S.N.D College of Pharmacy, Babhulgaon, Yeola.
Many plants, including red grapes, peanuts, and berry fruits, naturally contain the well-known polyphenolic compound resveratrol, which belongs to the stilbene family. Polygonum cuspidatum, a herbal medicinal plant known for its antioxidant, anti-ageing, anti-inflammatory, anti-diabetic, and neuroprotective qualities, is a common source of this compound. This study examines the physical and chemical properties of resveratrol utilising a nanostructured lipid carrier system, which is a colloidal drug delivery system composed of solid and liquid lipids. Because resveratol is unstable in light and only slightly soluble in water, proper formulations are necessary for better clinical efficacy. Thus, the goal of this study was to develop a lipid-based nanostructured gel containing resveratol for topical delivery. Because of its promise of longer medication availability in skin tissue, the NLC gel could be employed to improve the treatment of inflammatory diseases. This article educated readers on the potential of a promising natural substance as one of the best therapeutic medications and neutraceuticals in the medical industry.
Natural active ingredients, such as resveratrol, are chemicals derived from plants, microbes, or animals that have been studied for their pharmacological and therapeutic effects, including antibacterial, anti-inflammatory, and antioxidant capabilities. Because of their potential as efficient therapies for illnesses with fewer side effects and cost-effectiveness when delivered properly, these substances have become more important in modern medicine than the bulk of pharmaceutical medications. Natural active ingredients have been increasingly popular in skincare products in recent years. This widespread application is attributed to the skin's therapeutic benefits, which include antibacterial, anti-inflammatory, and wound-healing properties. These ingredients are commonly used to treat specific skin concerns or disorders, such as inflammation, dryness, ageing, and acne. Despite their numerous benefits, natural chemicals in topical dosage forms remain difficult to deliver through the skin without losing effectiveness. Poor skin permeability, which prevents penetration into the stratum corneum and outermost layer, is a significant barrier. Because of this phenomenon, natural substances are unable to reach the deeper layers and achieve maximal efficiency. Natural compounds may also decay and lose efficacy when exposed to light, heat, and air. Natural components might be challenging to incorporate into skin care products due to variances in skin permeability, solubility, and other physical properties. Natural substances may nevertheless cause skin irritation or allergic reactions in certain people, which raises safety concerns when compared to synthetic products. It has been proposed that lipid-based drug delivery systems (LBDDS) that mimic the function of the skin barrier can improve the performance and distribution of natural active ingredients. LBDDS has been shown to improve skin permeability and protect natural components from degradation, hence increasing stability and bioavailability while reducing toxicity. Nanostructured lipid carriers are the most popular. Physically, LBDDS is typically liquid; however, when high-melting lipids are used or adsorbed onto the carrier, it can be solid or semi-solid at room temperature. Lipid particulates may also be present.
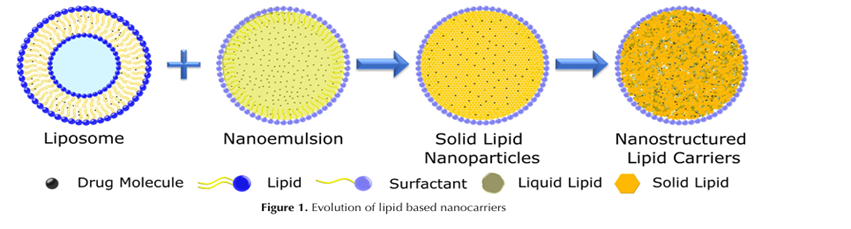
The figure below depicts the morphological models of several LBDDS, including nanostructured lipid carriers. Nanostructured lipid carriers (NLCs) are drug delivery devices that have a core matrix composed of both liquid and solid lipids.
Furthermore, NLCs are second-generation lipid nanoparticles with excellent drug loading capacity and an unstructured matrix, making them suitable for drug delivery systems. Because of their unique properties, NLCs have been extensively studied as alternate carriers for the cutaneous delivery of pharmaceuticals, particularly natural active compounds. Biocompatible chemicals, drug release modification, skin adhesion, film-forming ability with hydration of the superficial skin layers, and increased penetration and permeation into deeper skin layers are among the associated benefits identified. NLCs, or nanostructured lipid carriers, represent a novel type of drug delivery vehicle. NLC offers several advantages, including biocompatibility, biodegradability, non-immunogenicity, high drug loading capacity, increased stability, controlled drug release, and ease of manufacture with scalability. These carriers are ideal for drug delivery due to their advantages. Nanogels are attractive delivery methods for transdermal medication delivery. Transdermal drug delivery devices have several advantages, including improving patient compliance, lowering dosing frequency, eliminating first-pass metabolism, and easily stopping drug action following device removal. Transdermal administration helps to build up adequate drug concentrations in the target location. The critical characteristics for producing successful TDDS are high drug loading, biocompatibility, and biodegradability, all of which are present in nanostructured gels. Nanogels are attractive delivery methods for transdermal medication delivery. Transdermal drug delivery devices have several advantages, including improving patient compliance, lowering dosing frequency, eliminating first-pass metabolism, and easily stopping drug action following device removal. Transdermal administration helps to build up adequate drug concentrations in the target location. The critical characteristics for producing successful TDDS are high drug loading, biocompatibility, and biodegradability, all of which are present in nanostructured gels. Topical treatment is a significant usage in dermatological medicine. The physical chemistry of the skin and the patient's application method dictate how a topical drug is given. The type of carrier influences the topical's efficacy. Nanogels may improve the success rate of treating people with skin diseases.
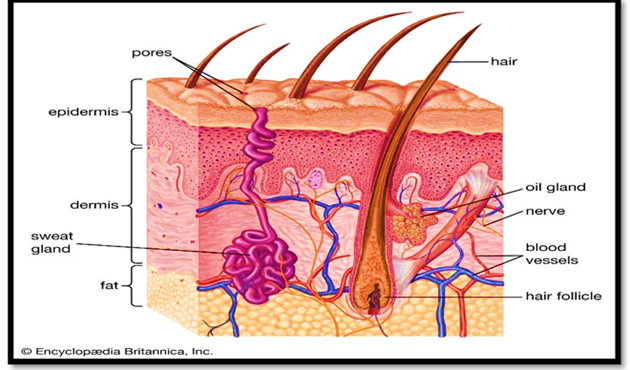
Skin:
Topical medication delivery systems are applied to specific parts of the body's surface. To treat localised skin problems, they provide drugs locally rather than systemically. Topical administration has a number of advantages over other techniques of administration. When topical therapy is applied to the affected area, the primary benefit is that there are seldom systemic side effects [1]. Topical administration prevents first-pass metabolism by spreading the active ingredient through the skin.
It bypasses the active ingredient's metabolism before reaching the point of action. Topical medicines can improve patient compliance since they are easy to use and suitable for self-administration. Topical therapy avoids the risks and complications associated with intravenous administration by eliminating the need for complex delivery techniques. Furthermore, the skin contains the majority of the human body's surface area. It has a fairly broad variety of applications and can deliver more medication to specific locations with greater precision. It has the potential to reduce dose frequency by maintaining a high local drug concentration in the surrounding tissues over time. Because the medicine does not reach the bloodstream, topical treatment reduces the risk of systemic side effects. However, there are some downsides. These consist of:
Several semi-solid topical dosage formulations with antibacterial and anti-inflammatory characteristics were developed as part of this study.
The three most important pathways of skin absorption are those for medication penetration via the skin. [3, 4]
This is a breakthrough in pharmaceutics or cosmeceuticals using a nanostructured lipid carrier system loaded gel. The formation of gel.
Gels are semi-solid structures composed of a liquid phase trapped within a three-dimensional matrix of polymers. They are widely used for topical drug administration due to their excellent patient compliance, ease of application, and ability to deliver both hydrophilic and lipophilic medications. "Gelatin" is the source of the word "gel," and "gel" and "jelly" share a shared origin. Gelu means "drop" in Latin, whereas gel denotes "freeze" or "freeze." This source demonstrates the essential concept that liquids are solids that retain liquid properties and are elastic but do not flow. In the late 1800s, scientists attempted to differentiate semisolids based on their phenomenological features rather than their chemical composition, and the name "gel" was first used to describe these materials. There are currently no analytical methods available for identifying drug compounds. Gels are tougher than jellies because they have more cross connections, are denser, or are just less liquid. Gel-forming polymers create materials of varied hardnesses, including sols, slimes, jellies, gels, and hydrogels.
GEL DEVELOPMENT OBJECTIVES-
COMPONENT OF GEL-
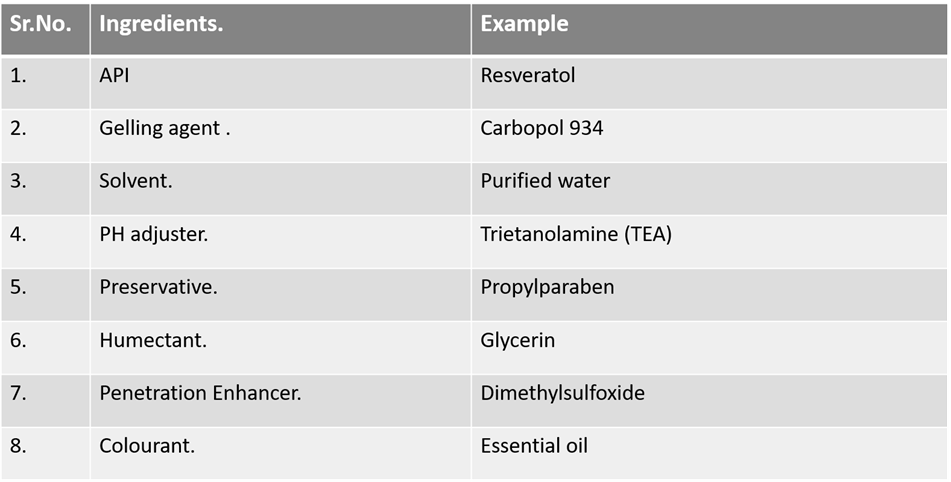
1. Gelling agent: The primary component of a gel is a gelling agent, which is a substance that imparts a gel-like texture, functioning to thicken or stabilise mixtures. An example of this is CARBOPOL.
2. Solvent: A solvent is a substance that dissolves a solute to form a solution; it is typically a liquid. It serves as the medium in which other components are dispersed or dissolved. An example is purified water.
3. Active Pharmaceutical Ingredient (API): An API is the physiologically active component of a pharmaceutical drug that produces the intended effects in the body. It is the substance that provides the medication's therapeutic action. For example, RESVERATOL.
4. Penetration enhancers: A penetration enhancer is a chemical that promotes the absorption of active substances through the skin or other biological barriers. Specifically, DIMETHYL SULPHOXIDE
5. Preservatives: By inhibiting the growth of microorganisms such as moulds, fungi, and bacteria, preservatives extend shelf life and prevent spoilage. Examples include PROPYL PARABEN and METHYL PARABEN.
6. pH Adjusters: Using a pH adjuster, you can vary and stabilise the acidity or alkalinity (pH) of your product. It is required in formulations where stability, safety, and efficacy rely on maintaining a specific pH range. For example, TRIETANOLAMINE.
APPLICATION-
RESVERATROL is the natural active ingredient.
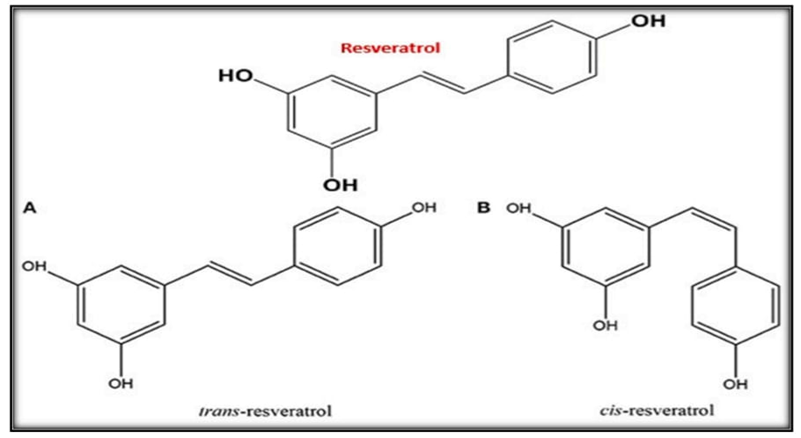
The phytoalexin resveratol (3,5,4'-trihydroxystilbene) is a polyphenol. (For example, a chemical that plant tissues produce when they come into contact with a parasite and specifically inhibits the parasite's growth.) Plants use the enzyme stilbene synthase to produce this stilbenoid, a stilbene derivative. Resveratrol is a fat-soluble compound that exists in both cis and trans molecular structures. offering a range of effects, including immunomodulation, neuroprotection, anti-inflammatory, anti-ageing, and anti-cancer.
Resveratrol offers numerous health benefits, such as increasing NO synthesis, reducing oxidative stress, and alleviating inflammation. Resveratrol has been shown in early studies to reduce lipid peroxidation [6] and decrease the oxidation of human low-density lipoprotein (LDL) [5]. Furthermore, resveratrol reduces oxidative stress by boosting the expression of numerous antioxidant enzymes and blocking ROS production by NADPH oxidase [7]. Resveratrol's anti-inflammatory characteristics include suppression of the pro-inflammatory enzyme cyclooxygenase-1 (COX-1), which reduces the generation of proinflammatory eicosanoids [8,9]. SIRT1 can exert anti-inflammatory effects by deacetylating nuclear factor-B, the key inflammatory transcription factor [10]. Additionally, Resveratrol has anti-ageing properties. Resveratrol has the capacity to regulate oxidative stress by boosting the activity of nuclear factor erythroid-2 related factor 2 (Nrf2) and antioxidant enzymes, including catalase (CAT) and superoxide dismutase (SOD), which reduce the production of reactive oxygen species (ROS). Resveratrol may downregulate the Akt/mTOR pathway and activate the antiaging factor sirtuin1 (Sirt1) in mitochondria, reducing ROS and improving mitochondrial biogenesis and function. Resveratrol may boost NF-κB and Sirt1 activity, leading to lower levels of inflammatory markers such as IL-1β, TNF-α, and MCP-1. Resveratrol may affect the levels of apoptotic proteins Bim and Bax, as well as the antiapoptotic protein Bcl, which may regulate apoptosis. It may also activate Sirt1, promote head box protein O1 (Foxo1), and suppress p53. Resveratrol has a considerable antioxidant activity in its neuroprotective effect by scavenging free radicals and metals, protecting against NO toxicity, lowering QR2 activity, and upregulating endogenous enzymes such as glutathione peroxidase, HO-1, AMPK, and LKB1. Numerous malignancies, including those of the mouth, thyroid, breast, lung, liver, pancreas, stomach, colon, bladder, prostate, and ovaries, can be avoided or treated with resveratrol. The fundamental processes, which include preventing cell division, preventing metastasis, inducing apoptosis, promoting autophagy, adjusting the immune system, reducing inflammation, controlling gut microbiota, and amplifying the effects of other anticancer medications, have been extensively studied. Resveratrol's vasculoprotective actions include increased production of vasculoprotective nitric oxide (NO). Human umbilical vein endothelial cells (HUVECs) and EAhy 926 cells derived from HUVECs both exhibited this effect. The effectiveness of antioxidants. Oxidative stress is defined as an imbalance between the creation of reactive oxygen species and antioxidant defence, which favours oxidant synthesis. Many age-related ailments, including cancer, diabetes, chronic renal disease, cardiovascular disease, and neurological diseases, are caused by increasing oxidative stress, which degrades macromolecules and impairs their function. Furthermore, excessive ROS creation leads to cell death, inflammation, and mitochondrial malfunction. Furthermore, it has been proven that glucose auto-oxidation might contribute to ROS overproduction and an increase in oxidative stress levels. Resveratrol's structure has three hydroxyl groups, which contribute to its powerful antioxidant effects. Resveratrol prevents lipid peroxidation, aberrant mitochondrial distribution, and excess ROS production. Resveratrol administration of primary epidermal keratinocytes results in a quantitative decrease in cellular redox environment and endogenous ROS production, as well as a 1.3-fold increase in endogenously generated glutathione. Resveratrol can maintain cellular redox balance in astroglial cells treated with ammonia by inhibiting both an increase in ROS production and a decrease in mitochondrial membrane potential. Resveratrol protects fibroblasts exposed to rotenone from the Anti-inflammatory qualities. Resveratrol suppresses IL-6 transcription and translation, so macrophages produce less of it. Adding resveratrol to monocyte cells reduces inflammatory mediators like TNF-α and IL-8 without producing cytotoxicity. Resveratrol significantly inhibits pancreatic stellate cells' ability to create extracellular matrix proteins, which are linked to the development of pancreatic fibrosis. Resveratrol also helps to suppress toll-like receptors, which can activate innate and adaptive immunity and release proinflammatory cytokines and chemokines. Resveratrol reduces IL-1, IL-6, and TNF-α production as well as matrix-metalloprotease expression in osteoarthritic chondrocytes in a dose-dependent manner. harmful effects of ROS by preventing the attenuation of oxidative phosphorylation, minimizing mitochondrial fragmentation, and maintaining the potential of the mitochondrial membrane. Resveratrol therapy following oral implant surgery reduces serum levels of TNF-α, IL-1β, and IL-17A, while increasing levels of IL-2, IL-6, and IL-10. Ma and colleagues discovered that resveratrol effectively suppresses NF-κB signalling by limiting the actions of NF-κB and IκB kinase, as well as the activation of JAK/STAT signalling pathways. Resveratrol protects against intestinal ischemia-reperfusion injury by inhibiting mast cell degranulation and lowering intestinal epithelial cell apoptosis, hence avoiding total organ failure. Resveratrol's anti-inflammatory activities are also observed in immune-mediated diseases and acute small intestinal inflammation. It also prevents the fast accumulation of cholesterol and the disruption of macrophage lipid homeostasis in response to glycation products.
Neuro-protection: Furthermore, resveratrol improves central nervous system performance while decreasing neuronal damage and apoptosis. Resveratrol has been shown to enhance memory recovery after fluoride exposure and reduce neurodegeneration in the mouse cerebral cortex. Additionally, resveratrol therapy improves memory, learning, and cognition in rats suffering from vascular dementia. According to Corpas and colleagues, resveratrol improves cognition in mice models of Alzheimer's disease and boosts neuroprotection in amyloid and tau disorders. However, human resveratrol treatment produces varied responses. A meta-analysis of randomized controlled studies suggests that resveratrol may be beneficial or have no meaningful effect on the chosen measures of cognitive performance. Resveratrol has been shown in studies to have neuroprotective properties against intracerebral hemorrhage, cerebral neurodamage, and central nervous system traumas such as stroke. Resveratrol also has neuroprotective effects in rat brains injured by cerebral ischemia/reperfusion by reducing the volume of cerebral infarction and increasing the expression of intracellular signalling pathway components such as kinases like JAK2, PI3K, or Akt, as well as anti-apoptotic molecules, while suppressing the expression of pro-apoptotic caspase-3 and Bax.
Anti-cancer properties: Resveratrol may have anti-cancer properties due to its various actions, including antioxidant effects and inhibiting the production of pro-apoptotic proteins and molecules that contribute to tumour growth, according to multiple in vitro and in vivo studies. Resveratrol is well known to reduce the chance of developing several cancers, including thyroid, breast, colorectal, gastric, pancreatic, and cervical cancer. According to study, resveratrol preserves healthy cells while eliminating malignant cells. This can be connected to different cellular targets and resveratrol metabolic pathways in both malignant and healthy cells. This can be connected to different cellular targets and resveratrol metabolic pathways in both malignant and healthy cells. Furthermore, dosage influences the dual pattern of resveratrol action. While higher amounts induce cell necrosis or apoptosis regardless of whether the cell is healthy or sick, lower levels stimulate the creation of cell survival proteins. High dosages of resveratrol damage cellular structure, impede protein and nucleic acid synthesis, and eventually cause cell death. Monteillier and colleagues found that when mice with developed lung cancer were given 60 mg/kg resveratrol intranasally, tumour multiplicity and volume decreased significantly due to enhanced apoptosis. Furthermore, when compared to untreated controls, resveratrol treatment of gastric cancer cells enhanced pro-apoptotic proteins like Bax while reduced anti-apoptotic proteins like Bcl-2. Resveratrol treatment at 20 μM inhibits STAT3 signalling and cytokine production in osteosarcoma cells, reducing cell viability, self-renewal, and tumorigenesis. Resveratrol's anticancer activities are mostly dependent on reducing the production of carcinogenesis-related proteins, such as phospholipid scramblase 1, activating the mitochondrial ROS signalling pathway, and triggering caspase 3 cleavage. Resveratrol also suppresses the cell cycle by inducing S-phase arrest in gastric cancer cells in a dose-dependent manner. Resveratrol has also been demonstrated to diminish drug resistance in cancer cells and improve the efficacy of anticancer treatments. In vitro and in vivo study support resveratrol's favourable anticancer effect.
Activities to avoid aging: Antiaging research must focus on longevity, which is also an important measure of antiaging efficacy. A growing corpus of studies suggests that resveratrol may help people live longer lives. Autophagy's antiaging and life-extending effects may be linked to its ability to promote the clearance of dysfunctional proteins and damaged cellular organelles including mitochondria and endoplasmic reticulum. A study found that resveratrol may induce autophagy in human cells in vitro and Caenorhabditis elegans in vivo. It also increased the lifespan of Caenorhabditis elegans, whereas sirtuin (Sirt)1 knockdown or deletion prevented this effect. According to the findings, resveratrol promoted longevity via triggering autophagy in a Sirt1-dependent manner.
RES has anti-atherosclerotic properties: Atherosclerosis predominantly affects the intimal layer of the arterial artery wall. Its distinguishing features include extracellular lipid deposition, local smooth muscle cell migration and proliferation, and chronic inflammation. Clinical events such as coronary artery disease, peripheral arterial disease, and stroke are triggered by luminal constriction and/or thrombus formation [11]. Improving the lipid profile may be important because lipids, particularly low density lipoproteins (LDLs), are involved in the atherosclerotic process. According to certain preclinical studies, RES may modify this profile, specifically by increasing HDL cholesterol while decreasing plasma triglyceride and LDL cholesterol levels [12]. According to Cho et al. [13], RES may increase the hypocholesterolemic impact of pravastatin by inhibiting 3-hydroxy-3-methyl-glutaryl-CoA reductase (HMG-CoA reductase), an enzyme that interferes with the early stages of cholesterol synthesis. Furthermore, RES may increase the expression of LDL receptors (LDL-R) in hepatocytes in vitro [14], lowering blood LDL cholesterol levels even further. Furthermore, RES's antioxidant properties resulted in a boost in numerous endogenous antioxidant systems [16], a reduction in LDL oxidation (a process directly linked to atherogenesis [15], and anti-inflammatory effects [17]. The reduction of smooth muscle cell migration influences RES' antiatherogenic actions [18].
These qualities all show how RES influences important aspects in the atherosclerotic process. As a result, several potential targets for the beneficial effects of RES in CVDs have been discovered. In particular, RES inhibits TNF production while activating SIRT-1 (a class III histone deacetylase), eNOS, Nrf2, and the antioxidant response element (ARE). Thus, the global effect of RES reduces endothelial apoptosis, activation, and vascular inflammation while increasing endothelial function [19]. RES has been proven to work in the early phases of the atherogenic process. In example, by preventing the activation of the NF-B pathway, RES has been found to lower the expression of adhesion molecules (vascular cell adhesion molecule-1, or VCAM-1, and intercellular adhesion molecule-1, ICAM-1) [20] RES may limit the formation of foam cells by inhibiting the expression of NADPH oxidase 1 and the creation of monocyte chemotactic protein-1 (MCP-1) in macrophages exposed to LPS [21]. RES may affect inflammation by modulating the expression of miRNAs with pro-inflammatory (miR-155) or anti-inflammatory (miR-663) effects [22]. In terms of anti-inflammatory properties, RES has also been shown to activate Nrf2 and inhibit the production of proinflammatory cytokines in cardiomyocytes, which helps to mitigate endotoxin-induced myocardial damage in mice and may be a means of preventing sepsis-induced cardiomyopathy [23].
Another effect of RES is the inhibition of vascular smooth muscle cell migration and proliferation, which may contribute to its anti-atherogenic characteristics [18,24]. However, a meta-analysis of seven clinical trials [25] discovered that the research either had no effect on the lipid profile or produced positive outcomes. For example, patients with type 2 diabetes who received 250-1000 mg RES/day observed a reduction in LDL cholesterol [26]. Similarly, RES therapy lowered plasma triglyceride levels in healthy adult smokers (500 mg/day) [28] and healthy obese men (150 mg/day) [27]. RES (350 mg/day of RES-enriched grape extract containing 8 mg RES) reduced oxidized LDL by 20% and LDL cholesterol by 4.5% in those at high CV risk who were taking statins for primary prevention [29]. However, the anti-atherosclerotic effect of RES must be proved in large clinical trials and should not be limited to an effect on serum lipid profile. RES' antihypertensive effects Hypertension is a major risk factor for cardiovascular diseases [30]. RES has been proven to have antihypertensive effects in several animal models of hypertension after being given 10-320 mg/kg body weight/day for 14-10 weeks, depending on the study [31]. Notably, in animal models of hypertension and insulin resistance, relatively low dosages of RES (5-10 mg/kg/day) significantly decreased blood pressure [32], suggesting that RES may function better in people with diabetes or metabolic syndrome. RES was administered before hypertension occurred in a few studies.
Resveratrol's topical administration is limited due to its low solubility, instability, and low skin permeability. The resveratrol nanostructured lipid carrier system loaded gel is designed to overcome this. Small and large molecules are dispersed in aqueous liquid carriers to form a semi-solid preparation known as gel. Gels are semi-solid systems in which colloidal particles in a liquid media form physical or covalent bonds.
TECHNIQUES FOR NLC PREPRATION-
The literature describes a variety of approaches for constructing NLCs. These consist of: -
1) HIGH PRESSURE HOMOGENISATION - Definition of high pressure homogenization. A lipid mixture is forced through a small aperture at extremely high pressure (typically 100-1500 bar) in a mechanical process known as high-pressure homogenization (HPH), resulting in nanostructured lipid carriers (NLCs). Extreme shear and cavitation convert lipid droplets into nanoscale particles, resulting in a stable and constant dispersion.
The two basic HPH approaches for NLC creation are as follows:
1. Hot High Pressure Homogenization:
The medication dissolves or disperses in the lipid phase, causing lipids to melt above their melting point.
A hot aqueous surfactant solution is used to emulsify the lipid phase, the pre-emulsion is homogenized under high pressure, and the completed product is chilled to form solid lipid nanoparticles.
2. Cold, high-pressure homogenization: -
Benefits:
1. High-Pressure Homogenization (HPH) reduces lipid droplets to nanoscale particles through mechanical stress, often between 400 and 1500 bar. This plays a role in NLC formation.
2. Increased Encapsulation Efficiency (EE): Because smaller particles have a larger surface area, they interact more efficiently with lipids and active substances.
3. HPH-produced NLCs are thermally and storage stable, preventing the breakdown of delicate chemicals such as carotenoids and surfactants.
4. Formulation Versatility: HPH is compatible with a variety of lipid combinations (such as Precirol ATO 5 and olive oil) and surfactants (such as Tween 80), allowing it to be prepared for oral, topical, and intranasal delivery.
5. Ability to scale
2. MICROEMULSION-
Definition
A microemulsion is a clear or translucent, isotropic, thermodynamically stable mixture of water, oil, surfactant, and frequently a co-surfactant. Droplets are ideal for pharmaceutical delivery and solubilization since their sizes typically range between 10 and 100 nm.
NLC formulation using microemulsion: This requires producing NLCs with a microemulsion as a precursor or template. To make NLCs, a microemulsion is often generated first, followed by processes like as high-pressure homogenization or ultrasonication.
Working Mechanism: Microemulsion formation. A microemulsion is formed by combining the water phase, surfactants, co-surfactants, and oil phase (lipids).
Surfactants make it possible to create nanoparticles by decreasing interfacial tension.
Conversion into NLC: - Cooling or treating the microemulsion hardens the lipid phase, resulting in nanostructured lipid carriers.
As a result, solid-liquid lipid nanoparticles are disseminated evenly.
Drug Encapsulation:
Benefits include:
3. PROBE SONICATION -
"Probe sonication" is the method of agitating and disturbing particles in a liquid medium using high-frequency ultrasonic waves, typically above 20 kHz, provided by a metal probe known as a sonotrode. Cell lysis, DNA shearing, and nanoparticle dispersion are all processes that use it extensively in biological, chemical, and medicinal applications.
The primary mechanism is cavitation, which involves the formation and dissolution of tiny bubbles in liquids caused by ultrasonic vibrations.
Important controllable parameters include amplitude, which determines the strength of ultrasonic energy.
4. SOLVENT DIFFUSION-
Definition and Technique: This low-energy emulsification approach generates NLCs by allowing a water-miscible organic solvent containing lipids to seep into an aqueous phase, resulting in the formation of spontaneous nanoparticles. Encapsulating lipophilic drugs in lipid-based nanocarriers is highly beneficial.
Working Principle:
The process consists of two phases: controlled diffusion and mixing.
1. Preparing for the Organic Phase
2. Aqueous Phase Preparation:
3. Diffusion and Nanoparticle Formation:
4. Solvent Removal:
Crucial Elements
5. SOLVENT EMULSIFICATION
Evaporation is a popular method for producing nanostructured lipid carriers (NLCs), especially when working with lipophilic pharmaceuticals and thermosensitive compounds. It creates stable lipid nanoparticles by combining solvent removal and emulsification.
Definition: Emulsification and Evaporation Method for Solvents
This method involves dissolving lipids and drugs in a water-immiscible organic solvent to form an oil-in-water (O/W) emulsion with an aqueous surfactant solution. The solvent is then evaporated, precipitating and producing NLCs.
Working Principle: The procedure involves three main steps:
Important characteristics:
6. SOLVENT INJECTION/ DISPLACEMENT-
Solvent injection (also known as solvent displacement) is a simple and effective approach for producing nanostructured lipid carriers (NLCs), making it ideal for lipophilic drug delivery. It is based on a solvent's spontaneous diffusion into water, which results in nanoparticles.
Definition: Techniques for Solvent Injection and Displacement.
Using this approach, an organic solvent containing lipids is introduced into an aqueous phase and agitated. Lipids precipitate and self-assemble into NLCs, which are stabilised by surfactants due to the solvent's rapid diffusion into water.
Lipid precipitation and solvent diffusion drive the process.
The key benefits include:
Critical Parameters:
7. PHASE INVERSION
It is a low-energy emulsification process that produces nanostructured lipid carriers (NLCs). It operates by adjusting the content or temperature of the emulsion to vary its kind. It is especially useful for producing stable nanoparticles with minimal mechanical effort.
Definition: Method of Phase Inversion
Phase inversion is the process by which an emulsion transitions from oil-in-water (O/W) to water-in-oil (W/O) or vice versa due to changes in composition (for example, surfactant concentrations) or temperature. This inversion results in the spontaneous formation of fine lipid nanoparticles.
Working Principle:
Phase inversion takes two major forms:
1. The PIT Method, also called temperature-induced phase inversion:
2. Phase Inversion. Induced by composition:
One of the primary advantages is that there is no need for sonication or high shear. Suitable for drugs that are sensitive to heat. Creates stable and consistent nanoparticles.
Critical Parameters:
CREATING GEL USING SUBSTITUTES-
A gel formulation's safety, effectiveness, and quality are assessed using a number of physicochemical, mechanical, and biological factors. Common evaluation criteria for gel formulations are listed below:
1. Physical characteristics:
2. Measurement of PH making use of an electronic pH meter:
Assures skin or application site compatibility (for topical use, 5.5–7.0 is optimum).
3. Viscosity:
Determined with a Brookfield viscometer. Establishes residence time and spreadability
4. The ability to spread:
Evaluates how easily the gel spreads over the skin.
measured using the glass slide technique.
{Spreadability} = \frac{M \times L}{T} is the formula.
5. Extrudability:
This determines the ease with which the gel exits the tube. The amount of gel extruded is measured along with the applied pressure.
6. Drug Content Uniformity:
Assessed by dissolving the gel in a solvent and using an HPLC or UV spectrophotometer to measure absorbance ensures the medicine is distributed evenly.
7. Drug Release in Vitro:
Using a Franz diffusion cell with cellophane or a dialysis membrane mimics the gradual release of a medication into a medium
8. In-vitro Permeation Study: This method uses Franz diffusion cells as well, but it uses animal or human cadaver skin to examine how drugs penetrate the layers of the skin.
9. Research on Stability:
As required by ICH criteria, observations were made in real time and at a high speed. Examine for microbial growth, viscosity, pH shift, or phase separation.
10. Microbial Research (if required):
11. Skin Irritation or Compatibility Test:
Administered to participants or animal models guarantees the absence of irritation, itching, or erythema.
CONCLUSION
The formulation and evaluation of the resveratrol-loaded nanostructured lipid carrier (NLC) gel demonstrated that incorporating resveratrol into an NLC system effectively enhances its stability, solubility, and skin permeation compared to conventional formulations. The optimized NLC formulation exhibited appropriate particle size, high entrapment efficiency, and sustained drug release characteristics. The prepared gel showed good spreadability, homogeneity, pH compatibility, and viscosity, making it suitable for topical application. Overall, the study concludes that the resveratrol NLC-loaded gel is a promising delivery system for improving the bioavailability and therapeutic efficacy of resveratrol in topical or dermal applications.
FUTURE DEVELOPMENT-
Further work on resveratrol nanostructured lipid carrier (NLC) gel should focus on optimising formulation for maximum stability and skin penetration, performing long-term stability and in vivo studies to confirm safety and efficacy. Scale-up, quality control, and regulatory evaluation are needed for clinical use or commercialisation. Advanced studies may explore targeted delivery, combination therapy, and improved patient acceptability.
In the future, the development of resveratrol NLC-loaded gel should focus on making the formulation more stable and effective for long-term use. The ingredients and their ratios can be improved to increase the gel’s ability to protect resveratrol from degradation and help it absorb better into the skin. More studies are needed to test how well the gel works and how safe it is through animal and human trials.
Further work should include large-scale production methods to ensure that the gel can be manufactured easily and consistently without losing its quality. Stability studies under different conditions should be done to determine its shelf life. The packaging can also be improved to protect the product from light and temperature changes.
In the long term, research can explore advanced delivery methods such as targeted or smart-release systems that release the drug only when needed. Combining resveratrol with other beneficial ingredients like vitamins or antioxidants can also be studied for better results. Overall, continuous research and development will help make the resveratrol NLC gel a safe, effective, and market-ready skincare or therapeutic product.
REFERENCE


Mayur Bhad, Vikas Shinde, Shubham Adhav, Pankaj Mahajan, Formulation, Development and Evaluation of Resveratol Nanostructured Lipid Carrier System Loaded Gel, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2906-2924. https://doi.org/10.5281/zenodo.17649649
 10.5281/zenodo.17649649
10.5281/zenodo.17649649
