1Department of Pharmacology and Clinical Pharmacology, Christian Medical College, Vellore.
23Department of Pharmacology, Government Medical College & Hospital, Tiruvallur. -480337
Background: Assessment of prescribing patterns is an important approach to evaluate the quality of healthcare delivery and promote rational drug use. The World Health Organization (WHO) prescribing indicators serve as standardized tools to assess drug utilization practices in healthcare settings. Objective: To analyze drug prescribing patterns in the outpatient department (OPD) of a tertiary care hospital in Thiruvallur using WHO core prescribing indicators. Methods: A prospective, cross-sectional observational study was conducted in the OPD over a two-month period (February–March 2024). A total of 665 randomly selected prescriptions were evaluated using WHO prescribing indicators. Data were compiled in Microsoft Excel 2021 and analyzed using descriptive statistics. Results: A total of 2,628 drugs were prescribed, with a mean of 3.94 drugs per encounter, indicating polypharmacy. Generic prescribing was observed in approximately 90% of drugs, and 98% were from the WHO Essential Drugs List. Antibiotics were prescribed in 35% of encounters, while injections accounted for 3%. Amoxicillin was the most frequently prescribed antibiotic, mainly for respiratory tract infections. Vitamin supplements and antiulcer drugs were the most commonly prescribed therapeutic classes. Conclusion: The study demonstrates appropriate practices regarding the use of essential medicines and injections. However, the higher average number of drugs per prescription and antibiotic use highlight the need for interventions aimed at reducing polypharmacy and promoting rational antibiotic prescribing
The evaluation of drug prescription patterns constitutes a fundamental aspect of patient care and serves as a critical indicator of the quality, safety, and efficiency of healthcare delivery systems. (1) Prescribing is one of the most complex and influential therapeutic decisions made by clinicians, as it directly affects clinical outcomes, healthcare costs, and patient safety. An optimal prescription should be evidence-based, individualized, cost-effective, and aligned with established treatment guidelines.(2) Consequently, systematic assessment of prescribing practices is essential for ensuring rational drug use and maintaining high standards of medical care.(3)Prescription pattern analysis is a valuable methodological tool that provides comprehensive insights into prevailing trends in drug utilization, therapeutic appropriateness, and compliance with standard treatment protocols. By examining prescribing behaviors, such analyses help identify irrational practices such as polypharmacy, inappropriate selection of drugs, unnecessary use of antibiotics and injections, and deviations from recommended clinical guidelines. These inappropriate prescribing practices not only increase the economic burden on patients and healthcare systems but also elevate the risk of adverse drug reactions, drug–drug interactions, and poor treatment adherence.(4)Inappropriate and excessive use of antimicrobial agents remains a major global public health concern, contributing significantly to the growing problem of antimicrobial resistance. Similarly, unjustified use of injectable formulations increases healthcare costs and exposes patients to avoidable risks such as injection-related infections. Therefore, continuous monitoring of prescription patterns plays a vital role in promoting rational pharmacotherapy, minimizing medication-related harm, and optimizing therapeutic outcomes. (5)To facilitate standardized evaluation of drug use practices across healthcare settings, the World Health Organization (WHO) has developed a set of core drug use indicators. These indicators are simple, reliable, and universally applicable tools designed to objectively assess prescribing practices in health facilities. The WHO prescribing indicators specifically evaluate the degree of polypharmacy, the extent of generic prescribing, the frequency of antibiotic and injection use, and adherence to the Essential Drugs List (EDL) or institutional formulary. Collectively, these parameters serve as key measures of rationality, cost-effectiveness, and standardization in prescribing behavior.(6) Assessment of polypharmacy provides insight into the tendency to prescribe multiple medications per patient encounter, which is often associated with increased risk of adverse drug events and reduced patient compliance. Generic prescribing promotes affordability, improves access to essential medicines, and supports sustainable healthcare delivery. Monitoring antibiotic and injection prescribing patterns helps identify irrational use that may contribute to antimicrobial resistance and unnecessary healthcare expenditure. Adherence to the EDL or hospital formulary reflects the extent to which prescribing practices align with national and institutional policies aimed at promoting safe and effective medication use.(7) Drug utilization research primarily aims to ensure the rational use of medicines at both individual and population levels. According to WHO, rational drug use implies that patients receive medications appropriate to their clinical needs, in doses tailored to individual requirements, for an adequate duration, and at the lowest possible cost to both patients and the community. Failure to adhere to these principles can lead to therapeutic failure, increased morbidity, higher treatment costs, and the emergence of drug resistance. (5)Given that medicine is a continuously evolving science with frequent updates in clinical guidelines and therapeutic options, regular evaluation of prescribing trends is imperative.(8) Periodic prescription audit and monitoring studies provide an evidence-based framework for identifying gaps in current practices, improving therapeutic decision-making, updating institutional formularies, and designing targeted educational interventions for prescribers. Such initiatives are essential for fostering rational prescribing habits and enhancing the overall quality of healthcare services.In this context, the present study has been undertaken to assess drug prescribing practices in the medical outpatient department of a tertiary care teaching hospital in Tamil Nadu using the WHO-recommended core prescribing indicators. The findings of this study are expected to provide valuable insights into existing prescribing patterns, identify areas requiring intervention, and contribute to the promotion of safe, effective, and economical use of medicines in routine clinical practice.
Aim and Objective:
To assess the WHO prescribing indicators in prescriptions given at outpatient department (OPD) of a tertiary care hospital, in Thiruvallur.
MATERIAL AND METHODS:
A prospective cross sectional observational study was carried out in the outpatient department of a tertiary care hospital, in Thiruvallur. The study was started after approval from the institutional ethics committee and the hospital authorities. The study was conducted in a tertiary care hospital, in Thiruvallur from February 2024 to March 2024 for duration of 2 months. The study included prescriptions collected randomly from all OPDs. Prescriptions were scanned for the record purpose. Prescriptions were handwritten and not electronic. Data obtained from 665 prescriptions based on the WHO guideline of including at least 600 patient encounters from the previous reference article. (1,6)Prescriptions of patients attending medical OPD and treated on outpatient basis for their ailments were included irrespective of the comorbidities. Basic demographic information in form of age, sex, diagnosis and treatment prescribed were recorded. Data were analysed as per WHO prescribing indicators. (6)
These are as follows:
The data were entered in Microsoft Excel 2021 and analysed as frequency distributions and percentages to assess the prescribing indicators.
RESULT
A total of 665 prescriptions were analysed over 2 months from February 2024 to March 2024. The demographic distribution of patients mirrored a decreasing trend with increasing age as a higher proportion of patients 50% (332) were <40 years and those aged 40 - 60 years were 31% (207) while 60 years and above were 19% (126) [Figure 1].
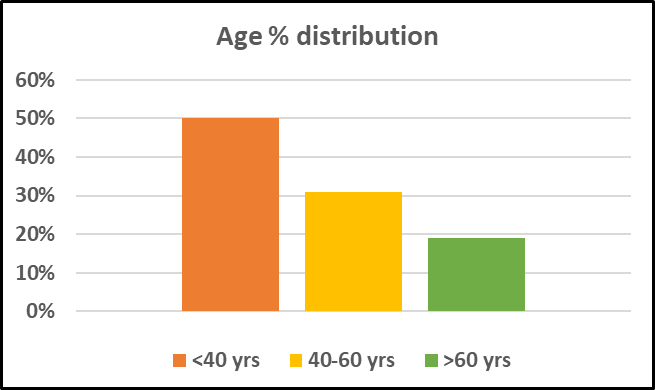
Figure 1: Age % distribution
Males were about 66% (440) compared to females 34% (225). Diagnoses were multiple and diverse. It was found that a total number of 2628 drug products had been prescribed in the 665 patient encounters, and thus, the average number of drugs per prescription was 3.94 and the standard deviation was 1.6 [Table 1]. Moreover, the median number of drugs per prescription was 4, which unlike the mean, would not be unduly influenced by the outliers. Analysing the patient encounters, it was found that 2376(90%) drugs were prescribed in generic names and 98% of drugs were from essential drugs list. It was evident that 35% of prescriptions had antibiotics and only 3% injections were prescribed. The most common indication for the antibiotic use was found to be Respiratory tract infections (29%) and the most common antibiotic used was Amoxicillin (56%). The number of prescriptions with fixed drug combinations was 18 accounting for 3%. The most common one being prescribed was Cotrimoxazole antibiotic.
Table 1: Comparison of the World Health Organization prescribing indicators observed with standard reference range
|
Indicator |
n |
Average/ percentage (SD) |
Standard reference range |
|
Average number of drugs per patient encounter |
2628 |
3.94 (1.6) |
1.6-1.8 |
|
Percentage of drugs prescribed by generic name |
2376 |
90% |
100% |
|
Percentage of encounters with an antibiotic prescribed |
234 |
35% |
20.0%- 26.8% |
|
Percentage of encounters with an injection prescribed |
18 |
3% |
13.4%-24.1% |
|
Percentage of drugs prescribed from essential drugs list |
2583 |
98% |
100% |
SD: Standard deviation
It was interesting to find that among the 2628 drug products prescribed, the highest percentage (18%) of prescribed drugs were supplements which ranked first followed by the antiulcer drugs (10%), antipyretics (9%), antibiotics (9%), anti-hypertensive drugs (7.5%), antidiabetic drugs (6.5%), NSAIDs (5%), antiplatelet drugs (3%), antiepileptics (2%), antihistaminic drugs (2%) and hypolipidemic drugs (2%) [Figure 2].
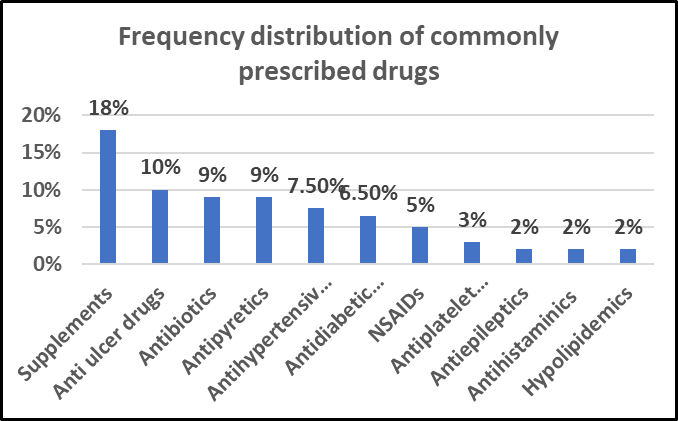
Figure 2: Frequency distribution of commonly prescribed drugs
DISCUSSION
The evaluation of prescribing indicators provides an objective measure of the performance of healthcare providers across key dimensions of rational drug use. In the present study, prescribing practices were assessed using WHO core prescribing indicators based on 665 patient encounters from the outpatient department of a tertiary care teaching hospital. The findings offer important insights I nto current prescribing trends and highlight areas requiring targeted intervention. The average number of drugs prescribed per encounter in our study was 3.94, which exceeds the WHO-recommended optimal range of 1.6–1.8. (7) This observation indicates a relatively high degree of polypharmacy in the study setting. Comparable studies conducted in Tamil Nadu (1) have reported a lower average number of drugs per prescription (2.95), whereas figures reported by Upadhyay et al. (3.76) were slightly lower than our findings, and those by Raj et al. (4.98) were higher.(8–10) In contrast, studies from other countries such as Sudan, Zimbabwe, and Ethiopia have documented substantially lower averages, ranging from 1.3 to 1.9 drugs per encounter.(11) These differences may reflect variations in disease burden, healthcare infrastructure, prescribing policies, and availability of essential medicines across regions. The high level of polypharmacy observed in this study may be partly attributed to the evolving epidemiological transition characterized by a rising prevalence of non-communicable diseases such as diabetes mellitus, hypertension, dyslipidemia, and coronary artery disease. (12) These chronic conditions frequently coexist in the same patient, necessitating multiple pharmacological interventions for effective disease control. Furthermore, patients with cardiometabolic comorbidities often require combination therapy to achieve therapeutic targets, which may contribute to an increased number of prescribed medications per encounter. While such prescribing may be clinically justified in certain contexts, it nonetheless warrants careful evaluation to minimize unnecessary drug exposure and potential adverse outcomes. An additional contributor to polypharmacy identified in this study is the excessive prescription of nutritional supplements, which often lacks clear clinical justification. The widespread perception among patients that supplements are inherently beneficial for health may lead to increased demand for such products. Yielding to patient expectations without appropriate clinical indication can foster irrational prescribing practices. Addressing this issue requires effective patient education aimed at correcting misconceptions and reinforcing evidence-based therapeutic decision-making among prescribers. (13)Generic prescribing is a key component of rational drug use, as it promotes affordability, accessibility, and sustainability of healthcare. In the present study, 90% of drugs were prescribed by their generic names, which, although encouraging, falls short of the WHO ideal value of 100%. (7) Previous literature indicates that generic prescribing rates tend to be higher in public sector institutions compared to private healthcare facilities. The residual preference for brand-name prescribing may be influenced by prescriber apprehensions regarding bioequivalence, perceived differences in quality, and pharmaceutical marketing practices. (14)Enhancing generic prescribing practices necessitates a multifaceted approach. Incorporating pharmacoeconomic principles into undergraduate medical education, conducting regular continuing medical education programs for clinicians, and addressing misconceptions related to the efficacy and safety of generic medicines are crucial strategies. Additionally, policy-driven measures such as enforcing statutory regulations, establishing clear institutional guidelines, and discouraging brand-name prescribing through legal and administrative mechanisms have been recommended to overcome existing barriers.The proportion of encounters in which antibiotics were prescribed in this study was 35%, which is higher than the WHO reference standard. (7) This finding raises concerns regarding the potential for inappropriate antibiotic use and the associated risk of antimicrobial resistance. However, it is important to note that the study duration was limited to two months, and therefore seasonal variations in infectious disease prevalence—which significantly influence antibiotic prescribing patterns—may not have been fully captured. In contrast, the percentage of encounters involving injectable formulations was low (3%), reflecting a positive trend toward minimizing unnecessary injection use. Reduced reliance on injectable drugs decreases the risk of injection-related complications and contributes to cost-effective patient care. Adherence to the Essential Drugs List was notably high in the present study, with 98% of prescribed medications conforming to the WHO EDL or hospital formulary. This finding is comparable to results from other Indian studies and exceeds adherence rates reported from countries such as Tanzania, Ethiopia, and Nepal. Similar to generic prescribing patterns, EDL adherence has been shown to vary between public and private healthcare sectors, underscoring the need for wider adoption of essential medicine policies across all levels of healthcare delivery. (15)One of the major strengths of this study lies in its prospective design, which involved direct analysis of prescriptions issued during outpatient visits. This approach minimizes data duplication and reduces bias associated with incomplete or inaccurate medical records, which are common limitations of retrospective prescription audits. Prospective data collection also enhances the reliability and validity of the findings.The results of this study emphasize the need for structured interventions such as educational workshops, training programs, and awareness campaigns aimed at promoting rational prescribing practices among healthcare professionals. By identifying existing gaps and suggesting corrective strategies, this research contributes to ongoing efforts to improve the quality of pharmacotherapy and patient safety.
CONCLUSION:
The present study demonstrates that while prescribing practices related to injectable use and adherence to the Essential Drugs List are largely rational and satisfactory, the extent of polypharmacy and antibiotic prescribing exceeds recommended standards. Although generic prescribing rates are relatively high, they remain below the ideal target. These findings underscore the need for targeted interventions to reduce unnecessary polypharmacy, promote complete generic prescribing, and encourage judicious use of antibiotics. Implementation of educational initiatives, institutional guidelines, and policy-level measures will be essential to strengthen rational prescribing practices and enhance patient safety and cost-effective healthcare delivery.
REFERENCES



Raja Priya, N. Asvini, G. Hemavathy, Drug Prescription Pattern at Outpatient Department in A Tertiary Care Hospital in Tiruvallur, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1642-1649. https://doi.org/10.5281/zenodo.18608409
 10.5281/zenodo.18608409
10.5281/zenodo.18608409
