Department of Pharmacy, Institute of Technology and Management, GIDA, Gorakhpur, Uttar Pradesh, India, 273209.
Polycystic ovary syndrome (PCOS) is a widespread condition in women that affects hormone levels and metabolism. A key element of PCOS is insulin resistance, which occurs when the body's cells don't respond effectively to insulin, resulting in elevated insulin levels. This exacerbates hormonal imbalances, leading to ovarian issues like irregular egg release and potential infertility. Insulin resistance also heightens the risk of developing type 2 diabetes, obesity, high cholesterol, and heart diseases, posing significant long-term health challenges. Furthermore, it can contribute to mental health problems such as depression and anxiety, negatively impacting the quality of life. This discussion delves into the role of insulin resistance in PCOS, its importance in disease progression, and how it is diagnosed. It covers treatments designed to address insulin resistance, including drugs like metformin and thiazolidinediones, alongside lifestyle modifications such as improved diet and regular physical activity. Emerging treatments, like inositol supplements and other natural remedies, are also examined. Consideration is given to the timing of treatments to enhance effectiveness. Understanding the impact of insulin resistance in PCOS is essential for creating effective management plans to improve the metabolic, reproductive, and mental well-being of women affected by this condition.
Polycystic ovary syndrome (PCOS) is a hormonal disorder in women that impacts reproductive and metabolic health. It leads to irregular menstrual cycles, high levels of male hormones, and ovaries with multiple cysts. PCOS affects about 6-13% of women in their reproductive years. Insulin resistance is a key problem in PCOS, where the body doesn't use insulin effectively, causing fertility issues and increasing the risk of developing type 2 diabetes and heart disease. The Rotterdam criteria are used to diagnose PCOS, requiring two of these three symptoms: irregular periods or not ovulating, high male hormone levels, and cystic ovaries. This results in four types of PCOS: O–H–P (ovulatory, high male hormones, and cystic ovaries), H–P (high male hormones and cystic ovaries), O–H (ovulatory and high male hormones), and O–P (ovulatory and cystic ovaries). The O–H–P type is most linked to insulin resistance, being about 2.5 times more likely to include insulin resistance than the other types [1]. Research indicates that up to 80% of women with PCOS (Polycystic Ovary Syndrome) experience insulin resistance, which can worsen their symptoms and raise the risk of metabolic disorders. This reduced sensitivity to insulin results in hyperinsulinemia, where there is an excess of insulin in the bloodstream. This condition not only contributes to weight gain but also triggers the ovaries to produce more male hormones, known as androgens. The rise in androgen levels further aggravates hyperandrogenism, leading to symptoms such as increased hair growth, acne, and irregular menstrual cycles [1], [2]. In PCOS, insulin resistance is caused by a combination of genetic factors and external influences like obesity. Having more body fat raises the levels of inflammatory substances, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). These substances disrupt the body's ability to use insulin effectively, leading to more severe metabolic problems [1], [3]. Understanding the challenges posed by insulin resistance in women with PCOS is key to proper management and treatment. This condition can lead to serious health problems, including type 2 diabetes, high cholesterol, and high blood pressure. It also disrupts reproduction by making ovulation difficult and causing issues during pregnancy. Additionally, PCOS can negatively affect mental health, often resulting in anxiety and depression, particularly because of visible symptoms like excessive hair growth and weight gain. By recognizing these issues, healthcare providers can develop more effective treatment plans that address both health and reproductive concerns related to PCOS. In conclusion, the relationship between insulin resistance and PCOS emphasizes the importance of continued research and tailored treatments to alleviate both immediate symptoms and long-term health risks. Identifying various forms of PCOS can assist in predicting adverse metabolic outcomes and enhancing management strategies [1], [4].
2. Pathophysiology of Insulin Resistance in PCOS
In polycystic ovary syndrome (PCOS), the body develops insulin resistance (IR) because several factors disrupt how insulin works. This disruption affects both metabolism and reproductive health. As a result, women with PCOS often experience high levels of male hormones, difficulties managing blood sugar, and an increased risk of developing type 2 diabetes.
Mechanisms of Insulin Resistance in PCOS:
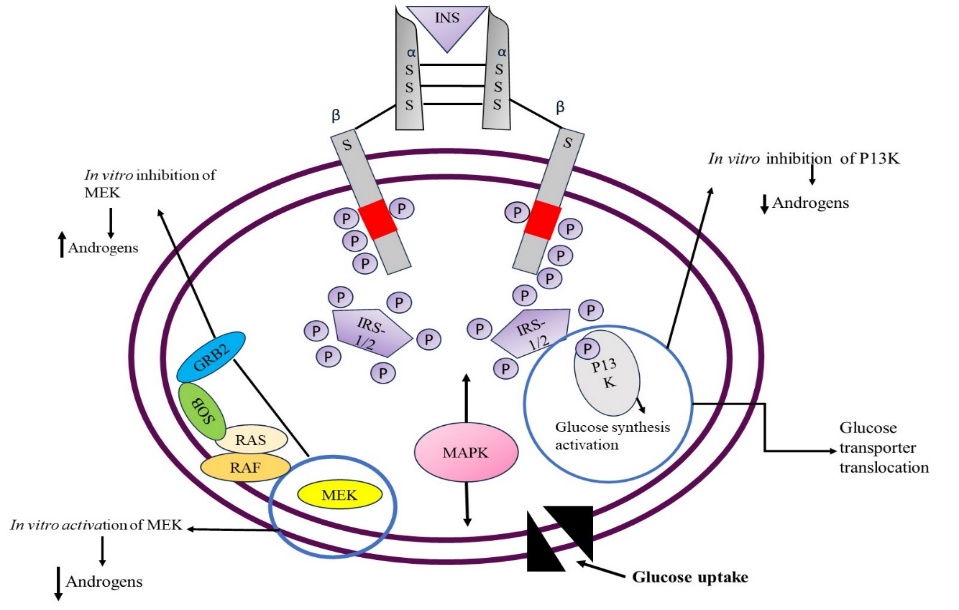
Figure 1. Molecular mechanism of insulin resistance in PCOS
Post-Receptor Defects in Insulin Signaling
In women with PCOS, insulin resistance is mainly due to issues that occur after insulin binds to its receptor, not because of changes in receptor numbers or binding ability. Studies show that even though insulin binds as expected, the signaling afterward is impaired. This particularly affects a pathway involving insulin receptor substrate (IRS)-1 and phosphatidylinositol 3-kinase (PI3K), crucial for glucose uptake. This defect is an inherent part of PCOS and is not due to obesity or type 2 diabetes [5].
Increased Serine Phosphorylation of Insulin Receptors
In people with PCOS, insulin resistance is often marked by unusual serine phosphorylation of insulin receptors. This change decreases the effectiveness of the receptors by reducing tyrosine kinase activity, which insulin needs to work correctly. Studies indicate that when serine phosphorylation increases, it creates issues with the receptors activating themselves. This makes it more difficult for insulin to control glucose metabolism, which is essential for providing energy to the body [6], [7]. The presence of serine kinases in this process shows that there could be an outside factor affecting the phosphorylation patterns seen in individuals with PCOS (Polycystic Ovary Syndrome) [5].
Role of Hyperinsulinemia and Compensatory Mechanisms
Having too much insulin in the blood, known as hyperinsulinemia, can both lead to and result from insulin resistance in women with PCOS (Polycystic Ovary Syndrome). When insulin levels are elevated, it causes the theca cells in the ovaries to produce more male hormones, called androgens. Additionally, the increased insulin levels enhance the activity of luteinizing hormone (LH), which further raises androgen levels. This combination makes the condition of having too many male hormones, or hyperandrogenism, even worse [8], [9]. When the body struggles with insulin response, it compensates by boosting IRS-2 in muscles to improve insulin effectiveness. Despite this effort, it's not enough to fully correct sugar management, so metabolic issues continue [5].
Genetic and Environmental Influences on Insulin Resistance
Insulin resistance in women with PCOS (Polycystic Ovary Syndrome) is influenced by both genetic and environmental factors. Certain genes can increase the risk of insulin-related issues by interfering with how the body uses energy, leading to insulin resistance. Environmental aspects like excess weight, an unhealthy diet, and exposure to harmful chemicals can worsen this condition. Being overweight is a major concern because it causes persistent, mild inflammation and disrupts body chemicals known as adipokines. This inflammation and chemical imbalance make it harder for the body to react properly to insulin, resulting in metabolic problems that affect how the body processes food into energy [10].
3. Metabolic Complications Due to Insulin Resistance in PCOS
Polycystic ovary syndrome (PCOS) is a complex condition affecting hormones and causing serious metabolic problems due to insulin resistance. This resistance means the body doesn't use insulin properly, which affects blood sugar levels. PCOS significantly raises the risk of developing Type 2 Diabetes Mellitus (T2DM). In T2DM, the body can't effectively use insulin, resulting in high blood sugar levels. Obesity is another problem associated with PCOS, which heightens the risk of metabolic syndrome. Metabolic syndrome includes conditions like high blood pressure, high blood sugar, extra fat around the waist, and abnormal cholesterol levels, all of which increase the chances of heart disease, stroke, and diabetes. Additionally, PCOS can lead to dyslipidemia, characterized by unhealthy levels of lipids, such as cholesterol and triglycerides, in the blood. This imbalance can cause cardiovascular disease (CVD), which affects the heart and blood vessels. Thus, PCOS can lead to significant metabolic and cardiovascular issues, making it crucial to understand and manage these risks to maintain better health.
3.1. Type 2 Diabetes Mellitus (T2DM)
Women with Polycystic Ovary Syndrome (PCOS) face a significantly higher risk of developing type 2 diabetes (T2DM), being four times more likely to receive a diagnosis than those without the condition. Additionally, T2DM tends to develop earlier in these women, often around the age of 31. The connection between insulin resistance (IR) and pancreatic β-cell dysfunction is crucial in the progression of the disease. Approximately 70% of women with PCOS experience insulin resistance, which prompts their bodies to produce extra insulin in an attempt to compensate. However, this compensation eventually becomes insufficient, leading to β-cell dysfunction in the pancreas. This dysfunction results in consistently high blood sugar levels, known as persistent hyperglycemia, which is a key characteristic of diabetes [11], [12].
Doctors suggest that women with PCOS adopt healthier eating habits and increase physical activity to manage and prevent Type 2 Diabetes. Research indicates that those at risk can delay or prevent diabetes by consistently following a structured plan of these lifestyle changes. This approach helps with weight control and enhances the body's use of insulin, which contributes to delaying the onset of diabetes [13]. Medications such as metformin are often used to improve how the body responds to insulin and assist in managing weight. However, their effectiveness can differ among individuals [12].

Figure 3. Cyclic progression of PCOS where insulin resistance fuels obesity, worsening metabolic and hormonal imbalances
3.2. Obesity and Metabolic Syndrome
People with PCOS often have extra fat around the belly and organs, which contributes to metabolic syndrome. The fat around the organs, known as visceral fat, is closely linked to insulin resistance and is more concerning than the fat under the skin, called subcutaneous fat. Visceral fat can worsen insulin resistance and lead to inflammation in the body [14]. Women with PCOS frequently experience high blood pressure, abnormal cholesterol levels, and issues with sugar processing, all of which are indicators of metabolic syndrome. Studies reveal that as many as 75.8% of overweight or obese women with PCOS satisfy the criteria for metabolic syndrome [15]. Substances from fat cells and persistent mild inflammation play a key role in metabolism problems. In women with Polycystic Ovary Syndrome (PCOS), body fat releases inflammatory substances, which interfere with insulin function. This situation contributes to a group of health issues called metabolic syndrome [14], [15].
3.3. Dyslipidemia and Cardiovascular Disease (CVD)
Dyslipidemia, or having abnormal levels of fats in the blood, is a major concern for those with PCOS (Polycystic Ovary Syndrome). This condition often results in high levels of LDL (bad cholesterol), low levels of HDL (good cholesterol), and increased triglycerides. These changes in blood fats greatly increase the risk of developing heart disease. Women with PCOS often face additional challenges like high blood pressure and issues with blood vessel function, which further raise the likelihood of heart-related problems. Another important factor is oxidative stress, which plays a significant role in artery health for people with PCOS. When oxidative stress is high, it can cause damage to blood vessels, leading to the development of atherosclerosis. This process involves the buildup of fatty deposits in the arteries, increasing the risk of cardiovascular issues even more [16].
4. Reproductive and Endocrine Complications Due to Insulin Resistance
4.1. Hyperandrogenism and Menstrual Irregularities
Insulin resistance (IR) is a major reason why women with polycystic ovary syndrome (PCOS) have high androgen levels. Elevated insulin levels prompt the ovaries to produce more androgens because insulin, along with luteinizing hormone (LH), boosts enzymes responsible for hormone production. This primarily takes place in ovarian theca cells, leading to increased testosterone in the bloodstream. Consequently, women with PCOS often experience symptoms such as excessive hair growth (hirsutism), acne, and menstrual irregularities, including missed periods (anovulation) or infrequent periods (oligomenorrhea). Studies show that menstrual cycle problems in women with PCOS are closely linked to higher insulin resistance and excess insulin in the body [2], [17], [18]. When insulin resistance (IR) interrupts normal hormonal signals, it affects androgen levels and other hormones like sex hormone-binding globulin (SHBG). SHBG is a protein that helps control hormone levels in the blood. High insulin levels cause the liver to produce less SHBG, leading to more free androgens in the body. These free androgens can disrupt the normal development of follicles in the ovaries, resulting in irregular menstrual cycles. This means periods might not be regular or might not occur at all, posing challenges for women trying to monitor their cycles or conceive [2], [19].
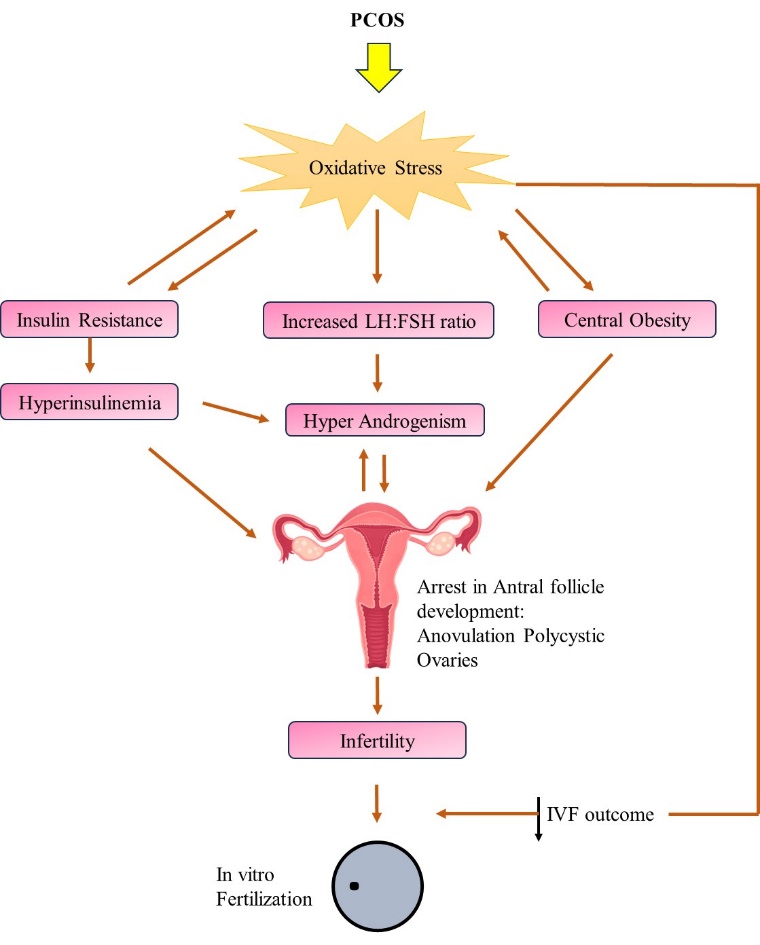
Figure 3. Polycystic ovary syndrome (PCOS) complications cause infertility
4.2. Infertility and Pregnancy Complications
Insulin resistance (IR) plays a major role in causing ovulation issues for women with polycystic ovary syndrome (PCOS), often leading to infertility. This occurs because hormonal imbalances from IR disrupt normal egg release. Additionally, women with PCOS have a higher risk of developing gestational diabetes mellitus (GDM), a type of diabetes that begins during pregnancy, and pregnancy-induced hypertension (PIH), which is high blood pressure triggered by pregnancy. Studies show that the metabolic problems linked to IR, such as elevated blood sugar and increased blood fats, raise the chances of GDM during pregnancy. Moreover, IR can affect the success of fertility treatments like in vitro fertilization (IVF). Women with PCOS and IR usually have fewer mature eggs collected during IVF, although their rates of fertilization and live births are similar to those of women without IR. This indicates that while IR might not influence every part of reproductive success, it does affect certain key factors crucial for successful fertility treatments [20].
5. Neurological and Psychological Complications Due to Insulin Resistance
5.1. Mood Disorders and Cognitive Dysfunction
Insulin resistance (IR) has been linked to an increased risk of mood disorders, including depression and anxiety, particularly in women with polycystic ovary syndrome (PCOS). A study found that elevated levels of the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) were associated with a 2.3-fold increase in the odds of depression among women with PCOS, even after adjusting for confounding factors such as age and body mass index (BMI) [21]. This suggests that insulin resistance may act as a physiological mediator of depression in this population. Furthermore, metabolic disturbances, including IR, have been implicated in cognitive dysfunction, with evidence indicating that women with PCOS show lower cognitive performance and white matter integrity at midlife compared to their non-PCOS counterparts [22]. The mechanisms behind these associations may involve altered insulin signaling in the brain, which is crucial for cognitive health [11].
5.2. Sleep Disorders and Obstructive Sleep Apnea (OSA)
Insulin resistance is also associated with sleep disorders, including obstructive sleep apnea (OSA), particularly in obese individuals with PCOS. The interplay between IR, obesity, and sleep disturbances can exacerbate metabolic dysfunctions [22]. Poor sleep quality has been shown to negatively impact metabolic health, contributing to further complications in individuals with insulin resistance. The relationship between these factors underscores the importance of addressing sleep issues in the management of metabolic disorders associated with PCOS [11].
6. Therapeutic Approaches Targeting Insulin Resistance in PCOS
Table 1. The various types of approaches targeting IR in PCOS
|
Category |
Intervention |
Mechanism of Action |
Benefits |
Limitations |
|
Pharmacological Interventions |
Metformin |
Reduces hepatic glucose production and increases insulin sensitivity |
Improves ovulation, menstrual regularity, and reduces androgen levels |
Variable effects on hormone production; potential gastrointestinal side effects |
|
|
Thiazolidinediones (TZDs) |
Enhances insulin sensitivity in fat and muscle tissues by increasing glucose transporter expression |
Improves ovulation and pregnancy rates, decreases insulin resistance |
Potential risks like weight gain, edema, and long-term safety concerns |
|
Lifestyle Modifications |
Low-GI & High-Fiber Diet |
Reduces postprandial glucose spikes, improves insulin function |
Decreases HOMA-IR, improves metabolic health |
Requires long-term dietary adherence |
|
|
Aerobic & Resistance Exercise |
Increases glucose uptake and insulin receptor activity |
Reduces insulin resistance, aids weight loss, improves overall metabolic health |
Consistency required for long-term benefits |
|
Emerging Therapies |
Myo-inositol |
Enhances insulin signaling and glucose metabolism |
Reduces insulin resistance, improves menstrual regularity and fertility |
Effectiveness may vary based on dosage and individual response |
|
|
D-chiro-inositol (DCI) |
Regulates insulin metabolism and reduces free testosterone levels |
Lowers insulin levels, enhances ovulation |
Requires proper Myo-inositol: DCI balance |
|
|
Nutraceuticals (Cinnamon, Ginseng, Licorice) |
Modulates glucose metabolism and enhances insulin action |
Lowers blood sugar and lipid levels, supports metabolic health |
Lack of standardized dosages and clinical trials |
|
|
Herbal Remedies (Vitex agnus-castus, Stachys lavandulifolia) |
Reduces androgen levels and improves menstrual cycles |
Potential natural alternative to pharmacological treatments |
Requires further research for efficacy and safety |
|
|
Chronotherapy |
Aligns treatment timing with circadian rhythms for better metabolic control |
May optimize insulin sensitivity and improve treatment outcomes |
Requires more research for clinical application |
6.1. Pharmacological Interventions
6.2. Lifestyle Modifications
6.3. Emerging Therapies
7. Future Directions and Research Gaps
Future research on polycystic ovary syndrome (PCOS) and insulin resistance (IR) should focus on several important areas. Personalized medicine is one key aspect, which means adjusting medical treatment to fit each patient's unique traits. This approach can make treatments for PCOS and IR more effective. Another crucial area is identifying new molecular targets—specific molecules in the body that can be targeted by treatments. Discovering these targets could lead to the development of new and possibly more effective therapies. Additionally, examining the long-term outcomes of various treatments is essential. This involves studying how well these interventions perform over time, providing valuable information for both doctors and patients to make informed choices about managing PCOS and IR.
Personalized Medicine
Novel Molecular Targets
Long-Term Outcomes
CONCLUSION
Insulin resistance (IR) plays a significant role in polycystic ovary syndrome (PCOS), impacting both reproductive and metabolic aspects of health. IR contributes to elevated insulin levels, excess androgens, and ovarian dysfunction, leading to infertility and irregular menstrual cycles. It also elevates the risk of type 2 diabetes, obesity, high cholesterol, and cardiovascular disease. Moreover, IR's connection to depression and anxiety underscores the importance of a comprehensive treatment approach. Addressing IR in PCOS is vital for improving overall health. Medications like metformin and thiazolidinediones, combined with lifestyle changes such as healthier eating and regular exercise, are essential for improving insulin sensitivity and reducing health risks. Additionally, new treatments like inositols, nutraceuticals, and chronotherapy offer promising options for further enhancing patient outcomes. Given PCOS's impact on multiple health areas, a multidisciplinary treatment strategy is crucial. This should include hormone specialists, gynecologists, dietitians, and mental health professionals. Future research should focus on optimizing treatment methods, discovering new therapeutic targets, and understanding the long-term effects of interventions to enhance the quality of life for women with PCOS.
REFERENCES

Sonali Kumari*, Shweta Singh, Polycystic Ovary Syndrome (PCOS) Complications Due to Insulin Resistance: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 5176-5189. https://doi.org/10.5281/zenodo.15562289
 10.5281/zenodo.15562289
10.5281/zenodo.15562289
