
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4, Student at Vidyaniketan Collage Of Pharmacy,Takarkheda More Road, Anjangaon Surji.
5Department of Pharmaceutical Quality Assurance, Vidyaniketan Collage Of Pharmacy,Takarkheda More Road, Anjangaon Surji.
Onychomycosis is one of the fungal infections of the toenail. Moreover, moderate to severe onychomycosis can be a chronic disease with high tendency to re-appear which also complicates treatment. Oral antifungal treatment is the existing gold standard of curing moderate to severe toenail onychomycosis. It is a great problem, as it can lead to paresthesias, local pains, difficulty in performing everyday activities, and social interaction difficulties. There are numerous skin problems that are treated with vinegar at home. To be able to properly recommend this popular drug to be used in skin diseases as well as to determine whether such a treatment would have any side effects, dermatologists need to know the studies of the use of the drug along with the possible side effects to be aware of how to recommend the safe use of such widely available medication. Vinegar is usually available as a food additive to flavor as well as to preserve. It is one of the first skin treatments that people have ever heard about. However, its role in treatment plans has been reducing over the years. The focal point of this paper is to illustrate its leper, venereology and dermatology treatment toolkit
Trans" means "through" and "Unguis" means "Nail", So transungual or preungual drug delivery system is nothing, but a system associated with drug delivery through the nail to achieve a targeted drug delivery system of the nail to treat diseases of nail itself. Trans" means "through" and "Unguis" means "Nail", So transungual or preungual drug delivery system is nothing, but a system associated with drug delivery through the nail to achieve a targeted drug delivery system of the nail to treat diseases of nail itself. The hardness and impermeability of the nail makes it a decidedly poor route by which to deliver drugs. However, improvement in the topical delivery of compounds for the treatment of nail fungal diseases (onychomycosis and nail psoriasis) would minimize the need for systemic administration of drugs with its associated side effects.
In addition, it may shorten the period of time needed for treatment and help to prevent relapse. Medicated nail lacquers are the formulations .that are used for transungual drug delivery for maximal antifungal efficacy now days . The preungual delivery system is used to solve the fungal infection of nail plate Onychomycosis. Onychomycosis (tineaunguium), is a fungal infection in the nail bed or the nail plate of the fingers or the toes that is caused by an organism from the group Trychophyton rubrum. It accounts for about 50% of the total illnesses of the nails and it is the most common disorder in adults.[1] Onychomycosis is found in 10% of the general population but is more common in the elderly; however, 50% in the age above 70 and 20% in the age above 60. Diabetes mellitus, immunologic diseases, and peripheral vascular diseases are related to increased frequency in the elderly. People with diabetes have a 1.9 - 2.8 times higher risk of onychomycosis than the general population.[2]
MICROBIOLOGY:
Many organisms but most often dermatophytes from the genus Trichophyton cause onychomycosis. Other organisms include a more common in the general population non-dermatophyte molds are less frequent cause in patients with persistent mucocutaneous candidiasis as well fingernail infections. However, recent research has concluded that they are the most common organisms in people who have HIV infection and onychomycosis.[2]
PATHOGENESIS:
Onychomycosis may result from direct contact of the nail with dermatophytes, with non-dermatophyte molds, or yeasts. The nail unit is susceptible to fungal infection due to previously stated lack of strong cell mediated immunity. Proteolytic, keratinolytic and lipolytic enzymes produced by the fungi provide help in the destruction of keratin in the nail plate and facilitate the invasion of fungi in the nail plate. The risk to develop fungal infection may be increased by factors that weaken infectious prevention barriers of fungi. Different clinical subgroups of onychomycosis which are caused due to location and pattern of fungal invasion. The development of fungal bio-films is one way that fungi can develop resistance to antifungal drugs and allow them to escape the effects of existing antifungal treatments.
ETIOLOGY:
Dermatophytes (tinea unguium), non-dermatophyte molds and yeasts may all cause onychomycosis. Dermatophytes, specifically Trichophyton mentagrophytes and Trichophyton rubrum, are the organisms responsible for 90% and 75% respectively of onychomycosis in the nails of the toes and hands respectively. Epidermophyton floccosum, Microsporum species, Trichophyton verrucosum, Trichophyton tonsurans, Trichophyton violaceum, Trichophyton soundanense, Trichophyton krajdenii, Trichophyton equinum, and Arthroderma species are the other dermatophyte infections. Aspergillus and Scopulariasis species, Fusarium, Acremonium, Syncephalastrum, Scytalidium, Paecilomyces, Neoscytalidium, Chaetomium, Onychocola, Alternaria are examples of species of non-matophyte molds that can cause onychomycosis. About 10% of cases of all onychomycosis worldwide are due to non-dermatophyte molds. Onychomycosis induced by yeast is rare. About 70% of acquired onychomycosis that is induced by yeast is due to Candida albicans. There are 2 more species of Candida - Candida tropicalis and Candida parapsilosis.[3]

Fig 1. Types Of Onychomycosis.[4]
CONVENTIONAL ANTIFUNGAL TREATMENT OF ONYCHOMYCOSIS :
Onychomycosis is the chronic fungal infection of the nail of the toes and the nails of the fingers, mainly caused by Trichophyton rubrum, T. mentagrophytes, Candida species and a number of fungal molds other than the dermatophytes. Due to the slow nail growth, biofilm, and poor drug penetration, therapy is often required for long term treatment. Conventional management comprises antifungal drugs (topical, systemic) and mechanical means and all these have their own advantages and disadvantages. Dangers of Antifungal Mouth Rinses Topical antifungals are recommended primarily for the treatment of mild to moderate onychomycosis or drug contraindications to the systemic drugs.[4] Commonly used agents include ciclopirox 8% lacquer, amorolfine 5% lacquer and efinaconazole 10% solution. Ciclopirox chelates metal ions which are essential for fungal enzymes but have poor nail penetration ratios therefore the complete cure rate is limited even after 48 weeks of therapy Amorolfine works by inhibiting ergosterol synthesis and shows better outcomes when combined with regular debridement of the nails, however the monotherapy is still less effective for severe infections.[5] Efinaconazole has a superior nail penetration rate and less keratin binding and therefore has had significantly higher mycologic cure rates in Phase III trials however treatment must be continued daily for almost one year.[6] Itraconazole is commonly used in Pulse of Uses and fluconazole also.[7] Treatment is weekly for several months with lower cure rates compared to terbinafine.[8]Itraconazole is commonly used in pulse doses (200 mg twice daily for one week per month), but it carries a higher relapse rate and significant CYP3A4 interactions. Fluconazole, although off-label, is used weekly for several months but produces lower cure rates compared to terbinafine,[9]Despite these therapeutic options, successful treatment remains challenging due to high recurrence rates, long treatment durations, cost, and increasing antifungal resistance.[10]
OVERVIEW OF APPLE CIDER VINEGAR :
Despite these therapeutic options, successful treatment remains challenging due to high recurrence rates, long treatment durations, cost, and increasing antifungal resistance,[11]The dominant antimicrobial principle is acetic acid, typically present at ~3–6%, which lowers local pH and exerts direct fungistatic and fungicidal effects by disrupting membrane integrity, impairing nutrient transport, and denaturing proteins in susceptible fungi; laboratory and sanitation studies confirm strong microbicidal action of vinegar solutions under controlled conditions.[12] The dominant antimicrobial principle is acetic acid, typically present at ~3–6%, which lowers local pH and exerts direct fungistatic and fungicidal effects by disrupting membrane integrity, impairing nutrient transport, and denaturing proteins in susceptible fungi; laboratory and sanitation studies confirm strong microbicidal action of vinegar solutions under controlled conditions.[13] Traditional, unfiltered ACV contains the “mother” a cellulose-rich matrix of acetic acid bacteria and residual yeasts which not only signals minimal processing but may also influence local microbial ecology when ACV is applied topically, though the direct probiotic benefit in nail infections remains to be proven.[14] Metabolomic and fermentation studies show that production method and microbial consortia markedly affect ACV’s organic-acid profile (malic, lactic, succinic acids) and phenolic concentration, which in turn change antimicrobial potency and keratolytic potential important because keratin softening could enhance topical contact with subungual fungal colonies.[15] Practical dermatologic investigations and clinical reports suggest that weak acid soaks or compresses (vinegar dilutions) can be useful adjuncts in superficial skin and nail infections, improving topical antifungal efficacy by lowering surface pH and aiding mechanical debridement, although achieving fungicidal pH at the nail bed is technically challenging in vivo and depends on concentration, exposure time, and formulation.[16] Practical dermatologic investigations and clinical reports suggest that weak acid soaks or compresses (vinegar dilutions) can be useful adjuncts in superficial skin and nail infections, improving topical antifungal efficacy by lowering surface pH and aiding mechanical debridement, although achieving fungicidal pH at the nail bed is technically challenging in vivo and depends on concentration, exposure time, and formulation.[17] In sum, ACV’s multifactorial pharmacology acidification, phenolic bioactivity, organic-acid keratolysis, and possible microbiome modulation by the “mother” makes it a scientifically plausible, low-cost adjunct or alternative for mild localized fungal conditions; however, controlled clinical trials specific to onychomycosis are still limited and required to establish efficacy, dosing, and long-term outcomes.[18]
MATERIAL AND METHOD FOR FORMATION OF APPLE CIBER VINEGAR:
1.Collection of Wild Apples: Fresh wild apples are collected from natural forest areas (such as the Ribnik municipality region). These apples contain diverse natural yeasts and acetic-acid-producing bacteria that support spontaneous fermentation[19], it show in figure 2.
2.Washing and Cleaning: Apples are thoroughly washed to remove dirt, soil, and surface contaminants while retaining natural microflora essential for fermentation.[20]
3.Pressing to Extract Juice: Clean apples are mechanically pressed. The extracted juice serves as the substrate for alcoholic and acetic fermentation.[21]
4.First Fermentation (≈20 Days): The filtered apple juice is transferred to wide-mouthed, gauze-covered containers and left for around 20 days. Wild yeasts convert the natural sugars into ethanol during this stage (alcoholic fermentation).[22]
5.Transfer to Fresh Containers (Second Fermentation Phase): After 20 days, the partially fermented juice is moved into new, clean gauze-covered pots and kept for another 24 days. This step increases oxygen exposure, which accelerates acetic acid formation by Acetobacter species.[23]
6.Acetic Fermentation (Oxidation Phase): Acetic acid bacteria convert ethanol into acetic acid, giving the vinegar its acidity and antimicrobial properties.[24]
7.Final Maturation: Once acidity stabilizes, the fermented liquid is filtered if necessary and filled into glass containers for storage. Glass prevents chemical interactions and preserves phenolic compounds.[25]
8.Resulting Product – Artisanal Apple Vinegar: This slow, natural fermentation technique produces vinegar with higher antioxidant potential, richer phenolic content, and better enzyme-inhibitory activity compared to industrial vinegars.[19,20]

Fig 2. The Formation of ACV.[42]
MECHANISM OF ACTION:
Acetic acid, a weak organic acid with potent inhibitory effects on dermatophytes, particularly Trichophyton rubrum, is the main cause of apple cider vinegar’s antifungal efficacy in onychomycosis.[21,26] The fungus cannot grow in the low pH that acetic acid creates; studies confirm that T. rubrum fails to grow at pH ≤ 3, demonstrating strong acid-dependent inhibition.[21,27] Since dermatophytes need a pH close to neutral for optimal enzyme and keratinase activity, the acidic environment instantly interferes with their metabolic processes and prevents the synthesis of keratin-degrading enzymes required for nail plate colonization.[27,28], it show in figure 3. Acetic acid diffuses into fungal cells in its undissociated form after penetrating the superficial layers of the diseased nail, either directly or more effectively when the nail is pre-softened using keratolytic agents such as urea.[23] Once inside the fungal cytoplasm—where the pH is higher—the acid dissociates into hydrogen and acetate ions. This intracellular acidification disrupts essential metabolic processes such as ATP generation, amino acid metabolism, and membrane transport mechanisms.[22,25] The sudden drop in cytoplasmic pH also disturbs the electrochemical gradient across the fungal membrane, compromising energy balance and nutrient flow.[22,23] (show in figure 3) ,In addition to metabolic inhibition, acetic acid directly damages the fungal cell membrane. It alters membrane fluidity and permeability by affecting phospholipids and ergosterol components, creating structural disorganization.[24,25] As integrity declines, ions, proteins, and enzymes leak out uncontrollably, leading to the collapse of osmoregulatory systems.[24,29] Progressive membrane breakdown results in swelling, cytoplasmic disintegration, and eventually complete fungal lysis.[25,29]
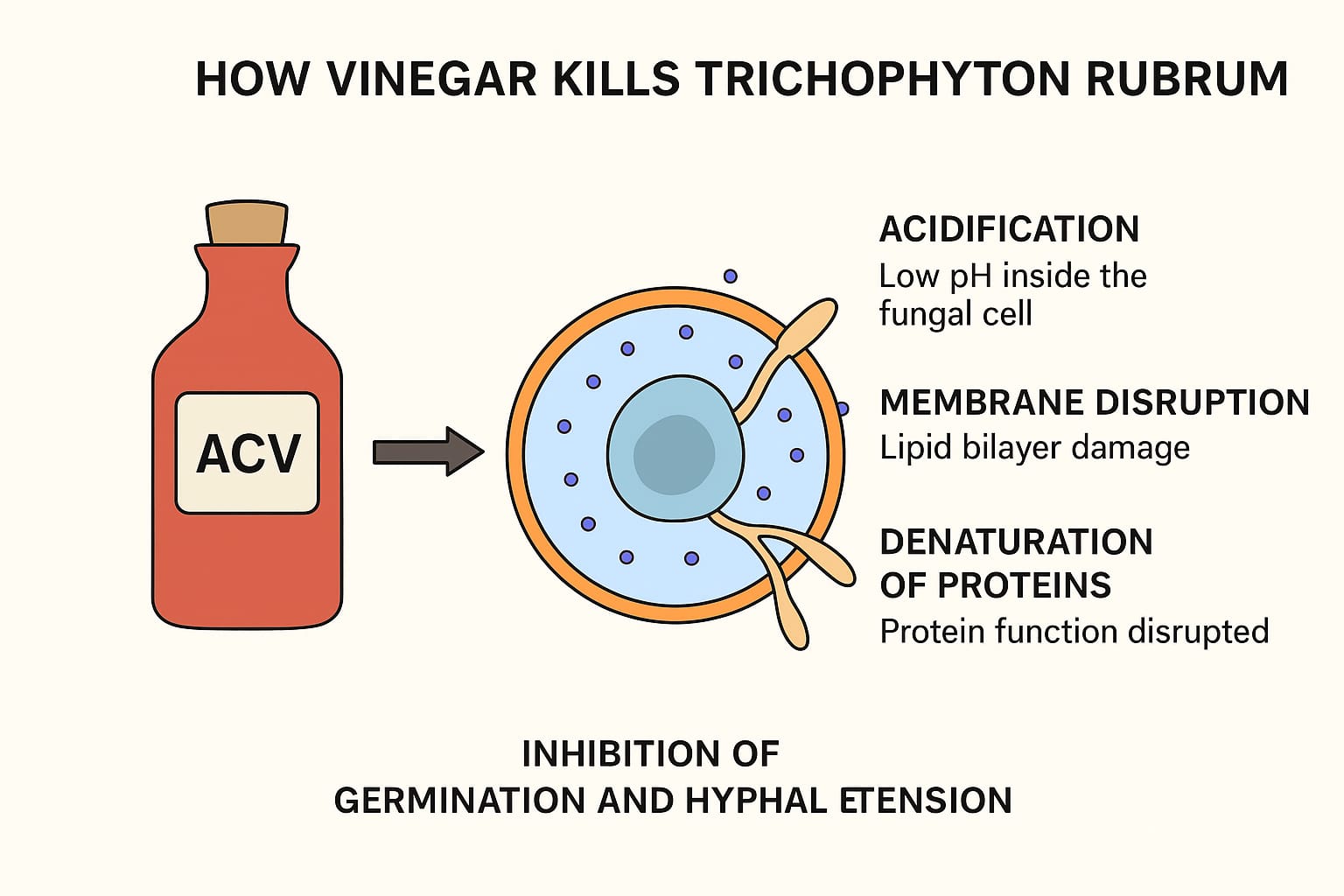
Fig 3. Mechanism of Action Of ACV.[21]
IN VITRO AND IN VIVO EFFICACY:
Laboratory data show acetic acid can inhibit fungi, though few studies target T. rubrum specifically. The Hong Kong study above demonstrated that no T. rubrum growth occurred at pH≤3, confirming acid’s inhibitory effect.[17] show in figure 4,

Fig 4. Experimental Evidence Demonstrates That Acetic Acid Effectively Inhibits Fungal.[38]
General disinfection assays support broad antifungal activity of vinegar: for example, standardized tests found 5% acetic acid eliminated >10^5 CFU of Candida albicans (a yeast) within 30 minutes.[30] In the Moroccan study of various apple vinegars, the sample with the highest acidity (~4%) showed “remarkable antimicrobial potency” against bacteria and yeast. Though that study did not include T. rubrum, it underscores that higher acetic acid content yields stronger fungicidal activity.[31] A veterinary dermatology study reported extremely low MICs of acetic acid against dermatophytes: for T. mentagrophytes (a species closely related to T. rubrum), the MIC of acetic acid was 0.28 μg/ml similar to terbinafine 0.295 μg/mL—and much lower than MICs of fluconazole or griseofulvin. (For Microsporum canis, acetic acid MIC≈1.05 μg/mL In that study, fluconazole and other azoles showed minimal activity against) dermatophytes, whereas acetic acid and terbinafine were most potent.[33] These data suggest acetic acid can inhibit dermatophytes in vitro at levels comparable to standard antifungals.[32] Clinically, data are limited. In a 2018 RCT on mild-to-moderate onychomycosis, daily application of a water-based acetic acid nail lacquer (peelable polish) was compared to weekly 5% amorolfine lacquer. After 180 days, both groups showed similar modest improvement: the mean healthy nail surface increased by 11.8% in the ACV group vs 13.2% in the amorolfine group.[34] “Improvement or success” (clinically judged) was 96.0% with daily ACV vs 79.6% with amorolfine.[35] thus, topical acetic acid performed comparably to a standard antifungal in this trial.[36] (This study likely included mostly T. rubrum and T. interdigitale, the usual onychomycosis pathogens, though culture data were not specified. No significant adverse events occurred in either group.[32] In contrast, no high-quality trials have tested ACV for T. rubrum tinea pedis (athlete’s foot). One health source notes there are “no studies” on vinegar foot soaks for tinea pedis.[34] Consequently, efficacy claims for ACV soaks derive mainly from theory and anecdote. Some practitioners propose nightly 1:1 vinegar–water soaks (giving ~2.5–5% acetic acid) to acidify the skin, but this is not evidence-based. As one review summarizes: home remedies like vinegar are “sometimes recommended” but “none…have been tested in good-quality studies. In short, in vitro data show acetic acid can inhibit dermatophytes at low pH, and one in vivo study (a nail trial) found acidification comparable to topical therapy. But we lack definitive clinical evidence for ACV against T. rubrum infections of skin or nails. Conventional antifungals target ergosterol or cell division specifically. Allylamines (terbinafine) and azoles (itraconazole, fluconazole) have known MICs against T. rubrum. In vitro, terbinafine MICs for dermatophytes are typically 0.01–0.1 μg/mL, while many T. rubrum isolates have fluconazole MICs in the 1–16 μg/mL range (often clinically resistant).[17] By comparison, the veterinary study above suggests acetic acid’s MIC (0.28 μg/mL) is in the same ballpark as terbinafine.[36] In that study T. mentagrophytes viability was “lowest” with acetic acid, followed closely by terbinafine. Fluconazole, however, had essentially no effect (MIC >>100 μg/mL) in those tests.[37] This implies ACV’s non-specific acidity can rival allylamine potency in vitro, whereas azoles show little activity. However, no trials have directly compared ACV to systemic antifungals in patients. The nail lacquer trial showed ACV ≈ topical amorolfine[38], but neither group was systemic. In practice, standard antifungals typically achieve higher cure rates; ACV’s benefit appears limited to acid pH rather than a targeted drug mechanism
LIMITATIONS AND CONFLICTING FINDINGS :
Several limitations temper enthusiasm for ACV;
(1) Skin barrier effects: Prolonged low pH exposures can damage the stratum corneum. The HK study noted that enzymes critical for skin lipid processing (e.g. β-glucocerebrosidase) require pH ≈5.6; exposure to pH?3.5 (as in vinegar soaks) can disrupt these enzymes and lipid synthesis, impairing barrier function[39]. Chronic foot soaking at high acidity may dry or weaken skin.
(2) Incomplete nail penetration: In the nail model, even 120 daily applications only acidified the superficial 0.5 mm of nail to ~pH3.4. [40] T. rubrum often resides deeper under the nail or in skin folds, so fungus may escape superficial acid. The authors concluded it is “difficult to achieve a fungicidal pH of 3.0 in the nail bed” with topical vinegar.[41]
(3) Lack of clinical trials: As noted, no controlled trials have demonstrated an actual mycological cure of T. rubrum infection using ACV alone. Prominent sources explicitly caution this gap: a German health review states that while vinegar soaks are sometimes recommended, “none of the home remedies [including cider vinegar] have been tested in good-quality studies.[36] Cleveland Clinic similarly notes that “nobody’s really researched the effect [of ACV] on athlete’s foot” and warns that it can cause chemical burns.[37] In short, enthusiasm is based on lab pH theory, but “real-world” efficacy is unproven and may be overestimated.
SAFETY AND TOLERABILITY:
Dilute ACV is generally safe on intact skin, but caution is needed. Acetic acid is an irritant: topical vinegar can cause burning, stinging, or dermatitis. The Cleveland Clinic points out that while ACV has disinfectant properties, its acetic acid content “can cause a chemical burn.”[37] An agricultural publication warns that solutions ≥11% acetic acid (much stronger than household vinegar) will burn skin and eyes.[38,39] Even 5% vinegar can irritate sensitive skin or open wounds. Case reports exist of vinegar plus other agents causing skin burns. Allergic contact dermatitis to vinegar is possible (nickel in vinegar can trigger reactions)[40] .on the other hand, in the 6-month onychomycosis trial, daily acetic acid lacquer was well tolerated with no reported side effects.[34] This suggests that controlled formulations (e.g. dilute, pH-buffered solutions or lacquers) can be safe. Nevertheless, experts recommend testing ACV on a small skin area first and avoiding high concentrations or prolonged soaking, especially on thin or eczema-prone skin.[37,40] ACV should not be used near mucous membranes or eyes. In summary, while ACV at ~5% is not highly toxic, misuse (high strength or extended exposure) risks burns and barrie damage.[40]
FUTURE PROSPECTS:
Apple Cider Vinegar (ACV) has shown strong antifungal activity against Trichophyton rubrum in laboratory studies, its therapeutic use still needs scientific validation. Future research should focus on advanced delivery systems such as nano-emulsion gels, trans-ungual patches, or medicated lacquers that can improve vinegar penetration through the hard nail plate. These innovations may enhance its effectiveness while reducing irritation.
CONCLUSION:
The conclusion of the document states that apple cider vinegar at a 5% concentration shows significant antifungal effectiveness against Trichophyton rubrum and can be considered a promising supportive treatment for onychomycosis. Its therapeutic potential is primarily attributed to acetic acid, which lowers pH, disrupts fungal enzymatic activity, interferes with keratin degradation, and ultimately weakens fungal growth. When used consistently, ACV leads to noticeable improvements in nail clarity, shape, color, and texture, confirming its ability to reduce fungal activity within the nail environment. Additionally, the study emphasizes ACV’s advantages over conventional antifungals, particularly its safety, availability, affordability, and lack of adverse effects. These qualities make ACV an appealing option for individuals seeking natural or low-cost treatments, as well as those who cannot tolerate prescription antifungals. The document also suggests that ACV may have potential usefulness in the management of other dermatophyte infections, though additional clinical investigation is needed. While ACV may not fully replace pharmaceutical treatments in severe infections, it shows strong potential as a complementary or early-stage therapy. The study encourages its continued use due to the slow growth rate of nails and the chronic nature of onychomycosis. Overall, ACV is presented as an effective, natural, and safe intervention that lowers fungal activity, enhances nail appearance, and provides relief without chemical toxicity. Its performance in the study supports its value as a natural antifungal option and encourages further research into its broader dermatological applications.
REFERENCES:
http://www.aafp.org/afp
http://www.aafp.org/afp


Dipti Kavatkar*, Om Iche, Bhvana Shinde, Arpit Shinganjude, Dipali Doifode, Pharmacological Review of Apple Cider Vinegar on The Treatment of Onychomycosis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1039-1049. https://doi.org/10.5281/zenodo.18513346
 10.5281/zenodo.18513346
10.5281/zenodo.18513346