1,2,3,4Department of Pharmacy Practice, Oxbridge College of Pharmacy, Bangalore.
5,6Department of Internal Medicine, Aster CMI Hospital, Hebbal, Bangalore.
7Department of Clinical Pharmacology, KIMS Hospital, Bangalore.
Stevens–Johnson Syndrome (SJS) is a severe, life-threatening mucocutaneous adverse drug reaction, usually caused by drugs like antiepileptics. We present a case of a 31-year-old Indian woman with epilepsy, who had been well-controlled on levetiracetam and oxcarbazepine since 2015, presenting with SJS due to an increase in the dose of lamotrigine. Upon a dose escalation of 50 mg to 75 mg per day, she developed fever, redness and burning in both eyes, painful oral ulcers, crusted lips, and erythematous rashes covering about 20–30% of the body surface area. Laboratory results were only mildly hyponatremic, while cultures were negative. Skin biopsy demonstrated extensive keratinocyte necrosis and basal vacuolar degeneration, securing lamotrigine-induced SJS. Lamotrigine was promptly withdrawn, and the patient was treated with intravenous immunoglobulin, corticosteroids, cyclosporine, antihistamines, and supportive care, leading to progressive recovery and discharge after stabilization. This case highlights the necessity for careful lamotrigine titration, prompt detection of manifestations of hypersensitivity, and timely drug withdrawal in order to avoid serious complications and enhance clinical outcome.
Stevens-Jhonson syndrome (SJS) is a rare but life-threatening condition marked by severe mucocutaneous reaction which includes widespread necrosis and detachment of the epidermis.[1] Stevens-Johnson syndrome is mediated by cytotoxic T lymphocytes and natural killer (NK) cells, which release cytotoxic molecules that cause widespread death of keratinocyte which leads to disengagement of epidermal tissue.[2] The condition occurs due to Type IV hypersensitivity reaction with a complex etiology arise from variety of causes. It can be medication related- common ones which cover Sulfonamides, antiepileptics, allopurinol and non-steroidal anti-inflammatory drugs. (NSAIDs).[3]
Steven-Johnson Syndrome (SJS) presents with unspecific symptoms like blistering or shedding of the skin. Toxic Epidermal Necrolysis (TEN) is the most severe form which indicates drug induced skin reaction and it includes denudation of more than 30% of total Body Surface Area (BSA). Steven-Johnson Syndrome affects less than 10% area whereas involvement of 10-30% is called Toxic Epidermal Necrolysis (TEN) overlap.[4] Steven-Johnson Syndrome (SJS) is a rare but has severe side effects of commonly administered antiepileptic drugs. Most of SJS reaction occur within two months of administration of the particular drugs but in some cases it can occur after several months of the drug administration. In some cases it has been seen that reintroduce of higher dose can increase the risk of SJS.[5] Lamotrigine is an antiepileptic drug which belongs to phenyltriazine class that indicated for focal and generalised seizure in epileptic patients as well as monotherapy or adjunctive treatment for bipolar disorder.[6]
Lamotrigine has multiple mechanism of action that results anti-seizures properties as well as psychotropic effects. The precise mechanism through which lamotrigine produces its antiepileptic and mood-stabilizing effects has not been fully clarified. Its primary antiepileptic action is believed to involve use-dependent inhibition of neuronal voltage-gated sodium channels. By blocking these channels, lamotrigine helps stabilize neuronal membranes and reduce presynaptic release of the excitatory neurotransmitter glutamate, thereby preventing seizure generation. This sodium channel blockade occurs predominantly during periods of excessive neuronal firing, such as seizure activity, which minimizes adverse effects under normal physiological conditions. Interestingly, lamotrigine demonstrates a broader spectrum of antiseizure efficacy than other sodium channel blockers like phenytoin, though the reason for this difference remains uncertain.[7]
In addition, lamotrigine has been shown to enhance the release of gamma-aminobutyric acid (GABA), the principal inhibitory neurotransmitter in the central nervous system. Although this GABAergic effect is relatively modest, it is not dependent on neuronal firing frequency, meaning it occurs outside of seizure activity. This property may partially explain lamotrigine’s psychotropic and mood-stabilizing effects.[8] Lamotrigine also exerts a weak inhibitory action on voltage-gated calcium channels, which could be relevant given the association between calcium channel modulation and mood regulation in bipolar disorder. Other pharmacological effects include mild inhibition of 5-HT? receptors and in vitro inhibition of dihydrofolate reductase, though their clinical significance is uncertain. Furthermore, lamotrigine is thought to possess anti-kindling properties, potentially reducing neuronal hypersensitivity over time. However, findings from animal studies have been inconsistent, and the relevance of these results to human epilepsy remains unclear.[8]
Lamotrigine can cause ADR like severe cutaneous reaction.The main features of severe cutaneous drug reactions, such as dosage, onset, and concomitant Valproic Acid(VPA) use which do not differ in patients with Lamotrigine-induced SJS or TEN. SJS or TEN may also be the cutaneous manifestations of LTG-induced Anticonvulsant Hypersensitivity Syndrome(AHS). induced cutaneous adverse reactions and the relative risk compared with other AEDs.[9]
Case Presentation:
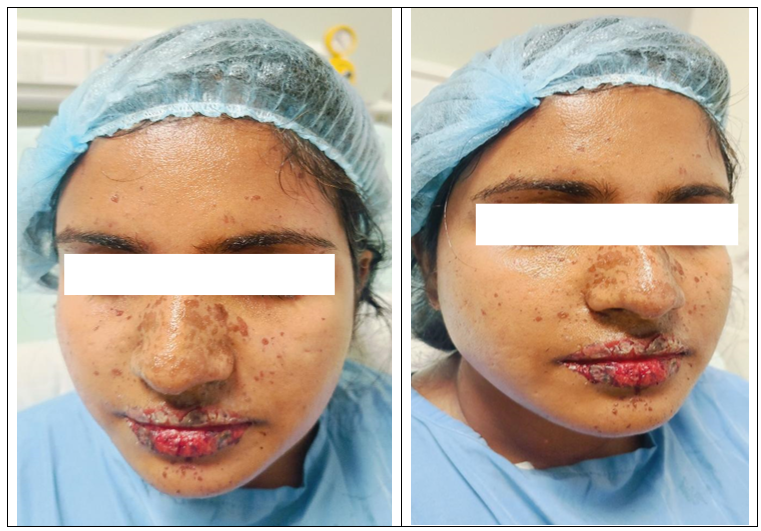
A 31 year old Indian female presented in our hospital with complaints of redness and burning sensation over both eyes since 2 days and blisters in mouth since 1 day. On hospital visit time crusts over lips was observed as well as multiple bullae inside the mouth. On admission she was febrile and hypotensive hence antipyretic and fluid bolus given. Upon examination redness and discharge was there from both eyes, redness in20-30% body surface area. she was conscious and oriented, her heart rate & respiratory rate also normal and SpO2 was 96% at room air. She was diagnosed with Epilepsy and on medication since 2015. She was taking levetiracetam and oxcarbazepine since 2015 for the treatment of Epilepsy. Recently she has Initiated lamotrigine 25?mg daily, after a week the dose was increased to 50 mg daily. Based on her clinical condition the dose was increased to 75 mg per day after one week of 50 mg daily dose. After 1 day of taking this dose the patient developed all the symptoms. The patient was investigated for the cause and common reports on day 1 (table 1). In the view of steven johnson syndrome she was admitted to ICU. Blood and Urine culture was negative, IgG was high & Skin biopsy shown steven johnson syndrome to Lamotrigine. Hence the medication was stopped.
Table 1
|
Lab Parameters (Normal Range) |
D1 |
D2 |
D3 |
D6 |
|
Hb (12-15 g/dl) |
12.6 |
11.7 |
10.6 |
12.9 |
|
Total WBC (4-11 K/uL) |
12 |
5.28 |
10.37 |
8.69 |
|
Platelet (150-400 K/uL) |
147 |
216 |
107 |
289 |
|
Creatinine (mg/dl) |
0.64 |
0.58 |
0.47 |
0.55 |
|
Sodium(135-145 mmol/L) |
127 |
128 |
130 |
126 |
|
Potassium(3.5-5.5 mmol/L) |
4.34 |
4.41 |
4.29 |
4.76 |
|
Total bilirubin (0.3-1.2 mg/dl) |
0.28 |
0.24 |
0.34 |
0.62 |
|
Sg0t (<32 U/L) |
24 |
20 |
14 |
22 |
|
Sgpt (<33 U/L) |
21 |
39 |
26 |
27 |
|
Prothrombin time (11-13.5 Sec) |
13.1 |
|
|
|
|
INR (0.8-1.2) |
0.98 |
|
|
|
|
ESR (0-30 mm/hour)) |
4 |
|
|
|
D: Day; Hb: Hemoglobin; WBC: White Blood Cell; SGOT: serum glutamate oxaloacetate transaminase; SGPT: serum glutamate pyruvate transaminase; INR: International Normalized Ratio; ESR: Erythrocyte sedimentation rate
On the view steven johnson syndrome, in ICU she was treated with IVIg 2g/kg STAT over 24 hours, hydroxyzine hydrochloride 1cc 4mg, Cyclosporine 100mg, prednisolone 20 mg, ointments and eye drops. Clobazam 10 mg was started to treat the seizure. Her sodium level was low which was treated with Sodium bicarbonate 500 mg. Her clinical features are shown on table 2. She was improving symptomatically hence she was shifted to wards on day 4. Her Old lesions were healing, face lesions are reduced, eyes - redness reduced hence she was started on soft diet orally. Vitals and lab parameters were monitored in the wards. As the patient improved symptomatically and was hemodynamically stable, patient was discharged with iv antihistamines, oral anti-epileptics, oral steroids and eye drops.
Table 2: Clusters over the lips.
HISTOLOGICAL FINDINGS:
Table-3:
|
Specimen |
Skin biopsy taken from face and soles |
|
MICROSCOPY |
There is a presence of neutrophils, scattered melanophages, necrotic keratinocytes, and extensive death of keratinocytes along with basal vacuolar degeneration. Lymphocytic and neutrophilic exocytosis is also observed. |
|
IMPRESSION |
The clinical features are suggestive of Steven-Johnson-Syndrome |
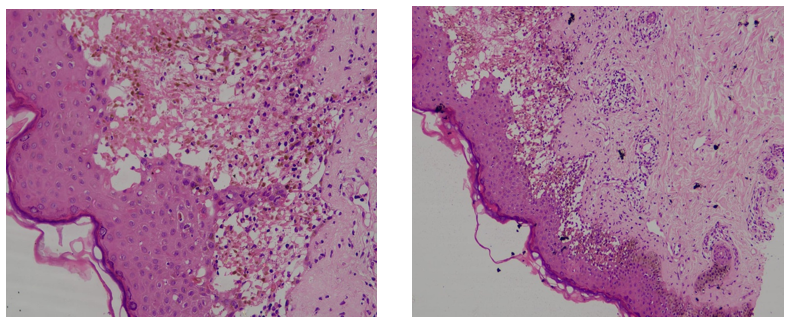
Fig.2. Lesional bulla, Perilesional area: - Features are separation of epidermis from the dermis, presence of neutrophils, scattered melanophages, necrotic keratinocytes, and extensive death of keratinocytes along with basal vacuolar degeneration, favoring Steven-Johnson-Syndrome
DICUSSION:
Both toxic epidermal necrolysis (TEN) and drug-induced Stevens-Johnson syndrome (SJS) are severe cutaneous adverse reactions that are not immunoglobulin E-mediated and carry a significant risk of morbidity, mortality, and negative effects on physical and mental health. Human leukocyte antigen (HLA)-specific genotypes, ethnicities, and several high-risk medications are linked to these. HLA class I: limited. In SJS/TEN, tissue-level oligoclonal CD8 cytotoxic T-cell responses take place. T effector chemicals granzyme B, perforin, granulysin, gamma interferon, tumor necrosis factor-alpha, and lipocalin-2 cause keratinocyte apoptosis, or cell death, which is mediated by cytotoxic T cells. Clinically, SJS/TEN is characterized by fever, at least two ocular, oral, or vaginal mucosal involvements, and a positive Nikolsky sign with epidermal detachment.[10]
Here, a 31-year-old woman with a long-standing history of epilepsy developed SJS within a short time of the dose increase of lamotrigine. The chronology of onset of symptoms after dose increment, coupled with clinical presentation—mucosal involvement, ocular manifestations, febrile illness, and erythematous rash on about 20–30% of body surface area—was strongly indicative of SJS. This was confirmed by skin biopsy results and the absence of infection etiologies (negative blood and urine cultures). Significantly, the patient had tolerated levetiracetam and oxcarbazepine well for many years, with lamotrigine recently added. The fast development of symptoms following dose escalation is a testament to the significance of careful titration and monitoring during initiation of lamotrigine, since rapid uptitration has been reported as a risk factor for SJS. Management here consisted of immediate discontinuation of lamotrigine and institution of supportive treatment in the ICU, namely IV immunoglobulin (IVIg), systemic corticosteroids, cyclosporine, symptomatic therapy for mucocutaneous lesions, and eye care. Her gradual recovery and stabilization over a few days and subsequent readiness for oral intake and discharge reinforce the value of early detection and intervention in enhancing outcomes.
This case highlights the urgent importance of monitoring for initial warning signs of hypersensitivity reactions in patients initiated on lamotrigine, particularly during dose escalation periods, and educating patients to report such symptoms promptly.
CONCLUSION:
This case highlights the severe potential of Stevens-Johnson Syndrome (SJS) caused by lamotrigine, especially in the early period of dose escalation. Early detection of symptoms, withdrawal of the causative drug at once, and early institution of intensive supportive measures are invaluable in the recovery of patients. Physicians need to take precautions in prescribing lamotrigine, following slow titration regimes, and informing patients about the appearance of early signs of drug-induced adverse reactions. Prompt diagnosis and management can considerably decrease morbidity and enhance clinical results in SJS caused by drugs.
ACKNOWLEDGMENT: The authors are thankful to Dr. Brunda MS and Dr. Jagadeesh for their kind guidance and support in case diagnosis and management. The authors also extend their heartfelt gratitude to Dr. Praveen Kumar for his help and valuable suggestions in shaping and preparing the manuscript.
Conflict Of Interests: There is no conflict of interests.
REFERENCES

Biswajit Haldar*, Aniket Saha, Gounak Sankar Mal, Shaikh Ashfaq Ashraf, Brunda M. S., K. Jagadeesh, Praveen Kumar, Lamotrigine Induced Stevens Johnson Syndrome (SJS) – A Rare Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 37-42 https://doi.org/10.5281/zenodo.17499545
 10.5281/zenodo.17499545
10.5281/zenodo.17499545
