1,3 Ashokrao Mane College of Pharmacy, Shivaji University, Kolhapur, India
2 D.Y. Patil College of Pharmacy, Kolhapur, India
Buccal drug delivery refers to the administration of medications through the buccal mucosa, the inner lining of the cheek. Owing to its relatively high permeability and rich vascular supply, the oral mucosa offers a unique and effective route for both local and systemic drug delivery. This route allows drugs to be absorbed directly into the systemic circulation while avoiding degradation in the gastrointestinal tract and hepatic first-pass metabolism. This review provides a functional foundation for buccal drug delivery by outlining the anatomical and physiological characteristics of the oral mucosa, the mechanisms governing drug permeation, and the experimental techniques used to evaluate buccal formulations. In addition, it examines the concept of mucoadhesion, including its advantages, limitations, and theoretical basis, and presents an overview of commonly employed mucoadhesive polymers, their methods of preparation, and the different categories of buccal drug-delivery systems. The development of advanced drug-delivery strategies, particularly mucoadhesive systems, has demonstrated significant potential to enhance therapeutic performance. By adhering firmly to the mucosal surface, the primary site of drug absorption, these systems allow controlled and localized drug release. This targeted delivery approach improves bioavailability while supporting both local therapeutic effects and systemic drug absorption. Mucoadhesion has been explained through several theoretical models, including electronic, adsorption, wetting, diffusion, fracture, and mechanical theories. Although numerous in vitro and in vivo techniques are available to study mucoadhesive behavior, the underlying mechanisms are still not fully understood. This review aims to consolidate current knowledge by discussing widely used mucoadhesive polymers, evaluation methodologies, and prevailing theories that describe mucoadhesion in pharmaceutical drug-delivery systems. The growing demand for patient-friendly dosage forms has further accelerated interest in innovative drug-delivery technologies that improve safety, convenience, and therapeutic efficacy. Among these, buccal films have emerged as a
To overcome the limitations associated with poor gastrointestinal absorption, increasing attention has been directed toward alternative routes of drug administration. Buccal drug delivery, particularly through bioadhesive dosage forms, has emerged as an effective and patient-friendly approach. Several therapeutic agents have already been successfully administered systemically via this route. Delivery through the buccal mucosa enables drugs to bypass degradation in the gastrointestinal tract and hepatic first-pass metabolism. An additional safety advantage of this route is the ease with which the dosage form can be removed from the cheek in the event of an adverse reaction, allowing rapid cessation of further drug absorption.
The buccal mucosa possesses several anatomical and physiological features that make it well suited for drug delivery. A dense vascular network within the lamina propria facilitates rapid transport of absorbed drug into the systemic circulation, while the consistently moist environment of the oral cavity promotes quick drug dissolution and efficient permeation. Although the general structure and function of the oral mucosa are well characterized, age-related changes, including variations in salivary secretion and mucosal integrity, may influence adhesion, residence time, and drug-release behavior of buccal formulations.
Compared with many commercially available orally disintegrating tablets, which often require specialized packaging due to their fragility, buccal films are less brittle and easier to handle. Mucoadhesive buccal films offer further advantages by adhering directly to the mucosal surface, thereby maintaining close and prolonged contact with the primary absorption site. Depending on formulation design, these systems can be tailored for either local or systemic drug delivery. For example, mucoadhesive films have been developed for targeted local delivery of antifungal agents in the treatment of oral candidiasis.
Bioadhesion broadly describes the attachment between a material and a biological surface, whereas mucoadhesion specifically refers to adhesion to mucosal tissues. Despite growing clinical and commercial interest, achieving consistent product quality remains a significant challenge in buccal film development. Addressing this challenge requires systematic formulation optimization, continuous performance evaluation, and a thorough understanding of the physicochemical and mechanical properties that govern film behavior.
1.2 Buccal Mucosa [14-27]
In contemporary drug-delivery research, the oral route remains highly preferred by both patients and clinicians because of its convenience and broad acceptance. However, conventional oral administration is associated with significant limitations. Many therapeutic agents, particularly peptides and protein-based drugs, exhibit poor bioavailability due to extensive first-pass hepatic metabolism and enzymatic degradation within the gastrointestinal tract. These challenges have driven growing interest in alternative delivery strategies that exploit mucosal surfaces for systemic drug absorption.
Compared with conventional oral administration, transmucosal delivery via the nasal, rectal, vaginal, ocular, or oral mucosa offers several advantages. These routes can bypass hepatic first-pass metabolism, reduce presystemic drug degradation, and in some cases provide a more favorable enzymatic environment for labile drug molecules, resulting in improved systemic exposure.
Within the oral cavity, transmucosal drug delivery is primarily achieved through buccal and sublingual routes. The buccal route, where the dosage form is placed against the inner cheek, is particularly suitable for controlled and sustained drug delivery. In contrast, the sublingual route enables rapid drug absorption and is typically employed when an immediate therapeutic effect is required, such as in the management of angina pectoris.16
Structure of oral mucosa
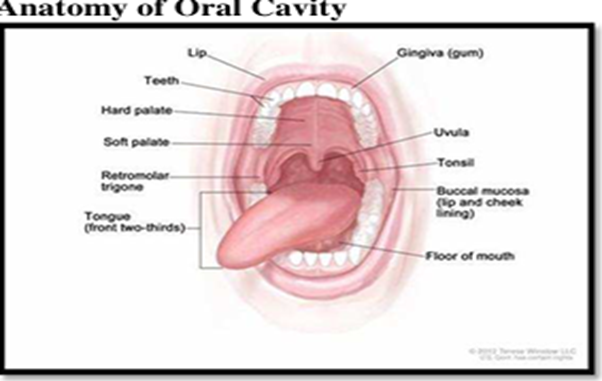
Fig.No.1 Structure of Oral Cavity
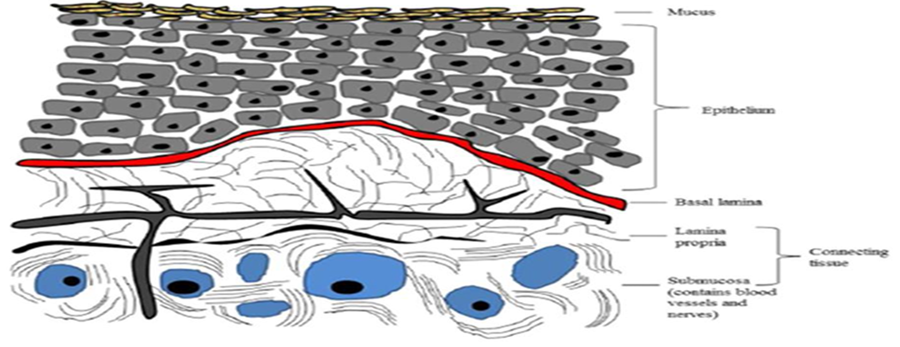
Fig.No.2 Structure of Oral mucosa
The mucus layer is the primary biological component responsible for providing the adhesive interface in mucoadhesion. It is a translucent, viscoelastic secretion that forms a continuous gel-like coating over the mucosal epithelium. In humans, the thickness of this layer typically ranges from approximately 50 to 450 µm, depending on the dynamic balance between mucus secretion and its degradation or shedding. This thickness also varies across different anatomical sites.
Beyond its protective function, the mucus matrix facilitates cell–cell adhesion and acts as a natural lubricant, allowing epithelial surfaces to glide smoothly over one another. Owing to these properties, mucus plays a pivotal mediating role in the interaction between mucosal tissues and mucoadhesive drug-delivery systems.
Approximately 70% of salivary mucins in the oral cavity are secreted by the minor salivary glands. At physiological pH, mucus forms a cohesive gel that adheres strongly to epithelial surfaces. Chemically, mucus is composed predominantly of water, in which mucins and inorganic salts are dispersed. Mucins themselves consist largely of water (around 95%), along with smaller proportions of glycoproteins and lipids, mineral salts, and trace amounts of free proteins. The long carbohydrate side chains of mucins are responsible for the characteristic viscoelastic properties of mucus, imparting both elasticity and viscosity.
Collectively, the mucus layer serves multiple essential functions, including surface protection, lubrication, hydration, and acting as the primary interface for mucoadhesive interactions. These roles highlight its critical importance in the design, performance, and optimization of mucoadhesive drug-delivery systems.
The thickness of the epithelial lining varies markedly across different regions of the oral cavity, directly influencing permeability and drug transport. The epithelium lining the cheeks and gingiva is relatively thick, typically measuring between 200 and 500 µm, whereas the floor of the mouth is considerably thinner, with a thickness of approximately 100–200 µm. The superficial epithelial cells forming the barrier layer contain specialized intracellular organelles known as membrane-coating granules or lamellar granules, which are responsible for delivering lipid components specific to each tissue type.
Keratinized epithelium is enriched with non-polar lipids such as sphingomyelin and glucosylceramides, whereas non-keratinized epithelium contains a higher proportion of polar lipids, including glycosphingolipids, cholesterol, and cholesterol esters. Upon secretion, these lipids are deposited into the intercellular spaces of the upper epithelial layers, where they play a crucial role in regulating mucosal permeability. Consequently, the depth at which membrane-coating granules are present serves as a useful indicator for estimating permeability limits for drugs and other exogenous molecules.
Unlike the intestinal and nasal mucosa, the buccal epithelium lacks tight junctions. Instead, intercellular cohesion is maintained primarily through gap junctions, supported by structural elements such as desmosomes and hemidesmosomes. This distinct architectural arrangement contributes to the relatively high permeability of the buccal mucosa, which has been reported to be several-fold greater than that of the skin.
Permeability also varies among different oral regions. The thin, non-keratinized sublingual mucosa exhibits the highest permeability, followed by the thicker, non-keratinized buccal mucosa, while the heavily keratinized palatal mucosa shows the lowest permeability. Experimental studies indicate that the flattened superficial epithelial layer constitutes the principal barrier to the penetration of drugs, enzymes, antigens, and toxins, whereas the deeper submucosal layers offer comparatively less resistance to molecular transport.
Mucoadhesion is generally described as a two-stage process comprising an initial contact phase followed by a consolidation phase. During the contact phase, the mucoadhesive formulation is placed in close proximity to the mucosal surface, where it begins to hydrate, swell, and spread. This swelling increases the surface area of contact and facilitates intimate interaction with the mucus layer.
The consolidation phase is governed by the presence of moisture at the mucosal interface. Water acts as a plasticizer, softening the polymeric matrix and enhancing the mobility of polymer chains. Increased chain flexibility enables mucoadhesive polymers to interact with mucin through weak intermolecular forces, primarily hydrogen bonding and van der Waals interactions, thereby strengthening adhesive attachment.
Two principal theories are commonly used to explain the mechanisms underlying the consolidation phase. According to diffusion theory, polymer chains from the mucoadhesive system interpenetrate with the glycoprotein chains of mucus, leading to the formation of secondary bonds that stabilize adhesion. In contrast, the dehydration theory proposes that adhesive strength arises from the transfer of water between the formulation and the mucosal surface, resulting in closer contact and enhanced interfacial bonding.
Together, these complementary mechanisms contribute to the formation of a stable and sustained adhesive interaction between the dosage form and the mucosal tissue.
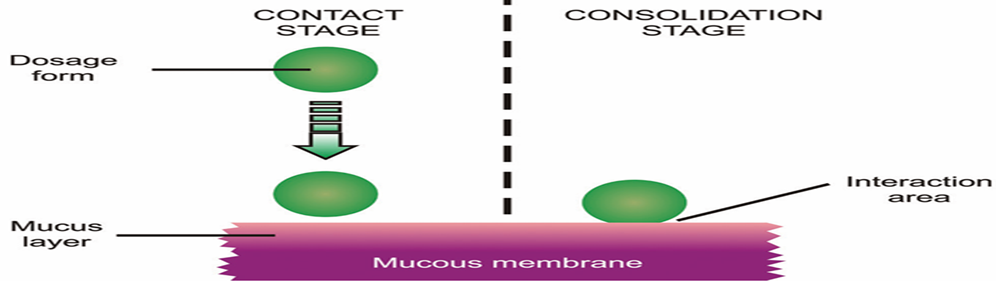
Fig. No. 3 Structure of Consolidation Stage
The dehydration theory proposes that certain mucoadhesive materials rapidly form a gel upon exposure to moisture. When such a formulation is applied to the mucosal surface, an osmotic gradient develops between the dosage form and the mucus layer. As equilibrium is approached, water is drawn from the mucus into the formulation in response to this gradient. This movement of water promotes intimate contact and intermixing at the interface, thereby increasing residence time and strengthening adhesive attachment.
According to this theory, the transfer of water—rather than direct interpenetration of polymer chains with mucin molecules—is the primary contributor to mucoadhesion. However, the dehydration mechanism does not apply to solid dosage forms or formulations that are already highly hydrated, as these systems lack the capacity to extract sufficient water from the mucosal surface to initiate or sustain adhesion.6-39
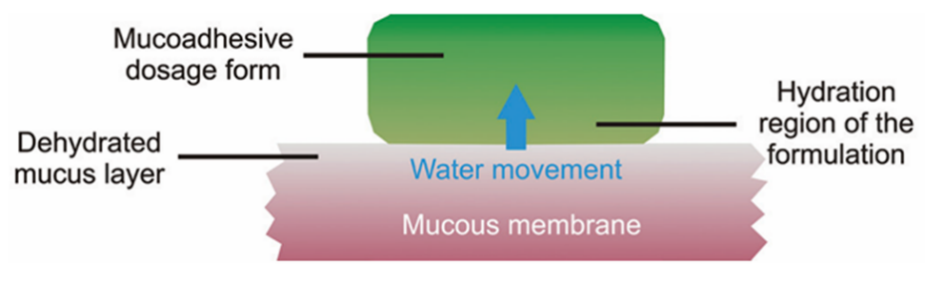
Fig.No.4 Structure of Dehydration Stage
Mucoadhesion has been described through six complementary scientific theories, each elucidating a specific mechanism or stage involved in the interaction between a mucoadhesive polymer and the mucosal surface. Rather than representing competing models, these theories describe distinct physicochemical events that may occur sequentially or simultaneously, collectively contributing to the formation and stabilization of the adhesive bond. The following sections outline these theories and discuss their relevance in understanding the complex and multifactorial nature of mucoadhesion.
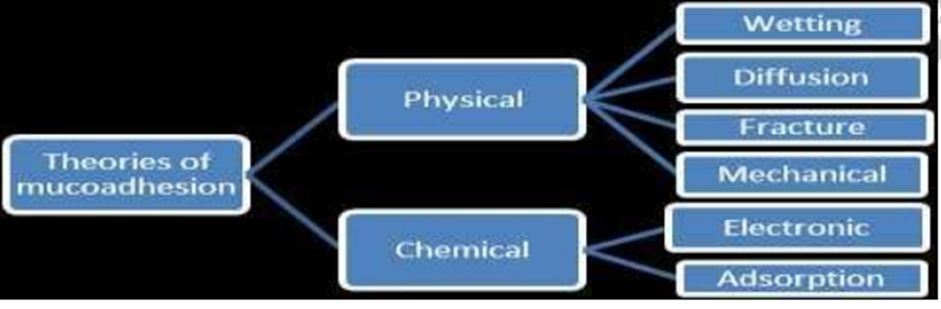
Fig.No.5 Theories of Mucoadhesion
4.1 Wetting Theory
Mucoadhesion is explained by six complementary theoretical models, each addressing a particular mechanism or stage in the interaction between a mucoadhesive polymer and the mucosal surface. These theories are not mutually exclusive; instead, they describe different physicochemical events that can occur either sequentially or in parallel, together leading to the development and stabilization of the adhesive bond. The following sections describe these theories and clarify their contribution to understanding the inherently complex and multifactorial process of mucoadhesion.
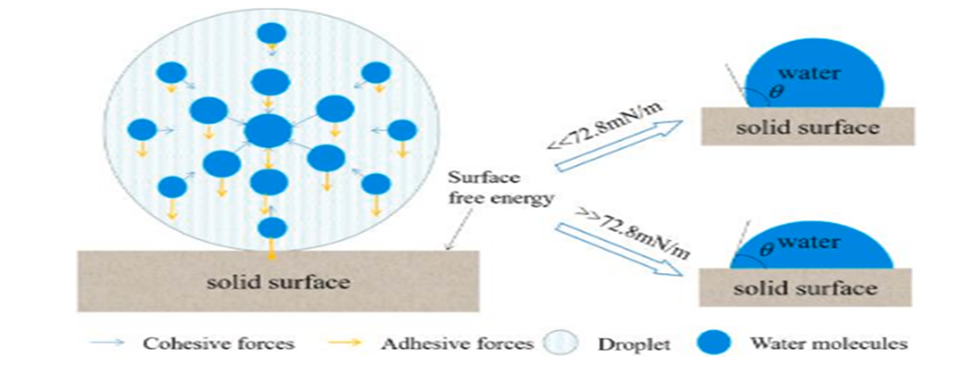
Fig.No.6 Wetting Theory
4.2 Adsorption Theory
This theory suggests that mucoadhesion arises from the formation of intermolecular interactions between the adhesive polymer and the mucus layer. After initial contact, adhesion is maintained primarily through non-covalent forces such as hydrogen bonding and van der Waals interactions. These attractive forces between polymer chains and mucin molecules stabilize the adhesive interface, enabling the mucosal surface to retain the dosage form at the site of application.
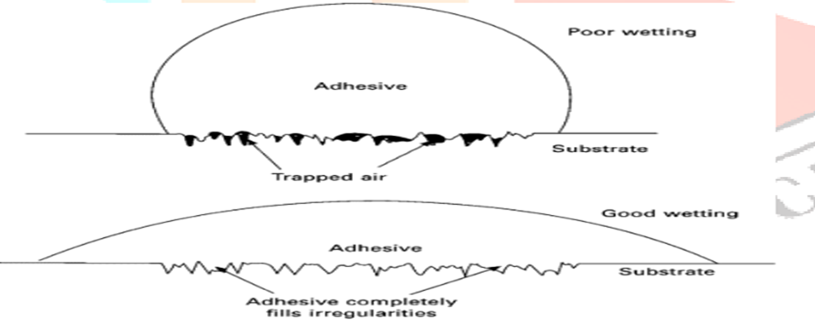
Fig.No.7 Adsorption Theory
4.3 Electronic Theory
According to this theory, mucoadhesion results from molecular-level interactions between the adhesive polymer and the mucus layer. Once contact is established, adhesion is sustained through weak intermolecular forces, predominantly hydrogen bonding and van der Waals interactions. These atomic-scale attractions between polymer chains and mucin molecules stabilize the interfacial region and maintain attachment between the two surfaces.
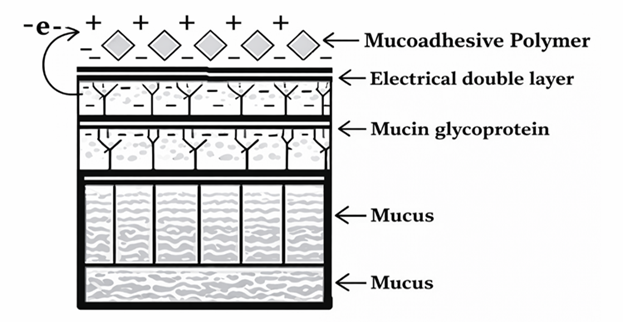
Fig.No.8 Electronic Theory
4.4 Mechanical Theory
According to this theory, mucoadhesion occurs when a mucoadhesive material penetrates and fills the microscopic grooves and surface irregularities of a rough mucosal surface. These structural features increase the effective contact area between the formulation and the mucosal tissue, allowing the material to anchor more firmly. The resulting mechanical interlocking strengthens adhesive attachment and contributes to prolonged retention at the site of application. The strength and stability of the adhesive bond.
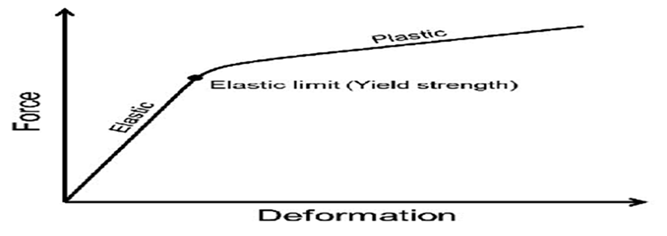
Fig.No.9 Mechanical Theory
4.5 Fracture Theory
This concept is based on the relationship between the force required to maintain adhesion between two surfaces and the force necessary to separate them. Mucoadhesive strength is quantified by measuring the mechanical force needed to detach a mucoadhesive polymer from the mucus layer. This approach allows mathematical estimation of detachment forces, providing a practical means to compare adhesive strength between different dosage forms and the mucosal surface.
According to this theory, adhesive failure occurs through crack formation and propagation at the interface, and the resistance of the adhesive bond to fracture determines mucoadhesive performance. The fracture strength (σ) is related to the critical crack length (L), Young’s modulus of elasticity (E), and the energy required for fracture.
In essence, this theory interprets mucoadhesion as the ability of the adhesive bond to resist mechanical separation.
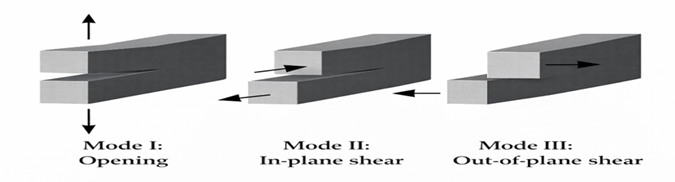
Fig.No.10 Fracture Theory
4.6 Diffusion Theory
According to this theory, mucoadhesion arises from the diffusion of polymer chains into the glycoprotein network of the mucus layer. The extent of this process is governed by the concentration gradient between the polymer and mucus, as well as the duration of contact. Diffusion occurs in two sequential stages. The first stage involves the formation of an interpenetration zone, where polymer chains and mucin molecules intermingle. The second stage leads to the development of stable adhesion, which is typically achieved when this interpenetrating layer attains a critical thickness of approximately 0.2–0.5 µm.
The formation and strength of the interpenetrating network are influenced by several factors, including polymer concentration, molecular weight, chain length, flexibility, and mobility. Collectively, these properties determine the ability of the adhesive polymer to penetrate the mucus matrix and establish a durable mucoadhesive bond.
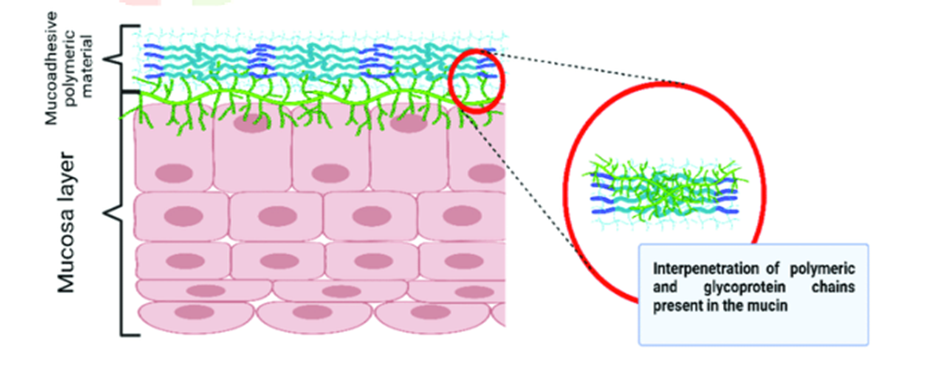
Fig.No.11 Diffusion Theory
5. MUCOADHESIVE POLYMER 47-54
Mucoadhesive polymers are characterized by a high density of hydrophilic functional groups, such as hydroxyl, carboxyl, amide, and sulphate moieties. These groups facilitate strong interactions with mucus and epithelial tissues through a combination of intermolecular forces. Their hydrophilic character also enables water uptake and swelling, which enhances polymer chain flexibility and exposes additional binding sites. This swelling promotes closer contact with the mucosal surface, leading to increased adhesive strength and prolonged residence time at the site of application.
6. FEATURES OF AN IDEAL MUCOADHESIVE POLYMER FOR DRUG DELIVERY:
An ideal mucoadhesive polymer should satisfy several key criteria. Both the polymer and its degradation products should be non-toxic, non-irritating, and should not be systemically absorbed. The material should be capable of forming strong yet reversible non-covalent interactions with mucus or epithelial surfaces and should adhere rapidly to moist tissues, preferably with a degree of site specificity. It must allow efficient drug incorporation without compromising drug release characteristics. In addition, the polymer should exhibit adequate physicochemical stability during processing, storage, and throughout the product’s shelf life. Finally, cost-effectiveness is an important consideration to ensure the affordability of the final dosage form.
7. CLASSIFICATION OF MUCOADHESIVE POLYMERS BASED ON ADHESION MECHANISM:
Mucoadhesive polymers can be broadly classified based on the nature of their interaction with mucosal tissues.
7.1 Non-specific, non-covalent interaction polymers adhere primarily through electrostatic forces. These interactions are reversible and play a key role in the initial attachment of the formulation to the mucosal surface.
7.2 Polymers containing hydrophilic functional groups exhibit mucoadhesion mainly through hydrogen bonding with biological substrates. Functional moieties such as hydroxyl, carboxyl, and amide groups enhance affinity for mucus and epithelial tissues by enabling the formation of multiple weak intermolecular bonds.
7.3 Receptor-specific binding polymers interact selectively with specific receptors present on mucus or epithelial cell membranes. This selective interaction enables targeted adhesion and can enhance localised or site-specific drug delivery.
Lectins are proteins or glycoproteins that specifically recognize and bind to carbohydrate residues on mucus or epithelial cell surfaces. Due to this selective binding capability, lectins have been widely investigated for targeted drug-delivery applications. Their ability to promote cellular adhesion, endocytosis, and transcytosis makes them particularly valuable for enhancing drug transport across mucosal barriers.
Thiolated polymers (thiomers) are hydrophilic macromolecules typically derived from polyacrylates or cellulose-based polymers and contain free thiol groups. These thiol groups form stable covalent disulfide bonds with cysteine-rich regions of mucin glycoproteins, resulting in prolonged mucosal residence time and improved bioavailability. In addition, thiomers enhance mechanical strength, swelling behavior, and water uptake, all of which contribute to more effective mucoadhesion.
Overall, both natural and synthetic polymers can function as mucoadhesive materials, depending on their chemical structure and the specific interaction mechanisms they employ.
8. MANUFACTURING METHODS OF BUCCAL FILMS [55-58]
Buccal films are commonly prepared using three principal methods: solvent casting, hot-melt extrusion, and direct milling. Among these, the solvent casting technique is the most widely employed due to its simplicity, reproducibility, and suitability for heat-sensitive drugs.
8.1. Solvent Casting Method
In the solvent casting method, the selected polymer is first dissolved in distilled water to obtain a uniform solution. The active pharmaceutical ingredient (API) is then incorporated, followed by the addition of a suitable plasticizer to improve film flexibility and mechanical strength. The mixture is stirred thoroughly until a homogeneous casting solution is formed. This solution is poured onto a flat surface, such as a Petri dish or casting plate, and dried in a hot-air oven at approximately 40 °C. After complete solvent evaporation, the formed film is carefully peeled from the surface and placed in a desiccator for 24 hours to remove residual moisture. The dried film is then cut into units of the required dimensions to deliver the desired drug dose.
Steps involved in the solvent casting technique:
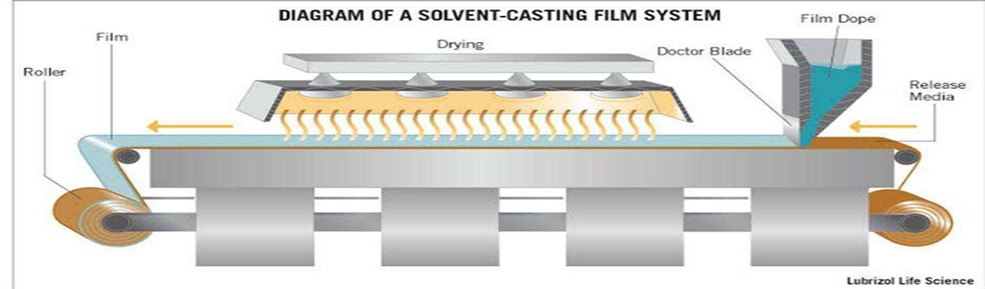
Fig.No.12 Solvent Casting Method
8.2. Hot-Melt Extrusion Method
In the hot-melt extrusion technique, the active pharmaceutical ingredient is uniformly blended with suitable excipients and subjected to controlled heating to form a homogeneous molten mass. This molten material is continuously forced through a die or orifice using an extruder, resulting in a uniform extrudate that can be shaped into solid dosage forms such as films, granules, or sheets.
Hot-melt extrusion is a solvent-free process, making it particularly advantageous for formulations containing drugs that are sensitive to organic solvents. The absence of solvents also eliminates the risk of residual solvent toxicity and simplifies regulatory compliance. Owing to these benefits, hot-melt extrusion has been widely explored in advanced drug-delivery systems, including buccal and transdermal applications.
Steps involved in the hot-melt extrusion method:
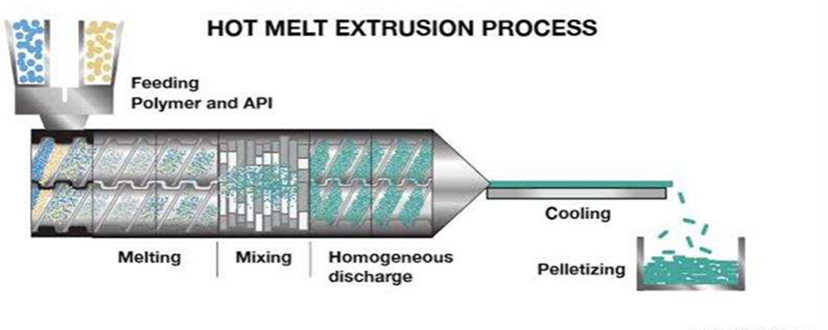
Fig.No.13 Hot Melt Extrusion Method
8.3. Direct Milling Method
The direct milling method is a solvent-free approach for the preparation of buccal films. In this technique, the drug and excipients are blended by kneading or mechanical milling without the use of any liquid medium. The resulting homogeneous mass is then rolled onto a release liner until the desired film thickness is achieved.
Elimination of organic solvents reduces the risk of residual solvent contamination, minimizes environmental and occupational hazards, and simplifies regulatory compliance. Owing to these advantages, direct milling represents a clean and safe alternative for buccal film manufacture, particularly when solvent exposure is a concern.
9. 3D PRINTING IN BUCCAL FILM FABRICATION [59-69]
Although solvent casting is simple and cost-effective, its multiple processing steps and susceptibility to batch-to-batch variability limit large-scale reproducibility. In recent years, three-dimensional (3D) printing has emerged as a versatile and precise manufacturing platform for buccal film fabrication, offering improved control over dose, geometry, and drug distribution.
9.1 Types of 3D Printing Techniques and Materials
Buccal films can be fabricated using various 3D printing techniques, including inkjet printing, extrusion-based printing, and semi-solid extrusion systems. Hydrophilic film-forming polymers are particularly suitable for inkjet and semi-solid extrusion approaches. In these methods, a printable “ink” containing the active pharmaceutical ingredient and excipients is deposited onto a blank film substrate or directly printed into the desired shape, followed by controlled drying.
10. CHALLENGES AND FORMULATION OPTIMIZATION
Printability is a critical challenge in 3D printing of buccal films and is strongly governed by the rheological properties of the printing formulation. Studies employing levocetirizine hydrochloride as a model drug with HPMC E15 as the film-forming polymer demonstrated that slurry viscosity plays a decisive role in determining film quality.
Low-viscosity formulations (approximately 10,920 cP) exhibited poor printability and produced films with elevated moisture content, resulting in surface curling and non-uniform thickness upon drying. In contrast, formulations with higher viscosities (10,920–19,380 cP) yielded films with improved dimensional uniformity, mechanical integrity, and consistent drug content. These findings highlight the importance of rheological optimization for successful 3D printing of buccal films.
Similarly, apigenin-loaded buccal films have been successfully fabricated using semi-solid extrusion 3D printing. To obtain the desired viscosity and shear-thinning conduct for extrusion, this method optimized the ink composition, which consisted of apigenin, ethanol, water, κ-carrageenan, poloxamer, and HPMC in a ratio of 2.5:4.7:4.7:200:200:200. 3D printing has many benefits, one of which is the elimination of the requirement for post-print trimming, which allows for the exact customization of film size, shape, and dosage. This reduces the risk of dose variation and minimizes film damage associated with uneven thickness.
11. APPLICATIONS AND INNOVATIONS
11.1 3D Printing–Enabled Design Flexibility and Drug Release Control
Three-dimensional printing enables the fabrication of buccal films with tailored architectures and precisely controlled drug-release behavior. By modifying internal geometries, layer arrangements, and filling patterns, dissolution characteristics and release kinetics can be finely tuned.
For example, double-layer estradiol buccal films fabricated using hydroxypropyl cellulose (H-HPC) with different internal designs—honeycomb, rectangular, and flat—exhibited distinct release profiles. Films with honeycomb and rectangular patterns demonstrated significantly faster drug release compared to conventional flat films, with the honeycomb structure showing the most favorable characteristics for oral administration.
Similarly, personalized theanine-loaded buccal films have been developed using carboxymethyl cellulose (CMC) through syringe-based extrusion 3D printing. The shear-thinning behavior of CMC-based inks enabled smooth extrusion through fine nozzles, facilitating fabrication of films with customized shapes, internal structures, and dose strengths. These examples illustrate the potential of 3D printing to support personalized medicine by allowing precise control over film geometry, drug loading, and release behavior.
12. CHARACTERIZATION OF BUCCAL FILMS [70,73]
The prepared drug-loaded matrix buccal films were evaluated for physicochemical, mechanical, and performance-related properties to assess their suitability for buccal administration.
12.1 Texture and Surface Characteristics
Film texture, flexibility, homogeneity, softness, and surface stickiness were initially evaluated by tactile examination to obtain a qualitative assessment of handling properties and patient acceptability.
12.2 Thickness and Surface pH
Film thickness was measured at five different locations using a digital micrometer to ensure uniformity. Surface pH was determined by allowing three films (1 cm² each) from each batch to swell in 5 mL of distilled water for 30 minutes, followed by pH measurement using a calibrated Thermo Fisher benchtop pH meter.
12.3 Drug Content Uniformity
Films (1 cm²) were cut from different regions of each batch and immersed in a methanol–water solvent system. The samples were agitated in a thermostatically controlled water bath at 37 ± 1 °C for 6 hours to extract the drug. The resulting solutions were filtered and analyzed by HPLC to determine drug content.
12.4 Folding Endurance
Mechanical strength was assessed by repeatedly folding a 4 cm² film along the same axis until breakage occurred. The number of folds sustained before tearing was recorded as the folding endurance.
12.5 Mucoadhesive Strength
Mucoadhesive strength was measured using a texture analyzer with rabbit buccal mucosa as the biological substrate. The mucosal tissue was mounted on a stationary platform, and a 1 cm² film was attached to the probe. The tissue surface was moistened with simulated saliva, and contact was maintained for one minute before detachment. Experimental parameters were selected based on previously reported methods.
12.6 Swelling Behavior (Percent Hydration)
Swelling behavior was evaluated in terms of percent hydration. Films (1 cm × 1 cm) were weighed initially (W?), placed on a stainless-steel mesh, and immersed in 10 mL of simulated saliva maintained at 37 ± 1 °C. At predetermined time intervals, films were removed, blotted to remove excess surface moisture, reweighed (W?), and percent hydration was calculated.
12.7 Fourier Transform Infrared Spectroscopy (FTIR)
Potential drug–excipient interactions were investigated using FTIR spectroscopy. Spectra of rizatriptan, physical mixtures, and the optimized F1 film were recorded over the range of 400–4000 cm?¹ using a Jasco FTIR spectrometer. Samples were prepared as KBr discs by mixing the drug with potassium bromide in a 1:5 ratio and compressing using a hydraulic press.
12.8 Differential Scanning Calorimetry (DSC)
Thermal behavior of rizatriptan, the optimized F1 film, and control formulations was evaluated using DSC. Approximately 5 mg of each sample was sealed in aluminum pans and heated from 50 to 300 °C at a rate of 10 °C/min under a nitrogen atmosphere.
12.9 Scanning Electron Microscopy (SEM)
Surface morphology of the optimized F1 films was examined using scanning electron microscopy. Samples were mounted on aluminum stubs with conductive silver tape, sputter-coated with gold, and observed under reduced pressure.
12.10 In Vitro Drug Release Studies
In vitro drug release from F1–F4 films was evaluated using a USP Type II dissolution apparatus employing the paddle-over-disc method. Films (2 cm × 1 cm) were affixed to glass slides and immersed in 900 mL of simulated saliva (pH 6.8) maintained at 37 ± 0.5 °C with a paddle rotation speed of 50 rpm. Samples were withdrawn at predetermined intervals, filtered through a 0.2 μm membrane, and analyzed by HPLC.
12.11 Ex Vivo Permeation Studies
Ex vivo permeation of rizatriptan from selected buccal films (F1 and F4) and a reference solution was evaluated using Franz diffusion cells fitted with rabbit buccal mucosa (effective diffusion area: 0.64 cm²). Films (0.6 cm²) or control solution containing 0.6 mg of drug were applied to the mucosal surface. The receptor compartment was filled with 5 mL of simulated saliva and stirred continuously at 50 rpm. Samples were withdrawn at regular intervals and analyzed by HPLC. Permeation flux was calculated from the slope of cumulative drug permeation per unit area versus time. All experiments were performed in six replicates (n = 6).
12.12 In Vivo Evaluation
Male rabbits weighing between 2.5 and 3.0 kg were randomly divided into two groups (n = 6 per group). Animals in Group I received the optimized F1 buccal film, measuring 1 cm × 1 cm and containing 10 mg of rizatriptan, which was applied directly to the buccal mucosa. Group II animals received an equivalent dose of rizatriptan administered orally as a gavage solution.
Prior to dosing, animals were anesthetized using ketamine (40 mg/kg) in combination with xylazine (5 mg/kg). Blood samples were collected at predetermined time points of 0.5, 1, 1.5, 2, 4, 8, and 12 hours post-administration. Plasma proteins were precipitated using a mixture of 2-propanol and acetonitrile, followed by centrifugation at 1789 × g for 10 minutes. The concentration of rizatriptan in the resulting supernatant was subsequently quantified using an appropriate analytical method.
12.13 Data Analysis
Statistical analysis was performed using GraphPad Prism version 6. Results were expressed as mean ± standard deviation, and differences were considered statistically significant at a p-value less than 0.05.
13. ADVANTAGES OF BUCCAL FILMS [74]
14. DISADVANTAGES OF BUCCAL FILMS [75]
15. CHALLENGES IN BUCCAL DRUG DELIVERY [76-81]
15.1 Limited Drug-Loading Capacity
The buccal mucosa provides a relatively small surface area of approximately 50 cm², which restricts buccal films to low-dose drugs and limits their application for high-dose therapies.
15.2 Saliva Interference
Continuous salivary secretion, estimated at 0.5–2 L per day, can erode or dilute the film, reducing residence time and leading to variable drug-release profiles.
15.3 Barriers to Biologics Delivery
Macromolecules such as peptides and proteins are susceptible to enzymatic degradation and exhibit limited permeability across the buccal epithelium.
15.4 Regulatory Challenges
Regulatory authorities such as the FDA and EMA require extensive safety, stability, and efficacy data. Compliance with updated regulatory guidelines (2023–2024), including biocompatibility and long-term stability requirements, adds complexity to scale-up and commercialization.
16. FUTURE PROSPECTS [82-84]
16.1 Integration of Nanotechnology
Incorporation of lipid-based carriers such as liposomes and nanoparticles can enhance drug stability, permeability, and protection against enzymatic degradation, particularly for biologics.
16.2 Advances in 3D Printing
Additive manufacturing enables precise control over film dimensions, drug distribution, and release kinetics, facilitating personalized dosing tailored to individual patient needs.
16.3 Innovative Polymers
Next-generation mucoadhesive materials, including thiolated polymers and chitosan derivatives, offer improved adhesion, extended residence time, and enhanced enzymatic protection.
16.4 Artificial Intelligence and Modelling
AI-driven tools can optimize formulation design, reduce experimental trial-and-error, and predict pharmacokinetic behaviour. Computational modelling may also support the development of advanced buccal vaccines and therapeutic systems.
17. FUTURE DIRECTIONS AND RESEARCH PRIORITIES [85-88]
18. CONCLUDING PERSPECTIVE
Mucoadhesive buccal films represent a versatile and patient-centered drug-delivery platform capable of providing both local and systemic controlled release. Continued advances in polymer science, nanotechnology, and manufacturing techniques—particularly three-dimensional printing—are steadily expanding their potential to deliver complex molecules and support personalized therapy. Although challenges remain related to residence time, drug-loading capacity, mucosal safety, and regulatory compliance, rational formulation design, standardized evaluation methods, and early regulatory alignment position buccal films as promising and broadly applicable therapeutic systems.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
Generative AI tools, including ChatGPT (OpenAI), were used to support the development of this manuscript by assisting with organization, language refinement, and the initial creation of draft tables and figures. All AI-generated content was thoroughly reviewed, revised, and validated by the authors to ensure accuracy, originality, and alignment with the journal’s standards. The authors assume full responsibility for the final manuscript and its scholarly integrity.
DECLARATIONS
Ethics approval and consent to participate
Not applicable. This article is a review and does not involve human or animal participants.
Consent for publication
Not applicable.
Funding
This work did not receive financial support from public, private, or not-for-profit funding agencies.
REFERENCES



Anuja More, Sonali Diwate, Akshada Deshmukh, Mucoadhesive Buccal Film: An Emerging Platform for Controlled Drug Delivery Systems, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1131-1151. https://doi.org/10.5281/zenodo.18213780
 10.5281/zenodo.18213780
10.5281/zenodo.18213780
