
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Neotech Institute of Pharmacy, Vadodara, Gujarat, India.
The atypical immune response that results in the body's defense mechanism attacking healthy tissues and failing to identify self-antigens is the cause of autoimmune disorders. From organ-specific diseases like type 1 diabetes mellitus to systemic diseases like systemic lupus erythematosus, these ailments cover a broad range. The growing incidence of autoimmune disorders around the globe emphasizes how critical it is to comprehend their intricate etiology, which includes hormonal variables, environmental triggers, genetic susceptibility, and dysregulated immune pathways. Recent developments in immunopathology have demonstrated the roles that inflammatory cytokine networks, autoreactive lymphocytes, and autoantibody synthesis play in the development of disease. In order to improve early detection, diagnostic methods increasingly combine clinical assessment with genetic, imaging, and serological methods. With the goal of restoring immunological tolerance while reducing side effects, therapeutic approaches have changed from traditional immunosuppressants to targeted biologics and new cell-based therapeutics. With a focus on converting immunological findings into better patient outcomes, this review summarizes the state of the art regarding the etiology, diagnostic techniques, and therapeutic approaches of autoimmune illnesses.
Chronic conditions known as autoimmune diseases (AIDs) occur when the body's own cells, tissues, and organs are mistakenly attacked by the immune system, resulting in tissue damage, inflammation, and functional impairment [1]. When immunological tolerance is compromised, autoreactive T and B cells can multiply and create harmful autoantibodies, leading to several disorders [2]. Systemic lupus erythematosus, rheumatoid arthritis, type 1 diabetes mellitus, and multiple sclerosis are among the more than 80 different autoimmune diseases that have been recognized [3]. Autoimmune illnesses are becoming more common worldwide; estimates place their frequency between 3 and 8% of the population, with a disproportionately high incidence among women [4]. Hormonal factors, environmental triggers, genetic predisposition, and changes in the microbiota are all associated with this growing burden [5].These illnesses' chronic nature has a significant financial and medical impact in addition to lowering patients' quality of life [6]. Depending on the spread of immune-mediated damage, autoimmune disorders are often classified as either systemic or organ-specific [7]. While systemic diseases, like systemic lupus erythematosus, impact numerous organ systems through extensive inflammatory processes, organ-specific disorders, such type 1 diabetes mellitus, focus on a particular tissue [8]. Immunological advancements have identified several processes as important contributors to disease pathogenesis, including bystander activation, epitope dissemination, molecular mimicry, and impaired regulatory T-cell activity [9]. The majority of modern treatments aim to regulate symptoms and inhibit the immune system generally rather than provide a permanent cure, even though our understanding of autoimmune mechanisms has increased [10]. Targeted biologics, antigen-specific immunotherapy, and immunological tolerance-restoring strategies are being investigated in recent years and show promise for more individualized and efficient therapies [11]. By incorporating the most recent mechanistic discoveries into clinical practice, this review seeks to offer a thorough examination of the immunopathology, diagnostic techniques, and treatment methods in autoimmune illnesses.
2. ETIOLOGY
Autoimmune disorders have a complex etiology that results from the interplay of immunological, hormonal, environmental, and genetic variables. Together, these factors lead to the onset of pathogenic immune responses and the collapse of self-tolerance [12].
1. Genetic susceptibility
One of the main factors influencing the risk of autoimmune diseases is genetic predisposition. Disease development is significantly influenced by variations in the human leukocyte antigen (HLA) genes. For example, HLA-B27 is linked to ankylosing spondylitis, while HLA-DRB1 alleles are linked to rheumatoid arthritis and type 1 diabetes mellitus [13]. Additionally, immunological dysregulation and disease susceptibility are influenced by non-HLA genetic polymorphisms such PTPN22, CTLA4, and IL2RA [14].
2. Environmental elements
In people who are genetically predisposed, environmental stimuli can cause or worsen autoimmune reactions. Multiple sclerosis and systemic lupus erythematosus have been linked to viral infections, specifically Epstein-Barr virus (EBV) [15]. Cigarette smoking, nutrition, occupational exposures, and UV radiation are further important variables [16].
3. The effects of hormones
Women are more likely to have autoimmune disorders, which may indicate that sex hormones play a part in disease modulation. While testosterone tends to decrease immunological responses, estrogen increases humoral immunity by promoting B-cell activity [17]. Variations in disease activity have also been associated with changes in hormones throughout pregnancy and menopause [18].
4. Disorders of the immune system
Autoreactive T and B cells survive when there is a loss of central tolerance in the thymus and bone marrow, together with impaired peripheral tolerance. Autoimmunity is sustained by mechanisms like aberrant antigen presentation, increased pro-inflammatory cytokine production, and compromised regulatory T-cell activity [19].
3. PATHOPHYSIOLOGY
Autoimmune disorders are caused by a series of immunological processes that culminate in the destruction of one's own tissue. Numerous similar pathways have been found, including loss of immunological tolerance, aberrant antigen presentation, activation of autoreactive cells, autoantibody synthesis, and persistent inflammation, even if the precise mechanisms differ across various autoimmune illnesses [20].
1. Immunotolerance breakdown
During development, self-reactive T and B cells are eliminated by central tolerance, which takes place in the thymus and bone marrow. Autoreactivity is further inhibited by peripheral tolerance mechanisms like immunological checkpoints, anergy induction, and regulatory T cells (Tregs). Autoreactive lymphocytes can survive and get activated when these pathways are flawed [21].
2. Unusual appearance of antigens
Autoreactive T cells are activated when antigen-presenting cells (APCs) in genetically predisposed people exhibit self-antigens in response to costimulatory signals. People are predisposed to disease because some HLA molecules have a greater propensity for presenting peptides produced from autoantigens [22].
3. Activation of autoreactive
lymphocytes After tolerance is breached, pro-inflammatory cytokines like TNF-α, IL-6, and IFN-γ are released by autoreactive CD4? T helper cells and CD8? cytotoxic T cells as they infiltrate target organs. This encourages tissue damage, inflammation, and the recruitment of more immune cells [23].
4. Production of autoantibodies
Autoreactive T cells stimulate B cells, which then develop into plasma cells and generate harmful autoantibodies. These antibodies have the ability to cause direct tissue damage, create immune complexes that accumulate in organs, or trigger the complement cascade, which results in further inflammation [24].
5. Prolonged tissue injury and inflammation
Chronic inflammation results from ongoing innate and adaptive immune response activation. Through oxidative stress, the release of proteolytic enzymes, and fibrosis, this environment perpetuates tissue damage. Widespread cytokine dysregulation plays a role in multi-organ involvement in systemic illnesses [25].
6. Differences in disease mechanisms
Autoreactive T lymphocytes attack pancreatic β-cells in type 1 diabetes mellitus, resulting in insulin insufficiency [26]. Autoreactive T lymphocytes penetrate the blood–brain barrier and harm myelin sheaths in multiple sclerosis [27]. Complement activation and immune complex deposition result in extensive tissue inflammation in systemic lupus erythematosus [28].
4. MECHANISM OF ACTION (MOA)
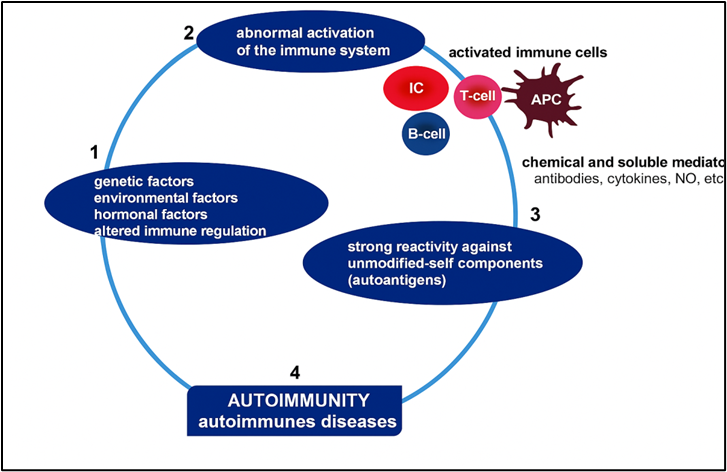
Figure 1. Pathophysiological Mechanisms of Autoimmune Diseases[61]
The sequence of immunological events leading from the breakdown of immune tolerance to target tissue harm is referred to as the mechanism of action in autoimmune disorders. The pathogenic processes including antigen detection, lymphocyte activation, cytokine-mediated signalling, and effector cell-mediated tissue damage are typically shared by autoimmune disorders, despite the fact that each one has distinct molecular targets [29].
1. Immune activation and antigen recognition Antigen-presenting cells (APCs) use major histocompatibility complex (MHC) molecules to present self-antigens to naïve T lymphocytes in genetically susceptible people in response to environmental or viral stimuli. Autoreactive T cell activation is made possible by aberrant costimulatory signals (such as CD80/CD86-CD28 interactions) and impaired checkpoint inhibition (such as CTLA-4, PD-1) [30].
2. Effector pathways mediated by T cells After differentiating into subsets like Th1, Th17, and T follicular helper cells, activated CD4? T helper cells release pro-inflammatory cytokines (such IFN-γ, IL-17, and IL-21) that attract B cells, neutrophils, and macrophages to the site of inflammation [31]. Target cells are directly lysed by CD8? cytotoxic T lymphocytes via the Fas–Fas ligand–mediated apoptosis and perforin–granzyme pathways [32].
3. The generation of autoantibodies and B-cell activation Activated by T helper cells, autoreactive B cells produce autoantibodies against self-antigens after clonally expanding and differentiating into plasma cells. Acetylcholine receptor antibodies in myasthenia gravis are an example of how these autoantibodies might neutralize or block receptors. Form immunological complexes that activate complement by depositing in tissues (e.g., lupus nephritis) Encourage phagocytosis and opsonization [33].
4. Activation of complement- When autoantibodies attach to self-antigens, the classical complement system is activated, producing membrane attack complexes and inflammatory mediators (C3a, C5a) that cause direct harm to host cells [34].
5. Inflammation induced by cytokines- TNF-α, IL-1β, IL-6, and IL-17 are examples of cytokines that are essential for promoting tissue damage, enlisting immune cells, and intensifying inflammatory cascades. A self-sustaining inflammatory cycle is produced by this "cytokine storm" [35].
6. Fibrosis and tissue damage- Chronic inflammation causes irreversible tissue damage and organ failure by triggering fibroblast activation, oxidative stress, and the release of proteolytic enzymes [36].
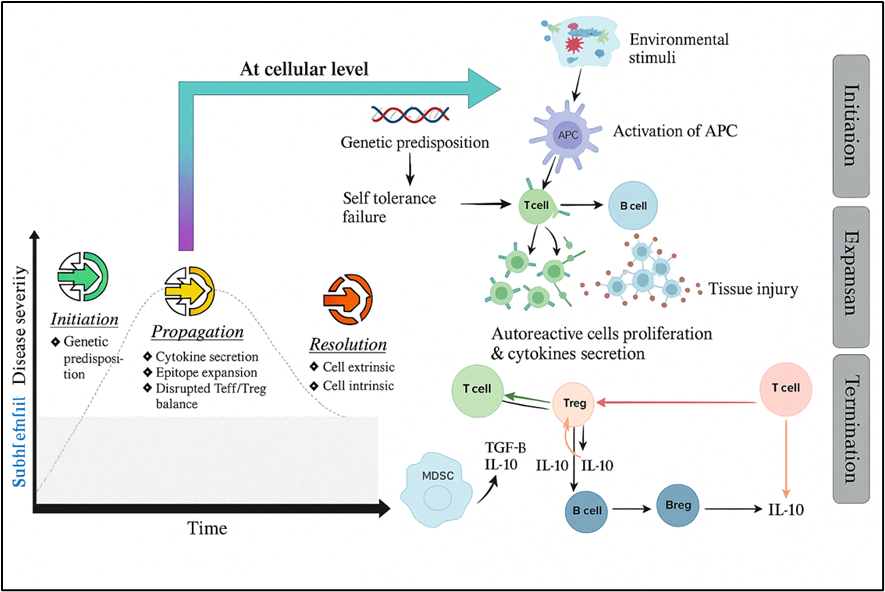
Figure 2: "Cytokine–Cell Interaction in Autoimmune Pathogenesis".[62]
5. DIAGNOSIS
Autoimmune disorders are difficult to diagnose because of their varied disease course, overlapping symptoms, and diverse clinical presentations. Clinical assessment, laboratory tests, imaging methods, and histological confirmation are all necessary for a precise diagnosis [37].
1. Clinical evaluation
A thorough patient history, including the beginning of symptoms, a family history of autoimmune diseases, and any possible environmental exposures, is the first stage in the diagnosing process. The goal of a physical examination is to find systemic or organ-specific indicators of inflammation, such as glandular enlargement, joint swelling, rash, or neurological impairments. [38].
2. Examination in a lab
A key component of diagnosing autoimmune diseases is autoantibody profiling. Antinuclear antibodies (ANA) for systemic lupus erythematosus, anti-thyroid peroxidase (anti-TPO) antibodies for autoimmune thyroiditis, and rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) for rheumatoid arthritis are examples of common markers [39]. In immune-complex-mediated illnesses such lupus nephritis, complement levels (C3, C4) are frequently decreased [40]. Although they are nonspecific, inflammatory indicators such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) aid in the monitoring of systemic inflammation [41].
3. Imaging methods
In order to identify demyelinating lesions in multiple sclerosis, magnetic resonance imaging (MRI) is crucial [42]. Computed tomography (CT) and positron emission tomography (PET) scans can identify organ involvement in systemic illnesses, whereas ultrasound and Doppler imaging help assess synovial inflammation in rheumatoid arthritis [43].
4. The study of histopathology
In some circumstances, tissue biopsies offer conclusive proof. For instance, a small salivary gland biopsy can diagnose Sjögren's syndrome, and a renal biopsy in lupus nephritis indicates immune complex accumulation [44].
5. New diagnostic instruments
The use of flow cytometry, multiplex autoantibody assays, and genetic testing for HLA typing to predict disease risk is a result of advancements in molecular diagnostics. For early identification and prognosis, biomarkers such microRNA signatures and cytokine profiles are being investigated [45].
6. TREATMENT
The goal of autoimmune disease treatment is to
(a) Manage symptoms and acute inflammation; (b) avoid irreparable tissue damage; and (c) alter the course of the disease by focusing on the immune system's underlying mechanisms. In addition to widespread immunosuppression and symptomatic treatments, other therapeutic options include small molecule inhibitors, highly targeted biologics, cell-based "immune-reset" techniques, and experimental antigen-specific tolerance therapies [46].
Table 1: Types of medicinal substances used to treat autoimmune disorders and how they work
|
Sr. No. |
Category |
Examples |
Mechanism of Action |
References |
|
1 |
Corticosteroids |
Prednisolone, Dexamethasone |
Inhibit pro-inflammatory cytokine production, reduce immune cell activation, and suppress antigen presentation |
66,67 |
|
2 |
DMARDs (Disease-Modifying Anti-Rheumatic Drugs) |
Methotrexate, Leflunomide |
Modulate immune cell proliferation, inhibit folate-dependent enzymes, and suppress pro-inflammatory pathways |
68,69 |
|
3 |
Biologics |
Adalimumab, Infliximab |
Neutralize cytokines such as tumor necrosis factor-α (TNF-α) to reduce inflammation and tissue damage |
70,71 |
|
4 |
Immunosuppressants |
Azathioprine, Cyclosporine |
Broad inhibition of lymphocyte proliferation via purine synthesis interference or calcineurin inhibition |
72,73 |
|
5 |
Targeted Therapies |
Fingolimod, Ocrelizumab |
Modulate lymphocyte trafficking (S1P receptor modulation) or deplete B-cells (anti-CD20 monoclonal antibodies) |
74,75 |
1. Principles of therapy
The kind of disease (organ-specific vs. systemic), severity (mild to life-threatening), organ or organs affected, comorbidities, pregnant status, and previous therapy response all influence the choice of treatment. Using the least effective immunosuppression, combining treatments when they work well together (such as steroid taper + DMARD), and closely monitoring for infections, cancer, and drug toxicity are general guidelines. [46] [47].
2. Symptomatic & supportive treatments
For discomfort and mild inflammation (such as osteoarthritic symptoms or small flare-ups of RA), NSAIDs and analgesics are prescribed. not able to change a sickness. Occupational therapy, physical therapy, and lifestyle choices, such as exercise, quitting smoking, protecting joints, staying vaccinated, and maintaining bone health (calcium/vitamin D, bisphosphonates when necessary). These actions lessen problems and incapacity. (Guides and evaluations that provide a summary of general management principles). [46] [48]
3. Glucocorticoids (GCs)
Role: Quick management of flare-ups and inflammation in a variety of AIDs (e.g., SLE, RA, vasculitis).
Mechanism: Reduced antigen presentation, leukocyte trafficking inhibition, and genomic and non-genomic suppression of cytokine synthesis.
Use: Oral taper to maintenance/lowest effective dose after receiving pulses for severe organ-threatening illness (e.g., methylprednisolone IV 250–1000 mg ×1–3 days).
Risks/monitoring: Prophylaxis (bone protection), glucose/blood pressure monitoring, steroid-sparing techniques, infection, osteoporosis, hyperglycemia, and adrenal suppression. [49] [50].
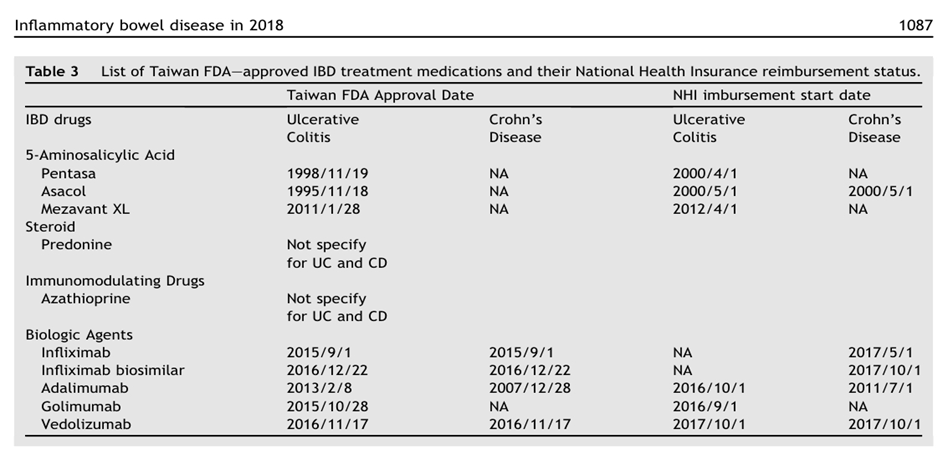
Table 2 lists the FDA-approved IBD therapy drugs in Taiwan together with the status of their National Health Insurance reimbursement. [63]
4. "Conventional DMARDs" or conventional immunosuppressants used to save steroids and sustain disease control. Methotrexate (MTX) is an antifolate that reduces the growth of lymphocytes and is an anchor medication in RA. Keep an eye on LFTs and CBC, and stay away during pregnancy. Azathioprine (AZA), a purine analogue, is used to treat autoimmune hepatitis, SLE, myasthenia gravis, and CBC, LFTs, and TPMT activities when available. Inhibiting IMP dehydrogenase, mycophenolate mofetil (MMF) is frequently used to treat organ-specific autoimmunity and lupus nephritis. It also monitors GI tolerance and CBC. Use MESNA and fertility counseling. Cyclophosphamide (CYC) is an alkylating drug that is only used for severe, organ-threatening conditions (such as severe lupus nephritis or vasculitis); hazards include infertility, hemorrhagic cystitis, and infection. Disease-specific functions of leflunomide, sulfasalazine, and hydroxychloroquine (e.g., leflunomide: RA; hydroxychloroquine: SLE maintenance). Baseline screening (infections, TPMT, hepatitis, TB) and periodic monitoring are necessary for these medications, which are well-established parts of regimens guided by guidelines. [46] [51]
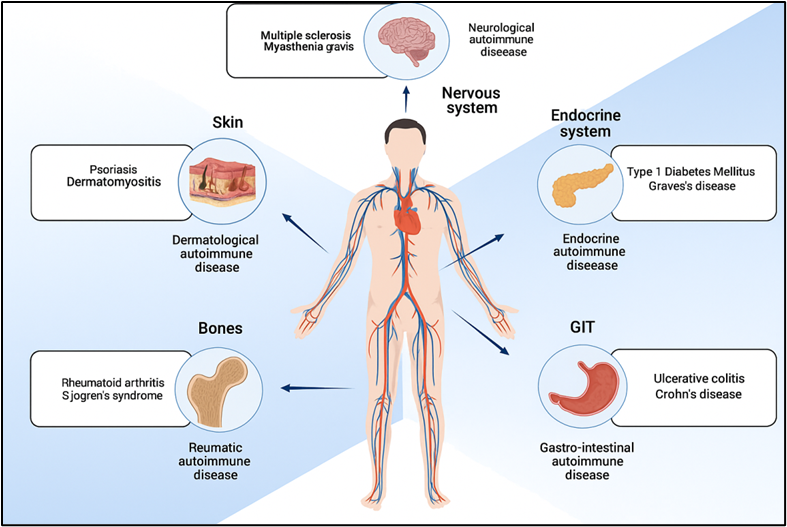
Figure 3: Overview of various autoimmune diseases categorized by affected body systems.[64].
5. DMARDs, or biologic disease-modifying agents
Biologics have transformed the treatment of various AIDS by targeting particular immune molecules and cells. Infliximab, etanercept, adalimumab, certolizumab, and golimumab are anti-TNF medications that inhibit tumour necrosis factor-α. They are very effective in treating psoriatic arthritis, RA, ankylosing spondylitis, and some vasculitis. Before using, check for latent TB and HBV. Anti-IL-6 receptor drugs (sarilumab, tocilizumab) inhibit IL-6 signalling, which is involved with giant cell arteritis and RA. Track neutrophil counts, LFTs, and lipids. B-cell depletion (rituximab; anti-CD20): depletes CD20? B cells; used in ANCA-associated vasculitis, pemphigus, RA that is resistant to TNF medications, some symptoms of SLE, and other B cell-mediated disorders. Important factors to take into account are the timing of vaccinations and the risk of infection (hypogammaglobulinemia). [52] [53].
Abatacept (CTLA4-Ig) is a costimulatory blocker that inhibits CD80/86-CD28 co-stimulation; it is used to treat RA and certain off-label autoimmune diseases. The newly targeted biologics, anti-BAFF (belimumab) and anti-type I IFN receptor (anifrolumab), have altered the paradigms of SLE care and are approved for use in SLE, including as an adjuvant for lupus nephritis in specific situations. These agents are now included in the list of suggested treatments for specific patients by guidelines bodies. [47] [54] Important rule of thumb: Modern guidelines for conditions like RA and SLE emphasize the early use of DMARDs and biologics as necessary to avert harm; the selection process is tailored to the comorbidities and disease profile. [46] [47]
6. Small molecule targeted therapies — JAK inhibitors & other kinase inhibitors
JAK inhibitors and other kinase inhibitors are small molecule targeted treatments. Oral inhibitors of the Janus kinase family, known as JAK inhibitors (tofacitinib, baricitinib, upadacitinib, and others), prevent downstream cytokine signalling, including GM-CSF, IL-6, and IFNs. approved for a number of indications, including psoriatic arthritis and RA. They can be used as substitutes for bDMARDs and are beneficial in patients who are not responding to biologics. [55]. Safety factors to consider: Regulatory bodies have released safety communications and label modifications due to the increased risk signal for serious infections, venous thromboembolism, herpes zoster reactivation, and cardiovascular events in specific populations; risk-benefit analysis is required (age, CV risk, past malignancy). Track LFTs, lipids, and CBC. [55] [56].
7. Complement & pathway-specific inhibitors
Inhibitors specific to certain pathways and complement blocking for complement-mediated disorders, such as paroxysmal nocturnal hemoglobinuria, is provided with eculizumab/ravulizumab (anti-C5), which is also being investigated more and more in some autoimmune situations. Although complement inhibitors have the potential to change lives, they also entail a danger of meningococcal infection; vaccination is necessary. [57]
8. "Immune-reset" and cellular treatments
Autologous hematopoietic stem cell transplantation (AHSCT) involves "rebooting" the immune system by first undergoing intense immunoablation and then rescuing stem cells. Although AHSCT carries significant short-term risks (infection, treatment-related mortality) and is only used for carefully chosen, refractory cases under specialized centres/clinical trials, it has demonstrated long-lasting remissions in refractory autoimmune diseases (such as severe multiple sclerosis and systemic sclerosis) [58][59].
CAR-T and modified cell therapies are promising, but experimental and safety/long-term data are still pending. Emerging early-phase data target autoreactive B cells (e.g., BCMA, CD19 CAR-T) for refractory autoimmune illness. [59]
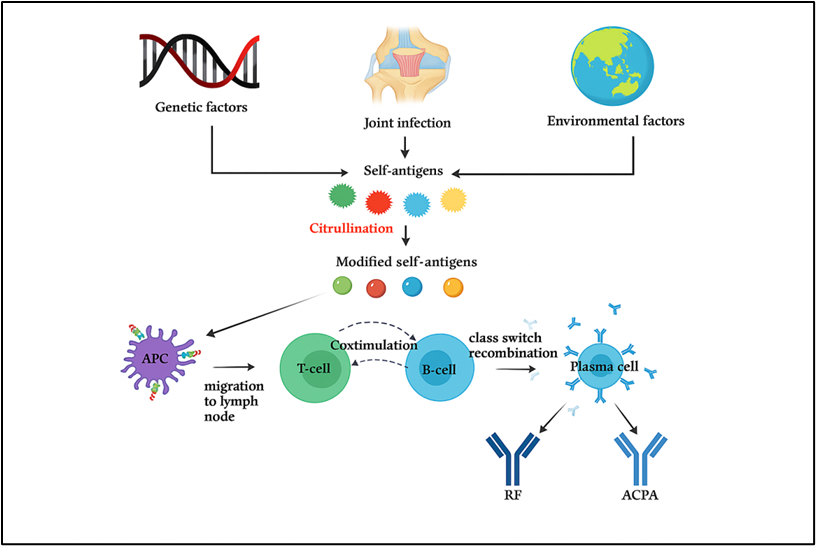
Figure 4: Pathophysiological mechanism of rheumatoid arthritis showing genetic and environmental factors leading to citrullination, activation of immune cells, and production of autoantibodies (RF and ACPA).[65]
9. Strategies that induce tolerance and are specific to antigens (future directions)
The goal of antigen-specific immunotherapies, which include tolerogenic dendritic cells, peptide/protein tolerogens, nanoparticle-based delivery, and AAV/mRNA tolerance platforms, is to create immune tolerance to autoantigens that cause disease without causing widespread immunosuppression. Although translational developments (nanoparticles, mRNA) and early clinical research (T1D, MS, celiac disease models) show promise, widespread clinical use is still being developed. Through the restoration of antigen-specific peripheral tolerance, these offer a possible "curative" approach. [60] [61]
10. Combination strategies & treatment sequencing
Sequencing of treatments and combination tactics Steroid tapering and improved results can be achieved by combining medicines with diverse mechanisms (e.g., GC induction + standard DMARD + targeted biologic). Strong agents (CYC, high-dose GC, or biologics) are often used to induce organ-threatening diseases, and then MMF, AZA, or belimumab are used for maintenance (e.g., lupus nephritis algorithms). Disease-specific sequencing and combinations are provided by guidelines. [47] [54]
11. Safety monitoring, vaccination, and infection risk mitigation
HIV, TB (IGRA/chest X-ray), hepatitis B/C serology, and vaccination status (avoid live vaccines when immunosuppressed) are baseline screenings prior to targeted therapy. Vaccination: inactivated vaccines (COVID-19, pneumococcal, and influenza) are advised; vaccinations should be timed in accordance with B-cell depletion or the start of JAK inhibitors. Long-term surveillance includes checking for cytopenias, LFTs, lipids, and infection symptoms, as well as screening for cancer if risk is high. For treatments (like JAK inhibitors) with established safety signals, shared decision-making about risks and benefits is crucial. [55] [56] [62]
12. Selecting therapy: useful factors
Disease activity and phenotype (organ-threatening vs. mild). Factors affecting the patient include age, desire to become pregnant, infections, concomitant cardiovascular disease, and previous cancer. Cost and accessibility: biosimilars can increase accessibility, while biologics and HSCT require a lot of resources. Control of symptoms, damage avoidance, steroid sparing, and, if possible, induction of long-term remission or tolerance are the objectives.
SUMMARY
With rapidly developing cellular and antigen-specific techniques, therapeutics for autoimmune disorders currently range from nonspecific immunosuppression to highly focused biologic and small molecule medicines. The focus of modern guideline-based care is on early, mechanism-based therapy selection, careful safety monitoring, and the creation of medicines that restore tolerance, which could eventually shift the paradigm of treatment from control to cure. [46][47][55][58][60].
CONCLUSION
Immune system abnormalities, environmental triggers, and genetic predispositions all contribute to autoimmune illnesses. These illnesses remain provide significant hurdles for diagnosis, treatment, and long-term management, despite great advancements in scientific understanding of their underlying causes. With fewer adverse effects than conventional immunosuppressants and improved symptom and disease progression control, tailored biologic treatments and innovative small-molecule medications have revolutionized therapy approaches.
The variety of disease presentations, variations in how each person reacts to treatment, and the possible dangers of long-term immune suppression continue to be significant barriers in spite of recent advancements. Improving quality of life and preventing permanent organ damage can be achieved by early diagnosis made possible by enhanced biomarker detection and advanced imaging.
It is anticipated that future management approaches would place a strong emphasis on personalized medicine, in which a patient's distinct genetic, molecular, and clinical profile will inform therapy choices. Curative medicines could be developed as a result of research into immunological tolerance restoration, which would move the emphasis from managing symptoms to actually curing the disease. Reducing the burden of autoimmune disorders and enhancing patient outcomes globally will require a cooperative, multidisciplinary approach that integrates clinical care, laboratory research, and patient education.
REFERENCES





Khushbu Shah, Shruti Rathod, Siya Patel, Shruti Rajput, Kajal Vable, Immunopathology and Therapeutic Strategies in Autoimmune Diseases: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 321-335. https://doi.org/10.5281/zenodo.17046807
 10.5281/zenodo.17046807
10.5281/zenodo.17046807