
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
K.V.N.N.S.P.S's Institute of Pharmaceutical Education and Research, Nashik
Controlled Drug Delivery Systems (CDDS) are advanced pharmaceutical formulations designed to release drugs at a predetermined rate for a specific period, maintaining optimal therapeutic levels in the body. The active pharmaceutical ingredient can be released to produce the intended therapeutic effect thanks to the drug delivery mechanism. In addition to having poor bioavailability and fluctuating plasma drug levels, conventional drug delivery methods (tablets, capsules, syrups, ointments, etc.) cannot provide sustained release. The entire therapy process could be ineffective without an effective delivery system. In addition, controlled drug delivery systems must deliver the medication at a precise target spot at a predetermined controlled pace in order to maximize safety and efficacy. Controlled drug delivery involves administering the medication locally or systemically for a predetermined amount of time at a predetermined pace.
Drugs can be administered through various routes; however, of all the routes of administration, oral route of administration is the most convenient for administering and for dosage adjustments. Convenience of use and ease of industrial preparation are key factor in their growth in popularity.(1)
When a polymer and an active ingredient or medication are mixed so that the release from the bulk material is pre-planned, this is known as controlled drug delivery. The maintenance of drug levels within a range, the requirement for fewer doses, the best possible use of the medicine in question, and improved patient compliance are all examples of controlled drug delivery systems.
The potential drawbacks of these benefits, such as the potential toxicity or non-biocompatibility of the materials used, undesired degradation byproduct, the need for surgery to implant or remove the system, the possibility of patient discomfort from the delivery device, and the higher cost of controlled release systems in comparison to conventional pharmaceutical formulations, cannot be disregarded.
Inertness, biocompatibility, mechanical strength, patient comfort, high drug loading capacity, safety from unintentional release, ease of administration and removal, and ease of fabrication and sterilization are all desirable qualities in a drug delivery system.(2)
Controlled drug delivery systems (3)
Medication is administered using this method, which keeps the drug's concentration in the blood and tissue stable for a long time. Pharmacokinetics (PK)Curves show a drug’s plasma concentration as a function of time for both traditional and regulated administration modalities. For multiple doses with oral tablets or injections, a typical bolus PK occurs in a traditional delivery system when the drug level varies above and below the minimal effective concentration. Conversely, the controlled delivery method exhibits zero-order PK after a single dose of a medication delivered under control using a particular formulation or apparatus. The therapeutic window is continuously maintained for medication levels.
Advantages and Disadvantages of controlled release preparation
Advantages
Disadvantages
Clinical advantages of controlled release dosage forms
Selection of Drug Candidates [10-12]
All the drugs cannot be formulated as their controlled release dosage forms. A drug must have the following characteristics for the formulation of controlled release dosage forms.
Factor Influencing the Design and Performance of Controlled Drug Delivery System
The design of a pharmaceutical formulation depends on the physicochemical properties of the drug and its pharmacokinetic behaviour. In conventional dosage forms, drug absorption through the biological membrane is usually the rate-limiting step for bioavailability. In contrast, in controlled drug delivery systems, the rate-limiting step is the release of the drug from the dosage form.
TYPES OF CONTROLLED DRUG DELIVERY SYSTEMS [13-16]
Controlled drug delivery systems are broadly classified as follows:
ORAL CONTROLLED RELEASE DRUG DELIVERY SYSTEMS
Most oral controlled release systems produce a delayed release of the drug into the gastrointestinal tract by using either diffusion, dissolution, or a combination of both.
The stability and coating thickness affect the rate of dissolution. In theory, the easiest oral medications to make are sustained release ones that use dissolution as the rate-limiting step.
Slow soluble polymers or microencapsulation control the drug's rate of dissolution in materials. Following the dissolution of the coating, the medication will be accessible for dissolution. By altering the coat's composition and thickness, the medication release rate can be controlled. Products with diffusion control can be made as tablets or encapsulated for use in pellet dosage forms. Two types of dissolution-controlled products can be distinguished:
a) Encapsulation Dissolution control
This device approach involves covering individual particles (or granules) with drugs using a slow dissolving substance. The coated particles may directly be packed (or stored in capsules) into tablets. Microencapsulation controls the rate of dissolution of the drug (and hence the availability for absorption). The substance will be available for dissolution until the coating is dissolved.
The coat's composition and thickness can be changed to control the rate of medication release. Chewing these can degrade the covering. One advantage is that embedded pellets are less vulnerable to stomach emptying to initiate absorption. Compared to non-disintegrating tablets, pellets typically enter the small intestine more uniformly.
b) Matrix Dissolution control
The medicine is compressed using a slow dissolving carrier, which is a different technique in this device. This regulates the rate of drug release through the matrix’s porosity, the presence of hydrophobic additives, the moistening system, the particle surface and the penetration of the dissolution fluid.
B) DIFFUSION CONTROLLED RELEASE
Diffusion systems are characterized by the release rate of a drug being dependent on its diffusion through an inert membrane barrier. Usually, this barrier is an insoluble polymer.
Movement of drug molecule from a region of higher to one of lower concentration. It is major process for absorption which no energy required. There are basically two types of diffusion controlled systems which have been developed over the past two decades,
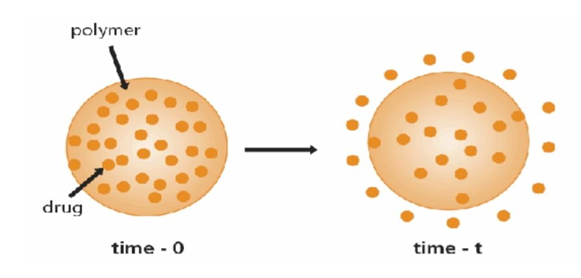
This method involves enclosing a core medication with a water-insoluble polymer. The drug partitions into the membrane and exchanges with the particles (or tablet) surrounding the liquid. The active agent is released into the environment through the rate-limiting membrane. In these systems, the rate of drug distribution is comparatively constant.
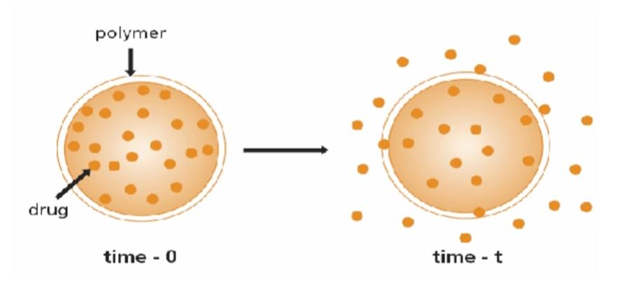
The homogeneous system, also known as a matrix system, disperses the medicine or active ingredient into a polymer matrix. An insoluble matrix disperses a solid medication in this system. The rate of drug diffusion determines the rate of drug release, but not the rate of solid dissolution.
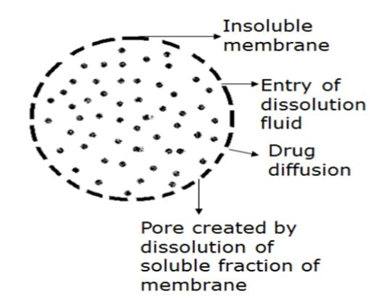
C) DIFFUSION AND DISSOLUTION CONTROLLED SYSTEMS
The main feature of this system is that the drug core is enclosed with a partially soluble membrane. Dissolution of part of the membrane allows for diffusion of the contained drug through pores in the polymer coat.
D) ION-EXCHANGE RESINS
Resins are water-insoluble materials containing anionic or cationic groups in repeating positions on the resin chain. The drug-charged resin is prepared by mixing the resin with a drug solution either by repeated exposure of the resin to the drug in a chromatographic column or by keeping the resin in contact with the drug solution for extended periods of time. The drug-resin is then washed to remove contaminant ions and dried to form particles or beads. When a high concentration of an appropriately charged ion is in contact with the ion-exchange group, the drug molecule is exchanged and diffuses out of the resin into the bulk solution.
They are mainly of two types: cation exchange and anion exchange resins.
A cationic drug forms a complex with an anionic ion-exchange resin e.g. a resin with a SO3 group. In the GI tract Hydronium ion (H) in the gastrointestinal fluid penetrates the system and activity the release of cationic drug from the drug resin complex.
H++ Resin - SO3 - Drug +→ Resin - SO3 -H+ + Drug+
An anionic drug forms a complex with a cationic ion exchange resin, e.g. a resin with a [N (CH3)3+] group. In the GI tract, the Chloride ion (Cr) in the gastrointestinal fluid penetrates the system and activates the release of anionic drug from the drug resin complex.
Cl + Resin - [N (CH3)3+] - Drug → Resin- [N (CH3)3+] - Cl + Drug [17-19]
E) pH - INDEPENDENT FORMULATIONS-
The granules are designed for the oral controlled release of basic or acidic drugs at a rate that is independent the pH in the GI tract. (Pederson, A.M, German patent). They are prepared by mixing a basic or acidic drug with one or more buffering agents, granulating with appropriate pharmaceutical excipients, and finally, coating with a gastrointestinal fluid permeable film-forming polymer. When the GI fluid permeates through the membrane, the buffering agents adjust the fluid inside to a suitable constant pH, thereby rendering a constant rate of drug release.
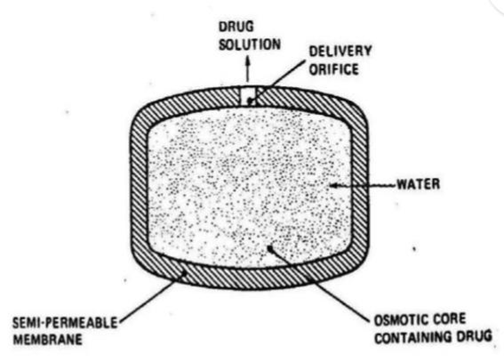
F) OSMOTICALLY CONTROLLED RELEASE-
In this type of drug delivery systems, osmotic pressure is the driving force that generates constant drug release. This system is fabricated by applying a semi permeable membrane around a core of an osmotically active drug or a core of an osmotically inactive drug in combination with an osmotically active salt. A delivery orifice is drilled in each system by laser or by a high-speed mechanical drill
Polymer
A polymer, also referred to as a macromolecule, is a large molecule composed of several repeating subunits. Both manufactured and natural polymers possess a variety of properties that make them commonplace and indispensable in everyday life. Examples of natural biopolymers are proteins and DNA, which are vital to the structure and operation of living things. Additionally, synthetic polymers such as polystyrene are also included in the category of polymers.
Polymers are a broad class of materials made up of many small molecules called monomers, which can be linked to form long chains and are therefore called macromolecules. [20]
Classification of Polymer:
Polymers are categorized into many categories based on various factors as stated in the below:
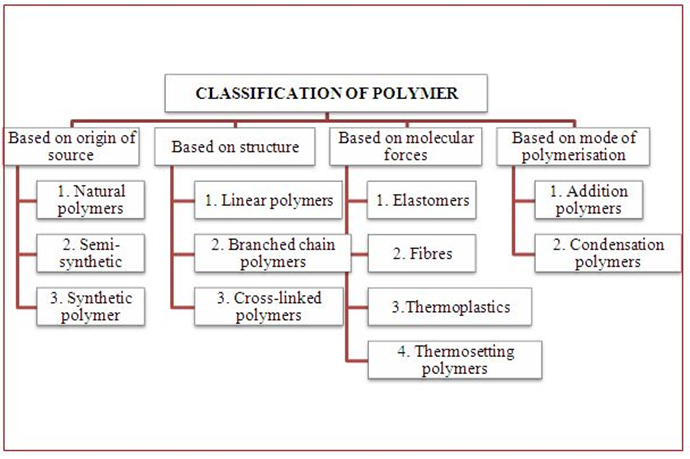
In these polymer, monomers are interconnected to form an elongated, linear structure. These chains do not possess any additional branches or side chains.
Ex: Polyester, Polyethene
The straight long chain of molecules is accompanied by various side chain. Due to there irregular packing these molecules exhibit low density, tensile strength and melting point.
Ex: Polypropylene, Amylopectin, Glycogen
The monomeric units are interconnected to form a three-dimensional framework in which cross link play a crucial role. These cross link contribute to the hardness, rigidity and brittleness of the network structure.
Ex: Bakelite, Formaldehyde resin, Vulcanized rubber.[21]
Advantages of Polymers:
The advantages of polymers are listed below:
Disadvantages of Polymers:
The disadvantages of polymers are:
REFERENCES


Mayuri Darade, Akansha Suryavanshi, Controlled Drug Delivery Systems, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2356-2364. https://doi.org/10.5281/zenodo.18653609
 10.5281/zenodo.18653609
10.5281/zenodo.18653609