021) |
|
Gastrointestinal |
Anorexia, diarrhea, nausea, abdominal pain |
Mehta et al. (2021) |
|
Neurological |
Headache, anosmia, confusion, stroke |
WHO (Long COVID Fact Sheet) |
|
Renal |
AKI, proteinuria, hematuria |
Mehta et al. (2021) |
|
Dermatological |
Rash, urticaria, chilblains (“COVID toes”) |
Mehta et al. (2021) |
|
Systemic |
Lymphopenia, thrombosis, MIS-A/MIS-C |
Mehta et al. (2021) |
Note: GGO = ground-glass opacities; MIS = Multisystem Inflammatory Syndrome.
Rural vs. Urban Prevention Behaviours
Public health guidelines (masking, distancing, hand hygiene, vaccination) were central to controlling COVID-19 spread, yet adoption varied across communities. U.S. studies found significant rural–urban disparities: rural Americans were far less likely to engage in key preventive behaviours than urban Americans. For example, in a national survey (May–June 2020), 73.7% of rural respondents reported wearing masks in public versus 84.6% of urban respondents (a 10.9% absolute difference) [3]. Other behaviours (sanitizing home/workspace, avoiding restaurants, working from home) were similarly lower in rural areas. In logistic regression, rural residence predicted 49% lower odds of mask use and 49% lower odds of working from home, even after controlling for demographics. In contrast, hand washing and social distancing showed smaller rural–urban differences[11].
These patterns likely reflect multiple factors: rural populations may have perceived lower local COVID risk early in the pandemic, lower trust in public health messaging, and different political and cultural attitudes. Indeed, the same analysis found that trust in expert sources and political ideology strongly influenced preventive behaviours. Internationally, similar trends have been observed: a Chinese cross-sectional study reported that rural residents had significantly lower scores on prevention behaviours, intentions and knowledge compared to urban residents. Socioeconomic factors (education, internet access) also play roles. The rural–urban gap implies that targeted education and resource allocation (e.g. vaccine clinics, credible communications) were needed to mitigate disparities[12].
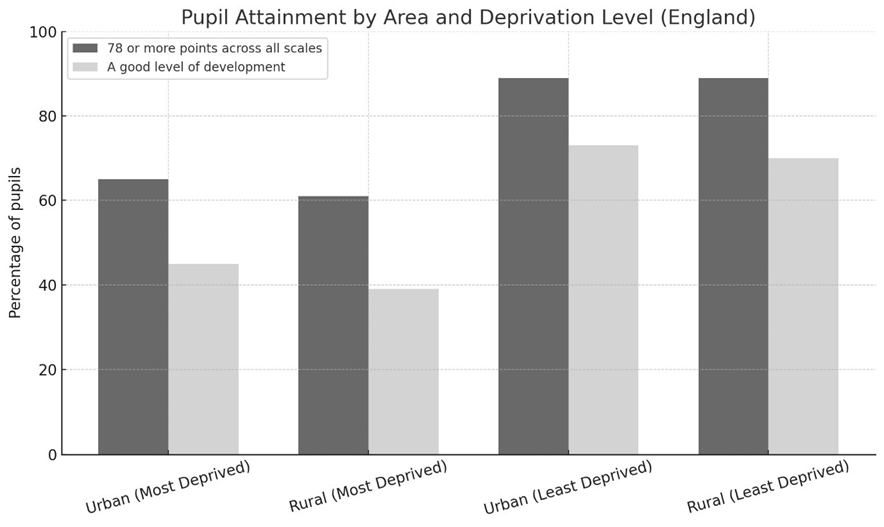
Figure 1 illustrates rural vs. urban rates for selected prevention behaviours from the U.S. survey[8].
The public health implication is clear: communities with lower uptake of NPIs were at higher risk for surges. A related finding is that rural Americans were also less likely to seek early testing or to trust official sources, potentially delaying diagnosis. Overall, this evidence underscores the need for regionally tailored interventions: a “one size fits all” strategy may fail if rural populations are less receptive to generic messages.
Vaccines: Impact and Evolution
Vaccination against COVID-19 has been the cornerstone of pandemic control. Three major vaccine platforms were deployed:
Table 2 summarizes key authorized vaccines and their reported efficacies:
Table 2. COVID-19 vaccines and their efficacy against original SARS-CoV-2 strains. (Real-world effectiveness and performance against variants vary; ongoing studies continue to refine these estimates.)
|
Vaccine (Developer) |
Platform |
Reported Efficacy (original strain) |
References |
|
BNT162b2 (Pfizer) |
mRNA (LNP) |
~95% |
Polack et al. NEJM 2020 (Pfizer trial) |
|
mRNA-1273 (Moderna) |
mRNA (LNP) |
~94% |
Baden et al. NEJM 2021 (Moderna trial) |
|
ChAdOx1 (AstraZeneca) |
Adenovirus |
~70% |
Voysey et al. Lancet 2021 (AZ trial) |
|
Ad26.COV2.S (J&J) |
Adenovirus |
~66% (single dose) |
Janssen trial (FDA report) |
|
CoronaVac (Sinovac) |
Inactivated virus |
~50–65% in trial (varied by study) |
WHO and trial reports |
|
NVX-CoV2373 (Novavax) |
Protein subunit |
~90% (trial) |
NEJM 2021 (Novavax trial) |
Early in 2021, these vaccines dramatically reduced COVID-19 incidence, hospitalization, and death, especially in high-income countries. By mid-2022, mass vaccination campaigns had averted millions of cases worldwide. Nevertheless, several challenges emerged:
Bivalent mRNA boosters (targeting Omicron BA.4/5 and ancestral spike) were developed in 2022–2023, improving protection against then-circulating strains. In late 2024, updated vaccines targeting JN.1 lineage were released. The CDC reported that the 2024–2025 vaccine (targeting Omicron JN.1 subline ages) provided moderate additional protection: ~33% effectiveness against emergency care visits and ~45% against hospitalization in adults≥18, compared to no booster.
Overall, vaccines have transformed the pandemic from an uncontrolled catastrophe into a state where severe outcomes are largely preventable. Booster doses are now part of routine COVID19 management: for example, CDC recommended a 2024–2025 booster for all adults, which was shown to reduce severe outcomes even against new variants. Future vaccines may target broader coronaviruses or utilize novel platforms (e.g., nasal vaccines to induce mucosal immunity). Pharmaceutical research continues to optimize formulations for longer durability and variant coverage[5].
Diagnostic Strategies
Timely and accurate diagnosis of COVID-19 is essential for patient care and public health measures. RT-PCR (reverse-transcription polymerase chain reaction) remains the gold standard for detection of SARS-CoV-2 RNA. PCR tests, usually performed on nasopharyngeal or saliva samples, have very high sensitivity and specificity when done properly. They can detect low viral loads but require specialized laboratory equipment and 1–2 days for results. During the pandemic, PCR capacity scaled up globally, but supply chain issues (reagents, swabs) occasionally limited access.
Antigen tests (rapid diagnostic tests, often lateral-flow assays) detect viral proteins and give results within minutes at point-of-care or at home. They are far less sensitive than PCR, especially for asymptomatic or early-infection cases. A positive antigen test reliably indicates infection, but a negative result does not rule it out. Public health agencies (e.g. FDA) have made numerous antigen tests available for home use. According to FDA guidance, laboratory based molecular tests are generally more accurate than home antigen tests. Antigen tests played a crucial role in rapid screening and self-testing, despite trade-offs in sensitivity.
Imaging: Chest imaging (radiography or CT) is not diagnostic of SARS-CoV-2 infection per se, but it helps evaluate lung involvement. CT scans early in the pandemic often showed bilateral ground-glass opacities even when PCR was negative. Radiologists developed reporting criteria for COVID-compatible pneumonia. However, CT has lower positive predictive value in low-prevalence settings and is mainly used for assessing severity or complications[9].
Emerging diagnostics: Novel technologies have been developed to improve speed, cost, or decentralization of testing. CRISPR-based diagnostics (e.g. SHERLOCK, DETECTR) use Cas12/13 enzymes programmed to recognize SARS-CoV-2 sequences. These systems can produce a fluorescent or colorimetric readout in under an hour without high-end equipment. They offer high sensitivity and specificity and can be lower-cost. For instance, Roaa Hadi et al. note that CRISPR assays for SARS-CoV-2 are “cost-effective, time-efficient, highly sensitive, and specific,” and do not require sophisticated instruments. Some CRISPR tests can even detect variants by targeting unique mutations. However, most are still in development or limited use due to regulatory and manufacturing hurdles.
Biosensors and point-of-care devices: Researchers have created electrochemical and microfluidic sensors for SARS-CoV-2. These include paper-based assays, wearable biosensors, and smartphone-based readers. While not yet widely used clinically, they hold promise for future outbreaks. For example, Cas13a-based fluorescence or Cas12a-based lateral-flow biosensors have been demonstrated to detect virus RNA with high sensitivity. Integrating these with mobile devices could enable rapid decentralized testing and surveillance.
In practice, COVID-19 diagnosis often involves a combination: symptomatic patients may do a rapid antigen test at home; if negative but suspicion remains, an RT-PCR is performed. Screening in hospitals and airports typically relies on rapid PCR devices. Serological (antibody) tests also exist but are used more for surveillance or research, not acute diagnosis.
Long COVID: Prevalence, Symptoms, and Risk Factors
Many patients experience a prolonged recovery after acute SARS-CoV-2 infection. The World Health Organization has defined post COVID-19 condition (PCC) – often called “long COVID” – as symptoms persisting or new onset at least 3 months after infection and lasting ≥2 months. WHO estimates that about 6 in 100 people with COVID-19 develop long COVID. Importantly, this figure mainly reflects infections from the pandemic’s early years, and preliminary data suggest the risk may be lower with Omicron-era infections, though evidence is still evolving. Nonetheless, because millions have been infected, long COVID represents a substantial public health burden[3].
The symptom profile is highly heterogeneous. Over 200 symptoms have been reported, but common features include:
WHO’s fact sheet notes that fatigue, breathlessness, pain, and sleep issues are particularly common. These symptoms can significantly impair daily functioning and work capacity. Notably, some patients developed new medical conditions post-COVID (kidney problems, heart disease, diabetes, mental health disorders) at rates above baseline.
Risk factors for developing long COVID have been identified: female sex and older age are associated with higher risk. Other factors include smoking, obesity, and pre-existing chronic diseases. Critically, the severity of the initial illness is a strong predictor: hospitalization or ICU admission markedly raises long-COVID odds. Repeated SARS-CoV-2 infections may cumulatively increase risk. Social determinants (e.g. limited healthcare access) also affect outcomes. For example, WHO notes higher long-COVID numbers among people with disabilities or in regions with poor health equity.
Estimates of prevalence vary widely between studies. Meta-analyses have reported anywhere from 10% to 30% of all infected individuals (depending on the variant wave and definition) experiencing prolonged symptoms. A CDC report in early 2024 indicated that roughly 22% of long-COVID adults have significant activity limitations. A global review found higher prevalence in lower-income countries (e.g., ~30% in middle-income vs ~14% in high-income nations). These differences may reflect viral variants, vaccination rates, and study methodology.
Importantly, WHO emphasizes that not every survivor develops chronic sequelae. Symptoms often improve over time for many: about 15% of people still have symptoms at 12 months, implying most long-COVID symptoms resolve within a year. Nonetheless, even a modest percentage of millions of infected translates to a large absolute number living with chronic illness.
Clinically, management focuses on symptom control and rehabilitation. No specific treatments are proven yet; guidelines recommend supportive care (e.g. graded exercise for deconditioning, cognitive therapy, medications for pain or sleep) and multidisciplinary rehabilitation programs. Healthcare systems must prepare for ongoing follow-up clinics. Long COVID also underscores the importance of preventing initial infection: vaccines, by reducing severity, also reduce longCOVID risk.
In summary, long COVID is a multi-dimensional syndrome affecting a significant minority of patients. It spans fatigue, pain, autonomic dysfunction, cognitive impairment and other domains, with risk heightened in women, older adults, and those with severe acute disease. Continued research is needed to understand pathophysiology (e.g. viral persistence, autoimmunity, micro clots have been implicated) and to develop specific therapies[5].
Variant Surveillance and Impact
SARS-CoV-2 continually evolves. Viral replication errors and immune pressure have given rise to numerous variants, some of which are designated Variants of Concern (VOCs) or Variants of Interest (VOIs) by WHO/ECDC/CDC due to changes in transmissibility, virulence or immune escape. Major VOCs have emerged in successive waves:
These changes have implications for diagnostics and vaccines. Some RT-PCR tests targeting multiple gene regions exploited the “S-gene dropout” (S gene failure) caused by the Alpha variant’s del69-70 as a proxy marker. However, heavy reliance on single target tests can lead to false negatives if variants mutate that region. WHO warns that variant mutations “may affect the performance of…diagnostic tools”. Diagnostic assays thus need continual validation against emerging strains.
On vaccines, antigenic drift means older vaccine strains confer less protection against new variants. For example, two doses of mRNA vaccines were >90% effective vs Alpha, but only ~30–40% effective against Omicron infection (though still ~70–90% effective against severe disease with boosters). Accordingly, vaccine manufacturers developed variant-adapted vaccines: e.g. bivalent mRNA boosters targeting ancestral+Omicron BA.4/5 (authorized in late 2022), and more recent formulas for Omicron XBB/JN.1. These updates are akin to annual flu vaccine adjustments. Surveillance labs globally sequence positive samples (through GISAID/WHO networks) to detect new mutations. WHO’s CoViNet and ECDC’s SAVE programs review genetic data continuously[3].
Variant monitoring is communicated via lineage names (Pango), as well as WHO labels (Alpha, Beta, Gamma, Delta, Omicron, etc.). As of mid-2025, Omicron subline ages (e.g. JN.1, KP.2) account for the vast majority of cases globally; no fundamentally new VOC has supplanted Omicron. CDC wastewater surveillance indicates that XBB-derived variants remain predominant (though specific proportions fluctuate). The constant surveillance of variants is crucial: even subtle changes (e.g. new spike mutations) may herald waves of immune escape. WHO and ECDC emphasize maintaining “high levels of [surveillance]” as SARS-CoV-2 continues to circulate widely[6].
The pharmaceutical implication is that diagnostics and vaccines must adapt over time. For example, monoclonal antibody therapies may lose effectiveness against new variants (many early mAbs failed vs Omicron), requiring development of broadly neutralizing antibodies or small-molecule antivirals. Likewise, antiviral target regions should be conserved. In vaccine design, variant coverage has become routine: platforms like mRNA allow rapid redesign. Some next-generation vaccines aim for pan-coronavirus immunity to pre-empt future variants[8].
Special Populations: Pediatrics and Pregnancy
Pediatric patients: Early in the pandemic, children were underrepresented among severe cases. Most pediatric COVID-19 cases are mild or asymptomatic. Common symptoms in children include fever and cough, but gastrointestinal and otolaryngologic symptoms (nausea, sore throat) are also frequent. Hospitalization rates in children are much lower than in adults; when hospitalized, children often do well. However, severe cases do occur, particularly in those with comorbidities (cardiac, respiratory, immunodeficiency). Long-term sequelae in children (e.g. long COVID) appear to occur but may be less common than in adults[4].
A notable pediatric complication is Multisystem Inflammatory Syndrome in Children (MIS-C). MIS-C is a hyper inflammatory syndrome usually emerging ~2–6 weeks after SARSCoV-2 infection (often after an asymptomatic or mild infection). It presents with fever, rash, conjunctivitis, GI symptoms (abdominal pain, vomiting, diarrhea), hypotension, and cardiac involvement (myocarditis, shock). On labs there is elevated CRP, ferritin, D-dimer, and often troponin. In early U.S. data, around 570 cases of MIS-C were reported by mid-2020. Most affected children needed intensive care due to cardiac issues (myocardial dysfunction, arrhythmias, aneurysms). However, with prompt treatment (IVIG, steroids, supportive care), most recover. MIS-C underscores that COVID-19 can provoke severe post-infectious disease even in children, though overall pediatric mortality remains very low.
Pregnant patients: Pregnancy confers higher risk for severe COVID-19 compared to no pregnant women of the same age. Pregnant women with COVID-19 are more likely to require ICU care, ventilation, and have higher mortality than non-pregnant peers. Physiological changes in pregnancy (reduced lung capacity, immunologic shifts) may contribute. The most common symptoms in pregnant patients mirror the general population: fever (~62%), cough (~38%), malaise, myalgia. Some had diarrhea or nasal congestion as well. A systematic review of pregnant cases (n≈92) noted that about two-thirds presented with fever, but 31% tested negative on initial RT-PCR despite pneumonia on imaging. Intensive care admission was rare in reports up to 2020, and reported mortality was essentially zero, though larger data later showed some COVID-related maternal deaths. [3].
Pregnancy outcomes: Infection has been associated with adverse obstetric outcomes. Metaanalyses find higher rates of preterm birth, fetal distress, and caesarean delivery in COVID-19 pregnancies. For instance, one review reported ~64% preterm delivery and 61% fetal distress among infected pregnancies. However, it’s often unclear how much was due to iatrogenic preterm delivery out of caution. Crucially, early data showed essentially no evidence of intrauterine vertical transmission – i.e. the virus rarely crosses the placenta. In one cohort (n=41), none of the tested new-borns had SARS-CoV-2. However, rare cases of trans placental infection have been documented (first reported July 2020). A pooled analysis found about a 3.2% rate of vertical transmission (27/936 neonates). Overall, while most babies born to COVID-positive mothers test negative at birth, obstetricians should be aware of this small risk and monitor neonates accordingly. Notably, WHO recommends that mothers with COVID-19 continue breastfeeding with precautions (masks, hand hygiene) as benefits outweigh risks.
Neonatal outcomes: Most infants born to infected mothers do well. Some studies have reported low birth weight or NICU admission in 20–80% of cases – but again, many of these reflect premature births. No congenital malformations have been attributed to SARS-CoV-2. Neonatal COVID-19, when it occurs, is usually mild or asymptomatic.
In summary, children generally have less severe COVID-19, but must be monitored for MISC. Pregnant women have higher risks and certain adverse pregnancy outcomes; vertical transmission is uncommon but possible. These special populations also raise questions about vaccination: current guidance strongly recommends COVID-19 vaccination in pregnancy, as it protects both mother and infant (via trans placental antibodies) without apparent safety signals in studies[4].
CONCLUSION
The COVID-19 pandemic has presented multifaceted challenges to global health, revealing the complex interplay between virology, clinical medicine, and public behaviour. Clinically, SARSCoV-2 is not just a “respiratory virus” but a multi-system pathogen that can affect the lungs, heart, GI tract, nervous system, kidneys, skin, and more. Understanding the full spectrum of COVID-19 symptoms and complications has been essential for early diagnosis and management.
Public health responses highlighted the importance of social factors: rural communities often adopted fewer preventive measures (masking, distancing) than urban areas, contributing to disparities in disease spread. Tailored education and outreach were needed to bridge these gaps.
Vaccines have had the largest impact on the pandemic’s trajectory, transforming COVID-19 from a widespread lethal threat to a more manageable endemic disease. The rapid development of mRNA and vector vaccines is a triumph of modern science. Despite the emergence of variants and waning immunity, ongoing booster campaigns (including variant-adapted vaccines) continue to protect against severe outcomes, as confirmed by recent CDC effectiveness data.
Diagnostics have likewise evolved: while RT-PCR remains the gold standard, point-of-care tests (antigen kits, CRISPR assays) have expanded our capabilities for rapid screening. Combining clinical acumen (symptom assessment, imaging) with a battery of tests allows for timely diagnosis.
Long COVID is now recognized as an important chronic outcome of SARS-CoV-2 infection, affecting about 6% of survivors. Its breadth of symptoms and prolonged course pose challenges for healthcare systems and emphasize the need for ongoing support of survivors.
Continuous genomic surveillance of SARS-CoV-2 has been critical. The major variants of concern (Alpha through Omicron) have successively shaped the pandemic landscape. Variant emergence necessitates adaptation of vaccines and treatments, underscoring the dynamic nature of this virus.
Finally, the experiences of children and pregnant patients with COVID-19 remind us that “one size-fits-all” conclusions may not apply to all populations. Pediatric cases are often milder, but conditions like MIS-C can be life-threatening. Pregnancy increases risk for severe illness, and while vertical transmission is rare, obstetric and neonatal outcomes require vigilance.
In conclusion, the COVID-19 pandemic’s legacy will include these lessons: the critical importance of integrating clinical science with behavioural and social considerations; the power of vaccine technology; the need for adaptable diagnostics; and the imperative of equitable healthcare. As SARS-CoV-2 continues to evolve, sustained research and surveillance will be key to inform pharmaceutical strategies (vaccines, antivirals, monoclonal) and public health policies. The thorough understanding of COVID-19 provided by this review—backed by the latest data—aims to support pharmaceutical and medical professionals in making evidence based decisions as we transition from pandemic crisis to endemic management.
REFERENCES




Ruturaj Bhatiya, Haney Patel, Virali Parmar, Ankur Patel, COVID-19: A Multifaceted Review of SARS-CoV-2, Disease Dynamics, and Global-to-Rural Spread., Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2407-2419. https://doi.org/10.5281/zenodo.16027634
 10.5281/zenodo.16027634
10.5281/zenodo.16027634