
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Senior Consultant in Diagnostic Imaging, University of Nebraska Medical Center, Nebraska, USA
2 Associate Professor of Diagnostic Radiology and Imaging Informatics, University of Nebraska Medical Center, Nebraska, USA
3 Consultant Neuroradiologist and Clinical Imaging Researcher, University of Nebraska Medical Center, Nebraska, USA
Cancer remains one of the most complex and heterogeneous diseases in modern medicine, characterized by genomic instability, immune dysregulation, metabolic alterations, and tumor microenvironment diversity. Despite major advances in molecular diagnostics and targeted therapies, significant challenges persist in early detection, prognostic prediction, therapeutic stratification, and adaptive treatment planning. The emergence of artificial intelligence (AI), particularly foundation models, has introduced a transformative approach to precision oncology through large-scale learning from multimodal biomedical data. Foundation models are large pre-trained AI systems capable of performing diverse clinical tasks using transfer learning and self-supervised learning techniques. Recent developments in transformer architectures, vision-language models, and multimodal fusion systems have accelerated their applications in digital pathology, radiology, genomics, immuno-oncology, and clinical decision support. These models can integrate histopathological images, radiological scans, genomic and transcriptomic data, proteomic signatures, and electronic health records to generate biologically informed predictions for diagnosis, prognosis, and therapeutic response. Foundation models have demonstrated promising performance in tumor classification, molecular prediction, radiogenomic analysis, and survival estimation. However, challenges related to interpretability, algorithmic bias, data privacy, computational complexity, and regulatory validation remain barriers to clinical translation. This review highlights the architecture, applications, limitations, and future potential of foundation models in enabling adaptive and personalized cancer care.
Cancer represents a biologically heterogeneous disease involving extensive genomic instability, epigenetic dysregulation, immune escape mechanisms, and dynamic tumor microenvironment interactions. The complexity of cancer progression contributes substantially to therapeutic resistance, interpatient variability, and inconsistent clinical outcomes [1–6]. Conventional oncology workflows primarily rely on histopathological examination, radiological imaging, molecular profiling, and laboratory investigations; however, these approaches often remain limited by interobserver variability, fragmented data interpretation, delayed diagnosis, and inability to integrate large-scale multimodal biological information [7,8].
The rapid expansion of biomedical data generated through next-generation sequencing, digital pathology, radiomics, proteomics, and electronic health records has significantly exceeded the interpretive capacity of conventional analytical methods. Artificial intelligence has therefore emerged as a transformative technology in oncology by enabling computational analysis of complex heterogeneous datasets. Early oncology AI systems were dominated by conventional machine learning algorithms such as support vector machines and random forests, which were later replaced by convolutional neural networks capable of advanced image recognition and feature extraction [9,10].
More recently, foundation models have revolutionized computational oncology through their ability to learn generalized representations from large-scale biomedical datasets. Unlike traditional task-specific AI systems, foundation models utilize self-supervised learning and transformer-based architectures to adapt efficiently across multiple downstream oncology applications with minimal fine-tuning. Such adaptability is particularly important in precision oncology because tumor progression involves interconnected genomic, radiological, histopathological, immunological, and clinical variables [11].
The integration of multimodal learning has further accelerated the development of oncology-specific foundation models capable of simultaneously analyzing whole-slide pathology images, radiological scans, transcriptomic signatures, and clinical narratives. These systems can identify subtle biological relationships that are frequently undetectable through conventional analysis. The multimodal computational frameworks discussed in this introduction form the conceptual foundation for the pathology and radiogenomic systems described in subsequent sections [12].
2. Historical Evolution of Artificial Intelligence in Oncology
The evolution of artificial intelligence in oncology has progressed through several transformative stages. Early computational oncology systems primarily relied on statistical learning models designed for limited structured datasets. These approaches demonstrated modest utility in cancer risk prediction and biomarker classification but lacked scalability and generalizability across diverse clinical settings [13].
The emergence of deep learning significantly advanced oncology AI by enabling hierarchical feature extraction from complex biomedical images. Convolutional neural networks rapidly became dominant in digital pathology and radiology due to their ability to automatically identify spatial features associated with tumor morphology and imaging phenotypes. Deep learning systems subsequently demonstrated diagnostic performance comparable to expert clinicians in several cancer domains, including breast cancer, lung cancer, colorectal cancer, and melanoma [14].
The introduction of transformer architectures represented a major paradigm shift in computational medicine. Transformers utilize self-attention mechanisms capable of modeling long-range contextual dependencies, thereby enabling more sophisticated multimodal learning than conventional convolutional systems. Vision transformers and multimodal transformer architectures are now increasingly integrated into pathology, genomics, radiology, and clinical language processing [15].
Large language models have further expanded the scope of oncology AI by enabling automated clinical documentation, literature synthesis, evidence extraction, and therapeutic decision support. The emergence of these systems has accelerated development of highly integrated oncology intelligence platforms capable of supporting real-time precision medicine workflows [16].
3. Foundation Models: Concept, Architecture, and Computational Framework
Foundation models are large-scale pre-trained artificial intelligence systems capable of learning generalized biomedical representations from multimodal datasets. These systems utilize self-supervised learning, transfer learning, and transformer-based architectures to support diverse downstream clinical applications [17].
Transformer architectures represent the computational backbone of modern foundation models. Unlike conventional convolutional systems, transformers employ self-attention mechanisms capable of identifying contextual relationships between distant data elements. The self-attention operation can be mathematically expressed as:
Attention(Q,K,V)=softmaxQKTdkV

Self-supervised learning further enhances scalability by reducing dependence on manually annotated datasets. Instead of relying solely on labeled clinical data, models learn intrinsic biological structures through masked prediction tasks, contrastive learning, and multimodal representation alignment. This strategy is especially valuable in oncology because expert annotation of histopathological slides and genomic datasets remains resource intensive [19].
Multimodal learning frameworks integrate heterogeneous biomedical modalities including histopathology, radiology, genomics, transcriptomics, proteomics, and clinical records. Such integration substantially improves predictive performance and forms the basis for the precision oncology systems discussed in Sections 6–9 [20].
4. Transformer Architectures and Self-Supervised Learning in Oncology
Transformer architectures have become central to modern oncology AI because of their ability to process large-scale multimodal biomedical data while preserving contextual relationships. Vision transformers segment pathology slides into smaller image patches treated as sequential tokens, enabling efficient representation learning across gigapixel whole-slide images [21].
Self-supervised learning has emerged as a critical strategy in oncology because labeled biomedical datasets remain limited. Contrastive learning approaches train models to distinguish biologically related representations from unrelated samples, thereby improving feature robustness and generalizability. Masked autoencoders further enable reconstruction of missing image or genomic regions, allowing models to learn intrinsic biological structures without explicit annotations [22].
These transformer-based learning systems significantly improve scalability in pathology, radiology, and genomics. The computational frameworks discussed in this section directly support the pathology applications described in Section 5 and radiogenomic systems presented in Section 6 [23].
5. Foundation Models in Digital Pathology
Digital pathology has become one of the most important application domains for oncology foundation models. Whole-slide imaging technologies generate extremely high-resolution digital representations of tissue specimens capable of revealing complex histomorphological patterns associated with malignancy, immune infiltration, stromal remodeling, and metastatic progression [24].
Foundation models trained on millions of pathology image patches can identify subtle morphological signatures associated with tumor subtype, prognosis, and molecular alterations. These systems have demonstrated remarkable performance in breast cancer, lung adenocarcinoma, colorectal cancer, prostate cancer, and melanoma. Multiple-instance learning frameworks aggregate patch-level representations into slide-level predictions, thereby enabling accurate tumor classification and survival estimation [25].
A particularly important advancement involves molecular prediction directly from histopathological morphology. Transformer-based pathology systems can infer EGFR mutations, KRAS mutations, HER2 amplification, microsatellite instability, and PD-L1 expression directly from tissue architecture. Such capabilities may reduce dependence on expensive molecular testing while accelerating precision therapeutic stratification [26].
Tumor microenvironment analysis has also become a major focus of computational pathology. AI systems can quantify spatial relationships between tumor cells, stromal regions, immune infiltrates, and vascular structures to predict immunotherapy response and disease progression. The multimodal learning frameworks discussed in Section 8 substantially enhance these pathology systems through integration with genomic and transcriptomic datasets [27].
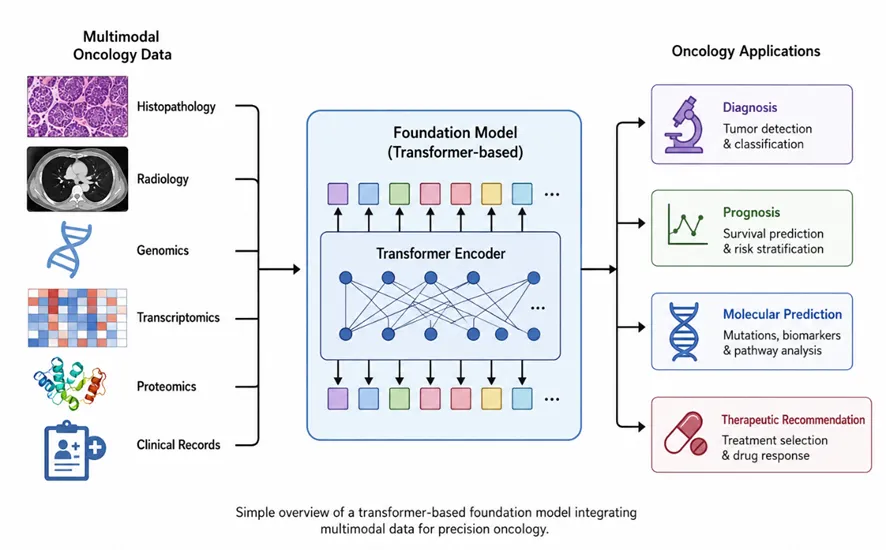
Figure 1. Foundation Model Architecture in Oncology
6. Foundation Models in Radiology and Medical Imaging
Radiology foundation models are transforming oncological imaging through automated lesion detection, tumor segmentation, radiogenomic prediction, and longitudinal disease monitoring. These systems analyze computed tomography, magnetic resonance imaging, positron emission tomography, mammography, and ultrasound data to identify imaging biomarkers associated with tumor biology [28].
Radiomics involves extraction of quantitative imaging features associated with intratumoral heterogeneity, vascularization, necrosis, and treatment response. Foundation models enhance radiomics through automated feature learning and multimodal integration. Such systems can identify high-dimensional imaging phenotypes beyond conventional human interpretation [29].
Radiogenomics represents an important translational application integrating radiological imaging with molecular profiling. AI systems can predict genomic alterations directly from imaging phenotypes, thereby supporting non-invasive precision diagnostics. These multimodal frameworks complement the molecular integration strategies discussed in Section 8 [30].
Transformer-based segmentation systems further improve delineation of tumor boundaries and metastatic lesions. Longitudinal imaging analysis also enables adaptive therapeutic monitoring and recurrence prediction, supporting real-time precision oncology workflows [31].
7. Multi-Omics Foundation Models in Precision Oncology
Cancer progression involves extensive molecular dysregulation across genomic, transcriptomic, proteomic, metabolomic, and epigenomic layers. Multi-omics foundation models integrate these heterogeneous biological datasets to generate comprehensive molecular representations associated with prognosis and therapeutic response [32].
Single-cell RNA sequencing has substantially advanced precision oncology by enabling characterization of intratumoral heterogeneity and clonal evolution. Foundation models trained on pan-cancer datasets can identify molecular signatures associated with metastasis, drug resistance, and immunotherapy responsiveness [33].
Spatial transcriptomics further enhances biological interpretation by combining gene expression profiling with spatial tissue context. These systems enable high-resolution mapping of tumor-immune interactions and stromal organization. Graph neural networks are increasingly incorporated into multi-omics systems to model pathway-level biological interactions and molecular signaling networks [34].
The multimodal architectures discussed in this section significantly improve pathology systems described in Section 5 and radiogenomic applications discussed in Section 6.
Table 1. Major Applications of Foundation Models in Oncology
|
Clinical Domain |
AI Application |
Clinical Utility |
|
Digital Pathology |
Tumor classification |
Faster diagnosis |
|
Radiology |
Lesion segmentation |
Early detection |
|
Genomics |
Mutation prediction |
Precision medicine |
|
Immunotherapy |
Response prediction |
Personalized therapy |
|
Clinical NLP |
Documentation support |
Workflow efficiency |
8. Foundation Models in Clinical Oncology and Personalized Therapeutics
Clinical oncology increasingly relies on AI-driven decision support systems capable of integrating pathology reports, radiological imaging, genomic data, laboratory findings, and electronic health records. Foundation models support therapeutic recommendation, toxicity prediction, clinical trial matching, and prognostic assessment [35].
Large language models have introduced additional capabilities in oncology through automated documentation, literature synthesis, evidence summarization, and clinical communication support. These systems substantially improve workflow efficiency and reduce clinician burden [36].
AI-assisted tumor boards represent another important application in which multimodal patient data are integrated to support multidisciplinary therapeutic decision-making. The explainability frameworks discussed in Section 10 are essential for ensuring clinician trust and regulatory acceptance of these systems [37].
9. Foundation Models in Immuno-Oncology
Immunotherapy has revolutionized modern oncology, although patient response remains highly variable. Foundation models increasingly support immuno-oncology through characterization of tumor microenvironment dynamics and immune cell interactions [38].
AI systems can quantify T-cell exhaustion, immune infiltration, stromal remodeling, and cytokine signaling patterns associated with immunotherapy responsiveness. Spatial immunomics integrates transcriptomics and digital pathology to identify biologically relevant immune niches within tumors [39].
Foundation models also support neoantigen prediction and personalized cancer vaccine development through integration of genomic and immunopeptidomic datasets. These systems contribute substantially to adaptive precision immunotherapy strategies [40].
10. Explainable AI and Interpretability in Cancer Medicine
Clinical implementation of foundation models requires transparency and interpretability. Explainable AI techniques improve clinician trust by identifying features contributing to model predictions [41].
Attention heatmaps, SHAP analysis, saliency mapping, and counterfactual explanations are increasingly used in pathology and radiology workflows to visualize biologically relevant prediction regions. Such interpretability is particularly important for regulatory approval and ethical implementation [42].
The explainability approaches described in this section are essential for overcoming the translational limitations discussed in Section 12.
11. Federated Learning and Privacy-Preserving Oncology AI
Cancer datasets remain highly sensitive and distributed across healthcare institutions. Federated learning enables collaborative model training without direct sharing of patient-level data [43].
In federated systems, local models are trained at individual institutions while only model parameters are aggregated centrally. This framework improves privacy preservation, regulatory compliance, and model generalizability across diverse populations [44].
Advanced federated systems incorporate differential privacy, secure aggregation, and decentralized AI architectures to further enhance cybersecurity and ethical governance. Such approaches may overcome several implementation barriers discussed in Section 12 [45].
12. Ethical, Regulatory, and Clinical Translation Challenges
Despite remarkable advances, substantial challenges continue to limit widespread implementation of foundation models in oncology. Dataset heterogeneity, annotation inconsistency, and demographic bias reduce model generalizability and may negatively affect underrepresented populations [46].
Large foundation models also require substantial computational infrastructure and energy consumption, limiting scalability in resource-constrained healthcare systems. Regulatory approval remains another major challenge because prospective clinical validation and real-world performance assessment are still limited [47].
Ethical concerns involving data ownership, informed consent, algorithmic transparency, and automated decision-making further complicate clinical implementation. The explainability systems discussed in Section 10 and federated learning approaches presented in Section 11 may partially mitigate these limitations [48].
13. Emerging Technologies Including Digital Twins, Generative AI, and Autonomous Oncology Systems
Future oncology ecosystems are expected to integrate foundation models with digital twins capable of simulating patient-specific tumor evolution and therapeutic response in real time [49].
Generative AI systems may accelerate oncology drug discovery, molecular design, and synthetic biomedical data generation. Autonomous pathology systems capable of real-time tissue interpretation are also increasingly under development [50].
Wearable biosensors and continuous monitoring platforms may further support adaptive therapeutic strategies through integration of longitudinal physiological and molecular data streams. These multimodal ecosystems may eventually enable highly personalized oncology care [51].
14. Future Perspectives in AI-Driven Precision Oncology
Future precision oncology systems will likely involve highly integrated multimodal AI ecosystems combining pathology, radiology, genomics, transcriptomics, immunomics, and clinical language models [52].
Digital twins, adaptive therapy systems, and real-time monitoring platforms may eventually support continuously optimized personalized therapeutics. Advances in explainable AI, federated learning, and efficient transformer architectures are expected to further improve scalability and clinical adoption [53].
The multimodal learning frameworks described throughout Sections 5–13 are likely to become foundational components of next-generation oncology ecosystems capable of delivering real-time precision medicine [54].
15. Discussion
Foundation models are emerging as a major breakthrough in cancer medicine and precision oncology because they can process and integrate diverse biomedical data sources such as pathology images, radiology scans, genomic profiles, and clinical records. By learning from these large multimodal datasets, these models improve diagnostic precision, predict molecular alterations, identify biomarkers, support treatment selection, and enhance clinical decision-making. Their applications across digital pathology, immuno-oncology, radiogenomics, and natural language processing highlight their growing translational impact in oncology practice.
However, several challenges remain before widespread clinical adoption can occur. Issues related to model interpretability, patient privacy, data bias, and regulatory validation must be carefully addressed to ensure safe and equitable use in healthcare settings. Despite these limitations, ongoing developments in explainable AI, federated learning, and multimodal foundation models are expected to strengthen their reliability and clinical utility. In the future, foundation models may become essential tools in precision oncology by enabling more personalized, scalable, and biologically informed cancer care.
CONCLUSION
Foundation models represent a transformative advancement in cancer medicine and precision oncology. Their ability to integrate multimodal biomedical datasets has substantially improved diagnostic accuracy, molecular prediction, biomarker discovery, therapeutic stratification, and clinical decision support. Applications across digital pathology, radiology, genomics, immuno-oncology, and clinical language processing collectively demonstrate the immense translational potential of these systems [55].
Despite important limitations involving interpretability, privacy, algorithmic bias, and regulatory validation, foundation models are expected to become central components of future precision oncology ecosystems. Continued advances in multimodal learning, federated AI, explainability, and adaptive therapeutic modeling may ultimately redefine modern oncology by enabling scalable, personalized, and biologically informed cancer care.
REFERENCES

Dr. Benjamin Walker, Dr. Eleanor Hayes, Dr. Christopher Nolan, Foundation Models in Cancer Medicine: Revolutionizing Precision Diagnostics and Clinical Oncology, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6733-6744. https://doi.org/10.5281/zenodo.20391588
 10.5281/zenodo.20391588
10.5281/zenodo.20391588