
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Yashwantrao Bhonsale College of Pharmacy Sawantwadi.
Periodontal diseases is a broad spectrum of inflammatory diseases which results in degeneration of Periodontium and involves all the supporting structures of teeth like gingiva, periodontal ligament, cementum and alveolar bone etc. followed by loss of teeth. WHO had estimated that 10-15% of the world population is suffering from severe periodontal status. It is multifactorial infectious disease due to virulent microbial growth on teeth. The primary purpose of this study is to give systemic update on periodontal disease in terms of its stages, occurrence, pathophysiology, diagnosis, management and treatment. The pathophysiology of periodontal disease is linked to dental plaque, microbial biofilm formation and host cell's immunogenicity. The severity of the disease is related to risk factors and chronological stages. Prevention is achieved through the regular oral hygiene. Microbial biofilm development can be managed by a host of surgical and nonsurgical treatment methods available for the same. Daily care and periodic control prevent aggravation of condition and exhibit obvious enhancement of oral condition.
An infection of the periodontium is called periodontitis. While "dont" denotes a tooth, "itis" denotes inflammation, and "perio" refers to the gingiva and other tissues around teeth. Thus, the entire word "periodontitis" denotes persistent inflammation of the dental cementum, alveolar bone, and gingiva[1] periodontal ligaments. The World Health Organization (WHO) claims that it is a chronic illness that is highly contagious worldwide [2]. It starts with plaque buildup around teeth, which creates bacterial microbiological biofilms. This is followed by localized gingival inflammation. Chronic periodontal disease is the result of neglecting this scenario. At this point, harmful byproducts and enzymes from periodontal bacteria, including collagenase, fibrinolysis, leucotoxins, and other Bacteroids spp., such as B. intermedius and B. gingivalis, as well as fusiform organisms, such as Actinobacillus actinomycetemcomitans, Wollina recta, and Eikenella spp.; Porphyromonas gingivalis, Taneerella for synthesis, and various bacilli and cocci; spirochetes; amoebas, and trichomonads, cause damage to the periodontal structure.[3,4,5] By keeping oral hygiene proper, it can be reversed at the initial stage but if at this stage plaque is not removed then formation of calculus or tartar take place which is not removable by tooth brush or floss. Due to this tartar, bacterial action commences on deeper tissues due to which periodontal ligaments surrounding teeth becomes weakened and cause resorption of alveolar bone.[6] There occurs a space between gingiva and tooth takes place which is known as "Periodontal Pocket" and it is mostly recognized as periodontitis or periodontal disease. The intensity of this disease varies depending upon microbial plaque formation.[7] The Screening and examination of this disease has been carried out by different ways, which leads to finding of severity of periodontal ligament. There are various tests available to diagnose the periodontal disease like radiograph technique, haematological screening, laser treatment, tissue engineering, etc. For the control of disease progression there are various treatment modalities available (surgical as well as non-surgical) based on the chronology of disease. Its maintenance is performed by intensive care and by maintaining good oral hygiene.[8,9]
Stages
There are primarily four stages of periodontal diseases which constitute various clinical sign & symptoms and radiological screening are mentioned as follows:[10,11,12]
1. Gingivitis
It is the sole stage where periodontitis can be reversed. At this stage the plaque formation around the teeth takes place. There are primarily few painless symptoms that are observed at this stage like bad breath, inflamed reddish gums and bleeding on intubation brushing and flossing. It can be reversed by regular checkups and good oral hygiene. Usually, 1-2 mm clinical attachment loss, less than 15% bone loss around root, probing depth 4mm or less happens.
2. Early stage
It is the second stage of periodontal disease. It can be controlled by oral hygiene but not reversed. At this stage, the infection begins spreading to adjacent tissues and begins demoralizing it. Signs at this phase are inflammation of gums, bad breath, and bleeding upon brushing or flossing, spacing between teeth become apparent and will increase over time. At this place, 3-4 mm clinical attachment loss, less than 15-33% bone loss around root, probing depth 5 mm or less happens.
3. Moderate stage
Similar second stage moderate stage cannot be reversed. Same symptoms as moderate stage occurs but space between teeth and gum recessions are more pronounced. Treatment such as deep cleaning, scaling and flap surgeries may be performed at this phase. Approximately 5 mm or more clinical attachment loss, 33%of four or fewer teeth loss, with advanced problems like probing depth 6 mm or greater, Class II-III furcations, and moderate ridge defects.
4. Advanced stage
Final stage of periodontal disease; where 50-90% of loss of periodontal tissues. Also other symptoms such as swollen gums that exude of pus, cold sensitivity, loosening of teeth, painful chewing and excessive halitosis occurs. If left untreated it produces more spaces or gaps between teeth and gums, gum recession, patient needling dentures, and other health issues that can be worst. Treatment are regular checkups, cleaning and regular good oral hygiene can stop the progression of Periodontitis. Secondary Occlusal trauma, extensive ridge defects, bite collapse, pathologic migration of teeth, fewer than 20 remaining teeth (10 opposing pairs) observed.
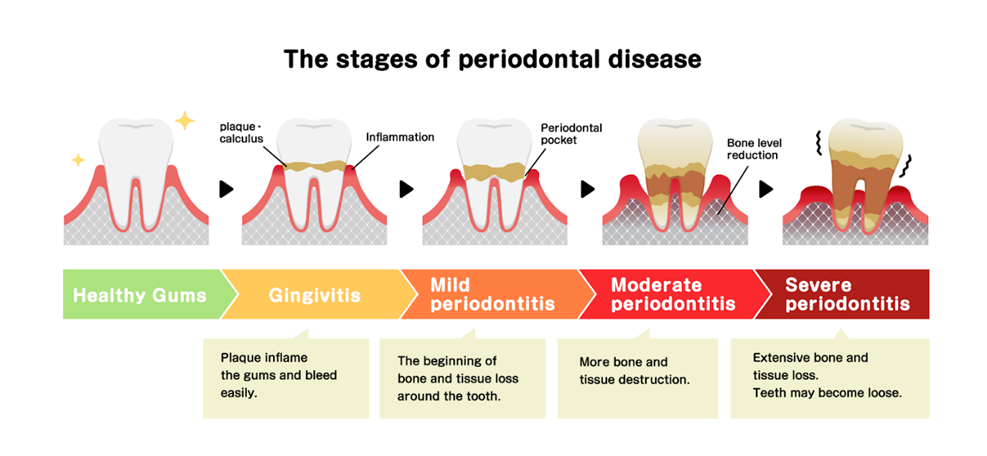
Figure No: 1
Types of Periodontitis [13, 14, 15, 16]
1. Gingivitis
According to the explanation above, gingivitis refers to inflammation of gums which can be turned back by regular oral hygiene.
2. Chronic periodontitis
In the case of this type of periodontal illness, symptoms include chronic gums inflammation, advanced bad breath and bleeding with brushing or flossing results. Loss of epithelial tissue, ligaments and bones which is irreversible.
3. Aggressive periodontitis
It may occur in localized or generalized forms, both are early onset type of chronic periodontal inflammatory disease, common presenting between puberty and early third decade of life. The presentation is same as chronic periodontitis.
4. Necrotizing ulcerative gingivitis
It occurs predominantly in individuals suffering from malnutrition, immune suppressive and HIV. Necrosis refers to cellular or living tissue death. It occurs predominantly due to deficit of nutrition required by individuals to stay healthy.
5. Systemic chronic periodontitis
This form of chronic periodontal disease occurs in patient who have systemic syndrome. Gum inflammation occurs because of systemic illness like Diabetes, Heart disease, Respiratory disease, etc.
Symptoms of periodontal disease
Herbal Remedies [17, 18]
1) Garlic

2) Tulsi

3) Neem

4) Clove

5) Guava [7]

6) Turmeric

7) Liquorice
8) Mint

Side Effect of Antimicrobial Drugs
Table No: 1
|
Sr. No |
Drug |
Side Effect |
|
1 |
Chlorhexidine (Perio-Aid) |
Staining of teeth and tongue, taste disturbances |
|
2 |
Doxycycline (Periostat) |
Vomiting, Diarrhea, Abdominal Pain |
|
3 |
Metronidazole (Flagyl) |
Abdominal pain, Metallic taste, Dizziness |
|
4 |
Azithromycin (Zithromax) |
Nausea, Vomiting, Diarrhea, Abdominal Pain, Hepatotoxicity. |
|
5 |
Linezolid (Zyvox) |
Anaemia, Lactic acidosis. |
Marketed Preparation
1) Amulya Dant Herbal Toothpaste:
This toothpaste uses a unique blend of natural herbs like neem, clove, and peppermint that fight plaque and freshen breath without harsh chemicals. It is Powerful herbal antiseptic paste used to kill the bacteria that cause cavities, gingivitis, and bad breath while soothing and protecting gums.
2) Tooth & Gums Tonic:
It is Truly Natural antimicrobial oral rinse designed to reduce harmful bacteria and gingival inflammation. It is Alcohol-free and non-staining. This award-winning rinse provides a valuable solution for periodontal treatment and maintenance. Tooth & Gums Tonic is ideal for periodontal therapy, post-procedure care, implant maintenance, oral malodor treatment or as an in-office preprocedural rinse.
3) Spice E Tooth Powder:
Spice E is a herbal toothpowder with 100% natural ingredients. Spice E is not only a tooth powder but also act as a mouth freshener. It contain the Ingredients: Clove has been used since ancient times as a natural toothache remedy. Clove contains an active ingredient called Eugenol, which is a natural aesthetic. It helps numb and reduce pain to ease a toothache. Cardamom is the major active component of cardamom is Cineole, which is a potent antiseptic known for killing the bacteria causing bad breath. It also inhibits the development of cavities, reverse cavities, cleanses the teeth and thwarts tooth decay. Black Pepper Black Pepper combats tooth decays as well as cavities and encourage healthy strong teeth. Black Pepper also heal tooth aches as well as reduce pains.

4) Bioayurveda Mouth Wash:
REFERENCES

Pratik Fagare*, Tushar Sonnar, Roshani Gosavi, Sneha Sawant, Dr. Vijay Jagtap, Herbal Antimicrobial Agents Used against Periodontal Pathogens, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 2571-2579 https://doi.org/10.5281/zenodo.15089302
 10.5281/zenodo.15089302
10.5281/zenodo.15089302