Channabasweshwar Pharmacy College (Degree), Kava Road, Basweshwar Chowk, Latur-413512
Ocular drug delivery remains a challenging area due to the eye’s protective barriers, rapid tear turnover, and limited corneal permeability, which significantly reduce the bioavailability of conventional ophthalmic formulations such as eye drops and ointments. Ocusert-based ocular drug delivery systems were developed as a controlled and sustained release approach to overcome these limitations by maintaining consistent therapeutic drug levels in the ocular tissues for extended periods. Ocuserts are sterile, thin, flexible ocular inserts designed to be placed in the conjunctival sac, where they release the drug at a predetermined rate through diffusion-controlled mechanisms. The first marketed ocusert system demonstrated improved therapeutic efficacy and reduced dosing frequency; however, issues related to patient comfort, retention, and commercialization restricted its widespread adoption. In recent years, advancements in polymer science, biodegradable materials, and formulation technologies have renewed interest in ocusert-inspired ocular inserts. This review provides a comprehensive overview of ocusert-based ocular drug delivery systems, including their design principles, materials used, formulation techniques, evaluation parameters, advantages, limitations, and clinical relevance. Emphasis is placed on recent research trends, polymer innovations, and future prospects aimed at improving patient compliance and therapeutic outcomes in ocular drug delivery.
Ocular drug delivery continues to be a challenging area in pharmaceutical research due to the complex anatomy and highly protective physiological mechanisms of the eye. These natural defense systems, although essential for maintaining ocular health, significantly restrict the penetration and retention of topically administered drugs. Conventional ophthalmic dosage forms such as eye drops, suspensions, and ointments typically exhibit very low ocular bioavailability, often less than 5%, because of rapid tear turnover, blinking, reflex lacrimation, and nasolacrimal drainage. As a result, a substantial portion of the administered dose is eliminated from the ocular surface within a short period following instillation.¹²
In addition to precorneal drug loss, the corneal epithelium acts as a major permeability barrier, limiting drug absorption based on physicochemical properties such as molecular size, lipophilicity, and degree of ionization. To compensate for these barriers, conventional formulations often require frequent dosing, which may lead to poor patient compliance, inconsistent therapeutic response, and increased risk of systemic side effects due to drainage into the nasolacrimal duct.³?
To overcome these limitations, various novel ocular drug delivery systems have been investigated, including in-situ gelling systems, nanoparticles, liposomes, niosomes, ocular films, and contact lens-based delivery platforms. Although these approaches have demonstrated improvements in ocular residence time and drug absorption, challenges related to formulation complexity, burst release, stability, and large-scale manufacturing still persist.??
Among the different strategies explored, ocular inserts—particularly ocusert-based systems—represent one of the earliest and most rational approaches for achieving controlled and sustained ocular drug delivery. Ocuserts are sterile, thin, and flexible devices designed to be placed in the conjunctival sac, where they remain for prolonged periods and release the drug at a predetermined rate. Unlike conventional eye drops, ocuserts are not rapidly eliminated by tear fluid, allowing relatively constant drug levels to be maintained in ocular tissues.³? This review focuses on the design principles, materials, evaluation parameters, advantages, limitations, and future prospects of ocusert-based ocular drug delivery systems, with emphasis on recent advancements aimed at improving patient compliance and therapeutic outcomes.
Ocular Barriers Affecting Drug Delivery
Effective ocular drug delivery is restricted by multiple protective barriers that are essential for maintaining ocular homeostasis but significantly limit drug absorption. Precorneal barriers such as tear dilution, tear turnover, reflex blinking, and lacrimation rapidly remove instilled drugs from the ocular surface within minutes of administration. The normal tear turnover rate, combined with nasolacrimal drainage, results in rapid clearance of conventional eye drops, reducing drug residence time and limiting absorption. These dynamic precorneal processes significantly decrease the contact time of formulations with the corneal epithelium and are a primary reason for the poor bioavailability of topical ophthalmic drugs.²?
In addition to tear dynamics, the mucus layer covering the corneal and conjunctival surface acts as an additional diffusional barrier that can restrict drug penetration. Drug molecules may bind to mucins or be trapped within the tear film, further reducing the effective concentration available for corneal permeation. Frequent blinking also contributes to mechanical elimination of formulations, creating variability in drug exposure and therapeutic response.¹?²?
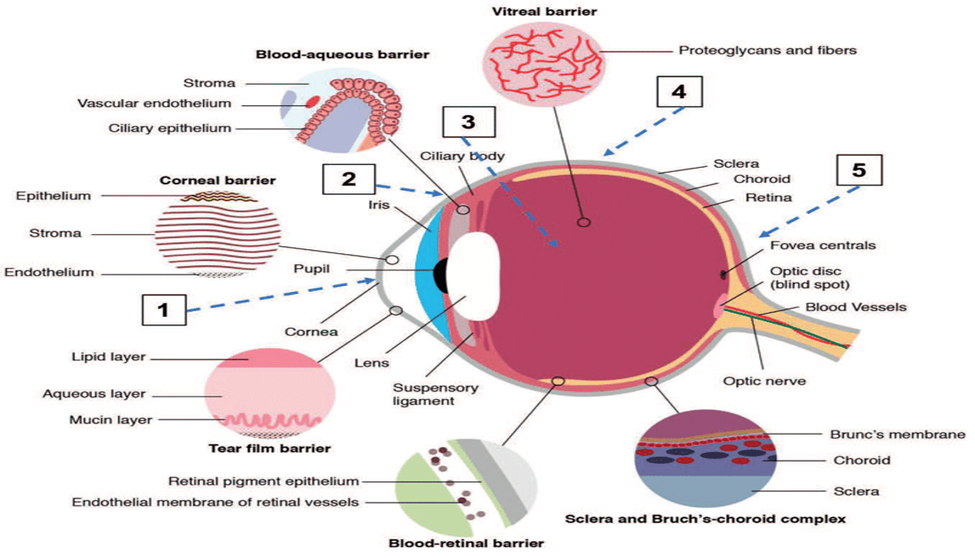
Figure 1 — Ocular Barriers Affecting Drug Delivery
The cornea itself functions as a highly specialized anatomical barrier composed of three major layers: the lipophilic epithelium, hydrophilic stroma, and endothelial layer. The epithelial layer contains tight junctions that restrict paracellular drug transport, making it a major rate-limiting barrier for hydrophilic compounds. Conversely, the stromal layer limits the diffusion of lipophilic drugs due to its aqueous structure. This biphasic barrier nature requires drugs to possess balanced lipophilicity and hydrophilicity to achieve optimal permeation. High-molecular-weight drugs and poorly soluble compounds face additional resistance across these layers.¹³¹?
Collectively, these anatomical and physiological barriers result in less than 5% of the administered topical dose reaching intraocular tissues. The majority of the drug is lost through tear drainage, systemic absorption, or surface elimination. Such low bioavailability necessitates frequent dosing of conventional formulations, increasing the risk of toxicity and reducing patient compliance. These limitations have driven the development of alternative controlled delivery systems, such as ocuserts, which aim to prolong ocular residence time, reduce drug loss, and provide sustained therapeutic concentrations at the target site.¹³²³
Concept and Design of Ocusert
An ocusert is a sterile, thin, flexible ocular insert designed to deliver drugs at a controlled and predetermined rate over an extended period. It is typically placed in the lower conjunctival sac, where it remains in intimate contact with ocular tissues and tear fluid. Unlike conventional ophthalmic dosage forms that are rapidly cleared, ocuserts are engineered to maintain prolonged residence time, enabling sustained therapeutic drug levels. The fundamental design principle of ocuserts is based on diffusion-controlled release, which allows predictable and reproducible drug delivery independent of patient variability.³? The classical ocusert design consists of a drug reservoir sandwiched between one or more rate-controlling membranes and surrounded by a peripheral sealing layer. The drug core may be present as a gel, polymeric matrix, or semi-solid reservoir containing a high concentration of active pharmaceutical ingredient. The surrounding membrane functions as a barrier that regulates the rate of drug diffusion into the tear film. By modifying membrane thickness, permeability, and polymer composition, it is possible to fine-tune release kinetics and achieve near zero-order drug delivery. This structural design minimizes peak–trough fluctuations commonly observed with eye drops and improves therapeutic consistency.?¹?
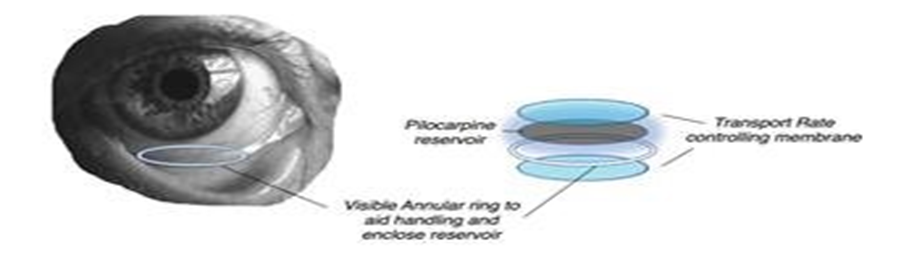
Figure 2 — Design of Occusert
Modern ocusert systems incorporate advanced polymer technologies to enhance comfort, flexibility, and ocular compatibility. Recent designs focus on reducing insert thickness, improving transparency, and increasing elasticity to minimize foreign body sensation. The integration of mucoadhesive polymers allows better retention within the conjunctival sac, while biodegradable materials eliminate the need for manual removal. These improvements represent a shift from early rigid ocuserts toward patient-centric ocular inserts with improved acceptability.?¹?
Classification of Ocusert Systems
Ocusert systems can be broadly classified based on their structural design, drug release mechanism, and behavior in ocular fluids. Such classification is essential for understanding their release kinetics, formulation strategy, and patient acceptability. Based on structural design and drug release mechanism, ocuserts are mainly divided into reservoir-type and matrix-type systems.³?
Reservoir-type ocuserts consist of a central drug reservoir enclosed within one or more rate-controlling membranes. In these systems, the drug is present in a concentrated form inside the reservoir, while the surrounding membrane regulates the rate of diffusion. This design enables controlled and prolonged drug release, often approaching zero-order kinetics, which is particularly advantageous for drugs requiring precise and sustained therapeutic levels. The membrane-controlled structure minimizes fluctuations in drug concentration and enhances predictability of drug delivery.¹?²?
Matrix-type ocuserts, in contrast, are composed of a homogeneous mixture of drug and polymer. The drug is uniformly dispersed throughout the polymeric matrix, and release occurs primarily by diffusion through the swollen polymer network. Matrix systems are generally simpler in design and easier to manufacture compared to reservoir systems. However, the release rate depends strongly on polymer characteristics, matrix thickness, and drug–polymer interactions, resulting in diffusion-controlled release behavior.?¹?
Based on their behavior in ocular fluids, ocuserts may be categorized as soluble, insoluble, or bioerodible systems. Soluble ocuserts are prepared using water-soluble polymers that gradually dissolve in tear fluid following administration. Drug release occurs as the polymer dissolves, and these systems do not require removal after drug depletion, thereby improving patient convenience and compliance.¹?²³
Insoluble ocuserts are fabricated from non-biodegradable polymers and remain structurally intact during the drug release period. After complete drug depletion, they must be manually removed from the eye. Although these systems provide prolonged and controlled drug delivery, extended retention may occasionally cause discomfort or foreign body sensation in some patients.?¹?
Bioerodible ocuserts represent a more advanced class in which biodegradable polymers are used to allow gradual erosion or degradation in ocular fluids. Drug release occurs concurrently with polymer erosion, eliminating the need for device removal. These systems are designed to reduce foreign body sensation and improve patient comfort, making them particularly attractive for modern ocular therapy.?¹?
Polymers Used in Ocusert Formulations
Polymers are the fundamental structural and functional components of ocusert systems, as they govern mechanical strength, flexibility, drug release behavior, ocular compatibility, and overall therapeutic performance. The choice of polymer determines swelling characteristics, permeability, bioadhesion, and degradation profile of the insert. An ideal ocusert polymer should be non-toxic, non-irritant, transparent, mechanically stable, and capable of providing predictable drug release while maintaining patient comfort.¹²
Hydrophilic polymers are widely used in ocusert fabrication due to their excellent film-forming ability and hydration behavior. Upon contact with tear fluid, these polymers absorb water and form a hydrated gel network that facilitates controlled drug diffusion. Commonly used hydrophilic polymers include hydroxypropyl methylcellulose (HPMC), polyvinyl alcohol (PVA), polyethylene oxide, sodium alginate, and carbopol. These materials exhibit good transparency and flexibility, minimizing visual interference and foreign body sensation. Their swelling behavior can be modulated to tailor drug release rates, making them particularly suitable for matrix-type ocuserts.³?
Hydrophobic polymers are frequently employed as rate-controlling membranes in reservoir-type ocusert systems. Materials such as ethyl cellulose, cellulose acetate, Eudragit derivatives, and polymethacrylates act as semi-permeable barriers that regulate drug diffusion. By adjusting membrane thickness and polymer composition, near zero-order release kinetics can be achieved. Hydrophobic polymers also enhance mechanical integrity and prevent rapid drug leakage, ensuring sustained delivery over extended periods.??
Biodegradable polymers represent an important advancement in modern ocusert design. Polymers such as polylactic acid (PLA), polylactic-co-glycolic acid (PLGA), chitosan, gelatin, and collagen gradually degrade in ocular fluids, eliminating the need for manual removal of the insert. These materials improve patient compliance and reduce the risk of foreign body sensation. In addition, biodegradable polymers can be engineered to exhibit predictable erosion rates, allowing synchronization of polymer degradation with drug release.??
Evaluation of Ocusert Systems
Evaluation of ocusert-based ocular inserts is essential to ensure their quality, safety, therapeutic performance, and patient acceptability. Because ocuserts are placed directly in contact with sensitive ocular tissues, rigorous physicochemical, mechanical, biological, and stability testing is required. Proper evaluation confirms reproducibility of drug release, structural integrity, and ocular compatibility, all of which are critical for clinical success.?¹?
Physical and mechanical properties are first assessed to confirm uniformity and durability of the insert. Thickness uniformity is measured at multiple points using a digital micrometer to ensure consistent drug distribution and predictable release kinetics. Weight variation testing is performed to verify batch uniformity and proper mixing of polymers and drug. Folding endurance evaluates flexibility by repeatedly folding the insert until breakage occurs, indicating its ability to withstand blinking stress. Tensile strength testing determines resistance to mechanical deformation during handling and insertion. Adequate mechanical strength prevents fragmentation and accidental loss from the conjunctival sac.?¹?
Surface and chemical properties are evaluated to ensure ocular safety and compatibility. Surface pH is measured after hydration in simulated tear fluid, and it should remain close to physiological tear pH to minimize irritation and discomfort. Drug content uniformity testing confirms accurate dosing and homogeneous drug distribution throughout the insert. Analytical methods such as UV spectrophotometry or HPLC are commonly used for quantitative determination. These tests ensure reproducibility and therapeutic reliability across batches.?¹?
In-vitro performance studies are conducted to predict in-vivo behavior of ocuserts. Drug release studies are performed using diffusion cells containing simulated tear fluid, allowing evaluation of release kinetics over time. Mathematical modeling using zero-order, first-order, Higuchi, or Korsmeyer–Peppas equations helps identify the dominant release mechanism. Swelling studies and hydration behavior are also assessed, as polymer expansion influences drug diffusion and retention within the conjunctival sac. These experiments provide critical insights into formulation optimization.¹?²?
Biological and microbiological evaluation is mandatory because ocuserts are sterile ophthalmic devices. Sterility testing is performed according to pharmacopeial guidelines to confirm absence of microbial contamination. Ocular irritation studies, often conducted using in-vitro or ex-vivo corneal models, assess biocompatibility and safety. Moisture uptake studies evaluate environmental stability, as excessive water absorption may alter mechanical properties and drug release. Stability studies under controlled temperature and humidity conditions are conducted to monitor changes in drug content, physical appearance, and performance over time.¹³²³
Mechanism of Drug Release
Drug release from ocusert systems occurs through diffusion, polymer swelling, and polymer erosion, depending on the insert design and polymer composition. These mechanisms regulate both the rate and duration of delivery, allowing sustained therapeutic drug levels in the tear film while minimizing fluctuations seen with conventional ocular dosage forms.¹²
In reservoir-type ocuserts, drug release is mainly diffusion-controlled. The drug is contained in a central core and diffuses through a semi-permeable rate-controlling membrane according to Fick’s law. By optimizing membrane permeability and thickness, near zero-order release kinetics can be achieved, providing a constant delivery rate over extended periods. This predictable behavior is particularly beneficial for chronic ocular therapy.³?
Matrix-type ocuserts contain drug uniformly dispersed within a polymer network. Upon hydration by tear fluid, the matrix forms a gel structure that permits gradual drug diffusion. Release depends on polymer swelling, porosity, drug solubility, and insert thickness, often resulting in diffusion-controlled or anomalous transport behavior.?
Swelling-controlled release is characteristic of hydrophilic polymers that absorb tear fluid and expand, creating diffusion pathways for drug transport. In bioerodible ocuserts, polymer degradation further contributes to drug release as the matrix gradually breaks down. This erosion-controlled mechanism eliminates the need for device removal and enhances patient convenience.??
Overall, the combined effects of diffusion, swelling, and erosion enable ocuserts to deliver drugs in a sustained and predictable manner, making them effective platforms for long-term ocular therapy.²
Sterilization of Ocuserts
Sterilization is essential in ocusert development because the inserts come into direct contact with delicate ocular tissues. Microbial contamination can lead to serious infections and inflammation, making strict sterility assurance mandatory. However, sterilizing polymeric ocular inserts is challenging since many methods can affect polymer structure, drug stability, and release behavior. Therefore, the sterilization approach must ensure microbial safety while maintaining physicochemical integrity.¹³²³
Thermal sterilization methods such as moist heat and dry heat are generally unsuitable for most ocusert formulations. Elevated temperatures can deform polymer films, accelerate drug degradation, and alter membrane permeability. Heat-sensitive drugs and polymers may lose mechanical flexibility, resulting in brittle inserts that reduce patient comfort. Consequently, thermal techniques are rarely preferred unless the formulation is specifically designed to tolerate high temperatures.?¹?
Gamma irradiation is widely used for sterilizing ocuserts because it is effective at ambient temperatures and penetrates polymer matrices without direct heating. It is suitable for thermolabile formulations, although excessive radiation may cause polymer chain scission or crosslinking, affecting mechanical properties and release kinetics. Controlled dose selection and post-irradiation stability testing are therefore necessary to preserve therapeutic performance.?¹?
Ethylene oxide sterilization is another important option for heat-sensitive inserts. The gas effectively sterilizes at low temperatures and penetrates complex polymer systems. However, residual ethylene oxide must be carefully removed, as traces may cause ocular irritation or toxicity. Adequate aeration and validation procedures are critical to ensure safety.¹?²?
Emerging sterilization techniques, including electron beam irradiation and plasma-based methods, are being explored to minimize polymer damage and chemical residues. These advanced approaches may improve compatibility with biodegradable and nanostructured ocuserts, supporting the development of modern ocular drug delivery systems.?¹?
Advantages of Ocusert Systems
Limitations of Ocusert Systems
Comparison with Other Ocular Drug Delivery Systems
Ocusert systems occupy a unique position among ocular drug delivery platforms because they combine prolonged residence time with predictable and controlled drug release. Conventional eye drops, although widely used, suffer from rapid precorneal elimination and poor bioavailability, often requiring frequent administration. In contrast, ocuserts maintain sustained drug levels by resisting tear washout and providing diffusion-controlled release. This difference significantly improves therapeutic efficiency and reduces dosing variability.¹²³
Ocular ointments and gels offer longer retention than eye drops but may cause blurred vision and patient discomfort due to their viscous nature. Ocuserts avoid visual disturbance because they are thin and transparent, allowing sustained delivery without compromising visual clarity. Additionally, inserts provide more reproducible dosing compared to semisolid formulations, where drug distribution can be inconsistent.³?
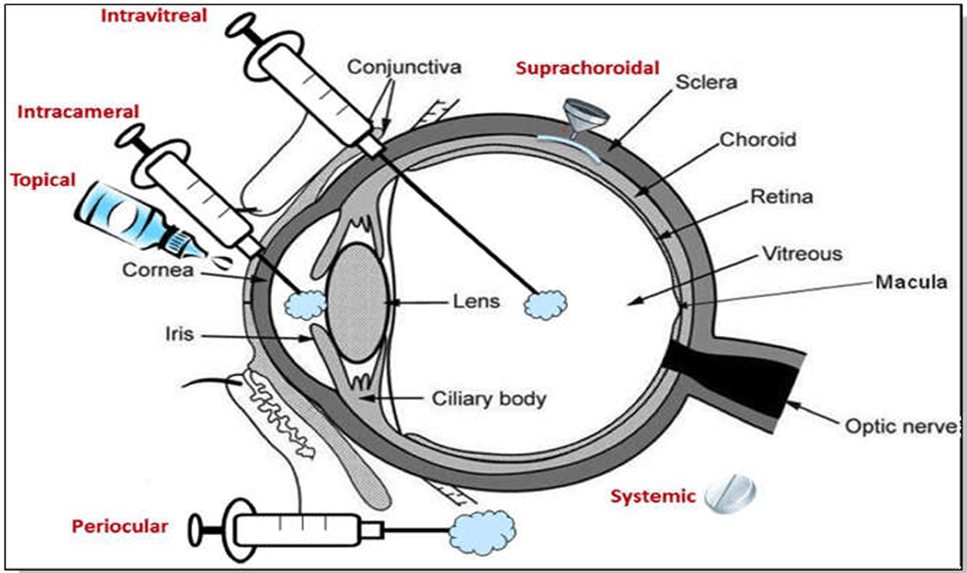
Figure 3. Comparison of major ocular drug delivery systems.
In-situ gelling systems and nanoparticle-based formulations represent modern alternatives designed to enhance ocular retention. While these systems improve bioavailability, they may still exhibit burst release or variability in gel formation depending on tear composition. Ocuserts, by contrast, rely on a physical device structure that allows precise control over drug diffusion, making them particularly suitable for therapies requiring steady long-term delivery.?¹?
Contact lens-based drug delivery systems have also gained attention as sustained ocular platforms. Although they offer prolonged residence time, concerns remain regarding lens hygiene, oxygen permeability, and patient compliance. Ocuserts present a simpler, disposable alternative that avoids many complications associated with extended lens wear. However, both systems share the goal of improving ocular drug retention and therapeutic effectiveness.¹?²?
Overall, ocuserts provide a balance between sustained release, dosing precision, and device simplicity. Their ability to maintain stable therapeutic concentrations distinguishes them from conventional and emerging ocular delivery systems, making them particularly valuable for chronic ocular therapy.?¹?
Regulatory and Commercial Aspects
Ocuserts are classified as combination drug-device products, requiring compliance with stringent regulatory guidelines. Evaluation includes sterility assurance, biocompatibility, safety, and performance testing. Regulatory approval demands detailed documentation of formulation, manufacturing, and quality control processes.
Commercial success depends on patient acceptability, cost-effectiveness, and clinical benefits over existing therapies.
Future Prospects
Recent advances in polymer science and formulation technology have renewed interest in ocusert-based ocular drug delivery systems. Current research is increasingly focused on the development of biodegradable and patient-friendly ocular inserts that can provide sustained drug release while minimizing discomfort and the need for manual removal. Biodegradable polymers with predictable erosion profiles are being designed to synchronize polymer degradation with drug release, thereby improving both safety and patient compliance.
The incorporation of nanotechnology into ocusert systems represents a significant emerging trend. Nanoparticle-loaded ocuserts and polymer–nanocomposite inserts have the potential to enhance drug loading efficiency, improve corneal permeability, and enable targeted delivery to deeper ocular tissues. Such hybrid systems may be particularly beneficial in the management of chronic ocular disorders that require long-term therapy and precise drug concentration control.
In addition, stimuli-responsive polymers capable of altering drug release in response to physiological triggers such as pH, temperature, or tear composition are being actively explored. These smart materials offer the possibility of adaptive and personalized ocular therapy. However, despite promising laboratory-scale results, challenges related to large-scale manufacturing, regulatory approval, and long-term safety evaluation must be addressed before clinical translation can be achieved.
With continued interdisciplinary research and improvements in regulatory frameworks for combination drug–device products, ocusert technology is expected to evolve into advanced therapeutic platforms. The integration of biodegradable materials, nanocarriers, and patient-centric design principles may position ocuserts as an important component of next-generation ocular drug delivery systems.
CONCLUSION
Ocusert-based ocular drug delivery systems offer an effective approach for achieving sustained and controlled drug release to the eye, addressing many of the limitations associated with conventional ophthalmic formulations. By prolonging ocular residence time and maintaining relatively constant therapeutic drug levels, ocuserts improve treatment efficacy while reducing dosing frequency and enhancing patient compliance.
Although early ocusert designs faced challenges related to comfort, retention, and commercial acceptance, recent advancements in polymer selection, formulation design, and fabrication techniques have significantly improved their performance and patient acceptability. The use of biodegradable and mucoadhesive materials has further addressed concerns related to foreign body sensation and device removal.
With ongoing research focused on advanced polymers, nanotechnology-based inserts, and smart delivery systems, ocuserts hold considerable potential for long-term ocular therapy. Continued optimization and clinical evaluation may enable these systems to emerge as reliable and patient-friendly alternatives for the management of various ocular diseases.
REFERENCES

Shubham Chillarge, Dr. Nasheer S. Shaikh, Vaishnavi Karbhari, Vidya Sirsat, Ocusesrt-Based Ocular Drug Delivery Systems: Advancements, Challenges, and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2136-2146. https://doi.org/10.5281/zenodo.18631318
 10.5281/zenodo.18631318
10.5281/zenodo.18631318
