1,2 R. G Sapkal College of Pharmacy, Sapkal Knowledge Hub, Kalyani Hills, Anjaneri, Trimbakeshwar Rd, Nashik, Maharashtra, India 422213
3 Mahatma Gandhi Vidyamandir's Pharmacy College, Panchavati, Nashik, Maharashtra, India 422003
4 MCE Society’s. Allana College Of Pharmacy, Hidayatullah Rd, New Modikhana, Azam Campus, Camp, Pune, Maharashtra, India 411001
5 RJS College Of Pharmacy, Kopargaon, Aahilyanager, Maharashtra, India 423601
Multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) remains a significant obstacle to global efforts in controlling TB, hindering advancements toward elimination goals. The emergence of MDR/RR-TB is mainly due to chromosomal mutations such as rpoB (rifampicin), katG/inhA (isoniazid), pncA (pyrazinamide), and gyrA/gyrB (fluoroquinolones), in conjunction with bacterial survival strategies like efflux pumps and dormancy. The heaviest impact is felt in low- and middle-income nations, where issues like poverty, co-infection with HIV, malnutrition, and weak healthcare systems worsen transmission rates and mortality. Diagnostic capabilities have improved with molecular technologies such as Xpert MTB/RIF, Xpert MTB/XDR, and Line Probe Assays, which allow for quicker detection of resistance compared to traditional culture methods. Whole Genome Sequencing provides extensive profiling and monitoring advantages, but its high cost and infrastructure needs limit its broad application. Treatment strategies have shifted from long, toxic injectable regimens to all-oral, more condensed options that include new drugs like bedaquiline, delamanid, pretomanid, and linezolid. The WHO now supports six- to nine-month treatment regimens like BPaLM that enhance outcomes and patient adherence. However, concerns about toxicity, the development of resistance to new medications, and limited access persist as critical challenges. Future approaches should prioritize affordable diagnostic tools, innovative treatment options, therapies aimed at host responses, digital tools for adherence, and enhanced global cooperation to ensure equitable access and continued progress toward the End TB objectives.
Tuberculosis (TB), which is caused by Mycobacterium tuberculosis, continues to be a significant global health issue, particularly in low- and middle-income nations. Despite ongoing international initiatives, TB remains one of the top ten causes of death and the leading infectious agent responsible for mortality, exceeding HIV/AIDS. In 2022, it was estimated that 10.6 million individuals contracted TB, with 1.3 million deaths recorded, highlighting its ongoing impact1. A particularly troubling issue is the rise of drug-resistant TB, especially multidrug-resistant TB (MDR-TB) and rifampicin-resistant TB (RR-TB). MDR-TB is characterized by resistance to at least isoniazid and rifampicin, the two most effective first-line anti-TB medications, while RR-TB specifically refers to resistance to rifampicin, which may or may not accompany resistance to other first-line drugs. These resistant forms of TB are notably more challenging and expensive to treat, often necessitating extended therapy with second-line medications that are less effective and have greater toxicity. In 2022, it was reported that around 410,000 individuals developed MDR/RR-TB, contributing to nearly 160,000 deaths, with India, China, and Russia facing the greatest challenges2.
Drug resistance in TB develops through two main processes: transmission of resistant strains (primary resistance) and the acquisition of resistance due to insufficient or incomplete treatment. Various risk factors propel the spread of MDR/RR-TB, including previous TB treatment, co-infection with HIV, malnutrition, substance dependence, poverty, and restricted access to quality healthcare. Delayed diagnosis, interruptions in treatment, stigma, and mental health issues also hinder adherence and exacerbate the global crisis. In response, the World Health Organization (WHO) and global partners have developed updated guidelines to enhance diagnostic, treatment, and surveillance methods3. Rapid molecular diagnostics, including the Xpert MTB/RIF assay, Xpert Ultra, and line probe assays, have transformed TB detection by allowing for the identification of both TB and rifampicin resistance within hours. Whole-genome sequencing (WGS) is being increasingly utilized to predict drug resistance and for molecular epidemiology, although access remains limited in resource-poor environments. Therapeutically, the advent of new medications like bedaquiline, delamanid, and pretomanid has broadened treatment options, facilitating shorter, fully oral regimens with higher efficacy. Additionally, host-directed therapies, repurposed drugs, and innovative combinations are under investigation4. Despite these advancements, significant challenges remain especially in low-resource areas where access to rapid diagnostics and new medications is still restricted, and health systems are further strained by the ongoing ramifications of the COVID-19 pandemic. In addition to diagnostics and therapies, innovations such as digital adherence technologies, artificial intelligence-based surveillance, and the creation of new TB vaccines are emerging as complementary strategies for managing MDR/RR-TB. However, effective management necessitates not only scientific and clinical advancements but also robust political commitment, fair health financing, and community engagement to mitigate stigma and enhance adherence5.
This review examines the intricate landscape of MDR/RR-TB by investigating the underlying mechanisms of drug resistance, current epidemiological patterns, advancements in diagnostics and treatments, and new strategies for disease management. By synthesizing recent findings and global guidelines, this paper underscores both ongoing challenges and promising innovations in tackling drug-resistant TB5.
The pathophysiology and mechanisms behind drug resistance:
Mycobacterium tuberculosis (M. tuberculosis), the bacteria responsible for tuberculosis, can be understood as follows: M. tuberculosis is a slow-growing, acid-fast, aerobic bacillus characterized by a uniquely intricate cell wall comprised of mycolic acids, glycolipids, and arabinogalactan. This lipid-dense structure inherently resists numerous conventional antibiotics and disinfectants and enables the bacteria to survive within macrophages by circumventing host immune responses. Its replication rate is slow, with a generation time ranging from 15 to 20 hours, which contributes to the persistent nature of tuberculosis and complicates treatment efforts since most antimicrobials are more effective against rapidly dividing organisms6. Although the primary infection site is the lungs, the bacteria can spread to other organs through the bloodstream. Within the host, M. tuberculosis exists in granulomas, organized immune structures consisting of macrophages, lymphocytes, and various immune cells. In this environment, the bacilli can remain in a dormant state for years, potentially reactivating when the immune system weakens, which poses significant challenges for treatment and increases the risk of relapse7.
Drug resistance in M. tuberculosis typically results from spontaneous chromosomal mutations rather than plasmid-mediated gene transfer, which is more prevalent in other bacterial species. These genetic changes alter the drug targets, lessen drug activation, or boost bacterial survival mechanisms, ultimately making treatment unsuccessful. Resistance to rifampicin a key indicator of multidrug-resistant tuberculosis often arises from mutations in the rpoB gene, which encodes the β-subunit of RNA polymerase. Such mutations occur within the rifampicin resistance determining region (RRDR), leading to decreased drug affinity for its binding site. Resistance to isoniazid generally stems from mutations in the katG gene, encoding the catalase-peroxidase enzyme necessary for prodrug activation8. Mutations in the inhA promoter region also play a role by increasing the expression of enoyl-acyl carrier protein reductase, the target of the drug, thereby reducing susceptibility. Additional genes, including ndh, kasA, and ahpC, contribute to the fine-tuning of isoniazid resistance mechanisms9.
Similar mutation-driven processes are involved in resistance to other first-line drugs. Ethambutol resistance is often associated with mutations in embB, which encodes arabinosyl transferase enzymes critical for the synthesis of arabinan in the mycobacterial cell wall. Pyrazinamide resistance commonly occurs due to mutations in pncA, which encodes the enzyme pyrazinamidase necessary for drug activation, although mutations in rpsA and panD have also been identified8. Genetic changes also affect second-line medications, including fluoroquinolones and aminoglycosides. Mutations in gyrA and gyrB located in the quinolone resistance–determining region interfere with fluoroquinolone binding to DNA gyrase, while aminoglycoside resistance arises from alterations in rrs (16S rRNA), rpsL (S12 ribosomal protein), or increased expression of eis, which inactivates kanamycin through acetylation10 (Figure No. 1).
Newer treatments, while promising, are also subject to resistance development. Resistance to bedaquiline can result from mutations in atpE, which encodes a subunit of ATP synthase, or from the upregulation of efflux pumps like mmpL5-mmpS5. Delamanid and pretomanid require activation by enzymes encoded by ddn and fbiA/B/C; mutations in these genes, or in fgd1, can impede drug activation and effectiveness. Resistance to linezolid, another essential newer drug, has been associated with mutations in rrl (23S rRNA) and rplC (ribosomal protein L3), both of which modify ribosomal binding11.
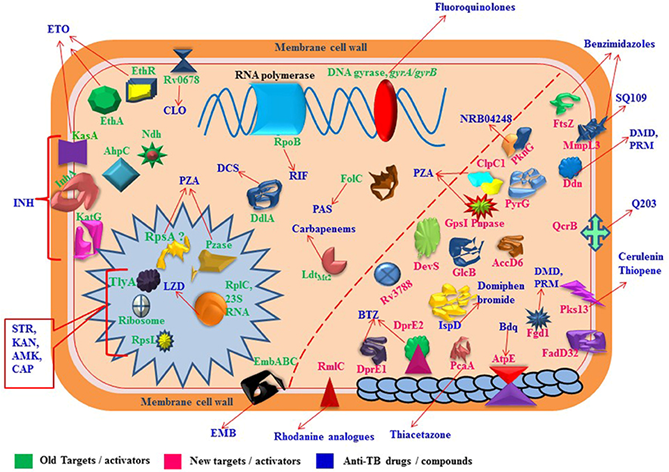
Figure 1: Molecular Targets Related Drug Resistance Mechanisms in MDR-, XDR-, and TDR-Mycobacterium tuberculosis Strains.
In addition to specific gene mutations, other mechanisms play a role in promoting drug resistance in M. tuberculosis. The overexpression of efflux pumps, including members of the mmpL family and Rv1258c, reduces intracellular drug concentrations and contributes to multidrug tolerance. Furthermore, the thick, waxy cell wall rich in mycolic acids presents a physical barrier that restricts drug penetration. Additionally, the presence of non-replicating "persister cells" allows the bacteria to endure antibiotic pressure without genetic changes, creating a reservoir for relapse after treatment cessation. Regulatory networks, such as the transcriptional regulator whiB7 and various sigma factors, further integrate responses to environmental stress with resistance pathways, enhancing the adaptability of the bacteria under adverse conditions12. The combination of molecular and physiological mechanisms illustrates the impressive resilience of M. tuberculosis. The interaction of genetic variations, efflux-mediated tolerance, dormancy, and cell wall impermeability clarifies why managing drug-resistant tuberculosis continues to be one of the most challenging infectious diseases12.
Transmission vs. Acquired Resistance:
Resistance to anti-tuberculosis medications arises through two principal pathways: primary resistance and acquired resistance. Primary resistance occurs when individuals are infected with drug-resistant strains of Mycobacterium tuberculosis, often transmitted from patients with improperly treated or recurring TB11. This type of resistance emphasizes the vital role of community-level transmission in sustaining the MDR/RR-TB epidemic. Conversely, acquired resistance develops during treatment, typically due to inadequate or incomplete therapy, insufficient drug regimens, poor patient adherence, drug interactions, or the use of inferior or counterfeit medications. In areas heavily burdened by the disease, both pathways coexist, leading to a harmful cycle where resistant strains are both produced and spread within communities. A notable characteristic of M. tuberculosis is that acquiring resistance mutations usually does not significantly affect the organism's fitness. Unlike some other pathogens for which resistance diminishes the ability to transmit, many resistant strains of M. tuberculosis are still capable of replicating and spreading as efficiently as drug-susceptible strains. In certain situations, compensatory mutations can even enhance bacterial fitness, allowing resistant strains to endure and dominate in endemic populations. This trait highlights the urgent necessity for early detection, timely implementation of effective treatment regimens, and robust adherence support to avert both the development of acquired resistance and the further spread of primary resistance13. (Figure 2.)
Epidemiology
Global and Regional Prevalence Tuberculosis continues to be a significant global health challenge, with the rise of multidrug-resistant (MDR) and rifampicin-resistant (RR) strains greatly hindering control measures. The World Health Organization (WHO) estimates that in 2022, around 410,000 people were diagnosed with MDR/RR-TB, leading to roughly 160,000 deaths directly linked to these strains. The worldwide distribution of MDR/RR-TB is highly uneven, with India, China, and the Russian Federation collectively representing a considerable portion of the burden14. However, MDR/RR-TB cases have been identified in almost every country, highlighting the global aspect of this epidemic. The prevalence in different regions varies significantly based on the effectiveness of national TB programs, the quality of healthcare systems, the prevalence of HIV, and socioeconomic variables. In nations with vulnerable health systems or inadequate TB control initiatives, the rate of MDR/RR-TB among newly diagnosed patients can greatly surpass global averages15.
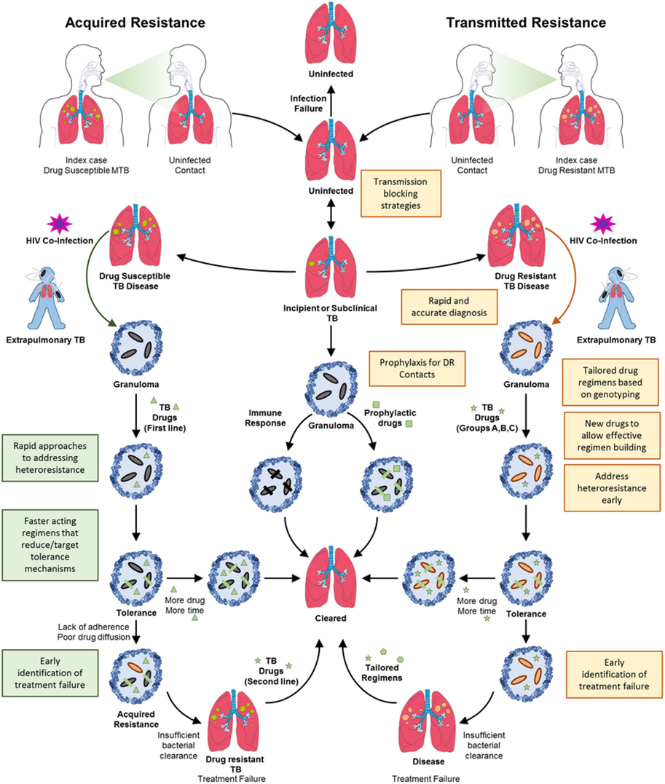
Figure 2. Transmitted (primary) and acquired drug-resistant tuberculosis pathways.
Risk Factors:
The emergence and transmission of MDR/RR-TB are affected by a complex interaction of biological, behavioural, and social factors. The strongest predictor for developing resistance is a previous history of TB treatment, especially in cases where the treatment regimens were insufficient, incomplete, or not consistently followed. HIV co-infection poses another significant risk, as it weakens the immune system, accelerating TB progression and complicating treatment. Additionally, other diseases such as diabetes and malnutrition heighten vulnerability, while lifestyle choices including smoking and alcohol consumption negatively impact treatment results. Environmental and structural factors such as being incarcerated, experiencing homelessness, exposure to air pollution, and occupational risks also contribute significantly to the transmission of TB. All these factors are rooted in socioeconomic disparities: poverty, overcrowded living conditions, stigma, and limited access to quality healthcare foster an environment where resistant TB strains can propagate without restraint16.
Trends in Resistance Development:
Fortunately, global data indicate some progress in mitigating the increase of MDR/RR-TB. Although the total number of cases remains substantial, the percentage of MDR/RR-TB among newly diagnosed TB patients has experienced a slight decrease from 4.0% in 2015 to 3.3% in 2022. This positive trend can be attributed to enhanced TB programs, improved diagnostic tools, and adherence to treatment regimens recommended by the WHO17. Nevertheless, the prevalence among patients with previous treatment is still significantly elevated, highlighting ongoing difficulties in preventing recurrences, reinfections, and treatment failures. A major concern is the rise of resistance to second-line therapies, which jeopardizes the efficacy of newer treatment regimens and could lead to extensively drug-resistant TB (XDR-TB). XDR-TB is characterized by resistance to isoniazid, rifampicin, fluoroquinolones, and at least one injectable second-line drug, representing a critical challenge due to limited treatment options, poorer outcomes, and increased mortality rates18.
Continued monitoring, the expansion of rapid molecular diagnostics, and fair access to innovative anti-TB medications are vital for addressing this issue. Without ongoing investment in both biomedical research and public health strategies, the global mission to eliminate TB by 2035, as specified in the WHO End TB Strategy, will face serious setbacks19.
Diagnosis of MDR/RR-TB:
The precise and prompt identification of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is essential for starting the right treatment, curbing further transmission, and enhancing patient outcomes. For many years, diagnosis depended mainly on culture methods and phenotypic drug susceptibility testing (DST), but these approaches tend to be slow and resource-demanding. The emergence of molecular diagnostics has revolutionized the field, allowing for quicker and more accurate identification of drug resistance, especially rifampicin resistance, which is broadly acknowledged as a reliable indicator of MDR-TB20.
Traditional Methods:
Traditional diagnostic techniques still heavily depend on culture-based methods, which serve as the standard for confirming tuberculosis (TB) and for drug susceptibility testing (DST). Solid media like Lowenstein–Jensen (LJ) and liquid culture systems such as the Mycobacteria Growth Indicator Tube (MGIT) are commonly utilized to support bacterial growth and subsequent DST. While these methods are highly effective, they are also labour-intensive, require considerable time (typically taking 4 to 8 weeks for growth, followed by additional weeks for susceptibility findings), and necessitate strict biosafety protocols and skilled laboratory personnel, which may be lacking in high-burden and resource-limited areas21. Nonetheless, culture and phenotypic DST remain crucial, particularly for verifying resistance to second-line medications and diagnosing resistance mechanisms that molecular techniques might miss. Additionally, standard smear microscopy with Ziehl–Neelsen staining or fluorescence methods is still used in peripheral labs due to its cost-effectiveness and ease of use, although its low sensitivity and inability to distinguish between drug-resistant strains considerably limit its clinical usefulness22.
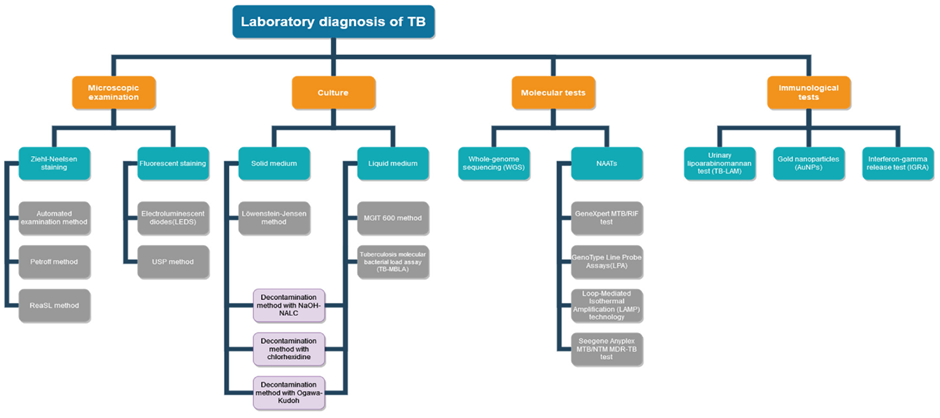
Figure 3. Flow diagram of the laboratory diagnosis process of tuberculosis, illustrating traditional culture-based and molecular methods (adapted from Evolution of Laboratory Diagnosis of Tuberculosis, MDPI, 2020).
Molecular diagnostic methods have transformed TB identification by facilitating the quick detection of multidrug-resistant and rifampicin-resistant TB (MDR/RR-TB). The Xpert MTB/RIF test, a cartridge-based real-time PCR assay, simultaneously identifies Mycobacterium tuberculosis complex DNA and mutations in the rpoB gene linked to rifampicin resistance, providing results within two hours directly from sputum specimens. Its advanced version, Xpert MTB/XDR, broadens the detection capabilities to include isoniazid, fluoroquinolones, and second-line injectable drugs, enhancing its clinical applicability23. Another pivotal molecular platform is the Line Probe Assay (LPA), like GenoType MTBDRplus and MTBDRsl, which accurately detects mutations associated with resistance to both first-line and second-line drugs with high sensitivity and specificity. Supported by the World Health Organization (WHO), LPAs are increasingly being used to inform personalized treatment approaches, although their dependence on laboratory infrastructure and trained personnel may hinder widespread implementation in remote locations24.
More sophisticated genomic technologies, particularly whole genome sequencing (WGS), offer a thorough understanding of resistance by identifying both established and novel mutations throughout the bacterial genome. WGS not only aids in tailoring individualized treatment plans but also supports epidemiological research, outbreak tracing, and monitoring transmission trends25. However, its considerable cost, technical intricacies, and the requirement for bioinformatics skills confine its use to reference laboratories in higher-resource environments. To tackle these obstacles, targeted next-generation sequencing (tNGS) has emerged as a cost-effective and clinically feasible option by concentrating on key resistance-associated genes while still producing actionable outcomes26.
In addition to traditional molecular approaches, various innovative methods are currently under development. CRISPR-based diagnostic tools such as SHERLOCK and DETECTR have shown exceptional sensitivity and portability in detecting TB DNA and resistance mutations, presenting potential as point-of-care solutions. Additionally, nanotechnology-based biosensors are being investigated for the rapid and low-cost identification of TB biomarkers in clinical samples. Moreover, artificial intelligence (AI) and machine learning techniques are increasingly utilized in the analysis of chest X-rays and CT scans, offering automated TB detection and triage assistance, particularly in areas where radiological expertise is scarce27. Some of these AI-enabled imaging tools have already received WHO approval for TB screening. Together, these emerging methods signify a substantial advancement toward more rapid, accessible, and accurate diagnosis of MDR/RR-TB, although their successful implementation in routine practice will necessitate thorough validation, reduced costs, and integration into current healthcare systems28.
Emerging Approaches:
New advancements such as next-generation sequencing (NGS)-based targeted tests, portable sequencing tools (e.g., Oxford Nanopore), and CRISPR-based diagnostics are being investigated to further increase the speed, accuracy, and accessibility of TB diagnosis. When combined with digital health technologies, these innovations have the potential to address diagnostic deficiencies in areas heavily burdened by TB and with limited resources29. Despite significant progress in diagnostic technologies, numerous challenges continue to hinder the timely and precise detection of MDR/RR-TB. A primary challenge is the restricted access to molecular testing in numerous high-burden nations due to financial constraints, underdeveloped laboratory systems, and insufficient healthcare infrastructure30. The lack of diagnostic tools, frequent equipment malfunctions, poor supply chain management, and a deficit of qualified laboratory personnel further obstruct the effective use of these technologies. Patients residing in rural and remote areas often encounter long travel distances to diagnostic facilities, resulting in delays in diagnosis and the commencement of treatment, which heightens the risk of ongoing transmission31.
Another major issue relates to the inconsistent sensitivity and specificity of molecular tests. Although assays like Xpert MTB/RIF effectively detect rifampicin resistance, they might not identify isoniazid resistance or resistance to newer medications such as bedaquiline and linezolid. This could lead to incomplete or inappropriate treatment plans, exacerbating the emergence of further resistance. Moreover, many rapid molecular tests are unable to detect rare or novel mutations that lie outside the commonly targeted gene regions, limiting their effectiveness in areas with varied resistance mechanisms. The emergence of patterns like pre-extensively drug-resistant TB (pre-XDR-TB) and extensively drug-resistant TB (XDR-TB) underscores the critical need for adaptable diagnostic platforms that can evolve with changing resistance profiles32.
Operational hurdles further complicate the situation. The high costs associated with cartridges, reagents, and sequencing platforms limit scalability in resource-constrained settings, while inconsistent electricity supply and lack of internet connectivity hamper the performance of devices like Xpert systems in decentralized locations. Furthermore, the integration of new diagnostic technologies into existing healthcare infrastructures is often sluggish, impeded by fragmented national policies, inadequate funding, and coordination gaps between public and private healthcare sectors. Socioeconomic and patient-centric factors significantly influence the situation as well33. Stigma, economic hardship, and a lack of awareness may dissuade individuals from seeking prompt testing, while weak referral systems and inefficient sample transport networks hinder timely case detection. In pediatric TB and extrapulmonary TB, diagnostic-related challenges are further magnified by difficulties in obtaining high-quality samples and the diminished sensitivity of standard tests in these situations. Lastly, the use of advanced methods such as whole genome sequencing (WGS) and targeted next-generation sequencing (tNGS) remains confined to high-resource settings due to their prohibitive expenses, infrastructural needs, and the requirement for specialized bioinformatics skills. Without significant investment in research, infrastructure, and international cooperation, the divide between diagnostic advancements and practical application in high-burden nations will endure, jeopardizing global TB control initiatives34.
Treatment and Management Strategies:
The management of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is complicated, resource-intensive, and significantly more challenging than that of drug-susceptible TB. It generally entails lengthy treatments with second-line anti-TB medications that tend to be less effective, more toxic, and significantly pricier. Acknowledging these struggles, the World Health Organization (WHO) has updated its guidelines numerous times in the last decade to include new data, integrate safer and more effective therapies, and streamline treatment regimens. The latest recommendations highlight the importance of using all-oral, shorter treatment plans wherever possible, to enhance adherence and lessen the strain on patients and healthcare systems. In contrast, the standard treatment for drug-susceptible TB continues to involve a four-drug regimen combining isoniazid, rifampicin, pyrazinamide, and ethambutol for six months. MDR-TB, characterized by resistance to at least isoniazid and rifampicin, requires second-line medications. These options include fluoroquinolones like levofloxacin and moxifloxacin, injectable agents such as amikacin, kanamycin, and capreomycin, along with newer oral drugs like bedaquiline, delamanid, and linezolid. The introduction of pretomanid combined with bedaquiline and linezolid (the BPaL regimen) has demonstrated encouraging results in clinical trials, achieving higher cure rates in a reduced timeframe of six to nine months. These newer medications have transformed MDR-TB treatment by decreasing the dependency on injectables, which were previously linked to serious side effects, including permanent hearing loss and kidney toxicity35.
Nonetheless, several obstacles persist. Second-line treatment regimens continue to pose significant toxicity risks, such as liver damage, bone marrow suppression, prolonged QT interval, and peripheral nerve damage. Extended treatment durations often lasting between 9 to 20 months create challenges for adherence, may lead to interruptions in therapy, and increase the risk of patients dropping out, all of which contribute to the development of further resistance36. Alarmingly, documented resistance to newer drugs such as bedaquiline and linezolid has surfaced, raising concerns about the long-term viability of current treatment approaches. The restricted availability of these medications in many high-burden, low-resource nations further complicates global efforts to control the disease37.
To address these challenges, research is increasingly aimed at developing innovative strategies. Host-directed therapies (HDTs), which involve adjunctive agents like metformin, statins, and vitamin D, are being investigated to boost immune responses and enhance outcomes. The repurposing of existing medications with established safety profiles also shows potential in expanding treatment options. Furthermore, cutting-edge drug delivery systems, including nanocarrier-based formulations, seek to improve drug absorption, reduce toxicity, and facilitate targeted delivery of medications to infected areas38.
WHO-Recommended Regimens:
The WHO currently recommends all-oral, shorter treatment regimens for suitable MDR/RR-TB patients to lessen toxicity and enhance adherence. The 6-month BPaLM regimen which includes bedaquiline, pretomanid, linezolid, and moxifloxacin—has shown encouraging effectiveness and safety, particularly in patients without fluoroquinolone resistance. For those ineligible for the BPaLM regimen, a 9-month all-oral regimen is an alternative option. This regimen typically contains bedaquiline, high-dose isoniazid, levofloxacin or moxifloxacin, clofazimine, ethambutol, pyrazinamide, and either linezolid or ethionamide, based on drug susceptibility patterns and patient tolerance. Individuals with extensive drug resistance or those who cannot tolerate shorter regimens may require longer, personalized treatment plans lasting 18 to 20 months. These plans are tailored based on detailed drug susceptibility testing (DST) and often incorporate newer medications like delamanid and pretomanid alongside traditional second-line drugs39.
Newer and Repurposed Drugs:
The advent of bedaquiline, the first new anti-TB medication in over forty years, has markedly enhanced treatment outcomes for MDR/RR-TB. Bedaquiline works by inhibiting the bacterial ATP synthase enzyme, thereby disrupting energy production in Mycobacterium tuberculosis. When used properly, it can shorten treatment duration and lower mortality rates. Delamanid, another recent drug, targets the synthesis of mycolic acid, which is vital for preserving the mycobacterial cell wall. It is particularly beneficial for patients who cannot tolerate injectable medications or have resistance to multiple drugs. Pretomanid, a nitroimidazole agent, operates in synergy with bedaquiline and linezolid, especially within the BPaL regimen. These medications provide a more effective and better-tolerated option for treating MDR/RR-TB, especially when used in innovative combinations. Linezolid, initially developed for treating gram-positive infections, has demonstrated significant anti-TB activity. However, its use is often constrained by dose-related side effects, including bone marrow suppression and peripheral neuropathy40.
Side Effects and Adherence Issues:
Adverse effects linked to second-line drugs present a major obstacle to achieving successful treatment outcomes. Frequent toxicities include liver damage (due to pyrazinamide and high-dose isoniazid), kidney damage and hearing loss (from injectable medications such as amikacin), as well as neurological damage (from linezolid and cycloserine). Addressing these side effects necessitates ongoing clinical and laboratory oversight. The engagement of skilled healthcare professionals, along with psychosocial support and nutritional assistance, plays a crucial role in encouraging patients to follow through with lengthy and challenging treatment plans. Approaches centred on patient care, such as directly observed therapy (DOT), community-based treatment aid, and mobile health technologies, are vital for enhancing adherence and ensuring completion of treatment41.
CHALLENGES IN CONTROLLING MDR/RR-TB:
Managing multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) poses one of the most intricate public health challenges of the 21st century. Despite advancements in diagnostics and therapies, MDR/RR-TB continues to disseminate, especially in areas with limited resources. The combination of biological intricacy, socioeconomic inequalities, issues within health systems, and global disruptions such as COVID-19 has made controlling MDR/RR-TB particularly challenging. A comprehensive understanding of the various obstacles to effective management is essential for enhancing patient outcomes and lowering transmission rates42.
Delayed and Inaccurate Diagnosis:
One of the primary difficulties in managing MDR/RR-TB is the delay in diagnosis or the complete inability to identify drug resistance, which contributes to ongoing transmission and deteriorating clinical results. In many high-burden nations, diagnostic services are mainly located in urban centres, making them less accessible to rural communities. Despite the significant time reduction in diagnosis brought about by Xpert MTB/RIF and line probe assays (LPA), their deployment is still limited due to high expenses, equipment needs, and the necessity for skilled technicians. Particularly, whole-genome sequencing (WGS), which can accurately identify resistance to both first- and second-line medications, remains largely restricted to research or reference labs due to its complexity and cost. Furthermore, traditional culture-based drug susceptibility testing (DST) requires several weeks to provide results, leading to further delays in starting effective treatment42.
High Cost and Toxicity of Second-Line Treatments:
Another major hurdle is the expense and toxicity associated with second-line treatment regimens. While first-line therapy for drug-susceptible TB is generally affordable and well-tolerated, MDR/RR-TB regimens are costly and call for extended administration, often lasting between 9 to 20 months depending on the resistance profile and availability of drugs. Medications such as linezolid, bedaquiline, clofazimine, and delamanid have led to improved outcomes, yet their side effects are significant and encompass hematologic toxicity, QT prolongation, liver damage, and neuropathy. Moreover, access to these newer treatments is uneven worldwide, and outdated regimens with injectable agents like kanamycin or amikacin are still utilized in many countries, despite their well-documented dangers, including permanent hearing loss42,43.
Patient Adherence and Treatment Completion:
The intricacy of treatment protocols and the duration of therapy pose significant challenges. Patients are frequently required to consume a multitude of pills daily for a span of 9 to 20 months, which can be both mentally and physically draining. Adverse reactions often lead patients to pause or discontinue their treatment, resulting in less-than-optimal outcomes and the rise of extensively drug-resistant TB (XDR-TB). Socioeconomic factors such as loss of income, expenses associated with travel to healthcare facilities, and a lack of family support further hinder adherence. Approaches like directly observed treatment (DOT), digital adherence technologies (DAT), psychosocial support, and nutritional assistance have demonstrated effectiveness in improving adherence, but their implementation is inconsistent due to limited funding44.
Social Stigma and Mental Health Burden:
Patients with MDR/RR-TB frequently contend with social stigma, which can result in delayed diagnoses, concealment of symptoms, and poor health-seeking behaviour. This stigma is heightened in communities where TB is linked to issues of poverty, HIV, and substance abuse, leading to isolation and discrimination. Numerous patients deal with anxiety, depression, and psychological distress during treatment caused by side effects, extended hospitalization, and the fear of transmitting the infection to family members. Mental health care has largely been overlooked in national TB programs, despite clear evidence connecting psychological support to improved treatment adherence and outcomes44.
Weak Health Systems and Infrastructure Gaps:
In many countries with high TB burdens, the healthcare system is inadequately prepared to effectively manage MDR/RR-TB. Problems include a lack of trained personnel, insufficient diagnostic facilities, drug shortages, and ineffective supply chain management. Surveillance systems are often inadequate for monitoring drug resistance trends or treatment outcomes, obstructing timely interventions. Furthermore, in numerous areas, TB services are not integrated with primary healthcare, leading to missed chances for early diagnosis and treatment initiation. International funding and technical support, such as that offered by the Global Fund and the Stop TB Partnership, are crucial for bolstering national TB control programs44.
Ineffective Contact Tracing and Community Involvement:
Contact tracing and proactive case identification are crucial for controlling TB, yet these measures remain underused in many endemic nations due to inadequate personnel, funding, and logistical resources. Community health workers often lack sufficient training and support, while cultural obstacles may hinder households from engaging with public health initiatives. Additionally, insufficient community awareness regarding MDR/RR-TB diminishes the success of education campaigns, resulting in ongoing transmission within high-risk populations45.
Lack of Coordination with HIV and Other Comorbidities:
HIV co-infection heightens the likelihood of developing active TB and complicates the treatment of MDR/RR-TB. Nonetheless, TB and HIV services continue to operate in isolation within numerous health systems, leading to lost chances for co-management and holistic care. Furthermore, other accompanying health issues such as diabetes and malnutrition are frequently overlooked in TB treatment, despite their recognized influence on treatment success and relapse rates46.
PROGRESS AND FUTURE PERSPECTIVES:
The fight against multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is now entering a new phase defined by scientific advancements, enhanced diagnostics, innovative therapies, and improved public health strategies. In spite of significant challenges, recent years have shown a transformation in global initiatives aimed at boosting the detection, treatment, and prevention of drug-resistant TB. These developments create encouraging paths to lessen disease burden, enhance patient outcomes, and advance toward the World Health Organization's (WHO) End TB Strategy objectives47.
Improvements in Diagnostic Technologies:
Swift and precise diagnosis is vital for the effective management and control of MDR/RR-TB. Recent innovations in diagnostics have revolutionized TB detection. The Xpert MTB/RIF test allows for the concurrent identification of TB and rifampicin resistance within two hours, significantly decreasing the time to diagnosis. Line probe assays (LPAs) further improve diagnostic precision by recognizing genetic mutations linked to both first- and second-line drug resistance. Moreover, whole-genome sequencing (WGS) is currently being utilized in reference labs to provide a thorough resistance profile, allowing for personalized treatment plans. However, its application is still constrained by costs and technical demands. Newer methods, such as Raman spectroscopy combined with machine learning techniques, are in development, offering rapid and non-invasive TB detection along with drug resistance markers, which may eventually be implemented in point-of-care environments48.
Creation of New Therapeutics and Shorter Treatment Regimens:
The treatment landscape for MDR/RR-TB has significantly advanced with the introduction of shorter and more effective treatment regimens. The WHO now endorses a 6-month all-oral BPaLM regimen (bedaquiline, pretomanid, linezolid, and moxifloxacin) for patients diagnosed with MDR/RR-TB who satisfy specific criteria. This regimen not only shortens the treatment time but also eliminates the need for potentially harmful injectable medications. Alternative regimens, like the 9-month modified shorter regimen that includes bedaquiline, levofloxacin or moxifloxacin, clofazimine, pyrazinamide, ethambutol, high-dose isoniazid, along with linezolid or ethionamide, offer options for individuals with limited drug resistance. These regimens have shown enhanced adherence and improved treatment outcomes due to decreased duration and pill burden. Additionally, bedaquiline (which targets ATP synthase) and delamanid (which inhibits mycolic acid synthesis) have emerged as fundamental elements of MDR/RR-TB treatment because of their strong sterilizing efficacy and favorable safety profiles when utilized properly. Pretomanid, a nitroimidazole, functions synergistically with other medications and is now included in the WHO-recommended treatment regimens. Ongoing clinical trials are continuously exploring combinations of new and existing medications to further lessen treatment duration, toxicity, and the emergence of resistance49.
Host-Directed Therapies (HDTs):
A promising area of research is the development of host-directed therapies (HDTs) aimed at modulating the immune response to improve treatment efficacy and reduce tissue damage. Unlike traditional antimicrobial therapies that target the bacterium directly, HDTs focus on enhancing the host’s innate and adaptive immunity, potentially accelerating bacterial clearance and minimizing side effects. Agents under investigation include non-steroidal anti-inflammatory drugs (NSAIDs), statins, and immunomodulators such as interleukin inhibitors. HDTs may also help in managing inflammatory lung damage caused by TB, which can persist even after microbiological cure, improving long-term pulmonary outcomes and quality of life50.
Advances in TB Vaccine Development:
Vaccines remain a crucial element in TB prevention. The BCG vaccine, though widely used, offers limited protection against pulmonary TB in adults. Recent advancements in vaccine research have led to the development of promising candidates such as M72/AS01E, which demonstrated about 50% efficacy in preventing active pulmonary TB in latently infected individuals during Phase IIb trials. Other vaccine strategies, including recombinant protein subunits, viral vectors, and live attenuated mycobacterial strains, are currently under various stages of clinical evaluation. If successful, these vaccines could significantly reduce the incidence of TB and curb the transmission of drug-resistant strains, especially in high-burden countries51.
Integration of Digital Health Tools and Artificial Intelligence (AI):
Digital innovations are transforming TB care delivery. Mobile health (mHealth) tools, such as smartphone-based applications and digital pillboxes, enable remote monitoring of treatment adherence and improve communication between patients and healthcare providers. AI-driven algorithms are increasingly used in radiographic interpretation, enabling rapid and accurate TB screening in settings where radiologists are unavailable52. In addition, electronic health records and data analytics platforms are being utilized to track patient progress, monitor drug resistance trends, and guide policy decisions. These technologies, when effectively implemented, can improve program efficiency, optimize resource allocation, and personalize care52.
Strengthened Global Policies and Initiatives:
Global initiatives continue to play a pivotal role in combating MDR/RR-TB. The WHO End TB Strategy aims to reduce TB incidence by 90% and deaths by 95% by 2035, focusing on early diagnosis, universal drug susceptibility testing, shorter and effective treatment regimens, and social protection for patients. Other global partnerships, such as the Stop TB Partnership, advocate for increased funding, innovation, and equitable access to diagnostics and treatments. The integration of TB services into universal health coverage (UHC) frameworks is also being prioritized, ensuring that all individuals, regardless of socioeconomic status, receive timely and quality TB care. International funding mechanisms like the Global Fund to Fight AIDS, Tuberculosis and Malaria remain instrumental in supporting programmatic expansion in low-income countries53.
CONCLUSION:
Multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) continues to pose a major challenge to global tuberculosis control, particularly in high-burden regions with limited resources. The rise of drug resistance, which is influenced by genetic mutations, bacterial persistence strategies, and factors related to treatment, highlights the intricacy of managing this illness. Innovations in rapid molecular diagnostics, such as Xpert MTB/RIF, Xpert MTB/XDR, and Line Probe Assays, have greatly reduced the time required for detection, while whole-genome sequencing and targeted next-generation sequencing offer detailed resistance profiling and epidemiological data. Treatment approaches have shifted from extended, toxic regimens to shorter, all-oral options that include new medications like bedaquiline, delamanid, pretomanid, and linezolid, leading to improved efficacy, patient compliance, and outcomes. Nevertheless, challenges remain, including drug toxicity, the emergence of resistance to new agents, limited access to diagnostics and treatment options, issues with patient adherence, and constraints within health systems. Future strategies should combine innovative therapeutics, host-directed therapies, and digital adherence technologies with enhanced surveillance measures, equal access to healthcare, and a strong public health framework. Global collaboration, commitment from political leaders, and active community involvement are critical to reducing stigma, enhancing treatment results, and preventing further spread of the disease. Ongoing investment in research, diagnostics, and healthcare infrastructure is vital for meeting the WHO End TB Strategy objectives and ultimately managing MDR/RR-TB on a global scale.
REFERENCES





Kartik Khairnar, Khushi Patodkar, Harshal Patodkar, Khan Heba, Shraddha Kamankar, Innovative Approaches to The Diagnosis and Management of Multidrug-Resistant and Rifampicin-Resistant Tuberculosis: Current Challenges and Future Perspectives, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 102-120. https://doi.org/10.5281/zenodo.17241573
 10.5281/zenodo.17241573
10.5281/zenodo.17241573
