Babu Banarasi Das Nothern India Institute of Technology, Lucknow.
In the current investigations, mouth dissolving tablets (MDT) were developed by using natural superdisinegranting agent isolated from Plantago Ovata Seeds. Direct compression method was applied for the preparation of MDT containing aspirin using 2 factorial designs with quantity of drug, microcrystalline cellulose (MCC) and Plantago Ovata cellulose as dependent variables. MCC and Plantago Ovata cellulose were used as superdisintegrants. Magnesium stearate was used as lubricant. Developed MDT were evaluated for characteristics like hardness, friability, disintegration time (DT) and in vitro drug release. Design described adequately impact of selected variables (MCC and Plantago Ovata cellulose) at various levels for response under study (DT and friability). The optimized batch showed disintegration time of 22-29 secs, friability within 1% and in vitro drug release of 75-98?ter 30 mins, respectively. The present study of experimental design revealed that MCC and Plantago Ovata cellulose are fruitful at low concentration to develop the optimized formulation. As per the results obtained from the experiments, it can be concluded that Plantago Ovata seeds cellulose use as binder and as well as superdisintegrants an effective and efficient approach for the development of quality into MDT with the application of Mouth Dissolving.
Nonsteroidal Anti-inflammatory Drug (NSAID)
All drugs grouped in this class have analgesic, antipyretic and anti-inflammatory actions in different measures. In contrast to morphine, they do not depress CNS, do not produce physical dependence, have no abuse liability and are weaker analgesics (except for inflammatory pain). They are also called nonnarcotic, nonopioid or aspirin-like analgesics. They act primarily on peripheral pain mechanisms, but also in the CNS to raise pain threshold. They are more commonly employed and many are over-the-counter drugs. Willow bark (Salix alba) had been used for many centuries. Salicylic acid was prepared by hydrolysis of the bitter glycoside obtained from this plant. Sodium salicylate was used for fever and pain in 1875; its great success led to the introduction of acetylsalicylic acid(aspirin) in 1899.Phenacetin and antipyrine were also produced at that time. The next major advance was the development of phenylbutazone in 1949 having anti-inflammatory activity almost comparable to corticosteroids. The term nonsteroidal anti-inflammatory Drug S(NSAID) was coined to designate such drugs. Indomethacin was introduced in 1963. A host of compounds heralded by the propionic acid derivative ibuprofen have been added since then and cyclooxygenase (COX) inhibition is recognized to be their most important mechanism of action. Subsequently some selective COX-2 inhibitors (celecoxib, etc.) have been added. The antipyretic-analgesics are chemically diverse, but most are organic acids.
Aspirin
Aspirin, also known as acetylsalicylic acid (ASA), is a medication used to reduce pain, fever, or inflammation. Specific inflammatory conditions which aspirin is used to treat include Kawasaki disease, pericarditis, and rheumatic fever. Aspirin should be given to patients with unstable angina or a suspected myocardial infarction immediately. The ISIS-2 trial demonstrated that aspirin at doses of 160 mg daily for 1 month,decreased the mortality by 21% of patients with a suspected myocardial infarction in the first 5 weeks. A single daily dose of 324 mg of aspirin for 12 weeks has a highly protective effect against acute myocardial infarction and death in men with unstable angina. Aspirin is also used long-term to help prevent further heart attacks, ischaemic strokes, and blood clots in people at high risk. For pain or fever, effects typically begin within 30 minutes. Aspirin is a nonsteroidal anti- inflammatory drug (NSAID) and works similarly to other NSAIDs but also suppresses the normal functioning of platelets. Aspirin, often used as an analgesic, anti- pyretic and non-steroidal anti-inflammatory drug (NSAID), is able to have an anti-platelet effect by inhibiting the COX activity in the platelet to prevent the production of thromboxane A2 which acts to bind platelets together during coagulation as well as cause vasoconstriction and bronchoconstriction. One common adverse effect is an upset stomach. More significant side effects include stomach ulcers, stomach bleeding, and worsening asthma Bleeding risk is greater among those who are older, drink alcohol, take other NSAIDs, or are on other blood thinners. Aspirin is not recommended in the last part of pregnancy. It is not generally recommended in children with infections because of the risk of Reye syndrome. High doses may result in ringing in the ears. (44,000 tons) (50 to 120 billion pills) consumed each year. It is on the World Health Organization's List of Essential Medicines. It is available as a generic medication. In 2019, it was the 38th most commonly prescribed medication in the United States, with more than18 million prescriptions.
Chemical Properties
Aspirin decomposes rapidly in solutions of ammonium acetate or the acetates, carbonates, citrates, or hydroxides of the alkali metals. It is stable in dry air, but gradually hydrolyses in contact with moisture to acetic and salicylic acids. In solution with alkalis, the hydrolysis proceeds rapidly and the clear solutions formed may consist entirely of acetate and salicylate. Like flour mills, factories producing aspirin tablets must control the amount of the powder that becomes airborne inside the building, because the powder-air mixture can be explosive. The National Institute for Occupational Safety and Health (NIOSH) has set a recommended exposure limit in the United States of 5 mg/m3 (time-weighted average) In 1989, the Occupational Safety and Health Administration (OSHA) set a legal permissible exposure limit for aspirin of 5 mg/m3, but this was vacated by the AFL-CIO v. OSHA decision in 1993.
Syntnesis
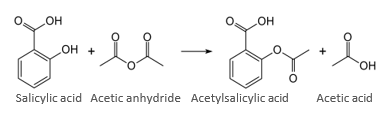
The synthesis of aspirin is classified as an esterification reaction. Salicylic acid is treated with acetic anhydride, an acid derivative, causing a chemical reaction that turns salicylic acid's hydroxyl group into an ester group (R-OH→ R-OCOCH3). This process yields aspirin and acetic acid, which is considered a byproduct of this reaction. Small amounts of sulfuric acid (and occasionally phosphoric acid) are almost always used as a catalyst. This method is commonly demonstrated in undergraduate teaching labs.
Physical Properties
Aspirin, an acetyl derivative of salicylic acid, is a white, crystalline, weakly acidic substance, with a melting point of 136 °C (277 °F) and a boiling point of 140 °C (284 °F).] Its acid dissociation constant (pKa) is 3.5 at 25 °C (77 °F).
Mechanism Of Action of Aspirin
Prostaglandins and thromboxane’s
Aspirin's ability to suppress the production of prostaglandins and thromboxane’s is due to its irreversible inactivation of the cyclooxygenase (COX; officially known as prostaglandin- endoperoxide synthase, PTGS) enzyme required for prostaglandin and thromboxane synthesis. Aspirin acts as an acetylating agent where an acetyl group is covalently attached to a serine residue in the active site of the PTGS enzyme (Suicide inhibition). This makes aspirin different from other NSAIDs (such as diclofenac and ibuprofen), which are reversible inhibitors.
COX-1 and COX-2 inhibition
At least two different types of cyclooxygenases, COX-1 and COX-2, are acted on by aspirin. Aspirin irreversibly inhibits COX-1 and modifies the enzymatic activity of COX-2. COX-2 normally produces proteinoids, most of which are proinflammatory. Aspirin-modified PTGS2 (prostaglandin-endoperoxide synthase 2) produces lipoxins, most of which are anti- inflammatory. Newer NSAID drugs, COX-2 inhibitors (coxibs), have been developed to inhibit only PTGS2, with the intent to reduce the incidence of gastrointestinal side effects. Several COX-2 inhibitors, such as rofecoxib (Vioxx), have been withdrawn from the market, after evidence emerged that PTGS2 inhibitors increase the risk of heart attack and stroke. Endothelial cells lining the microvasculature in the body are proposed to express PTGS2, and, by selectively inhibiting PTGS2, prostaglandin production (specifically, PGI2; prostacyclin) is downregulated with respect to thromboxane levels, as PTGS1 in platelets is unaffected. Thus, the protective anticoagulative effect of PGI2 is removed, increasing the riskof thrombus and associated heart attacks and other circulatory problems. Since platelets have no DNA, they are unable to synthesize new PTGS once aspirin has irreversibly inhibited the enzyme, an important difference with reversible inhibitors.
Additional Mechanisms
Aspirin has been shown to have at least three additional modes of action. It uncouples oxidative phosphorylation in cartilaginous (and hepatic) mitochondria, by diffusing from the inner membrane space as a proton carrier back into the mitochondrial matrix, where it ionizes once again to release protons. Aspirin buffers and transports the protons. When high doses are given, it may cause fever, owing to the heat released from the electron transport chain, as opposed to the antipyretic action of aspirin seen with lower doses. In addition, aspirin induces the formation of NO-radicals in the body, which have been shown in mice to have an independent mechanism of reducing inflammation. This reduced leukocyte adhesion is an important step in the immune response to infection; however, evidence is insufficient to show aspirin helps to fight infection. More recent data also suggest salicylic acid and its derivatives modulate signalling through NF-κB. NF-κB, a transcription factor complex, plays a central role in many biological processes, including inflammation.
Medical Use
Aspirin is an effective analgesic for acute pain, although it is generally considered inferior to ibuprofen because aspirin is more likely to cause gastrointestinal bleeding. Aspirin is generally ineffective for those pains caused by muscle cramps, bloating, gastric distension, or acute skin irritation. As with other NSAIDs, combinations of aspirin and caffeine provide slightly greater pain relief than aspirin alone. Effervescent formulations of aspirin relieve pain faster than aspirin in tablets, which makes them useful for the treatment of migraines. Topical aspirin may be effective for treating some types of neuropathic pain.
Fever
Like its ability to control pain, aspirin's ability to control fever is due to its action on the prostaglandin system through its irreversible inhibition of COX. Although aspirin's use as an antipyretic in adults is well established, many medical societies and regulatory agencies, including the American Academy of Family Physicians, the American Academy of Paediatrics, and the Food and Drug Administration, strongly advise against using aspirin for treatment of fever in children because of the risk of Reye's syndrome, a rare but often fatal illness associated with the use of aspirin or other salicylates in children during episodes of viral or bacterial infection. Because of the risk of Reye's syndrome in children, in 1986, the US Food and Drug Administration (FDA) required labelling on all aspirin-containing medications advising against its use in children and teenagers.
Inflammation
Aspirin is used as an anti-inflammatory agent for both acute and long-term inflammation, as well as for treatment of inflammatory diseases, such as rheumatoid arthritis.
Heart attacks and strokes
Aspirin is an important part of the treatment of those who have had a heart attack. It is generally not recommended for routine use by people with no other health problems, including those over the age of 70. The 2009 Antithrombotic Trialists’ Collaboration published in Lancet evaluated the efficacy and safety of low dose aspirin in secondary prevention. In those with prior ischaemic stroke or acute myocardial infarction, daily low dose aspirin was associated with a 19% relative risk reduction of serious cardiovascular events (non-fatal myocardial infarction, non-fatal stroke, or vascular death). This did come at the expense of a 0.19% absolute risk increase in gastrointestinal bleeding; however, the benefits outweigh the hazard risk in this case. Data from early trials of aspirin in primary prevention suggested low dose aspirin is more beneficial for people <70 kg and high dose aspirin is more beneficial for those ≥70 kg. However, more recent trials have suggested lower dose aspirin is not more efficacious in people with a low body weight and more evidence is required to determine the effect ofhigher dose aspirin in people with a high body weight. The United States Preventive Services Task Force (USPSTF), in 2016, recommended initiating low-dose aspirin use for the primary prevention of cardiovascular disease and colon cancer in adults aged 50 to 59 years who have a 10% or greater 10-year cardiovascular disease (CVD) risk, are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose aspirin daily for at least 10 years. However, in 2021, the USPSTF recommended against the routine use of daily aspirin for primary prevention in adults in their 40s and 50s, citing the fact that the risk of side effects outweighs the potential benefits. In April 2022, the USPSTF said "people ages 40 to 59 who are at higher risk for CVD should decide with their clinician whether to start taking aspirin; people 60 or older should not start taking aspirin to prevent a first heart attack or stroke."
Cancer prevention
Aspirin may reduce the overall risk of both getting cancer and dying from cancer. There is substantial evidence for lowering the risk of colorectal cancer (CRC), but must be taken for at least 10–20 years to see this benefit. It may also slightly reduce the risk of endometrial cancer, breast cancer, and prostate cancer. Some conclude the benefits are greater than the risks due to bleeding in those at average risk. Others are unclear if the benefits are greater than the risk. Given this uncertainty, the 2007 United States Preventive Services Task Force (USPSTF) guidelines on this topic recommended against the use of aspirin for prevention of CRC in people with average risk. Nine years later however, the USPSTF issued a grade B recommendation for the use of low- dose aspirin (75 to 100 mg/day) "for the primary prevention of CVD [cardiovascular disease] and CRC in adults 50 to 59 years of age who have a 10% or greater 10-year CVD risk, are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose aspirin daily for at least 10 years".
Adverse Effects
In October 2020, the U.S. Food and Drug Administration (FDA) required the drug label to be updated for all nonsteroidal anti- inflammatory medications to describe the risk of kidney problems in unborn babies that result in low amniotic fluid They recommend avoiding NSAIDs in pregnant women at 20 weeks or later in pregnancy. One exception to the recommendation is the use of low-dose 81 mg aspirin at any point in pregnancy under the direction of a health care professional.
• Contraindications
• Gastrointestinal
• Retinal vein occlusion
• Skin
Overdose
Aspirin overdose can be acute or chronic. In acute poisoning, a single large dose is taken; in chronic poisoning, higher than normal doses are taken over a period of time. Acute overdose has a mortality rate of 2%. Chronic overdose is more commonly lethal, with a mortality rate of 25%; chronic overdose may be especially severe in children. Toxicity is managed with a number of potential treatments, including activated charcoal, intravenous dextrose and normal saline, sodium bicarbonate, and dialysis. The diagnosis of poisoning usually involves measurement of plasma salicylate, the active metabolite of aspirin, by automated spectrophotometric methods. Plasma salicylate levels in general range from 30 to 100 mg/l after usual therapeutic doses, 50–300 mg/l in people taking high doses and 700–1400 mg/l following acute overdose. Salicylate is also produced as a result of exposure to bismuth subsalicylate, methyl salicylate, and sodium salicylate.
Interactions
Aspirin is known to interact with other drugs. For example, acetazolamide and ammonium chloride are known to enhance the intoxicating effect of salicylates, and alcohol also increases the gastrointestinal bleeding associated with these types of drugs. Aspirin is known to displace a number of drugs from protein- binding sites in the blood, including the antidiabetic drugs tolbutamide and chlorpropamide, warfarin, methotrexate, phenytoin, probenecid, valpr oic acid (as well as interfering with beta oxidation, an important part of valproate metabolism), and other NSAIDs. Corticosteroids may also reduce the concentration ofaspirin. Other NSAIDs, such as ibuprofen and naproxen, may reduce the antiplatelet effect of aspirin Although limited evidence suggests this may not result in a reduced cardioprotectiveeffect of aspirin Analgesic doses of aspirin decrease sodium loss induced by spironolactonein the urine, however this does not reduce the antihypertensive effects of spironolactone. Furthermore, antiplatelet doses of aspirin are deemed too small to produce an interaction with spironolactone. Aspirin is known to compete with penicillin G for renal tubular secretion. Aspirin may also inhibit the absorption of vitamin C.
Formulation of aspirin mouth dissolving tablet
Mouth dissolving tablet disintegrate or dissolve in saliva and are swallowed without the need for water. They offer an advantage over swallowing tablets and capsules. Difficulty to swallow is particularly experienced by paediatric and geriatric patients. Technique that are frequently employed in the preparation of mouth dissolving tablets include, freeze drying, sublimation, spray drying, moulding, mass extrusion and direct compression. Direct compression method was applied for the formulation of MDT containing aspirin using various excipients such as diluents and superdisintegrants and evaluated for different parameters like hardness, friability, disintegration time and dissolution profile to identify best combination further for preparation of MDT. As per the batches mentioned in Table.1, all ingredients like aspirin, cross carmellose sodium, spray dried lactose, microcrystalline cellulose and talc were sieved using sieve no. 40 individually. API was mixed with the superdisintegrants and other ingredients. Sodium stearyl fumarate was applied for lubrication of the powder mix and this blend was compressed into tablet using 9.7 mm biconvex punch on a tablet compression machine.
Method Of Pripation
• Direct compression
Evaluation Parameter
• Pre-Compression Evaluation-
• Bulk density
• Tapped density
• Angle of repose
• Carr’s index
• Hausner’s ratio
• Physical properties
• Melting rang
• Solubility
Post-Compression Evaluation-
• Weight variation test
• Thickness test
• Hardness test
• Percent friability test
• Disintegration time
• Percent drug release
Pre-compression study of powder blend
Bulk density. Accurately weighed sample was filled in measuring cylinder to determine volume of the powder as Vo. The formula for calculation of bulk density as follows.3,13
Bulk density (ρo) = M/Vo (1)
Where, M= mass of powder Vo= apparent unstirred volume Tapped density. The measuring cylinder tapped mechanically to determine tapped volume for calculation of tapped density using following formula.3,13
Tapped density (ρt) = M / Vt (2) Were,
Ρt = tapped density
M = weight of granules
Vt = tapped volume of granules in cm3
Angle of repose. In funnel method for determination of angle of repose, accurately weighed mix was allowed to pass freely onto the surface and form heap of the powder to which tip of the funnel just touched. Diameter of cone by powder mix and pile height ‘h’ was applied for the calculation of angle of repose using following formula.
Tan ? = H /R (3)
Thus, ? = tan –1 H /R (4) Where, H= Pile height
R= Radius of pile
Compressibility index (Carr’s index). Carr’s index calculated by substituting bulk volume and tapped volume in the following formula4,13, Compressibility index= 100 (Vo-Vf)/Vo ×10 …. (5) Where, Vo = Bulk volume
Vf = Tapped volume
Hausner’s ratio. Hausner’s ratio calculated by substituting bulk volume and tapped volume in the following formula
Hausner’s ratio = Vo/Vf (6)
Where, Vo = Bulk volume Vf = Tapped volume
Better flow property is detected from low values of Hausner’s ratio and vice a versa.
Post compression study of aspirin MDT Thickness.
Five tablets of each formulation batch was subjected to Vernier Caliper (Dial Cappiler/Advance) for detection of thickness. Average values in mm were considered for further study.
Hardness. Tablets of each formulation batch were subjected to Monsanto hardness tester (Dolphin) for detection of hardness (kg/cm2) and results were noted.
Friability. Tablet strength was determined using Friability test apparatus, Roche Friabilator (META LAB). Pre-weighed sample of 20 tablets were subjected to 100 revolutions, followed by de-dusted and reweighed. A loss of less than 1 % in weight in generally considered acceptable.
|
S. No |
Ingredient |
Quantity per tablet (F1) |
(F2) |
For 25 table TS |
|
1 |
Aspirin |
50mg |
50mg |
1.5g |
|
2 |
Lactose(diluent) |
50mg |
50mg |
1.50g |
|
3 |
MCC (binder) |
31mg |
31mg |
0.775g |
|
4 |
Talc(glidant) |
2mg |
2mg |
0.05g |
|
5 |
Magnesium stearate |
2mg |
2mg |
0.05g |
|
6 |
Sodium starch glycolate (superdi sintegrants) |
3mg |
- |
0.075g |
|
7 |
Plantago ovata seedmucilage |
- |
3mg |
00.075g |
|
8 |
Mannitol |
40mg |
40mg |
1g |
Weight variation test. Individual weight of each tablet and average weight for 20 tablets of each formulation batch were calculated. Single tablet weight against average tablet weight was applied to find the deviation in weight.
Formulation And Development
Isolation of mucilage from Plantago ovata seeds-
Isolation of Mucilage-Mucilage was isolated by soaking seeds of Plantago ovata in water (20-30 times) for at least 48 hrs, boiled for 2 hrs subsequently mucilage was released into the water completely. With the help of the muslin cloth the mucilage was squeezed out and separated from seeds. The mucilage collected and precipitated using 3 times of 95% ethanol. Collected mucilage was dried in the oven at 50- 55°. Dried mucilage was scraped and powdered using pestle and mortar. Powder was sieved using mesh no.60
Method Direct compression
Tablets are the most widely used solid dosage form and should meet a number of requirements for physical characteristics such as hardness, decay, durability and uniform mass, content. In order to meet the characteristics of the tablets in accordance with the selected components, the manufacturer can use three different compression technologies such as straight stamping (direct compression), dry grain rubbing and wetting of wet particles. Most of the medicinal substances need mixing with the excipients to rub seeds before the tablets. Today, in the pharmaceutical industry, there are many pre-manufactured manufacturers of multipurpose excipients and the introduction of modern stamping equipment that can help to extinguish directly, simply mix the mixture in a dry and compressed state without rubbing Particle or adjustment of physical characteristics. The method of direct stamping was previously understood to be single-stamping. Therefore, only used for substances that have a smooth and well-compressed substance such as potassium salts (chlorate, Chloride, Bromide, Iodide, nitrate and permanganate), ammonium chloride, ammonium bromide, sodium chloride, sodium tetraborate, zinc sulphate, Urotropine, Pancreatin and Methenamine Today, direct compression is understood as the method of tablet compression without the stage of grinding seeds. Direct compression is a simple, easy to control and least expensive stamping process. The direct compression has only two main steps, dry mixing, and tablet compression. The method of wet particle rubbing has 4 additional steps: Wet mixing, particle rubbing, drying, particle repair. Not only does that require more equipment, machinery, space, manpower, costs but also the risk of cross contamination and product losses.
Evaluation
Post compression study of aspirin MDT Tablet Hardness
The hardness was examined by using Hardness tester (Pharma Test Model PTB-31, Ser. No. I-4390/B). The mean and standard deviation were calculated from three determinations.
|
S. No |
Hardness test(F1) |
Hardness test(F2) |
|
1 |
4 |
2.5 |
|
2 |
3.5 |
2.0 |
|
3 |
4 |
2.0 |
Percent Friability
The friability of tablets was determined by using Erweka Abrasion Tester (Model 1AP No.24438, Germany). The method of determination was according to British Pharmacopoeia 1998 (BP 1998). The percent friability was obtained from 20-tablet sample.
|
S. No |
Initial weight |
Final weight |
%friability |
|
1 |
6.93gm |
6.91gm |
0.2886 |
Disintegration Time
The disintegration time was measured by using USP XXIV disintegration apparatus (Pharma Test, Model PTZ1 No. 1-3869/A) with purified water at 37?C as disintegration medium. The mean and standard deviation were calculated from six determinations.
|
IP/BP |
Average Mass Limit |
USP |
|
Tablets weight 80mg or less |
±10% |
Tablets weight 130mg or less |
|
More than 80mg or less than120mg |
±7.5% |
130mg to 324mg |
|
250mg or more |
±5% |
More than 324mg |
Thickness test
The thickness of the tablet is the only dimensional variable related to the tablet compression process. Generally, it is measure with a micrometre. The thickness should control within ±5% variation of a standard value and must control for patient acceptance and make the tablet packaging easier.
|
S. No |
Main scale |
Vernier scale |
Least count |
|
1 |
0.52 |
0.82 |
0.63 |
Percent Drug Release
The dissolution study was followed as stated in BP 1998. Five-hundred millilitres of acetate buffer was used as dissolution medium. The paddle was rotated at 50 rpm. The release profile of tablet was determined from six tablets. The five millilitres of sample were withdrawn and passed through 0.45 µm filter at the time interval of 2, 5, 8, 10, 15, 20, 25,30, 35, 40 and 45 minutes. Acetate buffer was replaced into the vessel in equal volume to maintain the constant volume of dissolution medium. The absorbance of sampling solution was determined by using spectrophotometer at 265 nm. Some collections were diluted with dissolution medium to obtain the appropriate absorption.
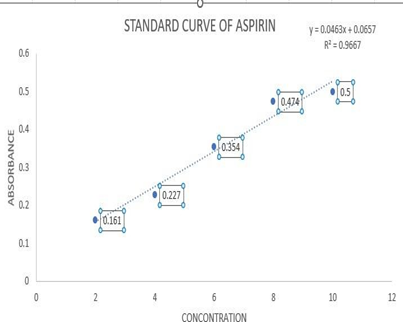
Standard Curve of Aspirin
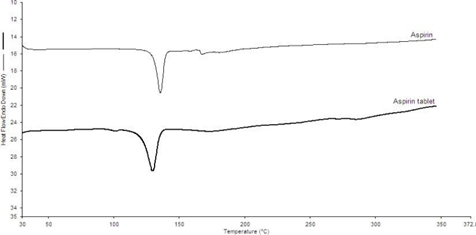
DSC of Aspirin and Aspirin Tablet.
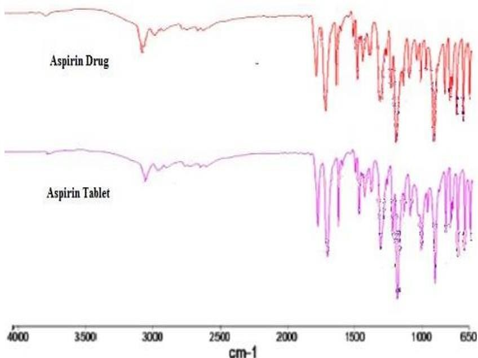
FTIR of aspirin and aspirin tablet
RESULTS AND DISCUSSION
Components of drug product.
Drug substance (aspirin).
After few trial runs, formulation is developed depending upon API’s various physiochemical and biological characteristics such as particle size, water content, solubility, biological activity, permeability, and stability etc. Thus, performance of the formulation and manufacturing process are enhanced using above mentioned characteristics.
Excipients
Microcrystalline cellulose.
For direct compression, Avicel PH 112 grade is used because of less % of moisture contentas compared to other grades, free from interaction between API and MCC. As per literature, physical binding / adsorption between the MCC and API is reported which is not found in studies of our formulation batches.
QTPP for aspirin MDTs.
Dosage form- As per the pharmaceutical equivalence requirement, dosage form of aspirin MDTs is same as reference listed drug (RLD).
Route of administration.
To improve the ease of administration, the route of administration is similar to the RLD.
Stability.
Stability of the product is important for safety and efficacy. Stability of aspirin MDTs is 36 months at room temperature and it should equivalent to or better than RLD shelf life.
Friability.
As per the pharmacopoeia requirement, friability of the MDTs found to be less than 1.0%.
Dissolution:
Bioavailability of any formulation depends upon results of dissolution specifications. Dissolution profile for MDTs was found to be more than 85% drug release at 30 minutes.
Critical quality attributes of the aspirin MDTs.
Desired quality in product can be ensured by maintaining physical, chemical, biological, or microbiological property or characteristic in appropriate limit, range which is known as critical quality attribute (CQA). Thus, QTPP helps to identify CQA. For the aspirin MDTs, disintegration, dissolution, assay, friability were identified as CQAs.
Physical Attributes
Appearance. Colour, odour of aspirin MDTs are indirectly associated to safety and efficacy. Hence appearance was not considered as CQA for the aspirin MDT’s (current product).
Odour. In current formulation batches, API and excipients are free from any unpleasant odour whereas manufacturing process did not apply any organic solvents. Hence odour is not considered as CQA for the Aspirin MDT’s (current product).
Friability. An objective with not more than 1.0% as mean weight loss is fixed as per pharmacopeial requirement. Hence, if it exceeds the standard limits (NMT 1%), it will cause impact on patient’s safety, efficacy and product handling. Hence friability is considered as CQA for the aspirin MDT’s (current product). Identification. Identification test establish the identity of the drug in the product. The most conclusive test for identity is the infrared absorption spectrum. Identification test was found to be positive for the aspirin. Drug identification was not affected by formulation and process variables. So, identification test is not considered as CQA for the Aspirin MDT’s (current product).
Dissolution. Drug release profile of aspirin MDTs was found to be same as RLD using predictive dissolution method. On the basis of trail batches, dissolution profile was dependent on variables of formulation and process. Hence, dissolution is considered as CQA for the Aspirin MDT’s (current product). Assay. Safety and efficacy of formulation get affected by assay variability. Variation in results of assay for any formulation depends upon process variables. Hence assay was evaluated throughout product and process development.
Disintegration test. As per compendial requirement, DT of MDT should not be more than 30s. Formulation or process variables effect on DT. Hence, disintegration test was considered as CQA for the aspirin MDT’s (current product). The particle size, shape and type of adherence of particles decide bulk density. The values for BD and TD are shown in table. 3. The results were found to be in range from 0.555 ± 0.03to 0.652 ± 0.025 (BD) and 0.625 ± 0.001 to 0.785 ± 0.013 (TD) for powder blend respectively. The angle of repose and Carr’s Index of powder blend was detected in between 22.55 ± 0.08 to 26.90 ± 0.07 and 8.02 ± 1.79 to 15.63 ± 1.31 respectively.
Hausner’s ratio
was detected in between 1.050 ± 0.004 to 1.85 ± 0.007.
Hardness. Hardness of tablets was detected in between 2.5-4.00 kg/cm2. The hardness of tablet varied although compression force was constant. The current outcome might be due to the increased concentration of the superdisintegrants in the formulations.
Thickness. The tablets observed from 6.148 to 6.526 mm in thickness with minimum standard deviation values showed uniformity in the thickness respectively.
% Friability. Friability was important to study weight loss of formulation. % Friability of tablets was found to be 0.20 to 0.80% which is within acceptable limit.
Weight variation. All the formulation were varied from 240.00-280.00 mg which indicated that the uniform distribution of excipients and drug.
Disintegration time. High concentration of MCC in the formulation increases the hardness of the tablet. DT of all tablets were found to be in range of 22-29 sec.
% Drug release. When MCC and CCS are used in low concentrations significantly gave higher drug release to 98.58%. Hence, % of drug release decreases with escalation of MCC concentration.
CONCLUSION
full factorial design revealed that the amounts of Plantago ovata mucilage (X1) and microcrystalline cellulose (f2) significantly affect the dependent variable (f11), the in vitro dispersion time. It is thus concluded that, by adopting a systematic formulation approach, an optimum point can be reached in the shortest time with minimum efforts. Direct compression method by using natural super disintegrants would be an effective approach compared with the use of more expensive excipients in the formulation of fast disintegrating tablets with smaller disintegration time, improved drug dissolution, patient compliance, convenience, and acceptability.
ACKNOWLEDGEMENT
This project consumed amount of work, research and dedication. Still, implementation would not have been possible if I not have a support of many individuals and organization. Therefore, I would like to extend my sincere gratitude to all of them. Primarily, I would than God for being able to complete this project with success. Then, it is my pleasure to express my deep sense of gratitude of thankfulness to Prof. Dr. Shailendra K. Saraf, Director of Pharmacy, B.B.D.N.I.I.T., Lucknow and, Ms Anushri Prakash, B.B.D.N.I.I.T., Lucknow, whose valuable guidance has been the one that helped me complete this project and make it full proof success. Their suggestions and instructions have served as the major contributor toward completion of the project. I am cordially grateful to my parents, my family members and my friends who always covered their shade of blessing and provide their valuable moral support and corporation in the completion of the project.
REFERENCES


Rahul Tiwari*, Anjali Tiwari*, Formulation and Evaluation of Mouth Dissolving Aspirin Tablet by Using a Natural Superdisintegranting Agent Isolated from Plantago Ovata seeds, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 3046-3059 https://doi.org/10.5281/zenodo.17002967
 10.5281/zenodo.17002967
10.5281/zenodo.17002967
