Matoshri College of Pharmacy, Ekhlahare, Nashik, Maharashtra, India 422105
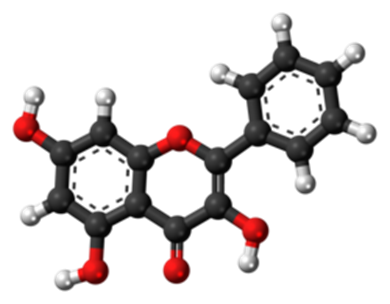
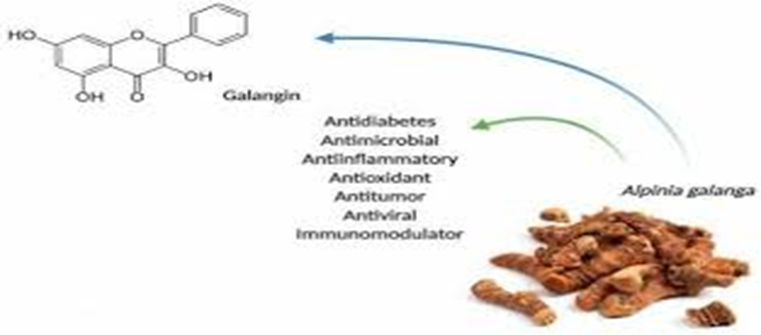
Galangin (3,5,7-trihydroxyflavone) is a naturally occurring flavonoid predominant in plants such as Alpinia officinarum (lesser galangal), galangal rhizomes and propolis. Its broad pharmacological profile includes antioxidant, anti-inflammatory, antimicrobial, anti-fibrotic, and cell-modulatory effects. Although most research has focused on cancer, cardiovascular, and fibrotic diseases, emerging evidence suggests potential roles for galangin in wound healing and dermal repair processes. However, critical challenges such as poor solubility, low bioavailability, rapid metabolism, and limited clinical translation have impeded its therapeutic development. Advanced delivery systems — including hydrogels, nanoparticles, and biopolymer carriers — provide promising strategies to overcome these limitations. This review synthesizes the current evidence on galangin’s pharmacology in wound healing, discusses mechanistic pathways, highlights challenges for clinical application, and explores advanced delivery platforms designed to enhance its therapeutic potential.Wound healing is a highly coordinated biological process involving inflammation, cell migration, angiogenesis, extracellular matrix deposition, and tissue remodeling. Impairment in any of these phases can lead to chronic, non-healing wounds, representing a significant clinical challenge. Galangin (3,5,7-trihydroxyflavone), a naturally occurring flavonoid found in Alpinia officinarum, propolis, and related plant sources, has attracted increasing attention due to its diverse pharmacological activities. Galangin exhibits potent anti-inflammatory, antioxidant, antimicrobial, and anti-fibrotic properties, which are highly relevant to key stages of wound repair. Experimental studies suggest that galangin can modulate inflammatory mediators, regulate fibroblast migration and proliferation, suppress excessive collagen deposition through the TGF-?/Smad signaling pathway, and reduce oxidative stress, thereby promoting more effective wound healing. Despite these promising effects, the therapeutic application of galangin is limited by poor aqueous solubility, low bioavailability, rapid metabolism, and insufficient in vivo and clinical evidence.
Wound healing is a complex, multi-step physiological process involving inflammation, cell migration, angiogenesis, collagen deposition, and remodeling. Chronic wounds — including diabetic foot ulcers, venous leg ulcers, and pressure sores — present a major clinical burden due to impaired healing and infection. Natural products, particularly flavonoids such as quercetin, naringenin, and galangin, have attracted interest due to their multifaceted bioactivities that may positively influence key pathways in wound repair. Flavonoids can modulate inflammation, oxidative stress, fibroblast proliferation, extracellular matrix remodeling, and microbial growth — all of which are crucial determinants in healing outcomes.
TYPES OF WOUNDS
Wounds can be categorized into various types based on their cause, depth, and characteristics. Wounds can be categorized in following types:
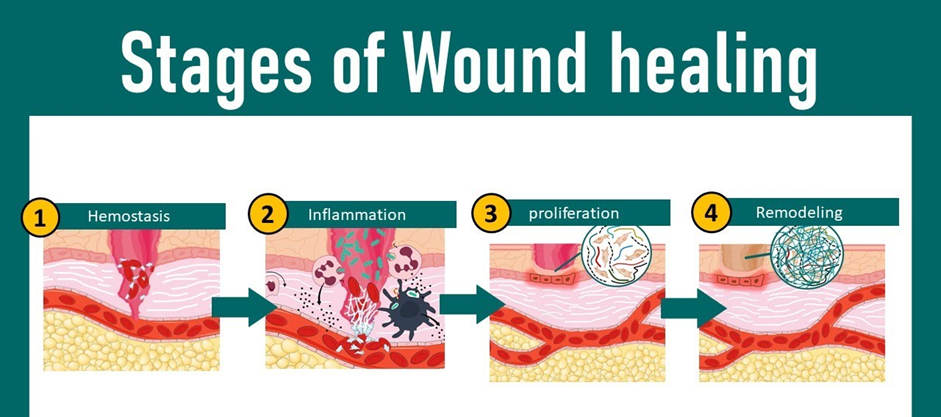
WOUND HEALING PROCESS:-
Wound healing is a complex biological process that involves several distinct but overlapping stages. These stages include hemostasis, inflammation, proliferation, and remodeling. There are the steps of wound healing:
ADVANCE MEDICATION THERAPY INVOLVED IN WOUND HEALING
Growth Factors:- Platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and epidermal growth factor (EGF) are commonly used growth factors in wound healing(4). Antimicrobial Agents: Silver-based dressings, antimicrobial peptides, and nanoparticles are among the advanced antimicrobial agents used in wound care.
Anti-inflammatory Drugs:- Corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), and cytokine inhibitors are advanced antiinflammatory drugs used to modulate the inflammatory response in wound healing.
Extracellular Matrix (ECM) Modulators:- Collagen-based dressings, hyaluronic acid derivatives, and extracellular matrix scaffolds are advanced ECM modulators used to facilitate tissue remodeling and regeneration.
Stem Cell Therapies: Mesenchymal stem cells (MSCs), adipose-derived stem cells (ASCs), and induced pluripotent stem cells (iPSCs) are being investigated for their potential to promote tissue regeneration in wound healing.
Gene Therapy: Gene-based approaches, such as the delivery of growth factors and cytokines, hold promise for enhancing wound healing by promoting angiogenesis and tissue regeneration.
Bioactive Dressings: Bioactive dressings containing growth factors, antimicrobial agents, and extracellular matrix components provide sustained release and localized delivery of therapeutic molecules to the wound site.
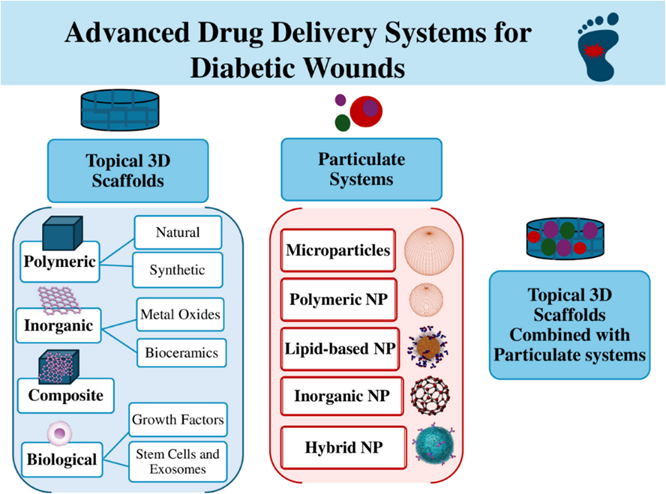
ADVANCE DRUG DELIVERY SYSTEM
Advanced drug delivery systems for wound healing have emerged as a promising approach to improve the efficacy of wound care treatments. These systems aim to optimize the delivery of therapeutic agents to the wound site, enhancing their bioavailability, and promoting faster and more efficient healing. There are some notable advanced drug delivery systems for wound healing:
Hydrogels: Hydrogels are highly hydrated polymeric networks that can retain large amounts of water. They are attractive for wound healing applications due to their ability to provide a moist environment conducive to wound healing. Hydrogels can be loaded with therapeutic agents such as growth factors, antimicrobial agents, and anti-inflammatory drugs, which are released slowly over time to the wound site.
Nanoparticles:- Nanoparticles offer unique advantages for drug delivery, including high drug loading capacity, sustained release profiles, and the ability to target specific cells or tissues. Various types of nanoparticles, such as liposomes, polymeric nanoparticles, and dendrimers, have been investigated for wound healing applications. These nanoparticles can encapsulate therapeutic agents and protect them from degradation, enabling controlled release at the wound site.
Microneedle patches:- Microneedle patches consist of arrays of micron-scale needles that penetrate the skin's outer layer, facilitating the delivery of drugs into the underlying tissue. These patches can be loaded with various therapeutic agents, including growth factors, antibiotics, and anti-inflammatory drugs, and applied directly to the wound site for targeted delivery and enhanced efficacy.
Electrospun nanofibers:- Electrospun nanofibers are produced by electrospinning polymer solutions into nanoscale fibers, which can mimic the extracellular matrix structure of natural tissues. These nanofibers can be loaded with therapeutic agents and fabricated into wound dressings, providing sustained release of drugs and promoting cell proliferation and tissue regeneration.
3D printed scaffolds: 3D printing technology enables the fabrication of customized scaffolds with precise control over their architecture and porosity. These scaffolds can be loaded with therapeutic agents and implanted at the wound site to provide structural support, promote cell attachment and proliferation, and facilitate controlled drug release for enhanced wound healing.
MARKETED FORMULATION USED AS ADVANCED DRUG DELIVERY SYSTEM FOR THE TREATMENT OF WOUND HEALING
Advanced drug delivery systems hold great promise for improving the treatment outcomes of various types of wounds, including acute and chronic wounds, burns, and ulcers, by enhancing the delivery and efficacy of therapeutic agents at the wound site. Several advanced drug delivery systems and marketed products are utilized in the treatment of wound healing:
Ag Hydro fiber Dressing:- Ag is a sterile, nonwoven dressing composed of sodium carboxymethylcellulose and ionic silver. It forms a soft gel when in contact with wound exudate, providing a moist wound healing environment. while delivering antimicrobial benefits due to the presence of silver ions. This dressing is effective for managing wounds with high levels of exudate and controlling infection.
Hydro-Alginate Antimicrobial Dressing:- Ag is a sterile, non-woven dressing composed of alginate fibers and silver ions. It absorbs exudate from the wound while providing sustained antimicrobial activity against a broad spectrum of pathogens. The combination of alginate and silver facilitates autolytic debridement and promotes granulation tissue formation.
Antimicrobial Activated Charcoal Dressing:- Silver 220 is an activated charcoal dressing containing silver ions. It absorbs Odor and exudate from the wound while providing broad-spectrum antimicrobial activity. The activated charcoal component helps manage malodor associated with infected wounds.
Dermal Regeneration Template:- It is a bilayer membrane system consisting of a porous matrix of bovine collagen and glycosaminoglycan (GAG) and a semipermeable silicone outer layer. It serves as a dermal substitute for full-thickness wounds, promoting vascularization and cellular infiltration. It is commonly used in the treatment of burn injuries and complex wounds requiring soft tissue reconstruction.
SOME HERBAL APPROACHESUSED AS ADVANCED DRUG DELIVERY SYSTEM FOR THE TREATMENT OF WOUND HEALING
Turmeric (Curcuma longa) Loaded Nanoparticles:- Turmeric, containing curcumin as its active ingredient, has been traditionally used for wound healing due to its anti-inflammatory and antioxidant properties. Incorporating curcumin into nanoparticles enhances its stability and bioavailability, enabling controlled release at the wound site.
Aloe vera Loaded Hydrogels:- Aloe vera is known for its wound healing properties attributed to its anti-inflammatory and antimicrobial effects. Incorporating Aloe vera extract into hydrogel formulations provides a moist wound environment and sustained release of bioactive compounds, promoting tissue regeneration.
Honey-based Nanofiber Scaffolds:- Honey has been used for wound healing for centuries due to its antimicrobial and anti-inflammatory properties. Fabricating honey into nanofiber scaffolds enhances its application to wounds, providing sustained release and improved efficacy.
Neem (Azadirachta indica) Oil-loaded Liposomes:- Neem oil possesses antimicrobial and anti-inflammatory properties beneficial for wound healing. Encapsulating neem oil in liposomes improves its stability and enhances its penetration into the skin, facilitating wound closure and tissue regeneration.
Pharmacology of Galangin in Wound Healing
Galangin accelerates the wound healing process by modulating several biochemical pathways across the phases of tissue repair (hemostasis, inflammation, proliferation, and remodeling).
This review explores the therapeutic potential of Galangin ($3,5,7$-trihydroxyflavone), a natural flavonol primarily derived from Alpinia galanga (galangal) and propolis, in the context of cutaneous wound healing. While galangin exhibits potent pharmacological properties, its clinical application is hindered by poor solubility and bioavailability, necessitating the development of advanced delivery systems.
1. Pharmacology of Galangin in Wound Healing
Galangin accelerates the wound healing process by modulating several biochemical pathways across the phases of tissue repair (hemostasis, inflammation, proliferation, and remodeling).
Challenges in Therapeutic Application
Despite its efficacy in in vitro models, galangin faces several hurdles for human clinical use:
|
Challenge |
Description |
|
Low Solubility |
Galangin is highly hydrophobic, making it difficult to incorporate into traditional water-based topical gels or creams. |
|
Poor Bioavailability |
Rapid metabolism and low skin penetration limit the amount of active compound that reaches the deeper dermal layers. |
|
Stability Issues |
It is sensitive to environmental factors such as light, temperature, and pH, which can degrade the molecule before it exerts its effect. |
|
Rapid Washout |
When applied as a simple solution or powder, it is easily removed by wound exudate, requiring frequent reapplication. |
Advanced Delivery Systems
To overcome these challenges, researchers are utilizing nanotechnology and biomaterials to enhance galangin's delivery to the wound site.
Nano-Carrier Systems
Scaffolds and Hydrogels
Pharmacology: How Galangin Heals
Galangin acts as a "biological orchestrator" that accelerates the body's natural repair mechanisms through several distinct pathways:
Clinical Challenges: The Solubility Barrier
Despite its high efficacy in laboratory tests, Galangin faces three primary "bottlenecks" that hinder its use as a standard medical treatment:
3. Advanced Delivery Systems
To solve these problems, researchers are using Nanotechnology to "wrap" Galangin in protective carriers:
|
Delivery System |
Mechanism of Action |
Benefit |
|
Nanofibrous Scaffolds |
Mimics the skin's physical structure. |
Provides a "home" for cells to grow while releasing drug slowly. |
|
Liposomes/ Niosomes |
Fatty "bubbles" that carry the drug. |
Penetrates the skin's lipid barrier more effectively. |
|
Hydrogel Nanocomposites |
Smart gels that respond to pH or heat. |
Releases Galangin only when the wound is inflamed or infected. |
|
Gold Nanoparticles |
Metallic carriers conjugated with Galangin. |
Enhances antimicrobial action and improves targeted delivery. |
Pharmacological Mechanisms in Wound Healing
Galangin accelerates tissue repair by orchestrating cellular responses across the four stages of wound healing (Hemostasis, Inflammation, Proliferation, and Remodeling).
A. Anti-inflammatory & Immunomodulatory Activity1
Chronic wounds often stall in the inflammatory phase.2 Galangin effectively "unlocks" this stage by:
B. Oxidative Stress Mitigation
Excessive ROS (Reactive Oxygen Species) destroys healthy tissue. Galangin acts as a "bio-shield" through:
C. Angiogenesis and Tissue Regeneration
D. Remodeling & Anti-Scarring
Key Challenges in Therapeutic Application
Despite its benefits, Galangin’s "natural" form presents significant hurdles for clinical use:
|
Barrier |
Impact on Wound Healing |
|
Hydrophobicity |
Virtually insoluble in water; difficult to formulate into standard gels. |
|
Poor Bioavailability |
Rapidly metabolized and poorly absorbed through the thick skin barrier. |
|
Stability Issues |
Highly sensitive to light and pH; degrades quickly in the alkaline environment of chronic wounds. |
|
Washout Effect |
Free Galangin is quickly diluted or removed by wound exudate (fluid). |
3. Advanced Delivery Systems (The "Solution")
To bridge the gap between lab and clinic, researchers are using Nano-Medicine to deliver Galangin effectively:
CONCLUSION
In summary, the transition of Galangin ($3,5,7$-trihydroxyflavone) from a traditional herbal constituent to a sophisticated therapeutic agent represents a significant advancement in the field of regenerative medicine. This review has delineated the multifaceted role of Galangin in wound healing, underscoring its ability to modulate the complex biochemical environment of injured tissue through a synergy of pharmacological actions, while also addressing the technological hurdles that have historically limited its clinical utility.
Pharmacological Integration
The pharmacological profile of Galangin is remarkably comprehensive, addressing the primary barriers to successful tissue repair. Its ability to act as a potent anti-inflammatory agent via the inhibition of the NF-1$\kappa$B and MAPK pathways is critical in preventing the chronicity of wounds.2 Furthermore, its role in oxidative stress management through the Nrf2/HO-1 axis provides a "bio-shield" for migrating fibroblasts and keratinocytes. Perhaps most importantly, Galangin’s influence on angiogenesis and the regulation of Matrix Metalloproteinases (MMPs) ensures that the remodeling phase results in functional tissue rather than pathological fibrosis. This multi-target approach makes it superior to single-target synthetic drugs that often fail to address the holistic complexity of the wound bed.
Addressing the Bioavailability Gap
Despite these benefits, the "Galangin Paradox"—the gap between its high in vitro efficacy and poor in vivo performance—remains the central challenge. The molecule’s inherent hydrophobicity, low aqueous solubility, and susceptibility to rapid metabolic degradation necessitate a departure from conventional topical formulations. Simple ointments and creams are insufficient to maintain the sustained therapeutic concentrations required for deep-tissue repair, particularly in the presence of wound exudates that can easily wash away free active compounds.
The Future of Advanced Delivery
The emergence of advanced delivery systems marks the "enabling" phase of Galangin research. The integration of nanotechnology, including liposomes, polymeric nanoparticles, and electrospun scaffolds, has successfully transformed Galangin into a viable clinical candidate. These systems do more than just deliver the drug; they protect the molecule from environmental degradation, enhance its penetration through the skin barrier, and provide a sustained-release profile that reduces the need for frequent dressing changes. The development of "smart" hydrogels, which can release Galangin in response to specific wound triggers such as pH shifts or bacterial enzymes, represents the next frontier in personalized wound management.
Final Verdict
In conclusion, Galangin stands as a promising "all-in-one" natural therapeutic for the treatment of acute and chronic wounds, including diabetic ulcers and severe burns. While the laboratory evidence is robust, the future of Galangin-based therapy depends on the successful translation of these advanced delivery platforms into human clinical trials. By bridging the gap between ancient pharmacology and modern material science, Galangin-loaded biomaterials are poised to become a cornerstone in the next generation of wound-care products, offering a cost-effective, natural, and highly efficient solution for global healthcare challenges.
REFERENCES

Pushkar Zambre, Nishigandha Dhokale, Galangin as a Therapeutic Agent for Wound Healing: Pharmacology, Challenges, and Advanced Delivery Systems, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1717-1728. https://doi.org/10.5281/zenodo.18280445
 10.5281/zenodo.18280445
10.5281/zenodo.18280445
