
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3Rungta Institute of Pharmaceutical Sciences, Kohka, Kurud, Bhilai.
5Rungta Institute of pharmaceutical Sciences and Research, Kohka, Kurud, Bhilai.
4J.k. college of pharmacy, Bilaspur.
Breast cancer is a leading health concern globally and the second highest cause of cancer-related deaths among women. Though predominantly found in women, it can also affect men, albeit infrequently. Its progression involves complex, multi-step processes that make prevention and treatment a significant challenge. The disease is characterized by its potential to spread aggressively to distant organs such as the liver, lungs, brain, and bones, complicating management and reducing survival rates in advanced stages. The classification of breast cancer spans stages 0 to 4, reflecting the size, type, and extent of tumor spread. Non-invasive tumors fall under stage 0, while stage 4 represents advanced, metastatic disease. Several risk factors contribute to its occurrence, including age, hormonal changes, genetics, lifestyle choices, and environmental exposures. Genetic mutations like BRCA1 and BRCA2, late menopause, lack of physical activity, alcohol consumption, and exposure to radiation significantly increase susceptibility to breast cancer. Early diagnosis has improved significantly due to advances in imaging technologies, such as mammography, MRI, and PET scans, alongside molecular diagnostic tools like biomarker identification and gene sequencing. Despite these developments, breast cancer’s diversity and complexity demand personalized treatment approaches and a deeper understanding of its underlying mechanisms. Enhancing preventive strategies and refining diagnostic methods are essential for reducing its global impact and improving patient outcomes.
The second most common cause of cancer-related fatalities in women is breast cancer. Both men and women are impacted by BC.[39] Male breast cancer is an uncommon cancer that makes up less than 1% of all breast cancers and less than 1% of all cancers in males. [6] It is still difficult to prevent breast cancer worldwide since it is a multi-step process that involves several cell types. [2] The term "breast cancer" describes malignancies that start in breast tissue, usually the lobules that provide milk to the ducts or the inner lining of the milk ducts.[38] Breast cancer is mostly incurable since it is a metastatic disease that frequently spreads to distant organs such the liver, brain, lung, and bone. [2] There are stage-0 to stage-4 Stages of the breast cancer depends upon the size and type of tumor and how much the tumor cells have been penetrated in the breast tissues . Whereas stage 0 describes the non invasive and stage 4 describes the invasive kind of tumor.[42] There are numerous risk factors such as aging, estrogen, sex, age of menopause, abortion, radiation, breast density, lactation, ovulation stimulating drug, gene mutations, and lifestyle, family history, etc which can increase the possibility of developing breast cancer [1] Mammography , magnetic resonance imaging (MRI) , single photon emission computed tomography (SPECT), ultrasonography and positron emission tomography (PET) are other commonly used imaging modalities . Based on the diagnosis and assessment of the extent of breast cancer, the need for preoperative systemic therapy is determined [57]
There are several histopathological subtypes of pre-cancerous and invasive breast cancer.
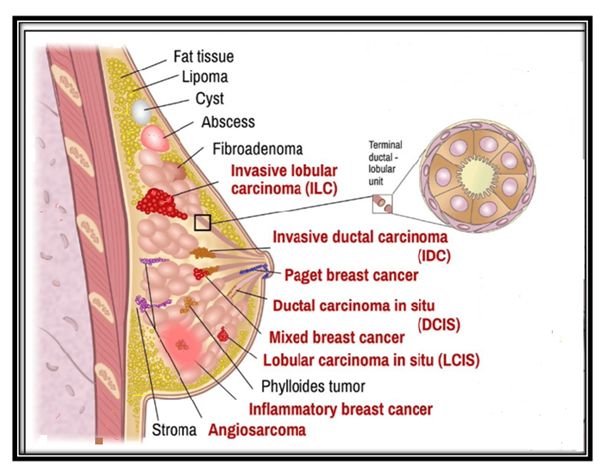
Figure 1 – Types of breast cancer
2.1 - Non-invasive(in-situ) breast cancer - kinds of breast tumors stay in a specific area of the bosom, without being spread into encompassing bosom tissue, lobules or pipes . The two main kinds of in situ cancers are perceived: ductal carcinoma, which address 80% of pre-malignant structures, and lobular carcinoma representing the next 20% . [39]
2.1.1 - Ductal carcinoma in situ (DCIS) – Another name for it is intraductal cancer. [39] Cellular and nuclear atypia, the propensity for malignancy, and both obligatory and non-obligatory inclinations to develop future invasive breast cancer are characteristics of this neoplastic proliferation of epithelial cells restricted to the ducts or lobules. Although they may be diminished or attenuated, the outer ductal layer's myoepithelial cells are often retained.[40]
2.1.2 - Lobular carcinoma in situ (LCIS) –It is the intralobular growth of tiny, loosely cohesive, and somewhat homogeneous cells that start in the TDLU and may or may not entail pagetoid involvement of terminal ducts. LCIS is a non-obligatory precursor and risk factor for the development of invasive cancer later on. [40] There are three primary forms of LCIS: pleomorphic, florid, and classical.[52]
2. 2-Invasive Breast Cancer- After invading the surrounding breast tissue, invasive breast cancer spreads to lymph nodes and other organs. The liver, lungs, brain, and bones are where these cells most commonly spread.[42] There are two main types of cancer: invasive lobular carcinoma (ILC) and invasive ductal carcinoma (IDC). Furthermore, certain cancers contain traits and cell types in common with cases that have been labeled mixed forms of carcinoma. [39]
2.2.1 -IDC (also called infiltrating ductal carcinoma) - IDC is the most well-known sort of invasive breast cancer (represents 70-80% of all cases). It happens for the most part in ladies older than 50 years and essentially those with acquired BRCA1 and additionally BRCA2 mutation . The risk of IDC is raised assuming the main feminine period preceded age 12 or on the other hand on the off chance that the lady entered menopause after age 55, because of delayed openness to female sex hormones . The 5-year endurance rate gauge is almost 99% when cancer has spread exclusively inside the breast or 86% in the event that malignant growth has spread into adjoining lymph hubs . Guess is deteriorating ( falls to 28%) in the event that it has metastasized to far off pieces of the body. IDC outgrowths beyond the milk channels to different pieces of the breast making a strong mass that the patient feels as the breast irregularity. It spreads through the lymph vasculature or circulatory system.[39]
It is a heterogeneous gathering of cancers with a few subtypes in view of morphological properties of growth cells
2.2.1.1 - Medullary carcinoma- Despite having a better prognosis and a better result than the typical IDC, medullary carcinoma (MC) is a rare and unique subtype of breast cancer that manifests as a well-defined tumor mass with anaplastic shape. Women around the age of fifty are affected. It is most prevalent in those who have BRCA1 mutations.In most series, it makes up less than 5% of mammary carcinomas, however reports of a frequency as high as 7% have also been made. [40]
2.2.1.2 - The classical nonspecific subtype – Pleomorphic cells with varying sizes, shapes, and big, irregular nuclei are characteristic of the classical nonspecific subtype. Most often, calcification, tissue necrosis, and squamous and apocrine metaplasias are seen.[39]
2.2.1.3 - The apocrine subtype - About 1% of all breast cancers are apocrine carcinomas, making them an uncommon kind of breast cancer.[49] Breast lesions that are benign, atypical, or malignant can all exhibit apocrine alteration. Most often observed in benign cysts with a simple or papillary shape, apocrine metaplasia is a common occurrence in the breast of women over 25. Other benign lesions, such as sclerosing adenosis, which is now called apocrine adenosis, are also recognized to exhibit apocrine transformation.[49] linked to a very bad prognosis. Large cells have granular cytoplasm that is usually very acidophilic. The unique and vesicular nuclei[39] 2.2.1.4 - Mucinous carcinoma - Mucinous breast carcinoma (MBC), otherwise called colloid carcinoma, is characterized by nests of cells floating in lakes of partitioned mucin and records for roughly 1-6% of all breast carcinoma. By and large, MBC is related with rare lymph node metastasis, low paces of neighborhood and far off repeat, and high 5-year illness free endurance rates .Most MBCs are positive for estrogen receptor (ER) and progesterone receptor (PR) articulation, though androgen receptor (AR) is communicated at a low level and human epidermal development factor receptor 2 (HER2) isn't enhanced. MBCs are separated into two kinds as indicated by the growth parts: unadulterated mucinous breast carcinoma (PMBC), with a mucinous part of over 90%, and blended mucinous breast carcinoma (MMBC), with a 51-90% mucinous part .[47]
2.2.1.5 - Papillary ductal carcinoma – Less than 1% of invasive BC is caused by papillary ductal carcinoma. It is common in postmenopausal, elderly women. These cells seem like small fingers (papillae) when seen under a microscope. Usually, cells are tiny.[39]
2.2.1.6 - Tubular ductal carcinoma - Tubular ductal carcinoma accounts for less than 2% of BC and is more common in women older than 50. The tumour cells are oval or elongated, well differentiated, randomly arranged, and lined with a single layer of epithelial cells and without the outer layer of myoepithelial cells. In all these last three phenotypes tumour cells are positive for ER and/or PR receptors and negative for the HER2 receptor [39]
2.2.2 - Invasive lobular carcinoma (ILC) – Accounts for 8–14% of all breast cancers . ILC is characterized by small, round cells that are bland in appearance and have scant cytoplasm, which infiltrate the stroma in single file and surround benign breast tissues in a targeted manner [43]
lobular carcinoma can also be divided into subtypes according to closer histological characterization:[39]
2.2.2.1- Classic (non-specific) subtype- Lobular invasive carcinoma's typical morphological characteristics are present in the classic (non-specific) subtype. The stroma is covered with tiny, evenly spaced cells that form a distinctive Indian pattern. Cells of the pleomorphic subtype, or at least some of them, are characterized by their eosinophilic cytoplasm and are significantly bigger than those of the classical subtype. These cells have hyperchromatic nuclei with a prominent nucleolus that are positioned eccentrically inside the cell. This subtype is also characterized by high expression of the tumor protein p53 and HER-2 receptor and lack of hormone receptor expression.[39]
2.2.2.2 - Tubulolobular subtype - Classical lobular cancer has a variation known as tubulolobular subtype. Cells that create a linear pattern resembling that of the classical subtype and tiny tubular forms with or without a lumen are its defining characteristics. This subtype is frequently characterized by an in situ lesion.[39]
2.2.2.3 - Histiocytoid subtype - A rare form of invasive lobular carcinoma is called histiocytoid breast cancer (HBC). with contentious histogenesis, which is typified by poor mitotic activity, big irregular nuclei or conspicuous nucleoli, linear or annular infiltration, plentiful foamy cytoplasm, and fuzzy cell boundaries.[51] Because of its histologic similarities to benign and other malignant tumors, it may be misdiagnosed.[50]
2.3 - Special types of breast tumours –
This category contains rare and histologically or clinically distinct breast cancer
2.3.1- Paget’s disease of the breast-
An rare illness influences 1-4% of breast cancer. Paget's sickness mainly influences postmenopausal ladies with a typical period of 62.6 years . The development of Paget's disease of the nipple is subtle. Usually unilateral, it first touches the nipple before growing centrifugally to the areola and subsequently the skin next to it. It mimics the appearance of Eczema, which is occasionally accompanied by weeping erythema. The skin turns from pink to crimson in tone. In severe Paget's disease, the nipple may retract, ulcerate, or bleed. The most commonly reported symptoms are pain, tingling, burning, and itching.[41]
2.3.2 - Inflammatory breast cancer – In the US, IBC causes between 1% and 3% of breast cancers, but it also causes around 10% of deaths from breast cancer .[44] Caused by cancer cells obstructing lymph arteries or channels in the skin of the breast, inflammatory breast cancer manifests as red, warm, enlarged breasts with dimples and/or wide ridges. Even yet, inflammatory breast cancer is rare and grows quite quickly. All multidisciplinary approaches, including as radiation therapy, surgery, chemotherapy, and imaging, must be carefully coordinated during treatment.[42]
2.3.3 - Angiosarcoma of breast – Angiosarcoma is quite possibly of the most uncommon cancer and includes 2% of all sarcoma . Angiosarcoma of the breast is quite possibly of the most rare malignancies . breast angiosarcoma can be characterized into primary when arising de novo and secondary to chronic lymphoedema or breast irradiation. . In contrast to primary breast angiosarcoma that generally affects young women, secondary breast angiosarcoma arises in older ladies (from 46 to 87 years), with a middle of 70 years Clinically optional angiosarcoma, particularly radiation-prompted angiosarcoma, influences the dermis of the breast and just sporadically creates inside the breast parenchyma. This is conversely, with essential angiosarcomas, which emerge inside the breast parenchyma and solely after include the skin.[46]
2.3.4- Phylloides tumour - Phyllodes tumor (PT) of the breast is an rare fibroepithelial neoplasm, representing 0.3% to 1% of all breast tumor . The grouping of PT proposed by the World Wellbeing neighborhood repeat going from 17% in harmless PT to 27% in malignant PT.[45]
2 - Stages of breast cancer [43]
2.1 - Stage 0- The non-invasive stage of a tumor is characterized by the presence of both cancerous and non-cancerous cells within the boundaries of the breast part where the tumor is growing, with no indication of their invasion in the surrounding tissues. DCIS is an example of stage-0 tumor . [42]
Figure 2 – Stage 0 Breast Cancer
2.2 - Stage 1 –This stage describes as the invasive breast carcinoma and microscopic invasion is possible in this stage. It has two categories that are 1A and 1B stage. The category 1A describes the tumor which measures up to 2 cm and none of the lymph nodes are involved in it while stage 1B describes that small group of cancer cells larger than 0.2 mm founds in lymph node. [42]
Figure 3 - Stage 1 Breast Cancer
2.3 - Stage 2 - This phase is also known by two other names, 2A and 2B, respectively. The staging process's Phase 2A shows cancer that has been discovered in the circulatory and lymphatic systems but not in the chest cavity. Cancer can range in size from less than 2 centimeters to more than 5 centimeters. Phase 2B, however, shows that although the cancer may be more than 5 cm in size, it has not spread to the axillary lymphatic nodes.[53]
Figure 4 – Stage 2 Breast Cancer
2.4 - Stage 3 - That although there is no tumor in the breast, it may be found in 4–9 axillary lymph nodes or sentinel lymph nodes, whereas stage 3B indicates that the tumor may be any size but has resulted in breast skin swelling or ulceration and may have spread to up to 9 axillary lymph nodes or sentinel lymph nodes. Inflammatory breast cancer, or stage 3B, is characterized by red, heated, and swollen breast tissue. Nevertheless, step 3C details the dissemination of 3A, 3B, and 3C are the three subcategories into which it has been separated. Of them, stage 3A characterizes tumors involving 10 or more axillary lymph nodes. and the lymph nodes above and below the collarbone have also been affected.[42]
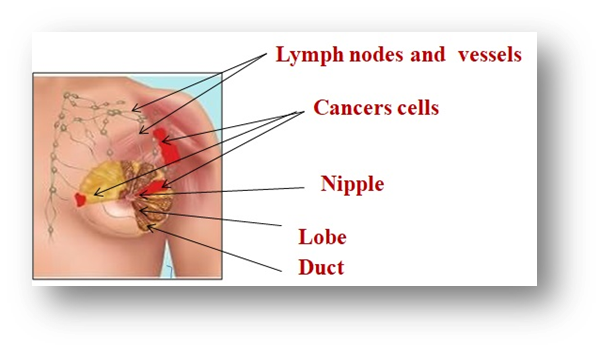
Figure 5- Stage 3 breast cancer
2.5 - Stage 4 – The disease has progressed to other organ systems, including the liver, brain, lungs, bones, and so forth. This is the advanced and metastatic stage of cancer.[53]
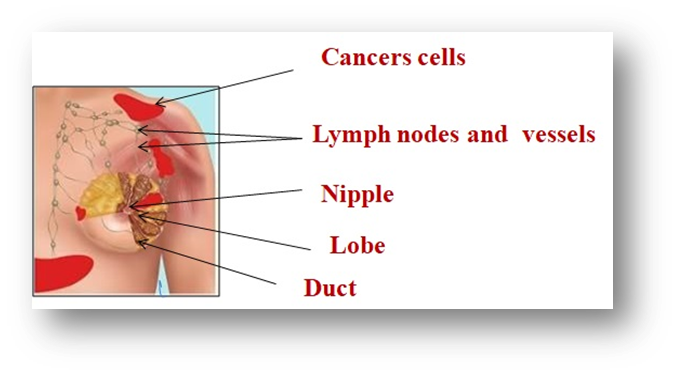
Figure 6 - stage 4 breast cancer
3 - Sign and symptoms -
A lump under the armpit or in the breast is the typical sign of breast cancer. Conducting a monthly breast self-examination (BSE) is an excellent method of being acquainted with the size, texture, cyclical changes, and skin condition of the breasts.
Breast cancer symptoms include breast swelling or lump (mass), breast swelling in the armpit (lymph nodes), clear or bloody nipple discharge, nipple pain, inverted (retracted) nipple, scaly or pitted skin on the nipple, persistent breast tenderness, and unusual breast pain or discomfort.
Underarm lymph nodes are found in advanced stages (metastatic) of the disease, often with additional symptoms such headaches, neurological discomfort or weakness, bone pain (bone metastases), shortness of breath (lung metastases), appetite loss (liver metastases), and inadvertent weight loss (liver metastases).[38]
4 - Breast cancer risk factor -
4.1 . Demographic factors -
4.1.1- Gender - Breast cancer growth is much of the time an illness that is novel to ladies and Male breast cancer contains <1>[6]
4.1.2- Age - The greatest recognized risk factor for breast cancer, after gender, age .[1] as the incidence of breast cancer rises with age, about doubling every ten years until menopause, at which point it sharply declines. Breast cancer occurs more frequently at younger ages than lung cancer. In certain nations, the age incidence curve flattens off following menopause.[4] Women above the ages of 40 and 60 accounted for around 99.3% and 71.2% of all breast cancer-related deaths in America in 2016, respectively.[2]
4.1.3 - Aob Blood group – Women who have blood type A and are Rhesus positive are more likely to get breast cancer, whereas women who have blood group AB and are Rhesus negative are less likely to do so, according to the findings of a review research. Despite a 2015 study that supported these findings, several studies did not discover a link between blood type and breast cancer.[1]
4.2 - Reproductive factor
4.2.1- Age of menarche – Unobtrusive height in breast malignant growth risk is related with early age of menarche .[8] also observation suggested that regular ovulatory feminine cycle increment a lady's risk of breast cancer . breast malignant growth hazard could be multiple times more prominent among ladies whose periods become normal in something like one year of their most memorable feminine period than among ladies with a five years or longer defer in the beginning of standard cycle.[7] Age at menarche and breast malignant growth risk are likely by implication related, with sustenance being the conceivable normal element. Research gauge that the risk of breast cancer can be diminished 10-20% for every year menarche is postponed. The consequences of a huge report uncovered that for every long term postpone in beginning of period, breast malignant growth risk was decreased by around 10%.[9]
4.2.2- Late age of menopause – The age of menopause over 50 years is related with an expanded risk of breast malignant growth . Ladies who experience menopause later have a drawn out ovarian action which expands the risk of creating breast malignant growth .It has been seen that for every 5 year contrast in age at menopause, the risk of BC changes by around 17%. [9] Ladies who arrive at menopause at a late age are bound to have a higher risk of breast cancer , albeit no reliable pattern is noticed . The higher breast malignant growth risk in ladies with a late menopause is in all likelihood made sense of by both the more extended length and more significant level of openness to estrogen and progesterone experienced by these ladies. They likewise may encounter a bigger number of anovulatory cycles bringing about an absence of cyclic progesterone. The impact of hormonal milieu on breast malignant growth during anovulatory cycle is less clear. Artificial menopause by reciprocal oophorectomy likewise extraordinarily decreases breast cancer risk and the impact is more prominent than that normal menopause . [7]
4.2.3-. Full term pregnancy – The risk of breast cancer is negatively correlated with the age at first full-term pregnancy (FP).[11] Perhaps the relationship is due to a long-lasting hormonal alteration, a maturity of breast cells during pregnancy that makes them less vulnerable to carcinogenic transformation, or both. A increased risk of breast cancer has also been linked to late age at last FP, however not all studies have found this. Apart from the initial and final research, very few others have examined the impact of age at FP.[1,10]
4.2.4 - Abortion – Studies have uncovered that the breast growths of women who have unconstrained or prompted abortion quite early in life have a higher pace of cell multiplication and a higher recurrence of aneuploid growths contrasted and the growths of other young women with breast cancer. During the primary trimester of pregnancy, the breast is portrayed by high mitotic action and expansion, and afterward in the mid to late pregnancy, cell separation prevail. In this manner, it is conceivable that those pregnancies that are not hindered for the rest of the main trimester could bring about the breast containing countless undifferentiated cells, comparative with the breast of women whose fetus removal was actuated right off the bat in pregnancy or the people who had no early termination by any means. [9] It has been proposed that abortion leave the breast epithelium in a proliferative state with an expanded defenselessness to carcinogenesis.[12]
4.2.5 - Ovulation menstrual cycle –
The ovulatory menstrual cycle may have a protecting role against breast cancer .[1]
4.2.6 - Pregnancy characteristics – ladies who were diagnosed to have pre -aclampsia and /or hypertension in their first pregnancy were at diminished hazard of breast cancer , contrasted with different ladies who didn't create pre -aclampsia and / or hypertension during their first pregnancy.[13]
Pregnancy, particularly the primary pregnancy, assumes a significant part in the risk of creating breast cancer. The consequences of studies showed that the risk of breast cancer is nearly multiplied in ladies who bring forth their most memorable youngster before the 33 weeks of growth .the risk of creating breast cancer increased in multiple births[1]
4.3 - Hormonal factors
4.3.1- Contraceptive methods – Oral contraceptives (OCs) among the most broadly utilized strategies are of viable and reversible family planning . Many inquiries exist concerning a potential relationship between the use of OCs and the development of cancer . Advantages and dangers of OCs use on cancer were explored by Working Gatherings of the Worldwide Organization for Exploration on Malignant growth (IARC/WHO) in 2007, which reasoned that OC are cancer-causing to humans.[14] . Family history of breast cancer is a laid out risk factor for breast cancer. Likewise, there is proof that oral contraceptive use might be related with a moderate increase in breast cancer risk.[15]
4.3.2- Ovulation - stimulating drug – The consequence of a case-control study showed that involving ovulation-invigorating prescriptions for over a half year builds the risk of creating breast cancer . Nonetheless, this finding was not affirmed in different examinations.
4.3.3 - Postmenopausal hormone therapy- Postmenopausal hormone therapy (HT), specifically estrogen in addition to progestin, increment and breast cancer risk. Postmenopausal estrogen and progestin use for a long time or more improves the probability of creating breast cancer that is analyzed at a high level stage. It isn't known whether breast cancer severity is increased even more in ladies with dense breast who use postmenopausal HT. [16]
4..4 - Hereditary factors
4.4.1- Genetic factors - Hereditary breast cancer is mostly caused by germline mutations in genes that are susceptible to breast cancer (BCs), such as BRCA1, BRCA2, TP53, CHEK2, PTEN, ATM, and PPM1D. Breast cancer is mostly caused by hereditary and genetic abnormalities in the BRCA1 and BRCA2 genes. [17]
4.4.2- Family history of breast cancer -Family background of breast cancer is generally perceived as a significant risk factor breast cancer [18] . family background of breast cancer in the sister, child, or male first-degree relative and maternal history of different diseases For rehash mammography, ladies with maternal history of breast cancer had a mean increment of 0.50 more mammograms in the beyond 6 years contrasted and ladies without maternal history of breast cancer . [19]
4.5 - Breast related factors
4.5.1- Lactation - Breastfeeding lessens chance of Breast cancer .non-breastfeeding moms have been displayed to have a higher risk of reproductive cancer . breast cancer have been viewed as more normal in ladies who didn't breastfeed . ladies who breastfed for something like two years during their lifetimes had a fundamentally lower chance of creating breast cancer than the individuals who breastfed for under two years. Contrasted and ladies who breastfed a sum of 0-11 months over their lifetimes, there was a 66.3?crease in breast cancer risk in ladies who breastfed for 12-23 months, a 87.4?crease in ladies who breastfed 24-35 months and a 94?crease in ladies who breastfed 36-47 months. The mean span of breastfeeding per youngster for something like a year was likewise connected with diminished hazard of breast cancer.[20] Breastfeeding is a positive, wellbeing advancing way of behaving, with breastfeeding term decreasing breast cancer risk. [21]
4.5.2 - Breast density - During the 2000s, breast thickness was recognized as a risk factor for breast cancer . A habitually cited size of this affiliation was a 4-to 6-overlap expanded risk in ladies with a percent mammographic thickness (PMD) at or higher than 75% compared with ladies with a thickness underneath 5% or 10%. . This made density one of the strongest known breast cancer risk factors. [22]
4.5.3- Benign breast disorders - The breast of breast malignant growth autonomously increased with the presence of harmless breast illness and with the increase in breast thickness. Ladies with harmless breast sickness and very thick breast had a triple raised hazard of breast cancer contrasted and those with dispersed fibro glandular thickness and without harmless breast illness . Ladies with harmless breast illness had a raised risk for over 15 years autonomously of their breast thickness category. Ladies with harmless breast illness and thick breast are at high risk for future breast cancer . [23]
4.6 - life style factors -
4.6.1- Obesity and overweight – Epigenetic changes brought on by fat raise the risk of BC. Genomic modifications known as epigenetic changes impact gene expression without changing the underlying DNA sequence. By modifying the action of hormone receptors, epigenetic modifications may impact hormone responses and contribute to the risk of breast cancer [BC] . [25] In addition to raising the chance of recurring breast cancer, obesity also raises the risk of serious comorbid conditions and lowers the quality of life for breast cancer survivors .[24]
4.6.2 - Alcohol consumption – Expanded liquor utilization was related with higher gamble of breast malignant growth. Ladies who polished off ?1 glass of liquor each day had a 33% higher gamble of breast cancer than nondrinkers in the unadjusted examination and 26% in the changed investigation [26]
4.6.3 - Diet – Diet might assume a part in both advancing and restraining human breast malignant growth development . [27] Unfortunate dietary propensities described by the high admission of refined starches, sugar, and both immersed and trans-saturated fats, as well as the low admission of omega-3 unsaturated fats, regular cell reinforcements, and fiber, adjust irritation and, in this way, have all the earmarks of being connected to expanded hazard of breast cancer and mortality.[28] responsive oxygen species (ROS); admission of phytoestrogen may lessen chance of breast malignant growth through genomic and non-genomic activity; vitamin D can diminish the risk of breast cancer by hindering the course of malignant growth intrusion .[27]
4.6.4 . Physical activity – Higher levels of physical activity may lessen a woman's chance of acquiring breast cancer when compared to women who engage in less physical activity.[30] PA at appropriate intensities may also operate as a preventive factor against the development of BC. Implementing public health initiatives that support and encourage an active lifestyle is crucial since it may lower the risk of BC. The association between physical activity and the risk of breast cancer will be better understood with the aid of future prospective research.[30]
4.6.5- Vitamin D – By preventing the process of malignant invasion, vitamin D can lower the incidence of breast cancer [27]. The largest was an Italian research that collected data on dietary sources of vitamin D using a 78-item food frequency questionnaire. The study had 2,569 cases and 2,588 controls. The incidence of breast cancer was 34% lower for women who consumed the most vitamin D (>190 IU) than for those who consumed the least amount (<60>[31]
4.6.6 - Smoking – Smoking was related with an unobtrusive however essentially expanded chance of breast cancer, especially among ladies who began smoking at juvenile or peri-menarcheal ages. The general risk of breast cancer related with smoking was more prominent for ladies with a family background of the sickness. [32] Menopausal status assumes a critical part in the connection among tobacco and breast cancer for all cancer subtypes. While smoking appears to expand the risk in premenopausal lady, bringing down chance of breast cancer among postmenopausal ladies with abundance weight may be related. [33]
4.7 - Other risk factor -
4.7.1- Air pollution – Air contamination has been connected with an increased risk of breast cancer . Parts of air contamination are cancer-causing including compound that possibly increment oxidative stress or DNA harm or have endocrine upsetting properties. Nitrogen dioxide (NO2) and nitrogen oxides (NOx), traffic-inferred air toxins, have been reliably connected with an increased risk of breast cancer .[34]
4.7.2 - Night work - The night shift work could increase the risk for breast cancer . Having at any point worked extremely durable or turning night shift was related with an increase risk for breast cancer compared with day work .[35]
4.7.3 - Socioeconomic status –A connection between high financial status and breast cancer . breast cancer is higher in ladies with higher financial status, which can be because of the immediate impacts of significant risk factors like paralysis , and more established age at the first childbirth and during menopause. In expansion, stationary way of life and a high-fat eating routine in this friendly class can directly and by indirectly affect the feminine cycle of ladies .[1]
4.7.4 – Radiation - Radiation therapy at moderate to high doses is known to raise the risk of breast cancer. Women who underwent diagnostic chest X-rays for pneumonia or TB and radiation for a prior malignancy were shown to have higher risks for breast cancer.[36]
4.7.5- Diabetes - Women with type 2 diabetes have a marginally higher chance of getting breast cancer. Any organ with high amounts of estrogen receptors, such as the breast, endometrium, and ovaries, is more susceptible to cancer when insulin resistance results in a lower level of estrogen. many ways that the amounts of IGFBP-3, IGF-1, and cytokines raise the risk of breast cancer.[37]
5 - Diagnosis –
Numerous techniques have been developed to diagnose breast cancer, primarily relying on imaging and molecular biotechnology analysis. [ 55]
5.1.1- Mammography- The recommended method for screening and diagnosing BC is mammography (MG), which also assists physicians in gathering clinic data on BC patients . [55] An x-ray of the breast called a mammography can show either benign or cancerous abnormalities. In order to create an x-ray picture, a little dosage of radiation is applied through the breast after compression between two plates. [57] The American Cancer Society [ACS] recommends annual mammograms for women starting at age 40. These screenings are especially helpful for women between the ages of 40 and 74. Age, ethnicity, personal history, radiologist experience, and technique quality all affect how sensitive a mammogram is. Premenopausal women and those with high breast density may have less sensitivity. Recently, contrast-enhanced (CE) digital mammography has been utilized as an additional breast screening method to mammography. CE uses tumor angiogenesis to identify breast cancer. It produces a little more radiation than mammography and employs intravenous iodinated contrast injections. CE mammography provides better detection accuracy than mammography and is more sensitive and performs better than both mammography and ultrasound .[56] The following are some of their benefits: Quick screening, excellent precision, affordable, and appropriate for advertising.[55] Among the numerous disadvantages of mammography include its use of ionizing radiation, its inability to be used on individuals with thick breasts, its comparatively high rates of false-positive and false-negative results, and its unpleasant nature. [56].

Figure 7 – Mammography
CONCLUSION-Breast cancer is still a major worldwide health issue, especially because of its complexity and variety, which make care and prevention more difficult. Personalized therapies, molecular diagnostics, and imaging technology advancements have all enhanced early detection and treatment results. But the disease's varied biochemical activity and potential for metastasis highlight how crucial it is to keep researching and developing new treatments. Improving public awareness, addressing risk factors, and supporting early detection initiatives can all help to drastically lower the worldwide incidence of breast cancer. Effectively battling this powerful illness requires cooperation in the fields of research, politics, and medicine.
REFRENCES


Rajendra Kumar, Jyoti Prakash, Mayank Borkar, Ravind Kumar, Chandraprabha Dewangan*, A Comprehensive Review of Breast Cancer: Classification, Stages, Risk Factors, And Diagnostic Method, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 2, 1604-1619. https://doi.org/10.5281/zenodo.14891839
 10.5281/zenodo.14891839
10.5281/zenodo.14891839