Rungta institute of Pharmaceutical Sciences and Research, Kohka, Kurud, Bhilai.
One of the most common chronic liver disorders worldwide, non-alcoholic fatty liver disease (NAFLD), is strongly linked to metabolic diseases such type 2 diabetes, obesity, insulin resistance, and dyslipidaemia. It is characterised by an excessive buildup of fat in hepatocytes in people who drink very little or nothing. Cirrhosis, fibrosis, simple steatosis, and nonalcoholic steatohepatitis (NASH) are some of the phases of the disease's evolution that might eventually result in hepatocellular cancer or liver failure. The primary care approach for NAFLD is still lifestyle modification because there isn't yet a single authorised pharmaceutical medication. There is growing interest in studying both conventional and herbal medicinal treatments to treat and prevent this illness.Using medicinal plants including Curcuma longa, Cuminum cyminum, Foeniculum vulgare, Trachyspermum ammi, Phyllanthus emblica, and Piper nigrum, the current work focuses on creating a polyherbal juice composition based on Ayurvedic principles. Numerous bioactive phytoconstituents, such as flavonoids, phenolic compounds, alkaloids, terpenoids, tannins, and essential oils, are known to be present in these plants. These components have important pharmacological actions, including hepatoprotective, antioxidant, anti-inflammatory, hypolipidemic, and digestive stimulating qualities, which may help lower the inflammation, oxidative stress, and lipid buildup linked to NAFLD.To maximize the phytochemical yield, the herbal components were extracted utilizing appropriate techniques such decoction and maceration. To find significant bioactive components in the extracts, preliminary phytochemical screening was done. To guarantee the quality, safety, and stability of the polyherbal juice formulation, preformulation investigations such as physicochemical evaluation, solubility analysis, viscosity determination, stability testing, and microbiological studies were carried out.The study emphasizes the possibility of polyherbal formulations as an all-natural and effective treatment strategy for NAFLD management. To confirm the new formulation's effectiveness, safety, and treatment mechanisms, more experimental and.clinical research is necessary
With an estimated 30% incidence globally, The most frequent cause of chronic liver disease is non-alcoholic fatty liver disease (NAFLD) [1]. Latin America had the highest reported prevalence of NAFLD (44.4%) in 2023, whereas South Asia had a frequency of 33.8% (22.9%–46.8%) [2]. The range of conditions known as NAFLD include all disease grades and stages. NAFLD is defined as ≥ 5% of the hepatocytes exhibiting macrovesicular steatosis in individuals who consume little to no alcohol (defined as <20 g/d for women and <30 g/d for men) without a readily identifiable alternative cause of steatosis, such as medication, starvation, or monogenic disorders [3].
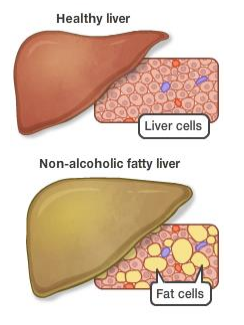
Three stages can be distinguished in the progression of NAFLD: Non-alcoholic steatohepatitis (NASH), which is characterised by inflammation and liver cell injury (ballooning); cirrhosis, the most severe stage, which is characterised by liver scarring and potential liver failure; and non-alcoholic fatty liver (NAFL), which involves fat accumulation and mild inflammation but no liver cell injury [4]. According to recent studies, the development of NAFLD is associated with lipid accumulation, oxidative stress, endoplasmic reticulum stress, and lipotoxicity [5].A chronic liver illness brought on by substances other than alcohol is referred to as non-alcoholic fatty liver disease (NAFLD). Steatosis, or excessive fat deposition in the hepatocytes, is one of its defining characteristics [8]. Non-alcoholic fatty liver (NAFL), which is characterized by benign liver cell steatosis, nonalcoholic steatohepatitis (NASH), and varying degrees of fibrosis upon liver biopsy are among the pathological processes associated with NAFLD [9]. Clinically, NAFLD is also linked to hepatocarcinoma and liver cirrhosis (Figure 1) [10].
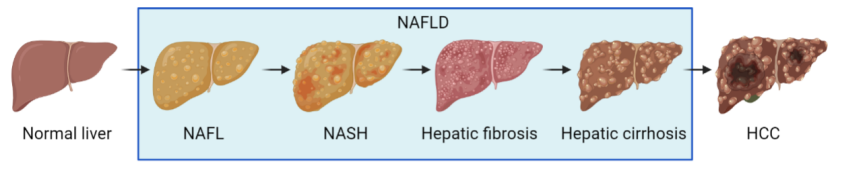
Fig : 2 Diagramatic Representation of NAFLD Progression.
The development of NAFLD can pose significant difficulties. It has also been noted that some individuals with NAFLD may experience symptoms including weakness, fatigue, nausea, and pain in the upper right abdomen. Consequently, this condition is often diagnosed through ultrasound examinations or tests that show elevated liver enzymes in many of these patients. Additionally, more advanced stages of the disease can lead to further health complications such as an enlarged spleen, yellowing of the skin and eyes, and fluid accumulation in the abdomen. Non-alcoholic fatty liver disease (NAFLD) poses both diagnostic and treatment challenges for medical professionals. Currently, there is no officially approved treatment specifically targeting NAFLD. Therefore, lifestyle modifications, especially regarding diet and physical activity, remain the primary strategy for managing the condition. These treatment methods mainly aim at reducing body weight and associated metabolic problems. There is a dose-dependent relationship observed in physical activity concerning NAFLD, with vigorous exercise being significantly more beneficial than moderate exercise. A calorie-restricted diet that is low in carbohydrates and saturated fats, while being rich in fiber and unsaturated fats, such as the Mediterranean diet, is recommended.
The use of herbal medicines in the treatment of nonalcoholic fatty liver disease (NAFLD) has been the focus of considerable research in recent decades due to their potential therapeutic mechanisms, convenience of use, and absence of adverse effects. Herbal remedies have beneficial effects on the onset and progression of NAFLD, according to preclinical and clinical study [6]. The safety and effectiveness of traditional Chinese medicine for non-alcoholic fatty liver disease have shown encouraging results in randomized controlled trials [7].
Ayurvedic Medicine:
Ayurveda is one of the traditional medicinal systems with an established history of many centuries. Furthermore known as Ayurvedic Medicine, this ancient Vedic knowledge is considered to be one of the oldest healing sciences and has survived until the present generation over many centuries of tradition. Originated in India thousands of years ago, The Sanskrit terms ayur (life) and veda (science or knowledge) are combined to form Ayurveda, which is referred to as the "Mother of All Healing" [20]. This means "the science of life," emphasizing the restoration of harmony and balance in the mind, body, and spirit.[21]

Fig:3 Ayurvedic Medicine
Polyherbal Formulation :
Ayurvedic drug formulation is predicated on two ideas: both single-drug usage and multiple-drug use, the latter of which is referred to as PHF. This important traditional therapeutic herbal approach, also referred to as polypharmacy or polyherbalism, takes use of mixing multiple medicinal herbs to obtain additional therapeutic effectiveness. The Ayurvedic text "Sarangdhar Samhita," which dates back to 1300 A.D., has historically emphasized the idea of polyherbalism in this antiquated medical system.[15] Plant formulations and mixed plant extracts are preferred above single plant extracts in the traditional Indian medical system. Ayurvedic herbal remedies are known to be made in a variety of dose forms, the majority of which are PHF.[16,17] Research has shown that the combination of various plants of different potencies may, in theory, yield a better outcome than either the use of the plant alone or the total of its separate effects. Synergism is the term for this favorable herb-herb interaction phenomena. When combined with other plants, several of the active ingredients in herbal remedies have significant pharmacological effects that are not apparent when taken by themselves.[18]


Fig:4 polyherbal formulation
Because of synergism, polyherbalism provides some benefits not available with a single herbal combination. It is evident that a single multi-constituent formulation can have a more effective therapeutic effect. A lower dosage of the herbal substance would be needed to produce the intended pharmacological action, reducing the likelihood of negative side effects. Additionally, PHFs increase patient convenience and indirectly increase compliance and therapeutic impact by eliminating the need for patients to take several single herbal formulations at once. All of these benefits have helped PHF become more well-known in the market when compared to a single herbal composition.[19].
HERBAL JUICE :
Many people in Asia, Europe, and America rely heavily on herbal juice in their daily lives due to its cultural significance, health advantages, and delicious flavors. These juices can be classified and identified based on their preparation methods and the specific plant components they include. In this context, herbal infusions are vital in traditional medicine, where edible plant parts with healing properties have been used as remedies for a long time. Moreover, they have gained popularity among health-conscious individuals.[22]

Fig:4 Herbal juice
Plant Details:
CURCUMA LONGA L.
The rhizome of turmeric (Curcuma longa) contains active ingredients known as curcuminoids, the most well-known of which is curcumin. Curcumin is recognized as a potent anti-inflammatory and antioxidant [23]. Among NAFLD patients, curcumin supplementation dramatically lowered total cholesterol, low-density lipoprotein, and liver enzymes [24].The impact of curcumin on the liver's ultrasonography morphological features in NAFLD patients has not yet been reviewed. Curcumin supplementation may be a useful adjuvant therapy for the treatment of mild to moderate NAFLD if it can be demonstrated to improve liver ultrasonography morphological parameters such as NAFLD severity and promote liver steatosis resolution [25].
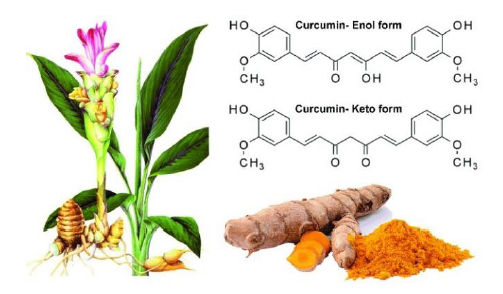
Fig:5 Curcuma Longa
According to liver ultrasonography results, curcumin decreased blood liver enzymes, lowered the severity of NAFLD, and promoted the resolution of liver steatosis. Curcumin has anti-oxidant and anti-inflammatory properties because it suppressed nuclear factor-Kβ and decreased oxidative stress and inflammation.[26] Given that oxidative stress has been linked to the pathophysiology of NAFLD, this discovery suggests that curcumin may be able to protect the liver by reducing oxidative stress.[27] A study that demonstrated curcumin enhanced the antioxidant defense system and reduced the level of lipid peroxidation highlighted this theory.[28] Additionally, curcumin's lipid-lowering ability decreased total cholesterol via influencing the expression of several genes, including lipoprotein lipase, cholesteryl ester transfer protein, and peroxisome proliferator-activated receptor alpha (PPAR-α).[29] By preventing the production of lipogenic genes, curcumin supplementation contributed to the reduction of plasma triglyceride and cholesterol levels. By reducing the amount of fat in the liver, this lessened the severity of NALFD [30].When compared to the placebo group, curcumin lowers serum liver enzymes and total cholesterol in trials lasting eight weeks or longer. Triglycerides were lowered after using curcumin supplements for longer than eight weeks.[31].
Taxononical Classification:[32,33,34]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Kingdom |
Plantae |
|
2 |
Subkingdom |
Tracheobionta |
|
3 |
Superdivision |
Spermatophyta |
|
4 |
Division |
Magnoliophyta |
|
5 |
Subclass: |
Zingiberidae |
|
6 |
Order |
Zingiberales |
|
7 |
Family |
Zingiberaceae |
|
8 |
Genus |
Curcuma |
|
9 |
Species |
Longa |
|
10 |
Scientific name |
Curcuma longa |
Components of phytochemicals:
1. 10-diene-9-one; 4-methoxy-5-hydroxybiosabola; 4-hydroxy-cinnamoyl-(Feruloyl)-methane; Alpha-atlantone; Alpha-pinene; Alphaterpineol; Ar-turmerone; Arabinose.
2. Azulene, ascorbic acid, ash, bis-(para-hydroxy-cinnamoyl)-methane, beta-carotene, beta-pinene, and beta-sesquiphellandrene.
3. Bis-desmethoxycurcumin, Bisabolene, Bixin, Borneol, Boron, Calcium, Caprylic acid, Caryophyllene, Chromium, Cineole, Cinnamic acid, Cuminyl alcohol, Curcumene, Curcumenol, Curcumin, Curdione, Cobalt, and Copper.
4. Gamma-atlantone, eucalyptol, eugenol, epiprocurcumenol, feruloyl-p-coumaroyl-methane, germacrone, germacrone-13-al, guaiacol, isoborneol, and L-alpha-curcumene [32,33,34]
Pharmacological Uses:
Turmeric has several therapeutic and pharmacologic activities. The following is the most important phytopharmacology and therapeutic properties of turmeric: Anti-inflammatory[35], Antimicrobial [36,38,37] Antidiabetic [39] , Antioxidant Effects[36,35,37], Anti-Cancer Effect[35,37]. Cardiovascular Effects[36,35,37]., Gastrointestinal Effects[35]
Hepatoprotective Effects :
Turmeric, like silymarin, has hepatoprotective and reno-protective properties mainly due to its antioxidant properties and ability to lower pro-inflammatory cytokine production (3–5). Animal studies have shown that turmeric has hepatoprotective properties against a variety of hepatotoxic stimuli, including carbon tetrachloride (????????????4), galactosamine, acetaminophen (paracetamol), and Aspergillus aflatoxin. In rats with acute and subacute liver injury brought on by ????????????4, curcumin therapy dramatically decreased liver damage as compared to controls. Turmeric extract successfully reduces fungal aflatoxin production by 90% when tested on ducklings infected with Aspergillus parasiticus. Because sodium curcuminate, a curcumin salt, promotes biliary excretion of bile salts, this prevents and treats cholelithiasis.
CUMINUM CYMINUM:
The East Mediterranean region and South-West Asian nations are home to the cumin plant (C. cyminum) [40]. Cumin seeds are used in many different culinary traditions worldwide. Terpenoids, cymene, and cumin aldehyde are the main volatile compounds present in cumin seeds [41]. Myrcene, 1-8-cineole, α-pinene, ρ-mentha-1, 3-dien7-ol, β-bisabolene, β-farnesene, limonene, caryophyllene, β-phellandrene, cuminyl alcohol, and some oleoresin, gum, protein compounds, mucilage, and malates were among the volatile compounds reported to be present in cumin seed oil [42]. Additionally, it has been demonstrated that cumin seed extract contains antihyperglycemic, anti-inflammatory, and free radical-inhibiting qualities [43, 44]. Cumin was also found to have cardioprotective, lipid-lowering, and hypotensive qualities. Considering the substantial quantity of advantageous phytochemicals and established health advantages, the study was carried out to investigate the lipid-lowering and antioxidant properties of cumin seed [30].


Fig:6 Cuminum Cyminum Seed and Flower.
The main component of C. cyminum oil is Cuminaldehyde, which is utilized in the fragrance industry. It enhances the flavor of food and also serves as a natural remedy for various health issues. It functions as a tonic that benefits the nervous, circulatory, respiratory, and excretory systems. The digestion-related effects are attributed to cuminaldehyde, which activates our salivary glands, facilitating the primary digestion of food.The astringent, stimulant, carminative, diuretic, and antispasmodic qualities of C. cyminum are well known [47]. Because to the presence of linalool, carvacrol, flavonoids, monoterpene alcohols, and other polyphenolic chemicals, its oil had the highest known antioxidant activity [48].
Taxononical Classification: [49,50]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Biological name |
Cuminum cyminum |
|
2 |
Phylum |
Tracheophyta |
|
3 |
Class |
Magnoliopsida |
|
4 |
Order |
Apiales |
|
5 |
Family |
Apiaceae |
|
6 |
Genus |
Cuminum |
|
7 |
Specie |
Cuminum cyminum |
|
8 |
Kingdom |
Plantae |
Phytochemical Constituents:
Numerous phytochemicals found in C. cyminum seeds are known to have antioxidant, carminative, and anti-flatulent qualities [51]. Seeds also contain the highest concentrations of flavonoid phenolic antioxidants, including lutein, carotenes, and zeaxanthin [52]. Anthraquinone, protein, alkaloid, glycoside, steroid, coumarin, saponin, flavonoid, resin, and tannin were all found in C. cyminum, according to phytochemical research [46]. The volatile oil components like cumin aldehyde, cinnamic7acid, safranal, beta-pinene, caryophyllene, alpha-pinene, p-cymene, thymoquinone, γ-terpene, cuminyl alcohol, limonene, beta-farnesene, linalool, beta-myrcene, alpha- terpineol, betaphellandrene, benzyl cinnamate, saponins, resin, and also comprises tannins, alkaloids (coniine), flavonoids (quercetin, lutein, carotene), vanillic acid and resorcinol present in diverse portions of the plant [53],[54]. The major compounds occur in C. cyminum are cumin aldehyde, α- and β-pinene, cuminicacid, limonene, p-cymene, safranal, linalool, beta- farnesene, α- and γ-terpinene[48].
Pharmacologicalconstituent:
Digestive stimulant action[55], Antidiabetic effects[56], Antiinflammatory effects[57], hypolipidemic and hypotensive effects that have a cardioprotective impact [58].Chemopreventive effects[59], Antioxidant Activity[60].
Antioxidant Activity:
Antioxidant activities and the total phenolic content also found a good correlation among their nonvolatile extracts. So, it concludes that there is good antioxidant potential in C. cyminum. This spice can be utilized to yield flavoring agents as well as novel natural antioxidants that can be used in several food products [61]. C. cyminum yield of 2.5 to 4% essential oil of the weight of the fruits. The oil yield of C. cyminumis 2.5 to 4% of the weight of the fruits and the main constituent of essential oil is cuminol. Higher antioxidant power is shown by C. cyminum and this property made it a virtuous source of natural antioxidant. The methanolic extract of this spice revealed higher antioxidant activities than the essential oil[62].
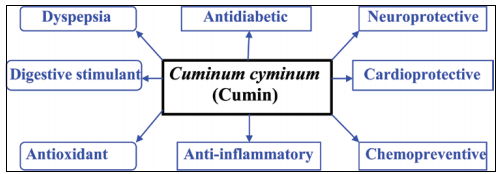
Fig:7 Pharmacological Activity of Cumin.
FOENICULUM VULGARE:
A member of the Apiaceae family, fennel (Foeniculum vulgare Mill.) is a famous aromatic plant and an important herbal remedy. It is related to cumin, dill, caraway, and anise, all of which have fragrant fruits that are often referred to as seeds [63].Fennel's seed has analgesic, antipyretic, and antioxidant qualities and is frequently used as a natural treatment for digestive issues such dyspepsia, bloating, and gas [64]. Additionally, it is utilized in the perfumery business and to flavor meals and liqueurs [65].


Fig:8 Fennel Seed and Flower
One of the best natural sources of antioxidants is fennel. Because of its high polyphenol and flavonoid content, this plant can suppress free radicals. Antioxidant activity was demonstrated by phenolic compounds found in this herb, such as quercetin-3-Ogalactoside, eriodictyol-7-orutinoside, rosmarinic acid, caffeoylquinic acid, and kaempferol-3-O-glucoside [70].
Taxonomical Classification:[71]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Kingdom |
Plantae |
|
2 |
Subkingdom |
Tracheobionta |
|
3 |
Division |
Magnoliophyta |
|
4 |
Class |
Magnoliopsida |
|
5 |
Subclass |
Rosidae |
|
6 |
Order |
Apiales |
|
7 |
Family |
Apiaceae |
|
8 |
Genus |
Foeniculum |
|
9 |
Species |
F. vulgare |
Phytochemical Constituent:
Trans-anethole, estragole, fenchone, and limonene are the primary ingredients of these monoterpenes and phenylpropanoids. Fenchone supplies the bitterness, estragole (methylchavicol) the sweetness, and trans-anethole, which is frequently the most common component, accounts for the anise taste [66].
Pharmacological Activity:
Fennel has anti-inflammatory, anti-bacterial, anti-fungal, and anti-parasitic properties in addition to being a strong antioxidant [68, 69]. Fennel has been shown in studies to have hepatoprotective benefits in a variety of liver lesions [67].
Anti-oxidant
Kaempferol and quercetin, two flavonoid antioxidants found in fennel, aid in the body's removal of dangerous free radicals, preventing illness and aging. Rutin strengthens blood capillaries, which helps with poor circulation.[7 2]
TRACHYSPERMUM AMMI [L.]:
Ajwain, sometimes called Carum copticum (or Trachyspermum ammi) seeds (CCS) [73], is an important Apiaceae family member that grows independently in eastern India. Carum copticum is mostly grown in India, Iran, Afghanistan, Pakistan, and Egypt. Ajwain seeds are small, oval, yellowish-brown fruits that smell like thymol and have medicinal properties. Because of its heated nature, CCS is also called a digestive, anti-flatulence, anti-diarrhea, appetizer, stomach and liver tonic, anti-dyspnea, and antitoxin in Iranian traditional medicine [74–76].


Fig:9 Trachyspermum ammi Seeds And Flowers
The ajwain plant may be helpful in the treatment of fatty liver and NAFLD patients due to its antibacterial properties [77] and positive effects on the modification of intestinal microbes [78]. Furthermore, it has been demonstrated that fat accumulation in the liver increases oxidative stress in mitochondria, liver cell inflammation, and ROS production in NAFLD patients, all of which result in cell death [79]. Therefore, the hepatoprotective properties of this plant [80,81], along with its anti-inflammatory and antioxidant properties [82], can stop the disease from getting worse. Because NAFLD is associated with hypertension (it is a component of the metabolic syndrome [83]) [74], ajwain's anti-hypertensive properties can help treat NAFLD patients.
Taxonomical Classification:[84,85]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Kingdom |
Plantae |
|
2 |
Subkingdom |
Tracheobionta, Vascular Plant |
|
3 |
Division |
Magnoliopsida- Flowering plant |
|
4 |
Phyllum |
Spermatophyta, Seed Plant |
|
5 |
Subphyllum |
Angiospermae, Seed Plant |
|
6 |
Species |
Ammi |
|
7 |
Family |
Apiaceae |
|
8 |
Genus |
Trachyspermum |
|
9 |
Order |
Apiales |
|
10 |
Class |
Magnoliopsida- Dicotyledons |
Phytochemical Constitute:
α-phellandrene, β-pinene, Cis-myrtenol, γ-terpinene, o-carene, Ot-pinene, p-cumin-7-ol, p-mentha-1,3,8 triene, Thymol, Carbohydrate, Glycosides, Saponins, Calcium, Flavones, Fiber, Moisture, Fat, Protein, and Mineral are among the phytoconstituents of T. ammi.
Pharmacological Action:
The pharmacological activities are Hepatoprotective, Antibacterial, Antioxidant, Antihypotensive, Abortifacient, Estrogenic, Insecticidal, and Antiulcer[86].
Antihyperlipidemic Properties:
Ajwain powder seeds are very effective in lipid profile and can reduce the amount of LDL-cholesterol, total lipids cholesterol, and triglycerides. In addition, seed extraction reduces the atherogenic index and increases HDL-cholesterol levels in albino rabbits. Compared to methanolic extract, petroleum ether extract showed more significant results in increasing HDL cholesterol levels and decreasing LDL cholesterol levels. Additionally, petroleum ether extract effectively decreased the atherogenic index [87].
PHYLLANTHUS emblica L.:
Amla, also known as Emblica officinalis, is a fruit of a deciduous tree in the Euphorbiaceae family. [88] (Newman et al. 2000). In India's tropical and subtropical regions, this fruit is commonly available. This well-known Indian medicinal herb has many health advantages. Gallic acid, ellagic acid, and rutin are the active ingredients found in amla. In addition to various other pharmacological qualities, it has analgesic, anti-inflammatory, and antioxidant effects (Khan et al., 2002) [89]. Nearly every part of this fruit has therapeutic qualities, especially the fruit, which is utilized in Ayurveda as a potent rasayana and in medicine to treat inflammation, diarrhea, jaundice, and a number of other conditions (Dasaroju and Gottumukkala, 2014) [90].

Fig:10 Phyllanthus emblica.L
Amla exhibits antioxidant, free radical scavenging, and heart-protective qualities (Patel and Goyal, 2011) [91]. Amla's soluble fiber lowers the risk of irritable bowel syndrome by controlling blood glucose levels and bowel movements. The risk of age-related macular degeneration is decreased by vitamin A content. Amla stops lens proteins from aggregating and becoming insoluble as a result of hyperglycemia. [92] (Suryanarayana et al., 2007). Phytonutrients and antioxidants aid in the battle against free radicals.
Taxonomical Classification:[93]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Kingdom |
Plantae |
|
2 |
Division |
Angiosperm |
|
3 |
Family |
Phyllanthaceae |
|
4 |
Class |
Dicotyledonae |
|
5 |
Order |
Malpighiales |
|
6 |
Genus |
Phyllanthus |
|
7 |
Species |
P.emblica L. |
|
9 |
Botanical Name |
Phyllanthus emblica .L |
Phytochemical Constituents:
Ascorbic acid (478.56 mg/100 gm), phytate (49.34 mg/100 gm), succinic acid (44.33 mg/100 gm), aspartic acid (36.1 mg/100 gm), glutamic acid (23.90 mg/100 gm), tartaric acid (14.06 mg/100 gm), β-sitosterol (11.50 mg/100 gm), leucine (4.25 mg/100 gm), histidine (2.40 mg/100 gm), and isoleucine[93].
Pharmacological Activity:
In addition to its anti-cancerous qualities, amla has analgesic, anti-atherogenic, adaptogenic, cardioprotective, gastroprotective, nephroprotective, and neuroprotective qualities. According to several studies (Sachan et al., 2013; Thilakchand et al., 2013; Dasaroju, et al., 2014) [90, 94], amla is effective in preventing and treating a number of illnesses, including cancer, atherosclerosis, diabetes, peptic ulcers, anemia, liver, heart, and other conditions.
Antioxidant properties :
Free radicals are neutralised by high amounts of phenolic substances and vitamin C, shielding liver cells from harm. Every metabolic process starts with emblica free radicals, which are constantly produced by the body's regular use of oxygen. The quantity of free radicals generated in the body and the quantity of antioxidants available to scavenge, quench, and protect the organism from their detrimental effects naturally exist in a dynamic balance. Khan (2009) [89].
PIPER nigrum L.
First found in India Piper nigrum belongs to the family Piperaceae. The plant's therapeutic qualities are widely recognized. It is also known as "the King of Spices" since it is the most often used seasoning. Blackpeppers come in a variety of varieties with different hues. Black and white peppers are the most common kind of peppers.[95] Black pepper (Piper nigrum) has been linked to NAFLD in a number of studies. Additionally, scientists are investigating if piperine could lessen the onset and severity of NAFLD. Piperine's bioavailability and bioactivity may be improved by novel drug development techniques, particularly when combined with other bioactive compounds or food additives.

Fig:11 Piper nigrum L.
There have been mixed results on the impact of black pepper (Piper nigrum) powder on liver function in individuals with nonalcoholic fatty liver disease. Previous research has demonstrated the effects of piperine on chronic illnesses, both on its own and in conjunction with other drugs and plant chemicals. Another study looked at the blood-liver enzymes, lipid profiles, and glycaemic indices of NAFLD patients using a combination of curcumin and piperine to increase curcumin bioavailability and reduce the severity of NAFLD. Another recent study has demonstrated that piperine, which is found in black pepper (Piper nigrum L.), improves the lipid profiles of overweight and obese individuals by increasing low-density lipoprotein (LDL) and decreasing triglycerides and total cholesterol [96].
Taxonomical classification:[97]
|
S.N |
DISCRIPTION |
PARAMETER |
|
1 |
Kingdom |
Plantae |
|
2 |
Division |
Manoliophyta |
|
3 |
Class |
Magnoliopsida |
|
4 |
Order |
Piperales |
|
5 |
Family |
Piperaceae |
|
6 |
Genus |
Piper |
|
7 |
Species |
nigrum |
Phytochemical constituents:
The black pepper It includes amides, flavonoids, alkaloids, lignans, and aromatic chemicals. Additionally, it contains up to 3.5% essential oil, which is made up of limonene, sabinene, pinene, phellandrene, and linalool. It also includes chavicine, an isomer of piperine, and piperine, a weak basic.[98].
Pharmacological Activity:
pharmacological characteristics including antioxidant, anti-inflammatory, anti-obesity, antitumor, anti-apoptotic, antipyretic, antifungal, anti-depressant, anti-infective and carminative behaviors. Piperine also augments the bioavailability of different natural compounds as well as drugs. Piperine stalls free radicals and reactive oxygen species with restrain of lipid peroxidation thanks to their flavonoids and phenolic contents.[99,100]
Black Pepper as Bioavailability Improver:
Piperine in pepper increases the availability of valuable phyto-chemicals present in food items in biological systems and can enhance the action of biochemically energetic compounds enclosed in it. It encourages the speedy absorption of certain chemicals from the gastrointestinal tract, defending them from being wrecked down by compounds in the intestinal lumen and by enzymes that happen in the cells lining of intestines.[101]
Black Pepper and its antioxidant property:
Black pepper is a readily available natural antioxidant, according to studies. Black pepper contains piperine, which is an effective antioxidant. It has been demonstrated that piperine can lessen oxidative damage brought on by a high-fat diet [102]. The amounts and value of significant antioxidant components are essentially maintained and increased by black pepper. Superoxide dismutase, gluthathione peroxidase, catalase, reduced glutathione volume, and the amount of protein carbonyl and malondialdehyde limitations in the hippocampus were all measured in order to project the antioxidant capacity of black pepper.[99]
Extraction Method:
Decoction:
An Ayurvedic mixture called kwatha is made by boiling plants in water. These are decoctions of water-soluble active ingredients found in modern medications, such as alkaloids. This kind of dosage has quick absorption and therapeutic effect since water is used as a carrier to extract vital plant elements for decoction preparation.

Fig:12 Decoction
Kwatha has water-soluble active ingredients. These water-soluble ingredients function quickly because they are easily absorbed from the intestine. As a result, the decoction is still sought after and sold as an over-the-counter drug. A product's quality is compromised by increased demand, which eventually causes problems with the dosage process's efficacy and safety. Therefore, in order to guarantee quality and safety, standardisation of the final dosage form—from the raw ingredients used to the processes involved to the finished product—is essential. Kwatha should be of standard quality, and in order to obtain good quality, it is crucial to focus on pharmaceutical aspects including temperature, preparation vessels, water quantity, raw drug particle size, and heating time.
Obtaining Extract:
Kwatha is typically one part raw product that can be reduced to one-fourth by boiling it with sixteen parts water.The most important factor to take into account in order to preserve the thermosensitive component of the Kwatha product is temperature. The Kwatha nature is protected when raw medications have the right particle size. In order to prepare Kwatha for full active principles, heating time is also crucial. To standardise Kwatha, a number of factors must be taken into consideration. Setting up a few parameters is therefore essential to achieving the optimal Kwatha shape.[103].
Maceration:
The room temperature maceration process was carried out on the Unimax 1010, Heidolph, Germany, using three particle sizes (0.3, 0.7, and 1.5 mm), three solid-to-solvent ratios (1:10, 1:20, and 1:30), five solvent types (30%, 50%, 70%, and 96% ethanol and water), and five extraction times (5, 15, 30, 60, and 90 minutes). In our initial screening, maceration may have caused a slight drop in TP yield at 90 minutes, particularly after 120 and 150 minutes (data not shown).


Fig:13 Maceration
A combination extraction technique used in pharmacognosy to maximise the yield of active ingredients from plant materials is maceration with water following decoction. In order to extract water-soluble chemicals, the coarsely ground plant material is first put through a procedure called decoction, which involves boiling it in water for a predetermined amount of time. The maceration phase involves filtering the decoction and then soaking the leftover plant residue (marc) in new water at room temperature. To allow the solvent to permeate the plant tissue and dissolve any remaining soluble components, the mixture is left for several hours with sporadic stirring. To increase the total extraction effectiveness, the filtered macerated liquid can be mixed with the decoction extract. The highest possible recovery of phytochemicals from the plant material is ensured by this technique. Following cooling, the decoction was put in a sealed container and left to macerate at room temperature for 24 to 48 hours. To enhance the phytoconstituent extraction, the contents were periodically agitated. After that, Whatman filter paper and muslin cloth were used to filter the extract. [132, 133].
Phytochemical Screening Herbal Extracts:
Phytochemical Screening of Curcima Longa L.:
Several phytoconstituents found in the powdered crude medication have been identified using qualitative chemical testing as part of the chemical evaluation. Several researchers conducted preliminary phytochemical analyses of the Curcuma longa rhizome's utilizing commonly used precipitation and coloration procedures to extract aqueous, acetone, ethanolic, chloroform, and methanolic substances. According to multiple researchers, these analyses showed the presence of carbohydrates, proteins, alkaloids, glycosides, terpenes, steroids, flavonoids, tannins, and saponins [104,105,106].
Preparation of the Extract
The rhizomes of Curcuma longa were collected and sun dried, cut into small pieces The small piece of dried rhizome was then grinded to get a fine powder, which is ready for use [105,106].
After combining the extract with three millilitres of diluted hydrochloric acid, it was thoroughly filtered. The filtrate was thoroughly examined using the subsequent test [106]:
(a) Mayer's Test :A few drops of Mayer's reagent are added by the test tube's side to one or two millilitres of filtrate. The presence of alkaloids was detected by a white or creamy precipitate [104, 107, 105, 108]
(b) Wagner Test: Wagner's reagent was added to 1 or 2 millilitres of the filtrate extract; the production of a brown, reddish precipitate indicates the presence of alkaloids [104, 107, 105].
(c) Dragendroff’s Test: The presence of alkaloids is indicated by the production of a noticeable yellow precipitate when 1-2 millilitres of Dragendorff's reagent are added to a few millilitres of filtrate [107, 105].
2. Glycoside Testing
(a) Adding equal amounts of Fehling's solutions A and B to a 2 ml test solution and heating the mixture yields a positive glycoside result. There was a brick-red precipitate [105].
(b) Legal's Test: Add pyridine and alkaline sodium nitroprusside to a 2 ml or 1 ml test solution; the presence of glycoside is indicated by a blood red or pink colour [104,105,106].
(c) Keller-Killani Test: Add a drop of FeCl3 treated with extract to two millilitres of glacial acetic acid.Glycoside is present when a brown ring forms [104, 106].
3. Flavonoids Test:
(a) Shinoda Test: Concentrated H2SO4 was added dropwise to a 2 ml test solution containing a few pieces of magnesium ribbon. The results shows pink scarlet or crimson red colour [104, 105].
(b) Alkaline Reagent Test: A sodium hydroxide solution was added to the test solution, giving it a yellow or red hue [104, 105].
4. Tannins Test:
(b) Gelatin Test: By combining two millilitres of test solution with a 1% Gelatin solution that contains ten percent sodium chloride, a white precipitate is produced [105].
5.Saponins Test :
Foam Test: The following is how researchers attempt to determine whether saponins are present: After shaking 5 ml of extract with 20 ml of distilled water, the mixture was brought to a boil. Saponins can be detected by frothing [104,107].
Phytochemical Screening of Cuminum Cyminum L. :
Screening for Phytochemicals
The Madurai local market is where the cumin seeds were bought. Using established methods, the methanolic extracts were put through chemical testing to identify several phytoconstituents [109].
Phenol Test (FeCl3 Test)
Three millilitres of distilled water and a few drops of a 10% aqueous ferric chloride solution were added to one millilitre of the extract. Phenols are present when a blue or green hue forms.
Flavonoid Test (Shinoda Test)
One millilitre of a 1% ammonia solution was added to two millilitres of the extract. The presence of flavonoids is indicated by a yellow appearance.
Tannin Test (FeCl3 Test)
One millilitre of 0.008 M potassium ferricyanide and one millilitre of 0.02 M ferric chloride with 0.1 N HCl were added to one millilitre of the extract. The presence of tannins is indicated by a blue-black appearance.
Alkaloids Test (Wagner's Reagent Test)
Two millilitres of Wagner's reagent were combined with about one millilitre of crude extract. Alkaloids are indicated by a reddish-brown precipitate.
Test for Carbohydrates (Benedict's and Fehling's tests)
Fehling's test
Two millilitres of crude extract were added to an equal volume of Fehling A and Fehling B reagents, which were then gently heated. Reducing sugars are present when a brick-red precipitate forms at the bottom of the test tube.
Benedict's examination
Benedict's reagent (2 ml) and crude extract (1 ml) were combined and heated. The presence of the carbohydrates was indicated by the formation of a reddish brown precipitate.
Protein Testing (Millon's Test, Ninhydrin Test)
Millon's examination
When 1 millilitre of crude extract and 2 millilitres of Millon's reagent were combined, a white precipitate formed that became red when heated gently, indicating the presence of protein.
Cardiac glycoside test (Keller-Kiliani test)
Two millilitres of glacial acetic acid with one drop of ferric chloride solution were added to five millilitres of extract. One millilitre of pure sulphuric acid was placed underneath this. The deoxy-sugar feature of carotenoids is indicated by a browning of the interface. A greenish ring may develop gradually over the thin layer of acetic acid, while a violet ring may emerge beneath the brown ring.
Saponin Test (Foam Test)
In a test tube, two millilitres of crude extract and five millilitres of distilled water were combined and forcefully shaken. Add a few drops of olive oil. Stable foam formation was interpreted as a sign that saponins were present.
Coumarin Test (Sodium Hydroxide Test)
The extract was mixed with 10% sodium hydroxide and chloroform. The development of a yellow hue indicates the presence of coumarin.
Terpenoids Test (Salkowski test)
To create a layer, 5 ml of extract, 2 ml of chloroform, and 3 ml of strong sulphuric acid were carefully added. The formation of a reddish-brown interfacial colouration suggests the presence of terpenoids.
Test for Steroids (Salkowski Test)
0.5 ml of crude extract containing 2 ml of sulphuric acid was mixed with 2 ml of acetic anhydride. The presence of steroids is indicated by the colour of the samples changing from violet to blue or green.
The sodium hydroxide test is used to detect quinones.
One millilitre of crude extract was mixed with diluted sodium hydroxide. Quinones are indicated by a blue-green or red hue.
Anthraquinone test (Borntragers test)
10% hydrochloric acid and 0.5 g of extract were heated in a water bath for a few minutes. After filtering, it was left to cool. The filtrate was mixed with an equal volume of CHCl3. The mixture was heated after a few drops of 10% ammonia were added. The development of a rose-pink hue signifies the presence of anthroquinones in n-hexane, chloroform, ethyl acetate, and methanol.
Analysis of Fourier Transform Infrared Spectroscopy (FTIR)
An Agilent Cary 630 FTIR spectrometer with Micro-lab PC software and an ATR sampling device with a resolution of 8 cm-1 and a scan range of 4000 cm-1 to 650 cm-1 was used to analyse the extracts.[110, 111]
Phytochemical Screening of Foeniculum vulgare:
Analysis of phytochemicals Using the corresponding calibration curve that was generated calorimetrically, phytochemical analysis was performed in hexane, chloroform, and methanol extracts of fennel seeds in terms of total phenolic content, total flavonoid content, and total tannin content.
Total phenolic content:
Chandrasekara and Shahidi slightly modified the Singleton and Rossi20 method to assess the total phenolic (TPC) content in hexane, choloroform, and methanolic extracts of fennel seeds [112]. In a centrifuge tube, precisely 0.5 mL of fennel seed extract and 0.5 mL of Folin Ciocalteu Reagent reagent were combined. Each test tube was filled with 1 mL of saturated Na2CO3 solution to neutralise the reaction, and the total volume was increased to 10 mL using distilled water. For 35 minutes, the mixture was incubated in the centrifuge tubes at 24°C in the dark. The mixture was then centrifuged for ten minutes at 4000 rpm, and the absorbance was measured at 725 nm in
comparison to the reagent blank.Gallic acid equivalents (mg GAEg-1) were used to record the data, and the TPC was calculated by creating a standard curve utilising various gallic acid concentrations.
Total flavonoid content :
The method used by Kim et al. [113] was modified by Chandrasekara and Shahidi [114] to determine the total flavonoid content (TFC). 4 mL of purified water and 1 mL of fennel extract were combined. The centrifuge tubes were then filled with 300 μL of NaNO2 and left to incubate for five minutes. After adding 300 μL of AlCl3 to the reaction mixture and letting it stand for a minute, 2 mL of 1M NaOH and 2.4 mL of distilled water were added. These solutions were immediately mixed and then incubated at 24°C for 15 minutes in the dark. After centrifuging the mixture for five minutes at 4000 rpm, the absorbance at 510 nm was measured. The TFC was expressed in milligrams of catechin equivalents (mg CAEg-1).
.Total tannins content:
The Sadasivam and Manickam method was used to determine total tannins [26]. After precisely 1 mL of extract was combined with 6.6 mL of water, 0.5 mL of Folin-Denis reagent and 1 mL of Na2CO3 solution were added, and the volume was increased to 10 mL with purified water. After 30 minutes of room temperature incubation, the test mixture's absorbance at 700 nm was measured in comparison to the reagent blank. Tannic acid (10–100 μg) was used to compute the amount of tannin from the standard curve. The standard was expressed as mg tannic acid equivalents (mg/TAE/g).[115]
Phytochemical Screening of Trachyspermum Ammi:
Flavonoid testing:
Alkaline Reagent Test: The crude extract was mixed with 2 millilitres of 2.0 percent NaOH. When two drops of diluted acid were added, the yellow tinge that indicated the presence of flavonoids vanished to colourlessness.[116]
Check for tannins:
Ferric chloride test: A few drops of a 10% ferric chloride solution were added to two millilitres of extract. A blackish blue tint appeared when gallic tannins were present, while a green-blackish colour appeared when catechol tannins were present.[117]
Check for alkaloids.
Mayer's test: Add 1 mL of Mayer's reagent to 1 mL of extract. A white, yellow, or cream-coloured precipitate indicates the presence of alkaloids [.118].
Check for saponins.
Foam test: A graduated cylinder was filled with 1 mL of extract solution diluted to 20 mL with distilled water and shaken for 15 minutes. The development of foam indicates the presence of saponins.[119].
Check for glycosides.
Keller-Kiliani test: Two millilitres of glacial acetic acid containing one or two drops of a 2% FeCl3 solution were combined with the crude extract. The extract was then transferred into a second test tube that included two millilitres of concentrated H2SO4. The development of a brown ring at the contact indicated the presence of cardiac glycosides.[120]
Phyllanths emblica Phytochemical Screening:
The ethanolic and aqueous extracts of Emblica officinalis were analysed using a conventional approach in the study by Jeevalatha et al. (2022) [121] to identify the presence of several phytoconstituents, such as alkaloids, tannins, glycosides, flavonoids, and saponins.
Check for Phenol :
Test for ferric chloride: One millilitre of the extract was mixed with three millilitres of distilled water and a few drops of a 10% aqueous ferric chloride solution. The presence of phenols is indicated by the formation of a green tint.
Check for Flavonoids :
Shinoda examination: One millilitre of a 1% ammonia solution was added to two millilitres of the extract. The presence of flavonoids is indicated by their yellow appearance.
Check for Tannins:
Ferric chloride test: Two millilitres of the extract were mixed with one millilitre (1%) of a 1% ammonia solution. The hue yellow indicates the presence of flavonoids.
Check for Alkaloids :
Mayer's examination :One millilitre of the extract, one millilitre of 0.02 M ferric chloride containing 0.1 N HCl, and one millilitre of 0.008 M potassium ferricyanide were mixed together. A blue-black appearance indicates the presence of tannins.
Check for Carbohydrates :
Fehling's test: Equal quantities of Fehling A and Fehling B reagents were mixed and heated gradually before adding two millilitres of crude extract. Reducing sugars are present when a brick-red precipitate forms on the bottom of the test tube.
Check for Proteins
a) The Millon test: One millilitre of crude extract and two millilitres of Millon's reagent were mixed to create a white precipitate that became scarlet when heated slowly, signifying the presence of protein.
b) The ninhydrin test :One millilitre of crude extract and two millilitres of a 0.2% ninhydrin solution were combined and boiled. A violet-colored precipitate indicated the presence of proteins and amino acids.
Check for Glycosides
a) Sodium hydroxide test The extract was treated with 1 millilitre of sodium hydroxide and 1 millilitre of water. Glycosides are indicated by the appearance of a yellow tint.
b)The cardiac glycoside Keller-Kiliani test: Five millilitres of extract were mixed with two millilitres of glacial acetic acid and one drop of ferric chloride solution. One millilitre of sulphuric acid concentration was added to this. A browning of the interface indicates the presence of a deoxy sugar property in cardenolides. A violet ring may appear beneath the brown ring, and a greenish ring may develop very slowly within the thin coating of acetic acid.
Check for Terpenoids
Salkowski examination:To make a layer, five millilitres of extract and two millilitres of chloroform were carefully mixed with three millilitres of strong sulphuric acid. The reddish-brown hue of the interface indicates the presence of terpenoids.
Check for Coumarin
The extract was mixed with 10% sodium hydroxide and chloroform to test for coumarins. The development of a yellow hue indicates the presence of coumarin.
Check for Saponins
Test of foam: Two millilitres of crude extract and five millilitres of distilled water were mixed together in a test tube and forcefully stirred. Add a few drips of olive oil. The creation of stable foam was thought to be a sign that saponins were present.
Check for Steroids
Salkowski examination: Two millilitres of sulphuric acid and two millilitres of acetic anhydride were combined with 0.5 millilitres of crude extract. Steroids are present when a sample's colour changes from violet to blue or green.
Check for Quinones
Quinone examination Diluted sodium hydroxide was mixed with one millilitre of crude extract. Red or blue-green hues are indicative of quinones.
Check for Anthraquinones
The Borntrager test:Each extract weighed 0.5 g and was briefly boiled in a water bath containing 10% hydrochloric acid. It was filtered and then allowed to cool. The filtrate was treated with the same volume of CHCl3. The mixture was heated after a few drops of 10% ammonia were added. When a rose-pink hue appears, anthraquinones are present.
Gallic acid was measured using High Performance Thin Layer Chromatography (HPTLC).[122]
Phytochemical Screening test of Piper Nigrum:
Check for saponins :
In a water bath, two grams of the powered sample were cooked in twenty millilitres of distilled water. To create a stable, long-lasting froth, ten millilitres of the filterable were combined with five millilitres of distilled water and forcefully shaken. Three drops of olive oil were added to the mixture, and it was vigorously shaken. then watched to see if an emulsion formed.
Check for tannins:
After boiling 0.5 g of the dried powdered sample in 20 ml of water, it was filtered. After adding a few drops of 0.1% ferric chloride, the colour was checked for brownish or bluish black.
Alkaloids test (Meyer's test):
After boiling 0.5 g of the dried powdered sample in 20 ml of water, it was filtered. Meyer's reagent was applied by t1 side of the test tube to a few drops of the filtrate. The test is positive if there is a creamy or white precipitate.
Check for flavonoids:
After heating a portion of the powdered sample with 10 millilitres of ethyl acetate over a steam bath for three minutes, the mixture was filtered. Ammonia that had been diluted was mixed with 4 millilitres of the filtrate. The presence of flavonoids is indicated by yellow colouring.
Check for cardiac-related glycosides:
One drop of 1% FeCl3 and two millilitres of glacial acetic acid were used to dissolve around 0.5 g of the extract. Concentrated H2SO4 was used to underlay this. The presence of a deoxy sugar, which is typical of cardiac glycosides, was shown by a brown ring that was produced at the interface. In the acetic acid layer, a greenish ring may form just above the ring and progressively expand throughout the layer, or a violet ring may appear underneath the ring.
Look for phenolic compounds.
Ferric chloride test: Five millilitres of distilled water were diluted with three hundred milligrams of extract, then filtered. Five percent ferric chloride was added to the filtrate. Phenolic substances are indicated by a dark green hue.[123]
Preformulation Studies of PolyHerbal Juice Formulation:
Physicochemical parameters (124–127): The herbal syrup was assessed for a number of physicochemical characteristics, including pH, Wt/ml, Specific Gravity, and physical appearance (colour, aroma, and taste).
a) Colour analysis: Five millilitres of the finished syrup were put into watch glasses and exposed to a white tube light on a white background. The colour was seen with the unaided eye.
c) Odour analysis: Two millilitres of the finished syrup were smelt separately. To counteract the impact of prior smelling, a two-minute gap was maintained between the two scents.
c) Taste test: A small amount of the finished syrup was taken and its flavour was assessed using the tongue's taste buds.
d) Determining pH: - Fill a 100 ml volumetric flask with precisely measured 10 ml of the finished syrup, then top it up with 100 ml of distilled water. For roughly ten minutes, the solution was sonicated. A digital pH meter was used to measure the pH.
e) Specific gravity at 250C: A completely dry and clean Pycnometer was chosen, and its contents were weighed after it was filled with freshly boiled and cooled water at 250C. Assuming that one millilitre of water at 250 degrees Celsius weighs 0.99602 grams in air with a density of 0.0012 grams per millilitre. The Pycnometer's capacity was computed. Adjusting the temperature of the final syrup to about 200C and the Pycnometer was filled with it. Then the temperature of the filled Pycnometer was adjusted to 250C, any excess syrup was removed and weight was taken.
Stability testing:
Nine portions of the final syrup (1A, 1B, 1C, 2A, 2B, 2C, 3A, 3B, and 3C) were taken in amber-colored glass bottles and kept at accelerated temperatures at 40C, room temperature, and 470C, respectively. The samples were tested for all the physicochemical parameters, turbidity, and homogeneity at intervals of 24, 48, and 72 hours to look for any changes.
Microbiological studies
Prepared juice blends were studies for microbial load. The microbial content of all the samples was estimated by using total plate count technique (APHA, 1967).[128]
Solubility Analysis:
An essential component of preformulation research for polyherbal juice compositions is solubility analysis. It is done to find out how soluble herbal components are in various solvents, including water, ethanol, and methanol. The physicochemical characteristics of the phytoconstituents in the formulation are better understood thanks to this investigation. The juice's active ingredients are distributed uniformly when they are properly soluble. It also aids in the selection of appropriate solvents for formulation development and extraction. To see how the polyherbal extract dissolves, it is combined with various solvents and agitated for a predetermined amount of time. The amount of dissolved components is then ascertained by filtering and analysing the mixture. The stability and bioavailability of the herbal formulation are improved by good solubility. Additionally, it enhances the polyherbal juice's medicinal efficacy. Solubility study is therefore essential to the creation of stable and potent herbal formulations.[130]
Rheology /Viscocity:
Using the equation, the apparent viscosity was used to calculate the amount of time needed for each sample to pass through a 10 ml pipette.
Flow rate is equal to pipette volume (ml) divided by flow rate (seconds) [129].
Preservative Compatibility:
A study on preservative compatibility is a crucial aspect of the preformulation analysis for polyherbal juice. This evaluation focuses on the interaction between the preservatives and the herbal ingredients in the formulation. Conducting this study ensures that the chosen preservative does not compromise the stability, efficacy, or safety of the herbal components. Commonly used preservatives, such as sodium benzoate or potassium sorbate, are incorporated into the polyherbal juice, and any physical or chemical alterations are monitored. The formulation is assessed for various parameters, including color alterations, precipitation, pH changes, and microbial growth over time. A suitable preservative effectively prevents microbial contamination and enhances the shelf life of the polyherbal juice. Thus, testing for preservative compatibility is vital for preserving the quality, stability, and safety of herbal formulations.
CONCLUSION
Non-alcoholic fatty liver disease (NAFLD), one of the most common chronic liver disorders in the world today, is closely linked to metabolic issues such obesity, dyslipidemia, and insulin resistance. Simple steatosis develops into non-alcoholic steatohepatitis (NASH), fibrosis, and eventually cirrhosis or hepatocellular carcinoma if treatment is not received. The cornerstone of treatment for NAFLD is lifestyle changes like dietary restriction and increased physical exercise, as there is presently no approved medication for the condition. Alternative therapy choices, especially herbal therapies, are becoming more and more popular due to their natural origins, therapeutic benefits, and relatively reduced side effects.
The potential use of a polyherbal formulation that includes therapeutic plants including Curcuma longa, Cuminum cyminum, Foeniculum vulgare, Trachyspermum ammi, Phyllanthus emblica, and Piper nigrum is highlighted in this review. Flavonoids, phenolic compounds, alkaloids, tannins, terpenoids, and essential oils with hepatoprotective, anti-inflammatory, antioxidant, hypolipidemic, and digestive stimulating qualities are among the many bioactive phytoconstituents found in these plants. Because oxidative stress, lipid buildup, and inflammation are important factors in the pathophysiology of NAFLD, these pharmacological actions are especially pertinent to its management.According to the Ayurvedic idea of polyherbalism, mixing several medicinal herbs may have a synergistic therapeutic impact that increases efficacy while lowering dosages and possible side effects. Decoction and maceration are two preparation techniques that aid in the extraction of water-soluble active components, improving the availability of phytochemicals. Preformulation research and phytochemical screening are other crucial procedures for assessing the herbal formulation's stability, safety, and quality.Overall, the results point to a potential natural strategy for promoting liver function and controlling NAFLD: a polyherbal juice formulation including several therapeutic herbs. However, before it can be suggested for broad therapeutic usage, more experimental research and clinical trials are required to scientifically establish its efficacy, safety, and mechanism of action.
REFERENCES
World Journal of Pharmaceutical Sciences, 2(5), 507–515.
World Journal of Pharmaceutical Sciences, 2(5), 507–515.

Aditi Shukla, Shweta Ram, Dr. Gyanesh Kumar Sahu, Suchita Wamankar, Hepatoprotective and Metabolic Restorative Potential of a Polyherbal Juice Formulation in Non Alcoholic Fatty Liver Disease, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1345-1374 https://doi.org/10.5281/zenodo.19479073
 10.5281/zenodo.19479073
10.5281/zenodo.19479073
