
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
B Pharmacy Students Smt. Sharadhchandrika Suresh Patil College of Pharmacy, Chopda.
Dysmenorrhea is a common gynecological condition that significantly affects women's quality of life. Conventional treatments, such as hormone therapy and NSAIDs, are effective but have several side effects, thus safer alternatives are needed. The current study's objective was to develop and evaluate herbal transdermal patch that uses natural ingredients to alleviate menstrual pain. Zingiber officinale (ginger) and Curcuma longa (turmeric) plant extracts were combined with essential oils such as peppermint, fennel, clove, cinnamon, and eucalyptus via solvent casting in a polymeric matrix. The first assessment tests conducted on the manufactured formulations (F1–F3) included thickness, weight uniformity, folding durability, moisture content, moisture uptake, peel adhesion, shear adhesion, skin irritation, and stability research. The mechanical and physicochemical characteristics of every formulation were excellent. F3 performed comparatively better than the others. Studies on skin irritation showed that using the patches topically was safe. There were no in vivo or clinical investigations carried out; this study was restricted to laboratory-scale formulation and initial assessment. To determine the therapeutic efficacy of the proposed herbal transdermal patch for dysmenorrhea, additional research is needed, including in vitro drug release and clinical evaluation.
Dysmenorrhea is a common problem with menstruation that causes pain. It is one of the most common gynecological problems that affects women in their teens and early 20s. It has a big effect on daily life and activities. Dysmenorrhea is generally divided into two main types: primary and secondary. Primary dysmenorrhea manifests without any discernible pelvic pathology and is primarily linked to heightened prostaglandin production, resulting in intense uterine contractions, diminished uterine blood flow, and ischemic pain. Secondary dysmenorrhea, conversely, is linked to underlying conditions such as endometriosis, fibroids, or pelvic inflammatory diseases. [5] Epidemiology and signs dysmenorrhea affects lot of women all over the world. Between 30% and 90% of women have it, and about 10% to 20% of those women have very bad symptoms. People usually say the pain feels like cramps in the lower abdomen that can spread to the lower back and thighs. It often comes with other symptoms that affect the whole body, like nausea, vomiting, diarrhea, headaches, and dizziness. These symptoms can make people miss school or work and make them less productive. [7]
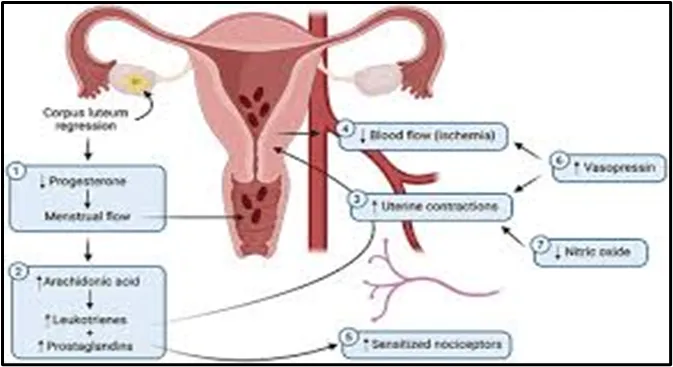
Figure no. 1: Mechanism of Dysmenorrhea
Conventional Treatment Approaches
Non-steroidal anti-inflammatory drugs (NSAIDs) are the first-line treatment for dysmenorrhea because they stop cyclooxygenase enzymes from working and lower the production of prostaglandins. NSAIDs can be helpful, but they can also cause problems like stomach irritation, headaches, and tiredness. Selective COX-2 inhibitors were made to reduce gastrointestinal side effects, but they might raise the risk of heart problems. Hormonal treatments, especially birth control pills, are also very common. Continuous regimens have proven to be more efficacious than cyclic regimens in alleviating menstrual pain. Levonorgestrel-releasing intrauterine devices offer similar alleviation. [5] For secondary dysmenorrhea, especially endometriosis, treatments like gonadotropin-releasing hormone agonists and oral progestins are used. However, these treatments may not work for everyone and can cause problems like bone density loss or irregular bleeding.
Along with NSAIDs and hormonal therapies, researchers have looked into a number of other drug options. Calcium channel blockers like nifedipine make the uterus contract less, while vasodilators like sildenafil and nitroglycerin make blood flow better and ease pain. Antispasmodic drugs like hyoscine and drotaverine work by relaxing smooth muscle. They have been helpful, especially when taken with NSAIDs. Researchers have also looked into vasopressin and oxytocin receptor antagonists, but the results are still not clear about how well they work. [7]
Herbal Medicine in Treatment
Herbal medicine is the use of plants to treat illnesses. It has been around for a long time. The World Health Organization says that herbal medicines are plant materials, extracts, and preparations that have active phytochemicals like alkaloids, flavonoids, tannins, and terpenoids. A large number of people around the world use herbal medicine because it is easy to find, cheap, and accepted by many cultures. People often think that herbal medicines are always safe, but this is not true. They can cause toxicity, allergic reactions, or interactions with regular medicines. Problems like lack of standardization, contamination, and differences in potency make them even less useful. [5]
Medicinal plants are really helpful when it comes to managing dysmenorrhea. Ginger is one of these plants. Ginger has things in it that can help with pain. For example ginger has something called gingerol. This gingerol stops some enzymes from working. As a result it helps reduce the amount of prostaglandin made by the body. This is good because it helps alleviate pain. Fennel is another plant that can help. Fennel has something called anethole. Anethole is good at helping muscles relax. Specifically it helps the muscles in the uterus relax. [6] Peppermint is also helpful. Peppermint has menthol in it. Menthol is good for reducing pain and helping muscles relax. Turmeric is another plant that's good for this. Turmeric has a lot of curcumin in it. Curcumin is really good at reducing inflammation and helping get rid of radicals. It does this by changing the way some signals are sent in the body. It also helps by reducing the amount of prostaglandin made. These plants like ginger and turmeric and peppermint and fennel all work, in ways. They can help reduce inflammation. They can help muscles relax. They can help get rid of radicals. They can also help with the way the body feels pain. [8]
Non-Pharmacological Therapies
There are some things that can help with dysmenorrhea that do not involve taking medicine. People have tried different things like using heat doing yoga getting exercise getting a massage and trying physiotherapy. Some people also try acupuncture and something called electrical nerve stimulation. Sometimes these things can help people feel better. We need to do more research to really know if they work. We need to do studies to see if these methods can really help with dysmenorrhea. [5]
Transdermal Drug Delivery System
Transdermal Drug Delivery Systems are a way to give people medicine. This way of giving medicine involves putting it through the skin and into the bloodstream at an steady pace. Transdermal Drug Delivery Systems have some things about them. They are better, than taking medicine by mouth or getting a shot. They help avoid problems that happen when the liver breaks down the medicine first. [9] They keep the amount of medicine in the body steady. They help the body use the medicine better. They make it easier for people to take their medicine. Transdermal Drug Delivery Systems have parts. These parts include a container that holds the medicine a thin layer that controls how fast the medicine comes out sticky things that help it stay on the skin special helpers that make the medicine go through the skin better and a strong layer that backs everything up. There are kinds of Transdermal Drug Delivery Systems. They can be classified based on how they're designed. The main kinds are Matrix-controlled systems, Membrane-controlled systems, Sandwich-type systems. [10]
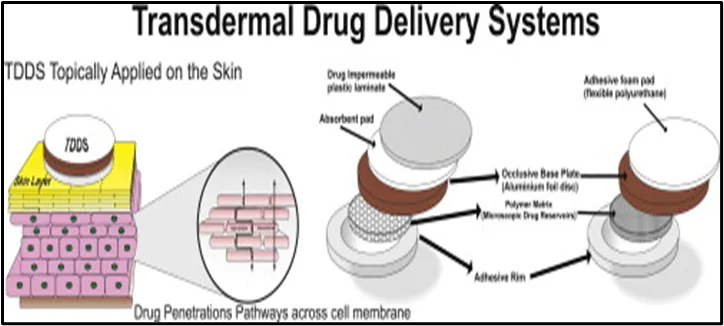
Figure no: 2 Transdermal Drug Delivery System
Even though Transdermal Drug Delivery Systems are helpful they are not perfect. Transdermal Drug Delivery Systems have some limitations. For example they cannot deliver molecules or molecules that have an electric charge. Transdermal Drug Delivery Systems also cannot hold a lot of medicine. Sometimes Transdermal Drug Delivery Systems can even irritate the skin.
FUTURE PROSPECTIVE
Dysmenorrhea is still a problem for many women. It affects their life. Now treatments like NSAIDs and hormonal therapies are commonly used. They have some limitations. So we need to look into options. [8] Herbal medicines and new ways of giving medicine like TDDS seem promising. We need more research to make sure they are safe and work well. We also need to make sure they are made in a way. Future studies should focus on doing clinical trials. They should also work on creating better formulations. [9] This will give us effective and easy-to-use treatment options, for dysmenorrhea. Effective treatment options will improve the lives of women with dysmenorrhea.
3. MATERIALS AND METHOD
A. COLLECTION OF PLANT MTERIALS
Dried rhizomes of Zingiber officinale (ginger) and Curcuma longa (turmeric) were used as the primary herbal drugs. Essential oils of Mentha piperita (peppermint oil), Foeniculum vulgare (fennel oil), Eucalyptus globulus (eucalyptus oil), Cinnamomum verum (cinnamon oil), and Syzygium aromaticum (clove oil) were obtained from institute lab. Polymers such as Hydroxypropyl Methylcellulose (HPMC) and Polyvinyl Alcohol (PVA), sodium alginate, glycerol, menthol and gum Arabic were used for patch preparation. Polyethylene glycol (PEG 400) was used as a plasticizer. All other chemicals and solvents and natural adhesive used were of analytical grade.
B. EXTRACTION
The dried rhizomes of Curcuma longa (turmeric) and Zingiber officinale (ginger) were cleaned, shade-dried, and ground into a coarse powder. Soxhlet extraction was performed on a known amount of each powdered medication individually. Each sample was extracted using around 250 milliliters of ethanol. The powdered material was put in a thimble and constantly extracted in a Soxhlet apparatus for six to seven hours, or until the colorless solvent in the siphon tube indicated exhaustive extraction. [11]
To get rid of insoluble material, the extracted materials were filtered. After that, a rotary evaporator was used to concentrate the filtrates under low pressure in order to eliminate superfluous solvent and produce a concentrated liquid extract. The extracts were utilized in their liquid state for the transdermal patch's subsequent preparation because they were not fully dried. Before being used, the produced extracts were refrigerated in sealed containers. [12]


C. PREPARATION OF HERBAL TRANSDERMAL PATCH
Using a magnetic stirrer and a hot plate, 30 mL of distilled water in a 100 mL beaker was heated gradually to 60–70°C to create a polymeric solution. Polyvinyl alcohol (PVA, 0.5 g) and hydroxypropyl methylcellulose (HPMC, 1.2 g) were gradually added while being continuously stirred until they were fully dissolved. After adding 0.2 g of sodium alginate and 0.1 g of gelatin to the mixture, stirring was continued until a clear, viscous polymeric solution was achieved. After being taken off the heat, the solution was let to cool to room temperature.
Plasticizers such as glycerol (1.0 mL), propylene glycol (1.5 g), and polyethylene glycol 400 (PEG 400, 0.3 mL) were added to the cooled polymeric solution. Until a smooth, uniform, and bubble-free blend was achieved, the mixture was constantly swirled.
Table no.1: Polymer Phase Ingredients & Quantity
|
Sr.no |
Ingredients |
Quantity |
|
1 |
Distilled water |
30ml |
|
2 |
HPMC |
2.5 g |
|
3 |
PVA |
1.5 g |
|
4 |
Gelatin |
0.75 g |
|
5 |
Sodium alginate |
0.3 g |
|
6 |
Glycerol |
1.0 ml |
|
7 |
PEG-400 |
1.0 ml |
Ginger extract (2-3 ml) and turmeric extract (2-3 ml) were placed in different beakers. In addition to camphor (0.05 g) and menthol (0.05 g), essential oils of clove, fennel, cinnamon, peppermint, and eucalyptus (2 drops each) were used. After adding about 20 milliliters of ethanol as a solvent, the mixture was gently swirled until all the ingredients were well combined.
Table no. 2: Herbal Ingredients & Quantity
|
Sr.no |
Ingredients |
Quantity |
|
1 |
Ethanol |
20 ml |
|
2 |
Ginger extract |
2-3 ml |
|
3 |
Turmeric extract |
2-3 ml |
|
4 |
Essential oils |
2 drops each |
|
5 |
Menthol |
0.05 g |
|
6 |
Camphor |
0.05 g |
The polymer-plasticizer mixture was continuously stirred while the prepared herbal extract phase was gradually added. To create a homogeneous, viscous, and bubble-free gel, the mixed mixture was agitated for 15 to 20 minutes at a low pace. After that, the mixture was left to stand for about ten minutes in order to release any trapped air bubbles. About 15 to 20 milliliters of the prepared mixture were evenly put into a clean, dry glass Petri dish with a diameter of 9 centimeters. [14]
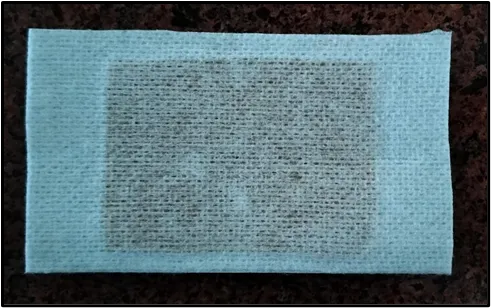
To avoid contamination, the dish was covered and left to dry for 24 to 48 hours at room temperature (25 to 30°C) or, alternatively, for 5 to 6 hours at 40°C in a hot air oven until a flexible film formed. After the film had dried, it was gently peeled off and trimmed to the appropriate size. The created patches were kept between butter sheets or in airtight containers to avoid absorbing moisture after being assessed for physical attributes such smoothness, flexibility, and transparency. [16]
The produced transdermal films were placed onto a non-woven adhesive backing layer (Rilekh Non-Woven Underwrap Adhesive Bandage) following drying and cutting. The backing layer gave the patch flexibility and mechanical support. To guarantee consistent adhesion without air entrapment, the film was carefully positioned onto the backing material's adhesive surface and gently pushed. To create patches of consistent size, the surplus edges were cut. The patch's exposed surface was then covered with a protective release liner (butter paper or the original liner of the adhesive material) to avoid contamination and sticking while being stored. After preparation, the patches were sealed in airtight containers and kept in a desiccator until further assessment. [15]
4. EVALUATION OF TRANDERMAL PATCH
A digital micrometer was used to measure the manufactured transdermal patches' thickness at various spots. To make sure the produced films were uniform, the average thickness and standard deviation were computed. This test assisted in verifying uniform medication distribution and consistency in film formation. [10]
Each patch was divided into distinct sections, each of which was weighed separately using a digital balance. To assess the uniform distribution of formulation components inside the films, the average weight and standard deviation were computed. [15]
A strip of the patch was repeatedly folded at the same position until it broke. The number of folds required to break the patch was recorded as the folding endurance, indicating the flexibility and mechanical strength of the film. [16]
The produced patches were weighed separately and stored at room temperature for a full day in a desiccator filled with fused calcium chloride. The patches were weighed again after the allotted period, and the following calculation was used to determine the percentage moisture content: The percentage of moisture content is equal to (final weight - initial weight) x100. This test revealed how much moisture was in the films.[10]
To maintain relative humidity, the patches were weighed and put in a desiccator with a saturated potassium chloride solution. The patches were weighed again after a day, and the following formula was used to determine the percentage moisture uptake: Moisture % Moisture Uptake = (Final weight – Initial weight / Initial weight) × 100. This study helped to evaluate the hygroscopic nature of the films. [15]
To guarantee consistent extraction of active ingredients, a small known portion of the patch was dissolved in an appropriate solvent and well mixed. A visual inspection of the solution revealed that the herbal extracts were distributed evenly throughout the patch. [15]
The lengths of three strips that were cut from various parts of the patch were measured. The homogeneity of flatness was assessed by observing the fluctuation in length. A consistent length demonstrated the patch's 100% flatness. [10]
The purpose of the skin irritation study was to assess the manufactured transdermal patches' safety. After applying the patch to a clean, intact skin surface, the area was checked for redness, itching, swelling, or irritation after a certain amount of time. If there was no obvious skin irritation or discomfort, the composition was deemed safe. [15]
For a predetermined amount of time, the manufactured transdermal patches were kept at both room temperature and a little higher temperature. Patches were frequently assessed for stickiness, color change, flexibility, and physical appearance throughout the trial. If there were no noticeable changes during the storage term, the formulation was deemed stable. (General standard procedure).
The force needed to remove the patch from a surface was ascertained using the peel adhesion test. After applying the patch on an appropriate substrate, it was peeled off at a consistent angle. The patch's adhesive strength was assessed by how easy or difficult it was to remove. A balanced adhesion was required to ensure proper sticking without causing discomfort during removal. [10]
The cohesive strength of the glue was assessed using the shear adhesion test. In order to generate a pulling force parallel to the surface, the patch was placed on it together with a tiny weight. It was noted how long it took for the patch to separate from the surface. Better adhesive strength of the formulation was demonstrated by a longer time. [15]
5. RESULTS
|
Sr. no |
Evaluation parameters |
F1 |
F2 |
F3 |
|
1 |
Appearance |
Smooth, uniform |
Smooth, uniform |
Smooth, uniform |
|
2 |
Color |
Light yellowish |
Slightly brownish |
Yellow-brown |
|
3 |
Texture |
Flexible |
Flexible |
Slightly thick |
|
4 |
Thickness (mm) |
0.21± 0.02 |
0.24 ± 0.01 |
0.27 ± 0.02 |
|
5 |
Weight uniformity (mg) |
112 ± 3 |
118 ± 4 |
125 ± 5 |
|
6 |
Folding endurance |
180 ± 5 |
195 ± 6 |
210 ± 8 |
|
7 |
Moisture content (%) |
4.2 ± 0.3 |
4.8 ± 0.2 |
5.1 ± 0.4 |
|
8 |
Moisture uptake (%) |
6.5 ± 0.4 |
7.2 ± 0.5 |
7.8 ± 0.3 |
|
9 |
Peel adhesion |
Moderate |
Good |
Good |
|
10 |
Shear adhesion (sec) |
120 ± 10 |
145 ± 12 |
160 ± 15 |
|
11 |
Skin irritability |
No irritation |
No irritation |
No irritation |
|
12 |
Stability (visual) |
Stable |
Stable |
Stable |

DISCUSSION
The solvent casting process was effectively used to produce the herbal transdermal patches (F1–F3), which had good physical properties like a smooth surface, uniform thickness, and flexibility. The distribution of the polymers caused slight changes in weight and thickness. The patches showed strong mechanical strength and satisfactory folding endurance.
The films appeared to be stable because the moisture content and absorption were within permissible bounds. Adequate adhesive qualities for skin application were verified by peel and shear adhesion tests. Studies on skin irritation revealed that the patches were non-irritating and harmless. Out of all of them, F3 shown generally superior qualities. Nevertheless, the study scope was restricted to initial assessment; more in vitro and clinical research is needed to verify efficacy.
CONCLUSION
The current work used the solvent casting process to successfully create herbal transdermal patches with essential oils and extracts of ginger and turmeric. Preliminary metrics including thickness, weight uniformity, folding endurance, moisture content, peel adhesion, shear adhesion, skin irritation, and stability were used to evaluate the formulations (F1–F3), and all of them shown satisfactory results for transdermal application. This work was restricted to laboratory-scale formulation and preliminary testing, hence no in vivo nor clinical evaluation was carried out. F3 outperformed the other formulas in terms of overall performance. To confirm the safety and therapeutic efficacy of the created patch in the treatment of dysmenorrhea, more research is needed, including in vitro drug release and clinical evaluation.
REFERENCES

Rajnandini Patil, Pooja Patil, Bhuvaneshwari Patil, Design Of Plant Based Transdermal Patch for The Relief of Dysmenorrhea, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6682-6691, https://doi.org/10.5281/zenodo.20391275
 10.5281/zenodo.20391275
10.5281/zenodo.20391275