Prin. K. M. Kundnani College of Pharmacy, 23, Jote Joy Building Rambhau Salgaonkar Marg, Cuffe Parade, Coloba, Mumbai – 400 005
The pharmaceutical landscape is constantly evolving, with drug developers seeking innovative pathways to bring new and improved therapies to patients. While generic formulations have traditionally played a crucial role in ensuring affordable access to medicines, the 505(b)(2) regulatory pathway has emerged as a strategic avenue for developing differentiated products that offer advantages over their generic counterparts. This review article explores the progressive trends in leveraging the 505(b)(2) pathway to create novel formulations that address unmet clinical needs, enhance patient compliance, improve drug efficacy and safety, and ultimately provide added value beyond that offered by conventional generic equivalents. We will delve into the key drivers behind this trend, the various formulation strategies employed, and the implications for both pharmaceutical companies and patients.
Generic drug development traditionally follows the 505 (j) pathway under the abbreviated new drug application (ANDA) system, focusing on bioequivalence without innovation. In contrast, the 505 (b) (2) pathway under the federal food and drug cosmetics Act permits reliance on existing clinical data, allowing for formulation innovation, new indications, altered dosages and novel routes of administration. The Hatch-Waxman Amendments of 1984 established a balance between incentivizing pharmaceutical innovation and facilitating timely generic drug entry (U.S. Congress, 1984). While the Abbreviated New Drug Application (ANDA) pathway (Section 505(j) of the Federal Food, Drug, and Cosmetic Act) allows for the efficient approval of generic drugs based on demonstrating bioequivalence to a reference listed drug (RLD), it inherently limits the ability to introduce meaningful product differentiation. Section 505(b)(2) provides an alternative regulatory pathway for new drug applications (NDAs) that rely, in part, on data not developed by the applicant and for which the applicant has not obtained a right of reference (Food and Drug Administration, 1999). This pathway allows applicants to leverage the FDA's prior findings of safety and efficacy for an approved drug (the RLD) while introducing their own non-clinical and/or clinical data to support changes such as a new strength, dosage form, route of administration, or formulation.
Over the past decade, there has been a noticeable increase in the strategic utilization of the 505(b)(2) pathway to develop formulations that go beyond simple generic equivalents. This trend is driven by several factors, including the desire for product differentiation in increasingly crowded generic markets, the opportunity to address specific patient needs, the potential for securing market exclusivity, and the ability to create intellectual property around novel formulations. This review aims to highlight the progressive formulation trends within the 505(b)(2) space that offer significant advantages over traditional generic formulations.
2. Understanding of 505 (b)(2) vs. 505 (j) (ANDA)
The U.S. Food and Drug Administration (FDA) provides two major regulatory pathways for the approval of small-molecule drugs: the 505 (j) pathaway for generic and and the 505 (b)(2) pathway for modified or improved version of the previously approved drug.
|
Aspect |
Generic drug development (ANDA) 505 (j) pathway |
505 (b)(2) development pathway |
|
Regulatory pathway |
Abbreviated New Drug Application (ANDA) |
505 (b)(2) New Drug Application |
|
Primary references |
Reference a previously approved brand- name drug (RLD – Reference Listed Drug or a RS – Reference standard) |
Can reference data from a previously approved drug but includes new studies or data |
|
Clinical studies |
Bioequivalence study only; no needs for full clinical trials. |
|
|
Nature of modification |
No innovation; must be bioequivalent to the reference drug |
Allows for innovation (eg. New delivery system, new dosage form, combination drugs, new indication, new patient age group or new dosing recommendation) |
|
FDA review time |
Shorter review time (generally 10 months) due to reliance on bioequivalence. |
Longer review time depending on the extent of the additional bridging requirements (typically 12 – 15 months) |
|
Development cost |
Lower cost compared to innovator and 505 (b)(2) formulation as only bioequivalence study required. |
Higher cost compared to generic, due to potential needs of additional clinical studies and higher submission fees. |
|
Approval requirements |
Must demonstrate bioequivalence to RLD |
Bioequivalence in fasting to bridge the safety and efficacy to the approved RLD. Must provide new clinical data supporting the modification or changes, but can use existing data for other aspects. |
|
Patent and exclusivity |
Can challenge patents under Hatch – Waxman Amendment Act via paragraph IV certification , granting 180 days exclusivity to the first filer |
May qualify for new patents and market exclusivity (3-7 years) depending on the type of studies.
|
|
Labeling |
Labeling must be identical to the reference drug (except for manufacturer details) |
Labeling may be different if the drug has new indication, route of administration, different dosing recommendation or formulation. |
|
Intellectual property |
Generic drug companies often file a paragraph IV certification to challenge the innovator patent |
Can file new patents on the changes made ( e.g., new formulation, indication), rather than challenging existing ones. |
|
Time to market |
Quicker to market (after patent expiration or successful paragraph IV challenges) |
Longer to the market due to additional clinical trials or changes to the original drug formulation. |
|
Risk |
Lower development risk due to reliance of proven data |
Higher development risk due to new clinical trial and additional regulatory scrutiny. |
|
Target market |
Patients seeking more affordable version of branded drug. |
Patients needing improvements in existing therapies, like new delivery methods, extended release formulation, etc. |
|
Reference |
1.https://www.raps.org/news-and-articles/news-articles/2020/6/505b2-applications-opportunities-challenges-and 2. https://www.fda.gov/drugs/types-applications/drug-application-process 3. https://www.fda.gov/media/94331/download |
|
3. Drivers for the Shift Towards Differentiated 505(b)(2) Formulations:
Several key factors are fueling the increasing interest in developing differentiated 505(b)(2) formulations:
4. 505 (b)(2) submission classification types [25]: -
4.1 New molecule entity submission continue to grow
Through Type 5 (new formulation and other differences ) and Type 3 (new dosage form ) NDA submission together continue to account for more than half of all 505 (b)(2) approvals, Type 1 (new molecular entity) submission increased sharply from 5% in 2019 to 18% in 2020 (Figure 1),
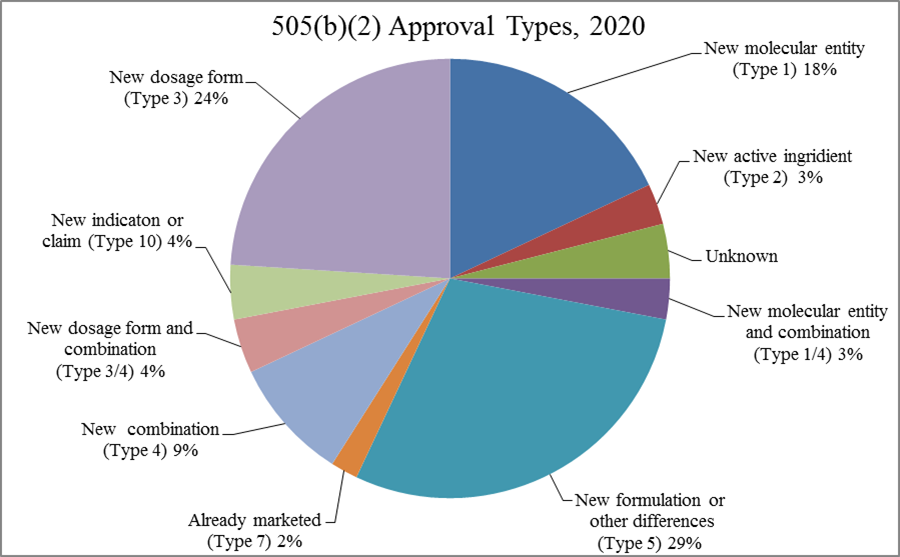
Figure 1 – 2020 505 (b)(2) approval by its types
4.2 Rare disease 505 (b)(2) approvals –
Developing strategies that leverage the 505 (b)(2) regulatory pathway can be particularly relevant with rare disease patient populations, for which full phase 1-3 clinical development programs may not be feasible. As shown in Figure, 2 more than one third (36%) of NDA approvals for orphan drug were developed via the 505 (b)(2) pathway.
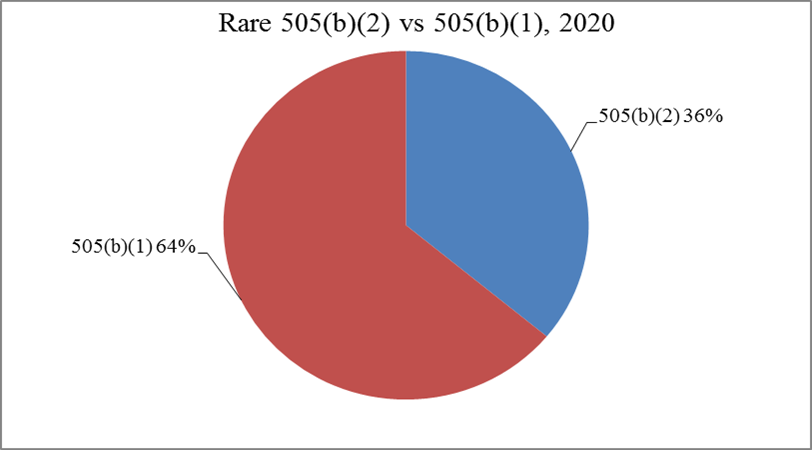
Figure 2 – 2020 CDER NDA approvals of orphan drugs.
5. Progressive Formulation Strategies in 505(b)(2) Development:
The 505(b)(2) pathway enables the development of a wide range of innovative formulations that offer advantages over generic equivalents. Some progressive trends include:
5.1 Modified Release Formulations:
1.Extended-Release (ER): Formulations designed to release the drug over a prolonged period, allowing for less frequent dosing (e.g., once daily instead of multiple times a day). This improves patient compliance and can reduce fluctuations in drug concentration, potentially minimizing side effects (Verma et al., 2010). Examples of extended release 505 (b)(2) formulation include oxycontin® [Extended Release OxyContin (NDA 022272)] and Glumetza®[ Glumetza (metformin hydrochloride extended-release) (NDA 021723)].
Table – Examples of extended release 505 (b)(2) formulation.
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
oxycontin® |
Oxycodone |
Polymer matrix for 12 hour controlled release |
Twice daily dosing better pain management |
505 (b)(2) ) NDA 20-553 |
|
Glumetza® |
Metformin |
Gastro-retentive system (GRDDS) |
Once daily dosing improved GI tolerability |
505(b)(2) NDA 021748 |
2. Delayed-Release (DR):
Formulations designed to release the drug at a specific point in the gastrointestinal tract, often to protect the drug from degradation in the stomach or to target drug delivery to the intestines. Enteric-coated tablets are a common example (Behrens et al., 1991). Examples of Delayed release 505 (b)(2) formulation include Zegerid® DR [Zegerid Delayed-Release (NDA 021849)] and Doryx® DR[Doryx Delayed-Release (NDA 050795)].
Table – Examples of Delayed release 505 (b)(2) formulation.
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Zegerid® DR |
Omeprazole + sodium bicarbonate |
Immediate buffer + delayed enteric release |
Rapid symptom relief + acid protection |
505 (b)(2) FDA NDA 021636 |
|
Doryx® DR |
Doxycycline hyclate |
Delayed release coated pellets |
Reduced GI irritation from antibiotics |
505 (b)(2) FDA NDA 050795 |
Formulations designed to release the drug in distinct bursts at specific times, mimicking the body's natural rhythms or targeting specific disease states (Gharse et al., 2012). Examples of pulsatile release 505 (b)(2) formulation include Covera-HS® [Covera-HS (NDA 020552)] and Uniphyl® [Uniphyl (NDA 018092)]
Table – Examples of pulsatile release 505 (b)(2) formulation.
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Covera-HS® |
Verapamil hydrochloride |
Delayed + pulsatile release (chronotherapeutics) |
Taken at bed time. Drug release early morning (when BP normally spikes) |
505 (b)(2) FDA NDA 020552 |
|
Uniphyl® |
Theophylline |
Delayed and sustained release. |
Once a daily dosing used in Nocturnal asthma |
505 (b)(2) FDA NDA 018092 |
5.2 Novel Dosage Forms:
Orally Disintegrating Tablets (ODTs):
Tablets that rapidly dissolve or disintegrate in the mouth without the need for water, improving ease of administration for patients with dysphagia (swallowing difficulties), children, and the elderly (Dobetti, 2001). Examples of ODT formulation include Abilify Discmelt® ODT [Abilify Discmelt (NDA 021729)]
Table – Examples of ODT
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Abilify Discmelt® ODT |
Aripiprazole |
ODT for psychiatric disorders |
Antipsychotic for schizophrenia and bipolar disorder. Used where patient may refuse or cannot swallow tablets. |
505 (b)(2) FDA NDA 021729 |
Thin Films:
Drug-loaded polymeric films that dissolve rapidly in the mouth, offering a convenient and discreet alternative to traditional tablets or capsules (Dixit & Shivhare, 2011). Examples of thin films include Bunavail® buccal film [Bunavail (NDA 205637)] and Exservan® oral film [Exservan (NDA 212640)].
Table – Examples of thin films
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Bunavail® buccal film |
Buprenorphine + Naloxone |
Buccal film technology (Bioerodible mucoadhesive BEMA®) |
Opioid use disorder. Better absorption compared to standard sublingual tablets. |
505 (b)(2) FDA NDA 2056637 |
|
Exservan® oral film |
Riluzole |
Thin film for ALS. (Amyotrophic lateral sclerosis) |
Treats ALS. Designed for patient with difficulty swallowing (very common in ALS) |
505 (b)(2) FDA NDA 212640 |
Chewable Tablets:
Palatable formulations that can be easily chewed and swallowed, particularly beneficial for pediatric patients (Allen & Popovich, 2004). Examples of chewable tablets includes Methylin® Chewable Tablets [Methylin Chewable Tablets (NDA 021475)].
Table – Examples of chewable tablets
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Methylin® Chewable Tablets |
Methylphenidate |
Chewable tablets for padeatric ADHD |
ADHD medication adapted for children Avoids need for swallowing pills. |
505 (b)(2) FDA NDA 021475 |
Liquids, Solutions, and Suspensions:
Formulations that offer ease of swallowing and can be easily dosed, especially important for pediatric and geriatric populations. Taste-masking technologies are often employed to improve palatability (Soppimath et al., 2001). Example of suspension include EOHILIA® [Eohilia (NDA 213976)]
Table – Example of suspension
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
EOHILIA® |
Budesonide |
First oral treatment for EoE, viscous formulation optimizes esophageal contact |
Non - invasive alternative to steroids or endoscopic intervention, better mucosal contact. |
505 (b)(2) FDA NDA 213976 |
5.3 Combination Products with Enhanced Value:
Combining two or more active ingredients into a single dosage form can simplify treatment regimens, improve patient compliance, and potentially offer synergistic or additive therapeutic effects (Osterberg & Blaschke, 2005). 505(b)(2) allows for the development of novel FDCs based on previously approved single entities. Example of fixed dose combination include Tecentriq Hybreza® [Tecentriq Hybreza (BLA 761347)].
Table – Example of fixed dose combination
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
Tecentriq Hybreza® |
Atezolizumbab /Hyaluronidase |
First subcutaneous anti-PD-L(1) cancer immunotherapy |
Facilitates faster administration ; reduce clinic time; maintains therapeutic efficacy |
505 (b)(2) FDA BLA 761347 |
Integrating drug formulations with delivery devices (e.g., pre-filled pens, autoinjectors) can improve ease of use, accuracy of dosing, and patient convenience, particularly for self-administered medications (EMA, 2019) [ MiniMed 770G (PMA P160017/S076)].
|
Product |
Drug |
Innovation |
Advantages |
Approval pathway |
|
MiniMed™770G system |
Insulin |
Automated insulin delivery for young children (insulin pump with continuous glucose monitoring) |
Real time glucose monitoring, automated insulin adjustment; enhance safety |
505 (b)(2) FDA PMA P160017 |
5.4 Switches from prescription product to OTC product -
The transition from prescription (Rx) to over-the-counter (OTC) products using the 505(b)(2) regulatory pathway is a growing trend in drug development. This transition is often driven by a combination of regulatory flexibility, commercial strategy, and patient-centric innovation.
Examples -
1) Zyrtec OTC (Cetirizine)
Original Rx Indication: Allergic rhinitis and chronic urticaria.
OTC Indication: Relief of allergy symptoms.
505(b)(2) Innovation: Utilized pediatric and adult safety data to support OTC use.
Approval Year: 2008
Reference: FDA Zyrtec Info
2) Prilosec OTC (Omeprazole)
Original Rx Indication: Treatment of GERD, ulcers, and other acid-related disorders.
OTC Indication: Relief of frequent heartburn.
505(b)(2) Innovation: Re-labeled for self-limited OTC use with a 14-day regimen.
Approval Year: 2003
Reference: FDA Announcement
5.5 Advanced Drug Delivery Systems:
Utilizing nanotechnology to enhance drug solubility, bioavailability, and targeted delivery to specific tissues or cells, potentially improving efficacy and reducing systemic side effects (Ferrari, 2005).
Encapsulating drugs within liposomes (vesicles composed of lipid bilayers) can improve drug stability, prolong circulation time, and enhance drug delivery to target sites (Gregoriadis, 2016).
Incorporating drugs into small polymeric spheres for controlled release over extended periods, often administered via injection (Freiberg & Zhu, 2004).
Developing pharmacologically inactive derivatives of an active drug that undergo enzymatic or chemical conversion in the body to release the active drug. This strategy can improve drug solubility, permeability, stability, or reduce side effects (Rautio et al., 2008)
While sometimes pursued through ANDAs, the 505(b)(2) pathway can be utilized when additional clinical data is required to support the improved efficacy or safety profile of a single isomer or a novel salt form compared to the RLD (Bolla et al., 2010).
1) Isomeric switches -
Product Name - Escitalopram (Lexapro®)
Parent drug: Citalopram (Celexa®) – racemic mix of R- and S-isomers.
Switch: S-isomer (Escitalopram) has primary serotonin reuptake inhibitory activity.
Innovation: Immediate-release tablets with higher therapeutic index.
Clinical Benefit:
Regulatory Note: Approved under 505(b)(2) leveraging Celexa safety/efficacy data.
Reference: FDA label for Lexapro [NDA 021323].
2) Salt modification -
Product Name - Quazepam Dihydrochloride (Doral®)
Parent drug: Quazepam (free base).
Salt Modification: Used dihydrochloride salt to enhance solubility and shelf stability.
Rationale: The salt form provides a slower onset and longer half-life, ideal for sleep maintenance.
Clinical Benefit:
Regulatory Note: Approved under 505(b)(2) as a salt of a known drug.
6. Case Studies Illustrating Progressive Trends:
Several successful 505(b)(2) products exemplify the progressive trends discussed above:
6.1 Case study 1 – Suboxone® sublingual film (Buprenorphine/Naloxone)
Background
Innovator product - Suboxone® sublingual tablet (Buprenorphine/Naloxone)
Problem with innovator product – High risk of misuse and medication diversion (e.g., tablets being crushed and injected)
505 (b)(2) development -
Reference - Suboxone Sublingual Film (NDA 022410)
6.2 Case study 2 – DepoSubQ-Provera 104® (Medroxyprogesterone Acetate Subcutaneous Injection)
Background
Innovator product - Depo-Provera® intramuscular (IM) injection (150 mg) was used for contraception.
Problem with innovator product - IM injections were painful, needed trained professionals for administration, and patients disliked frequent clinic visits.
505(b)(2) development -
Reference - Depo-SubQ Provera 104 (NDA 021583)
6.3 Case study 3 – Treximet® (Sumatriptan + Naproxen Sodium Combination Tablet)
Background
Innovator product - Sumatriptan (Imitrex®) was effective for migraine, but some patients needed anti-inflammatory help. Naproxen sodium (Aleve®) was commonly used separately for inflammation.
505 (b)(2) development -
Reference - Treximet (NDA 021926)
6.4 Case study 4 – Cabenuva® (Cabotegravir + Rilpivirine Long-Acting Injectable)
Background
Innovator product - Cabotegravir and rilpivirine were originally developed as oral tablets for treating HIV-1.
Problem with innovator product - Daily oral pills posed challenges like adherence issues and pill fatigue in HIV patients.
505(b)(2) development -
Reference - Cabenuva (NDA 212888).
6.5 Case study 5 – Mounjaro® (Tirzepatide Injection)
Background
Innovator product - Tirzepatide was initially explored in oral small molecule formulations targeting GLP-1/GIP receptors
Problem with innovator product – Oral versions had limited bioavailability and poor control over dose delivery.
505 (b)(2) development -
Reference - Mounjaro (NDA 215866).
6.6 Case study 6 – Kynmobi® (Apomorphine Sublingual Film)
Background
Innovator product - Apomorphine was used in injectable form for Parkinson's disease OFF episodes.
Problem with innovator product – Injection during tremors is difficult.
505(b)(2) development -
Reference - Kynmobi (NDA 210875).
7. Challenges and Considerations in 505(b)(2) Formulation Development:
While the 505(b)(2) pathway offers significant advantages, it also presents certain challenges:
8. Conclusion and Future Perspectives:
The development of differentiated 505(b)(2) formulations represents a significant and progressive trend in the pharmaceutical industry. By strategically leveraging this regulatory pathway, companies can create products that offer tangible benefits over generic formulations, addressing unmet clinical needs, enhancing patient compliance, and potentially achieving greater market success. The increasing focus on patient-centric drug development and the advancements in formulation technologies will likely continue to drive innovation within the 505(b)(2) space. Future trends may include an even greater emphasis on personalized medicine through tailored formulations, the development of more sophisticated drug-device combinations, and the application of cutting-edge drug delivery systems to improve therapeutic outcomes and patient quality of life. As the pharmaceutical landscape continues to evolve, the 505(b)(2) pathway will undoubtedly remain a crucial avenue for bringing innovative and value-added medicines to patients.
REFERENCES
Dhanesh Kokate*, Dr. Nalini Kurup, Progressive Trends in Development of 505 b (2) Formulations Over Generic Formulations, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 1679-1692. https://doi.org/10.5281/zenodo.15619422
 10.5281/zenodo.15619422
10.5281/zenodo.15619422
