
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Mahavir Institute of Pharmacy, Nashik, Maharashtra, India.
Advanced software, tools, and manufacturing technologies have significantly expanded the potential of three-dimensional (3D) printing in pharmaceutical sciences. The application of 3D printing enables pharmaceutical scientists to develop individualized, patient-centred drug delivery systems that move beyond the traditional “one-size-fits-all” approach. Additive manufacturing offers superior flexibility in customizing dosage form geometry, internal structure, and drug distribution, allowing precise control over drug release profiles and the incorporation of multiple therapeutics within a single formulation. These advantages contribute to improved patient compliance and enhanced clinical outcomes. This review provides a comprehensive overview of 3D printing technologies applied to drug delivery systems, covering fundamental principles, printable materials, and recent advancements across diverse pharmaceutical applications. The manuscript discusses major printing techniques, including fused deposition modelling, stereolithography, inkjet printing, selective laser sintering, and semi-solid extrusion, along with their pharmaceutical relevance. Various materials such as biodegradable and non-biodegradable polymers, hydrogels, and inorganic composites are highlighted due to their biocompatibility and processing suitability. Emphasis is placed on the role of digital modelling, simulation, and patient-specific data in designing personalized dosage forms to achieve optimal therapeutic outcomes. Additionally, the review addresses the characterization of 3D-printed pharmaceuticals and examines existing regulatory, ethical, and technical challenges [60,69,70]. Finally, future perspective’s including 4D printing, artificial intelligence–assisted design, and sustainable biomaterials are discussed [57,63]. Overall, 3D printing holds substantial potential to revolutionize personalized medicine by bridging the gap between digital manufacturing technologies and clinical practice.
Personalized medicine transforms an aspect of healthcare through tailoring an advanced treatment to specific physiological, genetic and lifestyle areas of a patient [49,50,55]. It goes beyond the conventional “one-size-fits-all” approach to treatment where medicines are manufactured and handed out to patients without the consideration of the patient’s individual specific characteristics. In the case of medications, more customized manufacturing and adaptable drug-delivery systems are surely needed [1]. Due to a growing range of patient demographics in terms of age, metabolic systems, and comorbidities, the necessity of tailored therapies has become even more pronounced. This design helps to achieve the intended clinical objectives while significantly reducing the chances of toxicity.
1.1 Need for Patient-Specific Dosage Forms
Conventional drug manufacturing method’s–like tablet compression or capsule filling–focus on uniformity and mass production over customization. These methods create standardized doses that don’t meet the therapeutic needs of each individual [2]. Dose adjustments or alternative formulations, for example, geriatric or paediatric patients face significantly different therapeutic challenges, which conventional manufacturing lines are unable to accommodate [56,59,62]. Finally, patients with polypharmacy, such as diabetics or people with cardiovascular disorders, might need consolidation of multiple drugs which traditional manufacturing approaches are unable to provide. In light of the above challenges, the need for precision therapeutics has directed research and pharmaceutical manufacturing toward flexible, customized, and on-demand fabrication technologies [2,56,59].
1.2 Limitations of Conventional Pharmaceutical Manufacturing
Batch-by-batch pharmaceutical manufacturing is inflexible, resource-heavy, and poorly individualized [3]. It is also poorly adaptable since the formulation of new dosage strengths or release patterns entails process parameter re-optimization, revalidation, and new regulatory approvals. Mechanical compaction, granulation, and solvent-based methods also use process geometry and the spatial arrangement of the drugs. The uniformity of mass production is enforced to ensure safety, but it is a double-edged sword for personalized drugs, integration of several drugs, and modifiable release profiles. Waste, inefficiency, and long wait times for production all compound the slow response to dynamic patient needs. The shift in healthcare to decentralization and precision targeting has exposed the many inadequacies of traditional methods[3,4,5].
1.3 Emergence of Additive Manufacturing in Pharmaceuticals
Additive manufacturing (AM), or 3D printing, has revolutionized pharmaceutical and biological applications. Layer-by-layer object construction gives 3D printers unprecedented control over shape, structure, composition, and microarchitecture [4]. Using CAD and digital fabrication, 3D printing facilitates the construction of complicated dosage forms for rapid prototype and production. Dosage forms can be designed for specific medication release rates. 3D printing pharmaceutical forms for small-batch or custom manufacture complements conventional procedures. The development, research and implementation of 3D printing technologies in the pharmaceutical sector accelerated rapidly following the creation of the first 3D printed drug, A levetiracetam tablet called Spritam®, was approved by the FDA in 2015 [5]. AM can 3D print tablets with specific porosity and medication concentrations, as shown by Spritam® pills. Ongoing research aimed at optimizing 3D printing for oral, transdermal, implantable, and injectable drug delivery systems is expected to further advance personalized medicine [4,5].
1.4 From Traditional to Digital Compounding
The digital transformation in compounding is a new chapter in the philosophy of manufacturing a pharmaceutical product. Whereas in classical compounding there is a lot of manual adjustments to formulation, empirical trial, and bulk processing, in digital compounding there is the use of predictive algorithms, computer-aided design, and automated bulk deposition for microstructural precision [6]. In digital additive manufacturing, a digital prescription of a “digital twin” of the patient serves as a guide in the design of a personalized dosage form, making in silico adjustments to the size, shape, concentration of the active ingredient, and the kinetics of release before actual fabrication [7]. This enhances dose precision and quickly adapts to therapeutic changes. A patient who gains weight or develops an illness may have their dose altered quickly. In addition, 3D printing with smart materials and the capacity to deposit various materials sequentially allow polypill production and improves patient-centred pharmaceutical care[6,7].
1.5 Aim and Scope of the Review
This review covers 3D printing applications in tailored medicine delivery systems. This technology enables customized treatment plans for each patient. This paper examines the various printing methods based on their foundational aspects, discusses the integration of printing into various systems, explores the functional compatibility of different pharmaceutical materials, and surveys innovative applications and case studies across multiple routes of drug delivery. Looking at the future of 4D printing, artificial intelligence, and eco-friendly materials, this paper discusses the ethical, legal, and industrial limitations applicable to the use of additive technology in the creation of drugs. Most importantly, the on-demand precise 3D printing of scalable therapeutics will transform the pharmaceutical industry[1,4].
2. FUNDAMENTALS OF 3D PRINTING
2.1 Basic Principles of Additive Manufacturing
Additive manufacturing (AM), commonly referred to as 3D printing, represents a diverse group of technologies that create three-dimensional objects by constructing them layer by layer, one cross-section at a time. Unlike computer-aided manufacturing (CAM), which cuts and mills, AM builds entities from scratch by constructing them in three-dimensional space, thereby offering unlimited geometric and structural design possibilities. AM creates a physically tangible object from a computer design, whereby a set of additive layers is generated. The pharmaceutical industry has experienced a profoundly significant impact from the application of 3D printing technology [8]. Advanced medications have been made possible by customising the formulation and dosage for a particular patient. Moreover, the drug’s 3D architecture can be designed to add features that control the dissolution rates, and the rates of release can be regulated to taper over time. Multiple active pharmaceutical ingredients (APIs) can be incorporated within a single unit of dosage form and positioned to deliver the drug within a targeted time frame [8]. This integrated approach can be applied to individualized therapy by spatially arranging the drug so the pharmacotherapeutic effects are tailored for the patient. 3D printing is suited for systems that require controlled release, drug-eluting implants, and multicompartment oral tablets. 3D printing is particularly useful for drug delivery systems that use thermoplastics, hydrogels, photopolymers, and mixed powders. Because 3D printing is automated and digitalized, it is possible to use it in laboratories and clinics to bridge the divide between pharmaceutical compounding and more sophisticated pharmaceutical manufacturing. This approach allows customized formulations that improve therapeutic outcomes and patient compliance. [8].
2.2 Stepwise Process of 3D Printing
The workflow of 3D printing involves several sequential stages, each crucial to ensuring the accuracy and performance of the final product. The process typically includes computer-aided design (CAD) modelling, slicing, printing, and post-processing.
Initially, a 3D model is created using a CAD system. CAD tools assist in repeatedly manipulating specific geometries, dimensions, and internal structures. In pharmaceutical modelling CAD involves specifying the parameters of a tablet’s shape, infill patterns, pore sizes, pore distribution, and the arrangement of the layered drug. Advanced models can incorporate patient-specific metabolic and anatomical details to produce customised dosage forms and implants.
Once the final digital model is complete, the next phase is slicing, which transforms the three-dimensional model into thin layers that can be printed in 3D. Each slice, along with the deposition path, flow rate, and speed, constitutes a detailed 2D cross section of the model. By converting a 3D model into numerous discrete layers, the printer can reproduce complex geometries with greater precision [9]. In addition to the essential printing parameters mentioned, the slicing software also enables the adjustment of the layer and infill density, which influences the drug's mechanical strength and release profile [8,9].
According to Zhang et al. [10], the polymer filament, resin, powder, or hydrogel used in printing is built and formed layer by layer according to the sliced file. Based on the different printing technologies, distinct methods of deposition are used: in extrusion-based printers, molten polymer is extruded through heated nozzles; in inkjet printers, drug-laden solution droplets are sprayed; laser-based printers modify powder through sintering; and in photopolymerization systems, laser curing is performed. Each layer adheres to the one below to form the complete structure. Uniform drug distribution and the protection of heat-sensitive active pharmaceutical ingredients (APIs) from degradation require a reduction in temperature, humidity, and pressure within the printing environment[10].
Following the printing of dosage forms, the next stage involves improving the forms’ mechanical stability and functionality and may include steps like moisture removal, curing, sterilization, surface finishing, or even drug loading if it was not incorporated in the printing process [11]. For instance, components made using the SLA-3D printing technology require UV light post-curing as a means to complete the polymerization, while those made using powder-tech needs to have sintering or binder removal done. Post-processing in drug-loaded systems aids in establishing uniform weight, porosity, and release kinetics, which becomes pivotal in controlled drug delivery [51,58,65]. For adequacy and consistency in a printed dosage, uniformity in weight, hardness, and various dissolution tests are done to ascertain the quality of reproducibility.
This step-by-step process helps bring together digital accuracy and carefully designed materials to make better drug-delivery systems. Most of the changes, or even all of them, that are needed to be made in a stage are in pursuit of a specific therapeutic targeting, or even patient or regulatory needs, or any of the three [59,61].
2.3 Role of Digital Modelling and Computer-Aided Design (CAD)
Fundamental aspects of 3D printing in pharmaceutical manufacturing are based on digital model ling and computer-aided design (CAD) techniques. With CAD, researchers have possess the capability to fabricate virtual prototypes, which allows them to design and test different dosage forms geometries and internal configurations in a cost effective manner, before actual fabrication. Moreover, CAD tools have expanded the designer's ability to fine-tune critical parameters of a dosage forms such as layer thickness, surface roughness, closure porosity, compartmentalization, and integration of the drug, which all dissolve and interrelate with the mechanical and dissolution properties. The integration of computer-aided engineering (CAE) tools and finite element analysis (FEA) software enhances predictive modelling of stress by integrating prediction of the stress distribution and modelling the degradation and diffusion of the drug [12]. This predictive modelling enhances prototype optimization and decreases the volume of experimental trials needed. Moreover, the integration of CT and MRI medical imaging facilitates design and fabrication of patient-specific digital models. This integration enhances the biocompatibility of the designed digital models such as drug-eluting scaffolds and implants by accurately fitting them to pathological tissues and anatomical structures. Data reproducibility and standardization is another major benefit of CAD-based digital design [13]. Once a validated digital model has been created, it can be duplicated and distributed to different printing systems with no deviation to the original. This digital traceability provides a robust system of qualitative measures and assists in meeting stringent regulatory requirements of standard operating procedures in a manufacturing environment. Digital modelling further assists in optimizing complex geometries and designing controlled-release drug profiles [12,13].
2.4 Classification of 3D Printing Technologies
3D printing technologies are classified based on the mechanism of material deposition and energy source used for solidification. The most relevant categories in the pharmaceutical sector are:
Continuous layers are formed by extruding material through a nozzle. For thermoplastic polymers like PLA, PVA, or even Eudragit, FDM is the best option. For hydrogel bioprinting or hydrogel bioprinting variants, the SSE technology fits well as it employs viscous gels or pastes.
Binder jetting involves deposition of liquid binder onto a powder bed to form layers [17]. The process functions effectively at low temperatures, making it suitable for heat-sensitive medications.
The methods involve curing liquid photopolymers, layer by layer, using either UV or visible light [19,20]. They guarantee excellent accuracy and a glossy finish. Nonetheless, for them to be used in healthcare, biocompatible polymers and non-toxic photo initiators are essential.
A laser scans polymer or composite powders, fusing them into solid structures. SLS provides the capacity to manufacture porous matrices and mechanically robust implants. However, the high temperature associated with SLS limits the technique's use with thermally unstable APIs.It is suitable for heat-stable drugs and allows creation of porous structures[22,23].
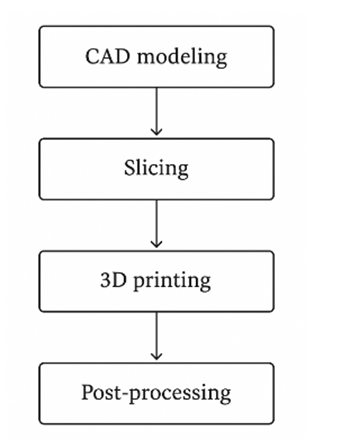
Figure 1. General workflow for 3D-printed drug dosage design.
3. 3D PRINTING TECHNOLOGIES IN DRUG DELIVERY
Pharmaceutical manufacturing integrates 3D printing technologies. This work streamlines the conceptualization, design, and construction of dosage forms. Each printing technology provides specific competitive advantages with regard to resolution, material versatility, and management of the printing process. Knowing which technology to choose is central to achieving a specific therapeutic aim [14]. The major 3D printing technologies used in drug delivery are Fused Deposition Modelling (FDM), Inkjet Printing (Binder Jetting), Stereolithography (SLA) and Digital Light Processing (DLP), Selective Laser Sintering (SLS), and Semi-Solid Extrusion (SSE)/Bioprinting, and their respective mechanisms, materials, and uses in pharmacy are described as follows [14].
3.1 Fused Deposition Modelling (FDM)
One of the most extensively studied technologies is Fused Deposition Modelling (FDM) and applied 3D used for pharmaceuticals, it is done using 3D printing and one of these techniques is printing using thermal extrusion. A thermoplastic polymer filament, already loaded with a drug, is heated beyond its melting point and then forced through a nozzle to create multiple layers on a substrate. These layers are built in a programmed sequence for the nozzle to build the requested 3D object. The main process parameters are bed temperature, layer height, extrusion rate, printing speed, and temperature of the nozzle [15]. These parameters need to be accurately set to assemble the active drug layer with the desired mechanical strength, porosity, and the controlled rate of release [52,54,66]. For example, the layers can be thermally bonded but the active drug layers can be degraded if the extrusion temperature is excessively high. For that reason, the process must have a well-defined window to maximize the fidelity of the print and stabilize the drug at the same time. In Fused Deposition Modeling (FDM), biocompatible thermoplastic polymers like polyvinyl alcohol (PVA), polylactic acid (PLA), polycaprolactone (PCL), and Eudragit are utilized [16,54,67].
These polymers enable an array of release profiles for a drug: immediate, sustained, or enteric (delayed) release. PVA is suited for formulations needing rapid release as it is water-soluble. For controlled release, PLA and PCL are preferable, as they are biodegradable. Eudragit’s various grades allow customization for controlled, pH-sensitive release of the drug in the gastrointestinal tract. Hot-melt extrusion (HME) and solvent blending are the two main techniques used for drug incorporation in the FDM process. For HME, drug and polymer are mixed and then heated to the point of forming a homogeneous filament which can use for printing. This method provides uniform drug distribution throughout the filament, but is limited to APIs that can withstand high temperature processing. For solvent blending, a drug is dispersed or dissolved in solvent with the polymer; then filament formation occurs at lower temperatures after the solvent is evaporated. This approach lessens the risk of deterioration of the drug during processing [16].
FDM's flexibility in creating personalized medicines has been documented in a lot of research. For example, Goyanes et al. created FDM-printed tablets of paracetamol and caffeine and modified the release profile by varying the infill density and surface geometry. Other works have shown the creation of multilayered polypills in which several APs and different release patterns were integrated. This clearly illustrates FDM's capability in polytherapy and on-demand dose personalization. However, FDM's high processing temperatures, possible drug degradation, and limited materials, especially with heat-sensitive drugs, pose serious challenges. Fortunately, the field is improving with low-temperature extrusion and the creation of new polymers, which is broadening the pharmaceutical use of FDM [15,16,17].

Figure 2. Schematic diagram illustrating the printing mechanism of FDM technology
3.2 Inkjet Printing (Binder Jetting):
Technology has advanced in drug formulation, especially in formulation for drugs that are heat-sensitive or need low temperatures - Inkjet printing, or Binder Jetting. The formation process of the desired 3D structure involves incremental layering of printing and fusing of powder particles. The printing of liquid binders or drug solution is deposited as small droplets onto a powder bed that is build up layer by layer. Where the droplets are printed acts as a fusing agent that selectively joins the powder particles. Because Inkjet printing offers low temperature or ambient temperature operations, incorporated drugs, especially thermolabile, are less likely to degrade. Other drug formulations that may be incorporated include certain biologics and therapeutics. The Inkjet printing formulation process is thermolabile and formulate heat-sensitive drugs without advanced degradation, making it especially useful for low heat drug formulations [64,68]. Powder-based materials include excipients like lactose, cellulose, or mannitol, selected for their flowability, compressibility, and compatibility with the binding solution. Binder solutions consist of APIs, and water, ethanol, or other suitable solvents, and include surfactants and other excipients. After each layer’s printing, the powder bed is recoated, and the sequence is repeated throughout the entire construction process [17].
Drying and curing advance the residual solvent removal and improve mechanical strength and solidity in the post-processing phase. The ability to perform multi-material and multi-drug inkjet printing makes it possible to produce intricate dosage forms with drug gradients and compartmentalized layers. An example is the polypill system, Inkjet printing was utilised to separate multiple printed drugs layered in a single tablet into different sections, thereby preventing drug–drug interactions. The rapid disintegrating oral film also exemplifies the technology [18].
APIs printed equilibrate on a polymeric substrate allow the crafted film to precisely control the dose and release features. The first FDA-approved 3D-printed drug is Spritam® (levetiracetam), which is designed using Aprecia Pharmaceuticals’ ZipDose® 3D printing technology [5]. The ZipDose® technology is capable of creating tablets with advanced porous structures that provide the rapid disintegration that is important for individuals who have difficulty swallowing tablets. Even with the pros referenced above, there are still concerns with the technology such as the flow characteristics of the powders, the control of the depth of penetration of the binder, and the strength of the binder. The technology is still a front-runner for advanced pharmaceutical manufacturing because of its precision and ability to print without the use of heat [5,8,10].

Figure 3. Schematic diagram of Inkjet printing (binder jetting)
3.3 Stereolithography (SLA) and Digital Light Processing (DLP):
Stereolithography (SLA) and Digital Light Processing (DLP) are 3D printing techniques that polymerize and cure resin using light, whether UV or visible. Laser SLA scans and solidifies resin, while DLP uses a Digital Micromirror Device or a projector to cure an entire layer, which speeds up printing. They have the best resolution and surface finish of any 3D printing technology, which is why they are preferred to manufacture complex drug delivery systems and implantable devices. When light interacts with the photo initiator present in the resin, it undergoes polymerization ell of the cross-linked chains to form a solid piece. For drug delivery systems, the resin has to be biocompatible, non-toxic, and non-residual [19].
Some common resin matrices are poly (ethylene glycol) diacrylate (PEGDA), gelatin methacrylate (GelMA), and acrylate polymers. These matrices can be designed to fit the required mechanical property and degradation profile, making them suitable for drug-eluting implants or micro devices designed for delivery. SLA and DLP are capable of producing high-quality prints (10–100 µm) which enabling the formation of micro-porous structures for controlled drug diffusion. The construction's accuracy enables the housing of diverse APIs in distinct compartments and facilitate programmable release patterns. For instance, the SLA-printed tablet of different lattice geometry demonstrated the design geometry can inversely influence pharmacokinetics showing different rates of dissolution [20].
Nevertheless, the application of UV-curable materials gives rise to concerns regarding depot and drug pharmacologic-liability. Photodegradable drugs pose potential problems and polymerization may be incomplete leading to residual cytotoxic monomer and initiator. Hence, limited research has been conducted to develop fully biocompatible photo-resins. In spite of numerous unresolved problems, there is abundant construction design and construction precision for SLA and DLP which explains the growing use for personalized implants, micro-needles, and tissue-engineered scaffolds[19,20].

Figure 4. Schematic representation of SLA and DLP photopolymerization-based 3D printing technique
3.4 Selective Laser Sintering (SLS):
Selective Laser Sintering (SLS) is a manufacturing technology that uses laser beams and advanced software to create 3D objects by sintering layers of powder without the use of binding agents. The software guides the laser to sinter the composite or polymer powder to the required design while regulating the powder sintering to control the final product’s density and porosity [21]. After a powdered layer is sintered, the system then lowers the powder bed, and fresh powder is deposited over the pattern, subsequently being sintered to create the finished part. The unsintered powder is a very effective support mechanism. This removes the requirement for extra support scaffolds during the sintering process. In SLS pharmaceutical applications, control over sintered objects’ mechanical strength and porosity impacts the rate of drug release. This control is achieved through variations in laser power and scan speed and is most effective when used with layer compression. Matrix density and diffusion rates can be designed to respond to drug release rates. For example, laser power can use to control matrix density for sustained release through dissolution or, as a lower laser sintering powder control, to create porosity for dissolution. SLS technology is versatile with regard to various powders as it can handle polyamide (PA), polycaprolactone (PCL), polyvinyl alcohol (PVA), and some composites with hydroxyapatite and calcium phosphate for biomedical implants. Furthermore, it can integrate some drugs by physically mixing them with the powder feedstock and also through impregnation after the printing process [22].
Yet, the procedure is carried out at very high temperatures, often more than 100 and 150 degrees Celsius, which makes it not ideal for applications with heat-sensitive Active Pharmaceuticals Ingredients (APIs). Still, SLS has managed to produce porous oral tablets, transdermal devices, and biodegradable scaffolds. For example, Fina et al. used SLS to print theophylline tablets which had tunable porosity and release profiles simply by varying the laser parameters. The technology’s capability to produce support-free complex structures is an advantage for implantable and controlled-release systems. However, the issues of powder recycling, uniformity of particle size, heat degradation of drugs, and expensive powders for some of the applications in the SLS process need to be solved for the print [21,22].
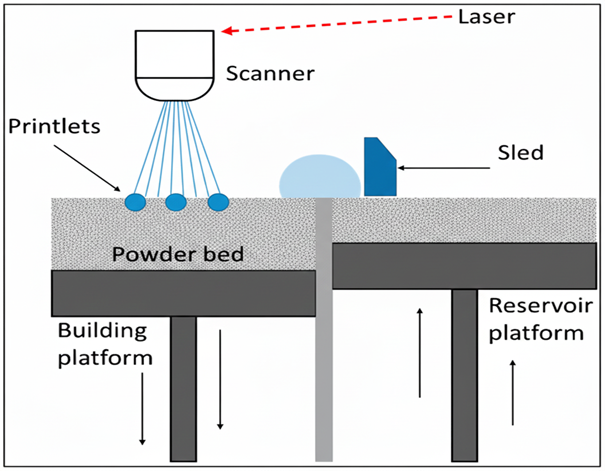
Figure 5. Schematic illustration of Selective Laser Sintering (SLS)
3.5 Semi-Solid Extrusion (SSE) and Bioprinting:
The term bioprinting involves the use of Semi-Solid Extrusion (SSE) technology which uses viscous gels, pastes, and hydrogel formulations as printing materials. In contrast to Fused Deposition Modelling (FDM) which uses melting and solidifying techniques, SSE is conducted at ambient or low temperatures. This makes SSE ideal for use with temperature- and pH-sensitive drugs and biologics, as well as with living cells. In this technique, a pneumatic or mechanical piston pushes the semi-solid formulation through a nozzle similar to a syringe, allowing for the sequential deposition of material according to the specified digital design. The SSE method also allows for the unique processing of hydrogel materials like alginate, gelatin, chitosan, GelMA, and Carbopol [23].
These SSE tissue scaffold materials can encapsulate therapeutic agents or living cells. SSE can use to print semi-solid formulations for personalized implants, tissue-engineering transdermal drug-delivery patches, and tissue engineering. Viscosity, shear-thinning behaviour, and crosslinking kinetics determine printing ability. Ionic, thermal, or photo-crosslinking stabilizes constructs after printing, depending on hydrogel chemistry. Calcium ions crosslink alginate structures, and ultraviolet light crosslinks GelMA formulations. The SSE's versatility allows intricate spatial arrangement of various materials and multiple drugs within one construct, enabling complex dosage designs and phase release patterns. SSE and bioprinting are being used in pharmaceuticals for wound dressings, localized cancer implants, and regenerative scaffolds. For example, bio-printed hydrogel wound dressings created for post-surgical use were designed to provide sustained local release of antibiotics or anti-inflammatories and be compatible with the tissues at the surgical site, thereby facilitating integration with the surgical site [24].
Additionally, bioprinting enhances the provision of cell-laden matrices that are aseptically integrated with the constructs, facilitating the creation of in vitro tissue models for drug testing that supports the personalization of therapy. In terms of advantages, SSE has low processing temperature, versatile materials, and biocompatibility. However, it also has limitations, and these include slow printing speed, lower structural integrity, and complex post-processing. However, it remains highly versatile in personalized medicine for having the gentle processing of hydrophilic and thermolabile APIs, the bio-fabrication and on-demand printing potential, and the capability to perform SSE [23,24]
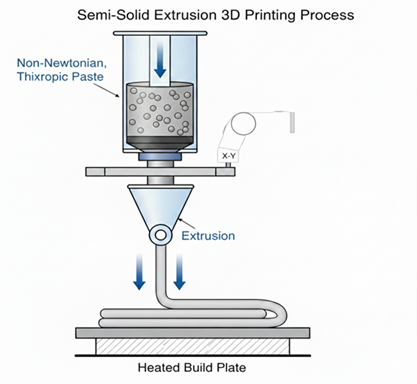
Figure 6. Schematic diagram of the Semi-Solid Extrusion (SSE) 3D printing process
Table 1: Comparison of Major 3D Printing Technologies for Drug Delivery Systems:
|
Technology |
Process Mechanism |
Suitable Materials |
Advantages |
Limitations |
Resolution Range |
|
FDM |
Thermal extrusion of polymer filaments |
PLA, PCL, PVA, Eudragit |
Simple setup, strong mechanical strength, customizable release |
High temperature, limited to thermally stable APIs |
100–300 µm |
|
Inkjet (Binder Jetting) |
Droplet deposition onto powder bed |
Lactose, cellulose, mannitol |
Low temperature, multi-drug capability, rapid disintegration |
Poor mechanical strength, binder penetration issues |
50–100 µm |
|
SLA/DLP |
Photopolymerization of resin |
PEGDA, GelMA, acrylates |
High precision, complex geometries |
Photo initiator toxicity, light sensitivity |
10–100 µm |
|
SLS |
Laser sintering of powder |
PCL, PA, PVA |
Controlled porosity, no support required |
High heat, limited materials |
100–200 µm |
|
SSE/ Bioprinting |
Extrusion of semi-solid gels |
Alginate, gelatin, chitosan |
Low temperature, biocompatible, cell-printable |
Low strength, slow process |
100–400 µm |
4. MATERIALS FOR PHARMACEUTICAL 3D PRINTING
Choosing the right materials is fundamental to the success of pharmaceutical 3D printing because these materials affect the printability, biocompatibility, mechanical properties, and drug release profile of the finished dosage form [25]. Unlike traditional pharmaceutical manufacturing, which involves few materials because of standardized excipient lists, additive manufacturing allows the thoughtful mixing of flexible doses of polymers, hydrogels, and inorganic composites to design customized multifunctional drug delivery systems. Any given material needs to meet two conditions: it should meet biopharmaceutical requirements and it needs to be processable using the selected 3D printing technology. This chapter describes the principal categories of materials used pharmaceutical 3D printing polymers, hydrogels, inorganic and composite matrices, and active pharmaceutical ingredients (APIs) [25].
4.1 Polymers
Out of all the materials used in pharmaceuticals, polymers stand paramount within the domain of 3D printing. This is largely due to the ease of processing and the compatibility of polymers across multiple additive manufacturing techniques. For drug delivery systems, there exists a spectrum of polymers to choose from. According to the targeted drug release kinetics, one can opt for either a biodegradable or a non-biodegradable polymer. To achieve prolonged drug release kinetics, biodegradable polymers are often the superior choice because their controlled breakdown facilitates slower, long-term drug delivery. Recognized for their biodegradable and non-toxic byproduct degradation, materials like polysaccharides, PLA, PCL, and PLGA Biopolymers, rank high as polymers of choice [26].
Furthermore, the use of PLA in Fused Deposition Modelling is more environmentally friendly due to its degradation into lactic acid, and it is widely used because of the mechanical properties of the polymer. Being biodegradable, lactic acid, along with other high molecular weight PLA and lactic acid degrades intermediately, poses no threats from accumulation, and consumable as a safe in vivo implant, is obliterated post-use. For non-instant release formulations, PLA poses challenges due to release control as less PLA is more beneficial in control. Slow drug release can be more desirable in sustained release implants; however, PLA will be less suited for immediate release formulations. Unlike PCL, which has a lower melting point (about 60°C) and is highly flexible, making it suitable for the development of thermally sensitive drugs and for implantable drug delivery systems, PCL has a slow degradation profile over a number of months, which is advantageous for chronic and localized delivery over prolonged periods for therapeutic, chronic, and palliative therapies. PLGA, a lactic and glycolic acid copolymer, has a flexible degradation profile due to the varying ratios of its monomers and offers a balance between mechanical strength and the controlled release of the drug. The versatility of PLGA, along with its biocompatibility and approved regulatory status, allows for the most varied applications in controlled and targeted delivery systems utilizing microspheres, implants, and scaffolds [27].
Uses of controlled and targeted delivery systems can include PLGA biocompatible microspheres, implants, and scaffolds. In the case of pharmaceutical 3D printing, the importance of non-biodegradable polymers, particularly for printing oral medicines, transdermal patches, and for enduring devices where mechanical toughness is essential and degradation is not required, is significant. Within this category, polyvinyl alcohol (PVA) is one of the most used polymers in Fused Deposition Modelling (FDM) printing due to its water solubility, film formation, and rapid-release formulation capabilities. There are two ways it can be used—for controlled-release profiles, it can be matrix former and for sullied release profiles, it can be support material. Another example is Eudragit polymers, which is a family of methacrylate-based copolymers, and use also for enteric coatings and for the modulation of pH sensitive release [28].
Eudragit grades, depending on their chemical composition, dissolve in specific pH ranges allowing for targeted delivery of the drug to the intestines or the colon or for selective release in the colon. Another non-biodegradable polymer of considerable importance is hydroxypropyl methylcellulose (HPMC). It is incorporated in semi-solid extrusion and inkjet-based systems for its gel-forming and controlled hydration properties. It enhances cohesive mass of layers in systems allowing for sustained release of drug. It has also been incorporated as a cohesive structural aid in multi-layered printed systems. The variations in temperature and pH have become a subject of growing interest for stimuli responsive and on demand and environment responsive drug delivery [28]. For example, poly(N-isopropylacrylamide) (PNIPAAm) exhibits thermos responsive behaviour. and control phase switching at and around physiological temperature, which allows implantable systems to control drug delivery. Also, copolymers which include swelling pH-triggering carboxylic acid and amine functional groups provide excellent candidates for site-specific delivery in the pH varied gastrointestinal tract. These devices introduce expanded possibilities by responding to variations in a patient’s physiological state, enabling the dosage form to continuously and dynamically adjust to individual conditions, thereby advancing the concept of fully personalized medicine [28].
4.2 Hydrogels
The properties of hydrogels such as high water content, biocompatibility and similarity to soft tissue and extracellular matrices, makes them, alongside other materials, important for 3D printing in Pharmacy. Hydrogels are most effective in Semi-solid extrusion (SSE) 3D bioprinting, for they can be manipulated to encapsulate small particles and biologics and can be delivered through viscoelastic hydrogels [29]. Their unique properties of moisture retention and diffusion of sustained release makes them ideal for localized, sustained and prolonged drug delivery like for wound and tissue regeneration and injectable drug depots [30].
Frequently used hydrogels such as gelatin methacrylate (GelMA), alginate and chitosan have their unique beneficial properties. Gelatin, as a source of GelMA, gives rise to a photo-cross-linkable hydrogel which possesses mechanical properties that can be customized and biological functionalities attributed to cell adhesion motifs. Crosslinking, which may be induced in UV and visible light, produces spatially controlled gelation and enables construction of tissue-engineered scaffolds and implantation of cell-laden scaffolds. This of course assumes that biocompatibility is ensured through the use of non-cytotoxic photo-initiators and proper light exposure parameters. Alginate is a polysaccharide biopolymer extracted from brown algae and is applied extensively due to its mild gelation properties and biocompatibility. It is considered for use in temperature-sensitive formulations due to its ability to form hydrogels through ionic crosslinking with divalent cations (such as calcium) and its weaker ionic gel state [30].
It supports drug and nutrient diffusion through its porous matrix and degradation is adjustable through blending and chemical constructs, and the degradation time. Chitosan is a derivative of Chitin and has innate antimicrobial, mucoadhesive, wound healing properties thus qualifies for transdermal and mucosal delivery. Chitosan's cationic character helps to form polyelectrolyte complexes with anionic biomolecules and drugs, which serves as a system for drug capture and controlled release. The application of stimuli-responsive hydrogels towards personalized drug delivery is a new development in the field. For instance, Pluronic F127 is a thermos responsive gel which provides an injectable system that solidifies in situ due to its ability to perform a sol-to-gel phase transition at a set temperature. PEGDA photo-crosslinkable hydrogels grant intricate design control, and the capability to integrate multiple materials for SLA or DLP printing. For intricate therapeutic designs, hybrid hydrogels that integrate biodegradable polymers or nanoparticles can achieve desired mechanical properties along with control over release kinetics. Hydrogels should next be targeted for patient-specific implants and drug delivery systems, as they incorporate printability, bio-functionality, and controlled degradation which can be tuned [29,30].
4.3 Inorganic and Composite Materials
While hydrogels and polymers continue to dominate pharmaceutical 3D printing, inorganic and composite materials are increasingly important for specialized uses in things like smart drug delivery, orthopaedic implants, and bone tissue engineering. Compared to organic polymers, these materials provide greater mechanical strength, multifunctionality, bioactivity, and other benefits. Calcium phosphates and hydroxyapatite are few of the main inorganic materials since they are chemically similar to the mineral portion of bone [31].
Because of bone scaffolds' positive osteo-conductivity and bone implant biocompatibility, they are good candidates for regeneration scaffolds and implant coatings. 3D printing of composite materials makes it possible to create porous, patient-specific implants that can facilitate the adhesion and vascularization of bone cells and the simultaneous delivery of therapeutic agents, including antibiotics and growth factor. After bone has formed, polyesters like PLGA and PCL, and hydroxyapatite will biodegradable composite scaffolds provide the bonded bridge for the scaffolds to mechanically robust and the scaffolds to progress through controlled incremental PCL or PLGA. This will ensure that they are replaced by the scaffolds that are natural bone tissue. Besides bioactive ceramics, conductive and magnetic additives are being integrated into 3D-printed drug delivering biomedical devices. Polymers and graphene are the building blocks for electro-stimulated release systems, that allow for localized drug release with the application of an external electrical field. Likewise, magnetic nanoparticles encapsulated in polymers allow for magnetically controlled, as well as thermally activated release. This control provides precise release and minimizes unwanted side effects [32]. These fillers are paving the way for “smart” implants. Controlled release and altered physiological responses are expected with remote and biofeedback control as implants respond to physiological changes. Ensuring uniform dispersion of inorganic fillers in polymer matrices, s maintaining surface biocompatibility, print fidelity, and surface biocompatibility are challenges yet to be solved. These challenges are being addressed, along with others, by formulation advances such as hybrid ink preparation and functionalization of nanoparticles. This offers a promising growth in the pharmaceutical 3D printing field [31,32].
4.4 Drugs and Active Ingredients
Choosing the active pharmaceutical ingredient (API) and combining it with suitable carrier materials is essential for making 3D-printed drug delivery systems effective. During the fabrication, the API needs to have stability, compatibility with excipients, and predictable release behaviour after administration. Different 3D printing methods have different thermal, mechanical, and photochemical conditions, so API integrity remains a challenge. In thermal FDM and SLS printing methods, APIs are at risk for drug instability when there is exposure to high thermal processing conditions [33]. Therefore, API candidates with elevated melting points or those stable with moderate temperatures, for example, ibuprofen and caffeine, are often selected. On the other hand, thermolabile drugs and biologics are best for low-temperature methods as inkjet printing or semi-solid extrusion. In these methods, the ambient processing environment protects from degradation. Photopolymerization techniques like SLA or DLP, use UV light or visible light to trigger drug degradation and photochemical reactions. Using light-activated API and visible light curable resins lowers this risk. Additionally, pre-mixing, co-axial deposition, and post- loading strategies, define release profile and drug distribution. For example, instilling APIs into a hydrophilic matrix accelerates release, while encapsulating them in a hydrophobic polymer slows release. It is critical to recognize the influence of residual solvents on the crystallinity, stability, and bioavailability of medications. While constructing a drug delivery system using solvent blending, one must ensure the preservation of distinct phases and the drug’s recrystallization upon drying. Although more sophisticated encapsulation techniques—such as embedding drugs in microspheres, incorporating them into nanoparticles, or forming inclusion complexes with cyclodextrins—are aimed at enhanced stability and controlled active pharmaceutical ingredients (APIs) release [34].
These techniques facilitate the integration of multiple drugs into a single 3D printed system, thereby streamlining personalized polytherapy for patients with multiple comorbidities. Incorporating active 3D printed biologics for patient-specific scaffolds is a new frontier for the 3D printing discipline, particularly in the context of 3D printing biologics for APIs geared towards gene therapy and other regenerative medicine technologies. Although these innovations are still in their conceptual phase., they highlight the possibilities 3D printing offers. The integration of engineering with biomedicine is the cornerstone of 3D printing pharmaceuticals. The development of thermoplastic polymers, hydrogels, and inorganic composites that enable the 3D printing of advanced scaffolds for fragile APIs shows the extent to which materials science and 3D printing can transform personalized medicine. The use of multifunctional, responsive, interactive, and clinically safe materials for therapeutic applications will greatly enhance the development of clinically applicable 3D printing systems for drug delivery [33,34].
5. DESIGN CONSIDERATION FOR PERSONALIZED DOSAGE FORMS
5.1 Geometry and Surface Design
3D printing technology integrated within contemporary pharmaceutical practices influences tailored medication delivery via customized dosage forms. Through a unique mechanistic capability within dosage forms optimal disintegration or dissolution is engineered and dissolution release kinetics attained. Traditional dosage forms utilizing a standard geometric configuration, for example a tablet, primarily sufficed due to costs involved in mass production and packaging. 3D printing technology integrated within contemporary pharmaceutical practices influences tailored medication delivery via customized dosage forms. Custom 3D printing enables manipulation of external geometric shapes and tailored internal porosity to shape a dosage form release profile. More complex geometric forms such as a toroid or honeycomb can be synthesized to create a desired ratio of surface area to volume control to optimize disintegration or dissolution of dosage form. An engineered high ratio of surface area to volume improves disintegration or rapid dissolution release kinetics. Conversely, a geometric form of high volume to surface area ratio sustains or controls release of dosage form.Different types of fill patterns, including rectilinear, concentric, and gyroid, as well as varying fill densities, produce microchannels that help induce and regulate fluid ingress and flow [35,36].
Because of the effects of surface texture on wettability and adhesion, the texture of a surface contributes to the overall drug release profile. Rough surfaces, for example, will promote contact and encourage dissolution, whereas smooth or coated surfaces will slow the release of a drug and, by design, provide sustained release. Shape and surface design features of a dosage form can also promote compliance. Smaller or differently shaped tablets, such as pyramidal or multi-lobed tablets, Provide an added benefit of easier swallowing for patients in both paediatric and geriatric groups. In advanced examples, implants can be made to have specific, modified geometries that correlate with particular anatomical spaces for localized and prolonged drug delivery. The combination of such geometric designs with surface treatment or alteration presents unique opportunities for achieving specific desired pharmacological results [37].
5.2 Drug Loading and Distribution
A significant advantage of 3D printing in drug delivery systems is the control over the spatial distribution of the drug within the dosage form [38]. Unlike conventional mixing or coating approaches that yield homogeneous formulations, additive manufacturing can deposit drugs in gradients, zonally, or in layers [38]. This feature facilitates tailoring of the release kinetics and the construction of fully integrated multi-drug delivery systems within a single dosage form. There are multiple approaches for drug loading. For example, the drug can be incorporated into the printing material before the deposition process as part of in-process techniques or into the printed structure afterwards as a post-printing technique [39].
The choice of either process is determined by the physicochemical properties of the active pharmaceutical ingredient (API) and its thermal stability in relation to the printing technique. This is evident in Fused Deposition Modelling (FDM), which requires heat-stable drugs to be pre-incorporated into polymer filaments, whereas, in semi-solid extrusion (SSE), one can incorporate thermolabile drugs into viscous gels under mild conditions. Posts on design strategies classify and accomplish optimised compartmental designs. Devices exhibiting concentration gradients along their architecture are capable of achieving biphasic and pulsatile release profiles [39]. These types of release profiles imitate the pharmacokinetics of condition drugs where varying plasma concentrations are required. In this case, coaxial and core-shell techniques allow for control over the sequencing of release, where the outer layer is designed for immediate release and the core of the device is for sustained release. The API engineered within the device minimizes inter-drug and inter-drug excipient interactions enhancing stability and bioavailability. The ability to program drug loading is a 3D printing technology feature that transcend passive dosage forms into actively responsive release systems [38,39].
5.3 Multi-Drug Combinations (Polypills)
A major advantage of 3D printing in pharmacy is its ability to produce polypills, which are single dosage forms that combine several drugs. These systems streamline the delivery mechanism of various medicines packaged as single units. The active ingredients in the system are formulated to be released at different stages of therapy and each serves a particular clinical function [40]. The construction of such systems involves complex formulation, and the traditional approaches often fall short due to the inconsistency of the APIs and the conventional methods limitations in coating or layer construction. Pharmacy's use of 3D printing technology has addressed these concerns by making it possible to create a system in which each medication is digitally separated within a particular area of the polypill. For example, a printed tablet can contain several drug-releasing and non-releasing layers where the active ingredients are packed in different polymer matrices designed for varying dissolution rates or other pH responsive release mechanisms. One such example is a polypill designed for the treatment of cardiovascular diseases [41].
The polypill incorporates antihypertensive agents and lipid-lowering agents in a clinically controlled sequence to maintain side effects. 3D printing also enables the construction of multi-reservoir implants designed for the simultaneous delivery of multiple chemotherapeutic agents to a specific site which greatly enhances the therapeutic value of the medicines while reducing the toxic effects. The customizability of 3D printing enables tailored polytherapy in which the specific combination and dosages of each medication can be adapted to factors such as a patient’s genes, age, metabolism, and clinical conditions. Reduction in the number of tablets a patient has to take increases adherence to treatment, thus decreasing burden, which also ful-fills a more general objective of precision medicine. This is the discipline that adjusts therapeutics to biological and contextual parameters of the individual. Printing complex polypills on demand at hospitals or pharmacies enables decentralized, patient-centred production of pharmaceuticals [40,41].
5.4 Digital Design Workflow: Patient Data to Customized Print
What distinguishes personalized pharmaceutical 3D printing is the merging of digital design with patient-specific information. The process usually commences with obtaining patient data, which may include pharmacogenetics, medical imaging, or other physiological data. Based on this information, a computational model reflecting the patient’s physiological and anatomical structures necessary for understanding the absorption and metabolism of a drug is created—a process referred to as making a “digital twin.” Computer aided design (CAD) software is then used to match the digital model of the dosage form with the digital twin, where adjustments are made to the form’s geometry, drug load, and release profile to achieve a patient-centred therapy [42]. Digital technologies support the designer in realizing multiple iterations and tests virtually before any fabrication is done, effectively minimizing the trial-and-error iterations and expediting the translation of the design to practice. Once design fabrication is done, the 3D model is prepared for printing and sliced into layers for the printer to read, The layers were constructed sequentially, in accordance with the selected printing method and materials. The complete digitized pre- and in-printing integration process ensures the model is pharmaceutical safe, process adjustable, and compliant with regulations on reproducibility and documentation. Moreover, with the application of artificial intelligence (AI) and clouded databased technologies, continuous feedback on and optimization regarding design parameters is incorporated in the system. With real-time adjusted and personalized response metrics to patient response data [43]. All these exemplify the convergence of pharmacology, digital manufacturing, and data science. With the potential fabrication of adaptive therapeutics of automated modification based on dynamic patient parameters, this convergence emphasizes patient centred and responsive pharmacology [42,43].
5.5 Modelling and Simulation
Designing and optimizing 3D-printed dosage forms relies, to a significant extent, on modelling and simulation. Assessing the influence of material composition, geometry of 3D-printed structures, and other parameters on the degradation and mechanical characteristics, as well as drug release, becomes feasible. The use of finite element analysis (FEA) to predict mechanical stress and strain on a given structure helps evaluate its strength for preclinical handling and the in vivo performance. Mathematical and computational modelling of dissolution remains central to the anticipation of drug release and disintegration under a diverse set of physiological conditions. Predicting software-optimized release kinetics prior to 3D printing the construct allows developers to greatly reduce time and material resources [44]. Some of the more advanced or pioneering studies adopt computational fluid dynamics (CFD) to model the penetration of fluids and the diffusion of drugs within porous formations. Fine-tuning infill density and surface area are other optimization points in the drug-embedded porous structure. Integrating machine learning and AI significantly enhances predictive modelling by identifying the complex relationships between printing attributes and the results of the process. AI can recommend optimized combinations of printing parameters and material compositions for targeted medications for particular population of patient based on the analysis of thoroughly documented experimental results.
Predictive modelling streamlines the design process and improves the design process for regulatory approval by showing reproducibility and predictability of performance. Using modelling and simulations for 3D-printed drug designs helps the designer shift from a fully trial-based approach to a more scientific and data-driven approach, ensuring that each 3D-printed dosage form ful-fills defined therapeutic objectives with precision and uniformity [44].

Figure 7: Schematic of digital workflow for patient-specific drug printing.
6. APPLICATION OF 3D PRINTING IN DRUG DELIVER
The implementation of three-dimensional printing technology in the pharmaceutical science has shifted the field of drug delivery and customized medicine from conventional large-scale production to made-on-demand, patient-centred production systems [45]. Researchers and clinicians were able to create custom designed dosages due to the invention of 3D printing technology, implants, and delivery devices that have specific geometries and compositions and control the release of drug. This has opened considerable variations in the therapies that could be offered through the oral, transdermal, implantable and parenteral systems as well as through sophisticated technologies such as bioprinting and on-site manufacturing. The subsequent sections address the primary use of 3D printing technology in drug delivery focusing on the clinical aspect, technological variations and importance of regulation.
6.1 Oral Drug Delivery
The convenience, safety, and adherence of oral delivery route of drug administration makes it the most popular option. However, classical oral dosage forms do not address the requirement of patients on different metabolic levels, those who have different abilities to swallow, or those with certain specific dose requirements. The problem has been sufficiently solved with the design of oral tablets through 3D printing techniques which can result in customized release kinetics, mechanical strength, and organoleptic properties. In 2015, Aprecia Pharmaceuticals, with the introduction of Spritam® (levetiracetam), became the first company to receive the FDA approval for a 3D-printed tablet [46]. This was a monumental achievement in the field. Spritam® was manufactured with ZipDose® technology and uses a powder bed printing process to create very porous tablets that are suitable for patients with dysphagia or young children. The approval was a watershed moment, establishing 3D printing technology as a legitimate option for pharmaceutical manufacturing. Beyond fast-dissolving formulations, 3D printing has been applied to produce tailored-release tablets where dissolution rate and drug release can be controlled and customized based on geometry, infill density, and polymer selection. By varying infill patterns and layered structures, researchers have achieved sustained-release and pulsatile-release profiles within the same dosage form. This ability to print tablets of varying sizes and doses from a single digital model enables personalized dosing, which is crucial for dose titration in children, the elderly, and patients with renal insufficiency. Moreover, 3D printing can encapsulate and multi-layer to taste-mask medicated formulations, increasing adherence to paediatric formulations. Unpleasant tasting and odorous drugs can be included in the inner layers of a multi-layered formulation and the outer layers can be sweetened and flavoured, providing a palatable cover. With these advancements, the oral route has become the primary target for 3D printing in the pharmacy, integrating functional customizations with the design for the end user [46].
6.2 Transdermal and Topical Systems
With the inability to be invasive and the controlled release, along with the absence of hepatic first-pass drug metabolism, transdermal and topical delivery systems have become a topic of interest. 3D printing provides new avenues of construction for microneedle arrays, personalized dermal patches and topical scaffolds to deliver drugs through the skin with precise accuracy and low discomfort. Microneedle systems can be engineered for the SLA or SSE methods to create microneedles that deliver drugs into the dermis and permeate the stratum corneum. The needles of these microneedles are designed and manufactured to the desired geometry, height, and density to specify and optimize for the desired penetration depth and drug release kinetics. drug release kinetics. After permeation, effective and sustained drug release into the deep layers of the skin can be achieved with biodegradable microneedles made from PVP, PLA and hyaluronic acid. Customizable porosity and spatially varied drug reservoir configurations largely allow the making of transdermal patches using 3D printing technology. These patches can also be adjusted to certain body parts or different skin shapes for improved fit, comfort, and adherence. Customization, as asserted by Trivedi et al. (2024) [47], can enhance or even accommodate adherence to the body’s contours. Furthermore, patches can be design to compartmentalize numerous drugs for combination therapy, which can facilitate purposeful and extended transdermal therapy. As for bioprinting therapy, hydrogel patches with anti-inflammatory and antimicrobial agents effectively manage and treat wounds, burns, and inflammatory skin disorders. 3D printing technology in transdermal systems certainly provides a new level of refinement and versatility [47].
6.3 Implantable and Injectable Devices
3D printed implantable injectable devices have advanced localized long-term drug delivery, enabling elastomers to be placed directly at the drug delivery site like tumors, bone defects, or infections. This results in clinically relevant localized concentration and minimized systemic exposure. Moreover, the customization potential offered by additive manufacturing makes it enable to produce patient-specific, anatomically matched implants using CT and MRI scans. Custom, biodegradable, PCL, PLA, and PLGA derived porous implants loaded with chemotherapy and antibiotic polymers have been made. As polymeric scaffolds, implants can safely promote drug elution for several weeks and months while filling the biodegraded space and helping to heal the tissues and regenerate the structures [48]. In oncology, 3D printed devices are made for localized chemotherapy by embedding polymer matrices made at the site of tumor for direct localized delivery. Systemic toxicity is minimized by encapsulating cisplatin and doxorubicin, which is primarily used for localized chemotherapy. Within the field of orthopaedics, the aforementioned technologies 3D bioprinting and 3D printing bone graft substitutes and osteoconductive scaffolds of calcium phosphate, hydroxyapatite, and composite polymers along with the addition of growth factors and/or antibiotics opens a wide range of possibilities. 3D bioprinting also allows the minimally invasive administration of compound proteins, peptides, and biologics through the use of injectable hydrogel depots and controlled released microspheres. The integrated structural and functional implantable systems affirms the 3D printing adaptability regarding the composite polymers and opens exciting new possibilities for localized and highly targeted pharmacological therapy without the requirement for incisions [48].
6.4 Bio-printed Tissue Models
Bioprinting extends 3D printing by integrating living cells and biomaterials to create structures for regenerative medicine and pharmacology. Bio-printed models are vital in drug delivery for assessing new medications and determining their toxic effects and customized therapies. Conducting these evaluations reduces the use of animal models which amplifies the predictive accuracy for humans. Hydrogels containing cells such as gelatin methacrylate (GelMA), alginate, and collagen are employed as bioinks to fabricate three-dimensional (3D) structures that replicate the human tissue scaffolds. These structures make it possible to study the release, diffusion and metabolism of a drug in vitro within human physiology models [2]. 3D-bioprinted liver and tumor tissues, for instance, are instrumental in studying the pharmacodynamics and pharmacotoxicology of potential drug candidates as well as drug-cell interaction at a level that transcends what is possible with the older 2D cell culture systems. Moreover, the regenerative applications of bioprinting are also rapidly advancing, exemplified by the creation of scaffolds with healing and regenerating tissues containing drug-loaded bioinks. Constructs used in tissue engineering also integrate molecules with bioactive properties, including growth factors for healing and cartilage, skin, and scaffolds that promote blood vessel regeneration. The activities of the bioactive molecules and the cells are released in a prescribed and designed manner, providing control over the tissue regeneration. Consequently, bioprinting is integral to the integration of engineering of tissues with active pharmacological therapy, laying the groundwork for individualized regenerative therapy [2].
6.5 Rapid Prototyping and On-demand Manufacturing
A key advantage of 3D printing in the pharmaceutical sector lies in its capacity to quickly create and produce prototypes and products as needed, which fundamentally alters the entire supply chain and the way medicines are delivered. Traditional drug manufacturing processes are centralized, inflexible, and slow [4]. however, 3D printing enables dispersed, digital manufacturing. Healthcare facilities can obtain patient-specific dosage forms in real-time and print them right at the point of care in hospitals, clinics, and pharmacies [4]. Healthcare practitioners can input the patient’s parameters, choose the required combinations of drugs, and Print a customized medication tailored to the patient's requirements in a matter of few hours thanks to digital design and cloud-based workflows. This approach is exceptional for situations that require emergency medication, for orphan diseases, and for situations in clinical trials where small-batch or single-dose production is necessary. Personalized medicine and real-time data underlie the concept of "pharmacy-based printing," which involves adjusting doses dynamically to meet the needs of individual patients. Also, the ability to quickly test new designs speeds up development of formulations and testing for regulatory approval since scholars can modify and experiment with varying shapes, different materials and release profiles, all of which can be done without costly moulds and tools. Such flexibility facilitates inventive progress in adapting paediatric and geriatric formulations where considerations of dimensions, configuration, and dosing vary considerably. This is coupled with innovations in automation, artificial intelligence, and novel policy frameworks, which will likely shift the emphasis of healthcare toward accessibility, sustainability, and precision by making on-demand 3D-printed medications a reality [4].
7. EVALUATION PARAMETERS
Assessing and characterizing 3D printed pharmaceutical drug delivery systems will make sure the product has the quality and consistency to satisfy the required therapeutic efficacy. 3D printed drugs entail more complex geometries, more materials, and novel manufacturing processes, which need to be validated through more comprehensive analyses compared to more traditional pharmaceutical dosage forms. To determine the compatibility of the drugs and excipients, the structure integrity, and the criteria for controlled release in the integrated disciplines of the physicochemical, mechanical, and pharmacokinetic the integration must be evaluated. The physicochemical will be the first step in quality assurance [5]. Within the different variations of the Differential Scanning Calorimetry (DSC), the drug’s thermal behaviour and the polymers will be assessed for the determination of melting point, glass transition temperatures, and decomposition which will occur during printing. The chemical interactions between the active pharmaceutical ingredients (APIs) and the excipients is assessed to determine any possible interactions in the extrusion or photopolymerization processes using Fourier Transform Infrared Spectroscopy (FTIR).
Scanning Electron Microscopy (SEM) improves our understanding of the surface and internal microstructures of the drug constructs, all of which affect drug release and dissolution kinetics, along with the morphological, porosity, and microstructures. To determine the bioavailability and solubility of the drug, X-Ray Diffraction (XRD) is used which distinguishes the crystalline and amorphous forms of the drug. Assessing the mechanical properties helps determine performance robustness and how the printed dosage forms would handle and stability. These include hardness, friability, tensile strength, and elasticity which are performed using the standard tablet testing apparatus. For disintegrating tablets, which have low hardness and high friability, the mechanical properties must fit the intended purpose. In dissolution testing using the USP apparatus I or II, active ingredient release rates are measured and compared with design parameters like infill density and surface area [5]. Specific release kinetics are predictable and reproducible due to the iterative testing on release. Geometric and material parameters are changed to achieve this. Another critical phase is the release profile and drug content quantitative evaluation. Quantitative tools such as high-performance liquid chromatography (HPLC) and UV-visible spectrophotometry assess the analytical drug profile and determine the uniformity of drug distribution and loading in the printed matrix. This also checks if the printed output corresponds with the target personalized dose, which is vital in personalized medicine [5].
In vitro studies that evaluate the erosion, diffusion, or swelling control mechanisms of drug release are the first studies that provide information on the potential therapeutic benefits of a solid printed dosage form. This information is also essential in advancing the more sophisticated stages of drug release studies [5]. For the printed formulation, stability testing determines the effect of the various elements of the environment (temperature, humidity, or light) on the formulation’s shelf life. Light and heat are also stability-testing elements for some 3D-printed systems which contain heat-sensitive APIs and use photopolymerizable resins. For reproducibility, multiple batches are printed and the stored parameters for comparison are the drug content, weight variations, and dissolution rates. As for the entire process of additive manufacturing, reproducibility on the small and large scales remains the main issue unsolved. Legislation compliance remains the means toward the end of this automation. Characterization process completes In vitro and In vivo Correlation (IVIVC) integration. The integration conjoins laboratory dissolution data and in vivo absorption data to estimate therapeutic performance [7]. A strong IVIVC will promote the development of a formulation and the coveting of the formulation's regulatory approval for use in new dosage forms. These methods, integrating, provide thorough elucidation and the approval of the 3D-printed pharmaceuticals [7].
8. REGULATORY, ETHICAL, AND QUALITY CHALLENGES
The challenges that the demand be addressed before the clinical adoption of 3D printing in pharmaceuticals expands on a global scale are largely regulatory and ethical in nature. The safety and quality of additive manufacturing products need improvement, and the FDA, EMA, and ICH need to enhance their regulatory approaches [55]. All three have claimed to be developing more comprehensive regulations regarding these issues. From a regulatory perspective, issues unique to 3D printing that do not exist in traditional manufacturing are concerning [56]. For example, each printed dosage form can differ in design, dosage, and geometry. This variation challenges the traditional definition of a ‘batch’ or ‘lot.’ The FDAs recently released guidelines on 3D printing emphasize the need for adherence to GMP, particularly in decentralized or hospital-based production environments. Risks regarding material control, process validation, and traceability of products are concerning and need to be addressed. The regulatory position concerning digital files, design blueprints, and patient-specific prescriptions is even now in its early stages and raises issues of data security, as well as concerns regarding the authenticity and ownership of the files. Quality control management remains yet another unresolved issue. Traditional pharmaceutical manufacturing processes show operational units consistently delivering results. With 3D printing, results are delivered incrementally. 3D printing operations can, under certain conditions, be calibrated, displaced, and controlled, allowing for variability and unpredictability in production. The complexities of formulation validation will require routine operational validations for 3D printing. Among other things, product differences will arise from varying laser intensity, disparate extrusion temperatures, and differences in layer height [57]. Customization of 3D printed medications will raise ethical concerns regarding risk, exposure, and the provision of unsupported claims when resolution of dosages is necessary [58]. Control of some adjustments in therapeutic dosages is required to avoid therapeutic failure while excessive personalized dosing may result in serious adverse consequences. Respecting intellectual property rights is necessary for digital design of 3D printed pharmaceutical products as they can be easily modified, and pose serious, unique, and unprecedented patenting and counterfeit challenges. Data integration into 3D digital designs is also necessary for replication. For the industry to develop, collaboration among the industry, policy makers, and the academic community will be crucial to facilitate the timely and advantageous 3D printed medicine to the world [58,59].
9. LIMITATION AND CURRENT CHALLENGES
Alongside the remarkable liberties and precision offered by 3D printing, there are notable practical and technical obstacles. Reproducibility is one of the main obstacles in 3D printing. Inconsistent print quality is mainly due to stochastic variations in the printing variables, constituent materials, and the surrounding environmental conditions. Additive manufacturing differs from conventional batch processing utilized in the pharmaceutical sector in the sense that it is far more sensitive to variations in temperature, clogging of the printing nozzles, and changes in printing speeds. These in turn affect the drug loading and release characteristics of the polymer [60]. The minimal availability of 3D printers that are capable of operating at an industrial scale is another factor that discourages potential users and implementation within the industry. Compared to pharmaceutical compression and coating, 3D printers are considerably slower, making high-throughput printing an impractical option at this time. In personalized medicine, this difference in scale is less of an issue than accuracy, printing flexibility, and the potential for automation, which is now the preferred option. The limited availability of materials that can be 3D printed is a considerable reason for this absence [61].
The range of polymer excipients and active pharmaceutical ingredients (APIs) that can be used is far greater than the range of grades that are acceptable for 3D printing. Number of active pharmaceutical ingredients become ineffective if exposed to high heat or UV light in 3D printing processes like as fused deposition modelling and stereolithography which limits the types of ingredients that can be used and incorporated. In addition, the post processing steps that remain after 3D printing, such as curing, drying, and sterilization transition the product into a more stable and acceptable form but can also affect the mechanical and chemical stability adversely [62]. In the case of implantable or bio-printed products, sterilization and regulatory validation can be particularly troublesome. In fact, autoclaving and gamma irradiation, while being conventional sterilization techniques, may ruin the integrity of the material, be it polymeric or bioactive. Moreover, the situation where regulatory and testing standards remain undocumented presents issues that neither enable the comparison of study results nor make the approval processes more rapid [62,63].
10. FUTURE PERSPECTIVE AND EMERGING TRENDS
Technological convergence will define the future prospects of three-dimensional printing in the pharmacy. The convergence of materials science with digital design coupled with artificial intelligence will develop adaptive smart biomedical therapeutic systems. Of the many concepts that will emerge from the convergence of these fields, 4D printing will be the most transformative. 4D printing not only surpasses 3D printing, but it also creates systems that are responsive to different stimuli [64]. These systems are able to change their structures, porosities, and drug release patterns in response to temperature, pH, and magnetic fields. The development of such dynamic systems poses the potential creation of self-adjusting drug delivery systems that can adjust to the real-time changing physiology of patients. The potential of artificial intelligence and machine learning integration in the design and printing process optimization is another area of advancement. Artificial intelligence can analyse previously defined print parameters, material characteristics, and release profiles to define and reduce the parameters of the trial and error process. The creation of digital twins will further enhancement of real-time monitoring, predictive modelling, and personalized therapy optimization. These digital twins are virtual replicas of printed dosage forms. The advanced systems that will be created with sensor-integration and automated drug systems will be shaped by the advancements of smart drug delivery systems [65]. Micro-sensors that monitor and respond to alteration in pH, temperature, and drug concentration will control feedback responsive drug release. These systems will be invaluable in the treatment of chronic diseases such as diabetes and cancer, as dynamic, continuous, real-time monitoring, and responsive dosing are essential. On-demand hospital printing is expected to be one of the first applications of personalized medicine. For pharmacists, the ability to print custom tablets or implants can be done in real time for individual patients. When the integration of advanced technology into the printing process occurs, emergency compartments will be able to print with little delay or necessary logistical hurdles [66]. Researchers look to innovate more sustainable mechanisms in biomedicals and incorporate biomaterials to be fully recyclable, the use of cellulose and biodegradable polymers are included. 3D printing facilitates the sustainable production of pharmaceuticals by eliminating large-scale infrastructure and waste to achieve environmentally “clean” production [67]. Over the next 10 years, the combination of 4D printing, AI, and advanced bioprinting is expected to rewrite the paradigms of therapeutic drug delivery to flexible, personalized systems, in place of current rigid, one-size-fits-all approaches [64-67].
11. CONCLUSION
The incorporation of 3D printing technology into the pharmaceutical industry allows for the integration of personalized medicine with dual digital 3D printing technology for the first time. This innovation offers opportunities for the customization of individual patient therapies. Specific technologies such as fused deposition modeling, binder jetting, stereolithography, and bioprinting have made it possible to diversify drug delivery systems, offering the pharmaceutical industry the construction of systems like oral, transdermal, implantable, and engineered living tissue systems. Although the challenges of regulation, scale, and decision-making regarding materials to be used for printing, the pace of innovation in 3D printing technology coupled with the innovation of materials and AI in other disciplines, will mean the fulfillment of the goals of geared personalized medicine will be within reach. 3D printing technology, with its ability to innovate pharmaceutical medicine, is positioned to revolutionize the industry for the on-demand personalized medicine approach.
ACKNOWLEDGEMENT
The authors are thankful to the faculty and staff of the SMES's Mahavir Institute of Pharmacy, Nashik, Maharashtra, India, for providing the necessary facilities, support and guidance to complete this review work.
AUTHOR CONTRIBUTION
All authors participated in the conceptualization and design of the review. The literature search and data extraction were conducted collectively. The initial manuscript was drafted by the authors, and all members contributed to the critical revision and editing for intellectual content. All authors have read and approved the final version of the manuscript for submission.
REFERENCES




Kajol Echale, Mahevish Shaikh, Vaishnavi Chauthe, Dr. Anil Jadhav, Customization of Drug Delivery using 3D Printing Technologies: A Material Driven Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1372-1400. https://doi.org/10.5281/zenodo.18245395
 10.5281/zenodo.18245395
10.5281/zenodo.18245395