1,2Department of Pharmacy Practice, Oxbridge College of Pharmacy, Bangalore, India.
3Department of Pediatrics, Aster CMI Hospital, Bangalore, India.
4Department of Clinical Pharmacology, KIMS Hospital, Bangalore, India.
Stevens-Johnson Syndrome (SJS) is an uncommon, life-threatening mucocutaneous syndrome usually caused by drugs or infections. Here, we present a case of a 6-year-old Indian girl with fever, erosive mucositis, conjunctival redness, and vesiculopapular eruption. Investigations revealed Mycoplasma pneumoniae to be the causative agent. The diagnosis was established by skin biopsy. The patient was managed with IV methylprednisolone, cyclosporine, IVIG, and azithromycin, coupled with intensive supportive care, amniotic membrane grafting for eye involvement. Prompt recognition and early immunomodulatory treatment ensured successful recovery and stressed the role of multidisciplinary care in children with SJS.
Stevens-Johnson syndrome (SJS) and Toxic epidermal necrolysis (TEN) represent a category of severe skin and mucosal responses primarily triggered by medications, associated with a significant risk of morbidity and mortality. Both SJS and TEN are rare conditions; data suggests that TEN has an incidence of 0.4 to 1.2 cases per million individuals. SJS/TEN are distinct from more common skin conditions like erythema multiforme (EM) or maculopapular exanthema (MPE) due to their unique feature of skin separation.[1] The exact biological processes causing SJS/TEN are still not fully known, however they may involve CD8+ cytotoxic T cell hyperactivation and the subsequent occurrence of cytokine storms. The plasma and blister fluids of those who are affected show elevated levels of the cytolytic protein granulysin and the inflammatory cytokine tumor necrosis factor (TNF)-α.[2]
The development of SJS/TEN can also be explained by a number of other genetic risk factors, including polymorphisms in the antigen presentation pathway, cytochrome P450, and other drugs. Phenytoin-induced SJS/TEN, for example, is associated with differences in CYP2C9 and CYP2C19 (more especially, CYP2C9 poor metabolizer genotypes), even in the absence of HLA-B. Another study revealed a correlation between SJS/TEN and polymorphisms in the proteasome pathway, which is necessary for peptide trimming for MHC presentation.[3]
Nikolsky's sign positivity and epidermal detachment are seen in cutaneous lesions. Pathological assessments show full-thickness epidermal necrosis. Based on how much of the body surface area is involved, SJS and TEN are distinguished; SJS includes less than 10%, SJS-TEN overlap covers 10% to 30%, and TEN involves more than 30%. initially proposed the severity-of-illness score for toxic epidermal necrolysis (SCORTEN) as a way to evaluate the disease's severity and prognosis. The most widely used scale for prognostication in SJS-TEN is SCORTEN, and several research have shown its usefulness as a tool. [4]
The most significant risk factor for SJS/TEN is the recent start of a treatment that has been linked to the onset of the illness. There is evidence that the risk of developing SJS/TEN is increased by greater dosages of these drugs or by lower medication clearance, such as that caused by impaired renal function. Furthermore, the chance of developing SJS/TEN is increased by recent exposure to certain infectious organisms, such as Mycoplasma pneumoniae and HSV. [5] There might be a 40% fatality rate. When patients receive care in specialized facilities near intensive care units (ICUs), their mortality result improves. Incidence in adults is between 2.6 and 5.76 cases/million annually, whereas in children it is 1.5 cases/million.[6] The European Society for Medical Oncology (ESMO) and the National Comprehensive Cancer Network (NCCN) recommend against the future use of immune checkpoint inhibitors (ICIs). They suggest the use of intravenous immunoglobulins (IVIG) and corticosteroids alongside comprehensive supportive care to address this condition. However, these recommendations are based more on professional consensus than on evidence-based medicine.[7]
CASE PRESENTATION:
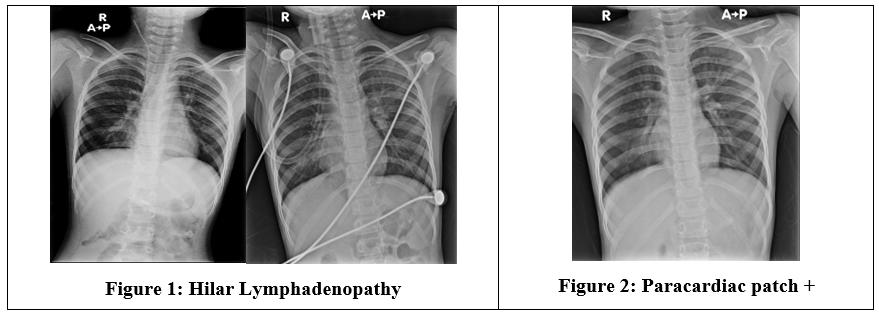
A 6-year-old Indian female presented in our hospital with complaints of itching and eye discharge for the last 5 days. On day 2 of illness noted rashes, which were initially papular in nature and few lesions progressed to become vesicular by day 4 of illness. The rashes were predominantly over her palms, trunk and back. On day 3 of her illness, she noted crusting and redness of her lips, and by day 4 of illness, she had difficulty swallowing and poor oral intake. She also had discomfort in the genital region and was unable to pass urine. History of low-grade fever noted on day 1 of illness. She has no history of travel/ drug intake. On admission she her BP was 96/72 mm Hg, RR-28/min, HR-121/min, Temp-100F, Spo2-88-92% in room air, she maintaining saturations with face mask 5 L/min O2. She was investigated for her lungs and chest X- ray was done (Figure1 and2). She was having no pallor/icterus/cyanosis/clubbing/lymphadenopathy/edema. On examination vesicular lesions over palms, lesions over the trunk and back- erythematous, with darkened halo. Genital region- Redness in the vulval region, lips- crusted, oral mucosa - limited mouth opening, mucosal erosions seen. Eyes- Redness with crusting and discharge +, Conjunctiva-congested, sub-conjunctival hemorrhage, thick pseudomembrane on the upper tarsal conjunctiva. RE cornea clear, LE near total epi defect, the remaining epithelium appears loose, pupils reactive lens clear BE. The hemogram was unremarkable (Hb 14 g/dl, TC 9800 cells/cu mm (N 68/L 18), PC 354000/cumm). CRP was 57.6 mg/L. A blood culture was sent and she was initiated on Inj Ceftriaxone. The renal function and liver function tests were normal. Based on the clinical symptomatology, the possibility of Stevens-Johnson syndrome and/or Reactive infectious mucocutaneous eruption was considered. On view of her clinical condition she was isolated and barrier nursing was initiated. She was treated with IV methylprednisolone (2mg/kg/day), oral cyclosporine (5 mg/kg/d) and IVIg 2 gm/kg (30 gms). Because of the extensive mucosal lesions and suspicion of mycoplasma-induced rash and mucositis and nasal swab showing Mycoplasma, a course of Azithromycin was given. Skin biopsy confirmed the diagnosis of Stevens-Johnson syndrome. The progression of skin lesions halted within 72 hours of starting the immunomodulation. Re-epithelization started on day 10 of the hospital stay, and cyclosporine was tapered and stopped. Steroids were tapered to 1 mg/kg/day. Supportive measures in terms of liquid paraffin, and fusidic acid ointment were applied. Strict aseptic measures were maintained in the isolation. For her pain management, she received fentanyl infusion, paracetamol, and oral tramadol. On view of the genital lesions, a course of valacyclovir was also given. Eye examination showed conjunctival congestion, sub-conjunctival hemorrhage, and thick pseudo membranes on the upper tarsal conjunctiva. Right eye-cornea was clear, whereas left eye cornea showed near total epithelial defect. On day 2 of the hospital stay, an amniotic membrane grafting was done. She tolerated the procedure well. Conformers were placed in bilateral eyes. Topical eye drops were continued. She remained afebrile, during the hospital stay and once the blood culture was sterile, IV Ceftriaxone was stopped. She was started on nasogastric feeding by day 2 of the hospital stay. She was supplemented with adequate calorie and protein intake. She was supported with Vitamins A, D, E, and K as per standard recommendations and zinc and calcium supplements. NG tube was removed on day 11 of hospital stay and oral intake was established. As the skin lesions had mostly re-epithelized and patient improved symptomatically & was hemodynamically stable, patient was discharged with oral steroid, vitamins and eye drops.
DISCUSSION: Stevens-Johnson syndrome (SJS) is the disease that involve immune-mediated involvement of the skin and mucous membranes. The disease damages organs like the liver, kidneys, lungs, and eyes, and its morbidity and mortality rate ranges from 5.4% to 15.3%. Infections and drugs are the causes of SJS/TEN. Not only has Mycoplasma pneumoniae (MP) been a leading cause of pediatric respiratory infections in recent years, but it also causes MP-related extrapulmonary illnesses (MpEPDS). According to reports, 20% to 30% of MP infection patients have skin mucosal symptoms such as urticaria, erythema multiforme, simple mucositis, and severe epidermal detachment.[8]
Here in our case of Stevens-Johnson syndrome (SJS), which was most probably caused by Mycoplasma pneumoniae infection. The patient had mucocutaneous involvement, including vesicular skin lesions and severe mucositis of the oral cavity, eyes, and genital area. Although Mycoplasma-related mucositis (also known as RIME) tends to present with minimal skin involvement, the severity of skin lesions and biopsy results favored a diagnosis of SJS. Early recognition and timely introduction of immunomodulatory therapy, such as IVIG, corticosteroids, and cyclosporine, served to arrest progression of the disease. Ocular involvement was addressed with amniotic membrane transplantation. The patient had a favorable response to therapy, with re-epithelialization and overall clinical recovery, underscoring the need for early supportive and specific therapy in pediatric SJS.
CONCLUSION: Stevens-Johnson Syndrome is an infrequent but serious illness that is highly suggestive and warrants high clinical suspicion, particularly in children presenting with mucocutaneous findings. This case highlights the role of Mycoplasma pneumoniae as an etiologic agent, even when there is minimal pulmonary disease. Early diagnosis and intensive immunomodulatory treatment—such as corticosteroids, IVIG, and cyclosporine—in conjunction with specific antimicrobial therapy and supportive care, were crucial in arresting disease progression and facilitating improvement. The favorable outcome in the present patient also emphasizes the importance of a multidisciplinary effort, including dermatology, ophthalmology, pediatrics, and critical care specialists, to provide for comprehensive care and reduce complications. Early intervention can result in good prognosis and complete recovery in children with SJS.
REFERENCES

Biswajit Haldar*, Ribul Ahmed, Chetan Gingiri, Praveen Kumar, Mycoplasma Pneumonia Induced Stevens-Johnson Syndrome: A Rare Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4422-4426 https://doi.org/10.5281/zenodo.17735700
 10.5281/zenodo.17735700
10.5281/zenodo.17735700
