The global urgency to combat Antimicrobial Resistance (AMR) and accelerate pharmaceutical pipelines has established Rapid Molecular Diagnostics (RMD) as a critical, dual-purpose technology. RMD platforms, including multiplex PCR, Next-Generation Sequencing (NGS), and advanced NAATs, provide actionable results in hours, fundamentally transforming clinical trial execution and hospital infection management. In drug development, RMD enables rapid patient stratification based on pathogen and resistance genotype, leading to more efficient enrollment and the use of molecular endpoints to objectively measure drug efficacy. Within the hospital setting, RMD drives effective Antimicrobial Stewardship (AMS) by rapidly guiding therapy de-escalation, while its use in Active Surveillance Testing (AST) and outbreak tracing significantly enhances Infection Prevention and Control (IPC). The evidence strongly supports RMD's impact on reducing unnecessary antibiotic exposure, decreasing hospital length of stay, and improving patient outcomes. Future success hinges on overcoming challenges related to cost-effectiveness, integrating results into Clinical Decision Support (CDS) systems, and the widespread implementation of automated, Point-of-Care (POC) testing.
The global landscape of public health is critically defined by the persistent threat of Infectious Diseases (IDs) and the accelerating crisis of Antimicrobial Resistance (AMR). Recent epidemiological data confirm that AMR is a leading cause of death worldwide, with drug-resistant infections now compromising the efficacy of essential, first-line treatments for common syndromes, such as bloodstream and urinary tract infections. This crisis places immense pressure on healthcare systems, driving up morbidity, mortality, and healthcare costs, particularly in critical care settings. The challenge is twofold: to rapidly develop new anti-infective therapies and to immediately optimize the use of existing agents within the hospital to slow the emergence and transmission of resistance. Both objectives are critically dependent on the speed and accuracy of microbiological diagnosis.
Limitations of Traditional Microbiology:
For decades, the culture-based methods of traditional clinical microbiology have been the gold standard. However, these techniques suffer from significant limitations that are increasingly untenable in the face of acute infection and the need for swift therapeutic decisions. Conventional methods require a long turnaround time (TAT), often spanning 48 to 96 hours to isolate, identify, and perform Antimicrobial Susceptibility Testing (AST). This protracted diagnostic window mandates the use of empirical broad-spectrum antibiotics, a practice that, while necessary to prevent adverse patient outcomes in time-critical conditions like sepsis, is the primary driver of AMR. Furthermore, culture-based methods possess reduced sensitivity for fastidious or non-culturable organisms and can yield false-negative results in patients who have received prior antimicrobial therapy. The inherent delay creates a profound barrier to both effective clinical management and efficient pharmaceutical development.
The Defining Role of Rapid Molecular Diagnostics (RMD):
The advent of Rapid Molecular Diagnostics (RMD) has initiated a paradigm shift in the diagnosis of infectious diseases. RMD encompasses a range of nucleic acid-based technologies, including multiplex Polymerase Chain Reaction (PCR), isothermal amplification methods, and Next-Generation Sequencing (NGS), that directly detect the genetic material of pathogens and their associated Antimicrobial Resistance (AMR) genes. The key advantage of RMD is its ability to deliver highly sensitive, specific, and actionable results in under 1 to 6 hours, dramatically shortening the diagnostic window. This technological leap provides a direct and immediate opportunity to transition from reactive, empirical therapy to precise, targeted treatment.
While the utility of RMD is widely acknowledged, its transformative potential is uniquely expressed across two distinct, yet interconnected, high-stakes environments: the rigorous setting of pharmaceutical clinical trials and the acute demands of hospital infection management. The research problem addressed by this review is the necessity of synthesizing the evidence demonstrating RMD's comprehensive impact across this translational spectrum. Specifically, there is a need to detail how RMD technologies streamline the complex, costly, and time-intensive process of anti-infective drug development while simultaneously acting as the central pillar of Antimicrobial Stewardship (AMS) and Infection Prevention and Control (IPC) in the tertiary care setting.
Objective of the Review:
The primary objective of this review is to provide a detailed, scientific, and accurate synthesis of the current state and emerging applications of Rapid Molecular Diagnostics. This article will systematically examine the evidence for RMD's dual-role impact: first, in accelerating the design, execution, and endpoint analysis of pharmaceutical clinical trials for new antimicrobial agents; and second, in optimizing patient care and resource utilization through enhanced hospital infection management. Finally, we will delineate the major operational challenges, strategic implementation requirements, and future perspectives, including the role of Point-of-Care (POC) diagnostics, necessary to fully harness this technology to mitigate the global threat of AMR. [1-6]
Rapid Molecular Diagnostics in Pharmaceutical Clinical Trials
The development of new anti-infective agents is characterized by high cost, prolonged timelines, and significant failure rates, challenges exacerbated by the time required for traditional microbiology. Rapid Molecular Diagnostics (RMD) has become an indispensable technology that fundamentally optimizes and accelerates the clinical trial lifecycle by providing unprecedented insight into pathogen characteristics, host response, and drug efficacy.
Accelerating Patient Stratification and Enrollment
A cornerstone of modern clinical trials for anti-infectives is the precise identification of patients who will most benefit from a specific drug candidate. RMD addresses this need by facilitating real-time patient stratification and enrollment, moving away from broad syndrome-based enrollment to targeted etiology-based inclusion.
Pathogen Identification: RMD platforms, such as multiplex Polymerase Chain Reaction (PCR) panels, can identify the causative bacterial, fungal, or viral agent directly from clinical specimens within hours. This contrasts sharply with the multi-day delays of culture. For instance, in trials targeting specific Staphylococcus aureus or Gram-negative infections, rapid identification is crucial for inclusion/exclusion criteria.
Resistance Marker Screening: Crucially, RMD can simultaneously screen for key resistance marker genes (e.g., mecA for Methicillin-Resistant S. aureus, blaKPC?, or blaNDM? for carbapenem resistance). This capability is paramount for trials evaluating narrow-spectrum or resistance-targeted agents, ensuring that only patients with the relevant resistance profile are enrolled. By rapidly confirming the molecular signature of the infection, RMD significantly reduces screen-fail rates and dramatically shortens the time from patient presentation to study enrollment.
Efficacy Endpoints and Surrogate Markers
RMD provides powerful tools for evaluating a drug's effectiveness, offering objective, quantifiable measures that complement or even supplant traditional clinical and microbiological outcomes.
Quantification of Pathogen Load: Using quantitative PCR (qPCR) or the highly sensitive digital PCR (dPCR), researchers can precisely measure the copy number of the target nucleic acid (pathogen load) in serial clinical samples. This allows for the precise determination of the drug's impact on microbial replication kinetics.
Objective Early Efficacy Measures: Pathogen load reduction or molecular clearance kinetics can serve as valuable primary or secondary endpoints. In viral or fungal trials, for example, a rapid, statistically significant reduction in pathogen RNA or DNA levels often serves as an early surrogate marker for treatment success, enabling faster decision-making regarding dose selection, duration of therapy, and overall trial progression, long before definitive clinical resolution is achieved. This is particularly relevant in trials with vulnerable populations, such as the immunocompromised, where rapid assessment of drug action is essential.
Pharmacodynamics (PD) and Pharmacogenomics (PGx) Integration
RMD technologies are pivotal in integrating microbiology with host biology, leading to more robust therapeutic strategies.
Pathogen Genotyping and Resistance Surveillance (PD): Throughout a trial, RMD is used for genotyping and sequencing of baseline and breakthrough isolates to detect the emergence of acquired drug resistance mechanisms. By comparing pre- and post-treatment isolates, RMD can elucidate the genetic pathways of resistance development, directly informing the optimal dosing regimen and highlighting potential limitations of the new drug.
Host Pharmacogenomics (PGx): Beyond the pathogen, RMD also facilitates the analysis of host genetic factors that influence drug metabolism and response. Polymorphisms in drug-metabolizing enzymes (e.g., Cytochrome P450) can be rapidly screened, allowing for the potential adjustment of dosing to minimize toxicity or maximize efficacy, supporting the move toward personalized medicine within the clinical trial framework.
High-Throughput Sequencing for Outbreak and Transmission Analysis
While trial data integrity is paramount, RMD also plays a critical role in safety and quality control by ensuring that patient infections are distinct and not due to transmission within the study site.
Phylogenetic Analysis: The application of Whole-Genome Sequencing (WGS) and other high-throughput sequencing methods provides ultra-high resolution genetic blueprints of isolated pathogens. This allows for precise phylogenetic analysis of isolates from different patients.
Contamination and Cross-Infection Tracking: By comparing the sequencing data, investigators can quickly determine if patients enrolled in the trial are being infected by closely related strains, signaling a potential trial-related contamination event (e.g., from a shared environmental source) or cross-infection within a study ward. Rapid identification of transmission clusters allows for immediate implementation of infection control measures, safeguarding trial integrity and patient safety. NGS thus serves as a powerful surveillance tool to maintain the scientific rigor and ethical standards of the study. [7-13]
Table 1 Impact of RMD application on clinical trials [14-15]
Key Area of RMD Application
Specific RMD Technology Used
Mechanism of Action / Information Gained
Impact on Clinical Trials
Patient Stratification & Enrollment
Multiplex PCR Panels, Real-Time PCR (qPCR)
Simultaneous detection of target pathogen (bacteria, virus, fungus) and associated key resistance genes
Dramatically reduces screen-fail rates; ensures rapid enrollment of patients with the precise etiological and resistance profile required by the trial protocol.
Efficacy Endpoints & Surrogate Markers
Quantitative PCR (qPCR), Digital PCR (dPCR)
Precise, highly sensitive enumeration of pathogen nucleic acid copies (viral/bacterial/fungal load) in serial samples.
Provides objective, quantifiable, and early measures of drug effect (e.g., molecular clearance kinetics), accelerating dose selection and go/no-go decisions.
Pharmacodynamics (PD) / Drug Resistance Surveillance
Sequencing (Sanger or NGS) of target genes, Genotyping Assays
Identifies new mutations or genetic alterations in the pathogen genome that emerge de novo during treatment (acquired resistance).
Elucidates the mechanism of treatment failure; informs optimal dosing and drug exposure levels to suppress resistance emergence.
Pharmacogenomics (PGx) Integration
Single Nucleotide Polymorphism (SNP) Assays
Screens for host genetic variants (e.g., in Cytochrome P450 enzymes) that influence drug metabolism and response (ADME).
Allows for stratification based on predicted drug safety and efficacy, paving the way for personalized dosing within the trial.
Generates high-resolution phylogenetic maps of all patient isolates within a study site.
Identifies clusters of closely related strains, quickly confirming or ruling out trial-related cross-infection or contamination events, thus preserving data integrity and patient safety.
Rapid Molecular Diagnostics in Hospital Infection Management (HIM)
The clinical application of Rapid Molecular Diagnostics (RMD) constitutes a transformative tool in acute care settings, directly influencing patient outcomes, resource utilization, and the integrity of hospital infection control programs. The immediacy of RMD results is crucial for effective Hospital Infection Management (HIM), particularly in the face of life-threatening conditions where every hour of delayed appropriate therapy increases the risk of mortality.
Syndromic Panels for Critical Care
The most impactful application of RMD in HIM lies in the deployment of syndromic molecular panels within high-acuity areas like the Emergency Department (ED) and Intensive Care Unit (ICU). These multiplex assays are designed to test for multiple potential pathogens (bacteria, viruses, fungi) and associated resistance genes simultaneously from a single patient sample, addressing the challenge of overlapping clinical presentations.
Actionable Results in Hours: Syndromic panels for Bloodstream Infections (BSIs), for instance, can identify organisms directly from positive blood culture bottles, often 24 to 48 hours earlier than conventional methods. This rapid identification of agents like Staphylococcus aureus or Gram-negative bacilli allows clinicians to transition from broad-spectrum empirical antibiotics to pathogen-specific, targeted therapy.
Guiding Therapy Optimization: In cases of severe respiratory illness, RMD respiratory panels quickly differentiate between bacterial and viral etiologies (e.g., Influenza vs. bacterial pneumonia). This allows for the timely de-escalation of unnecessary antibacterial agents when a viral infection is confirmed, or the prompt initiation of appropriate antiviral therapy, leading to better clinical trajectories and reduced antibiotic pressure. The net effect is a reduction in the time to effective therapy and a corresponding decrease in hospital length of stay (LOS) and overall costs.
Antimicrobial and Diagnostic Stewardship (AMS & DS)
The integration of RMD into the clinical workflow forms the technological backbone for successful Antimicrobial Stewardship (AMS) programs, facilitated by sound Diagnostic Stewardship (DS) principles.
Facilitating AMS Decisions: Faster turnaround times (TAT) are the most significant contribution to AMS. By providing species-level identification and resistance gene status (e.g., MRSA, ESBL, KPC) within hours, RMD empowers AMS teams to implement 'bug-drug' matching protocols rapidly. This process includes de-escalation (narrowing the antibiotic spectrum), optimization (switching to a safer or less costly agent), or discontinuation of unnecessary antibiotics.
Reducing Unnecessary Use: Studies have consistently demonstrated that RMD-guided protocols lead to a significant decrease in the duration and spectrum of unnecessary empirical antibiotic use. By offering definitive diagnostic clarity earlier, RMD allows clinicians to confidently avoid broad-spectrum agents that drive AMR, reserving them for cases where they are truly needed.
Infection Prevention and Control (IPC)
RMD plays a fundamental role in proactive and reactive strategies for Infection Prevention and Control (IPC), helping to contain the spread of Multidrug-Resistant Organisms (MDROs).
Active Surveillance Testing (AST): RMD is highly efficient for Active Surveillance Testing (AST) for key MDROs such as Methicillin-Resistant Staphylococcus aureus (MRSA), Vancomycin-Resistant Enterococci (VRE), and toxigenic Clostridioides difficile (C. difficile). Automated RMD platforms allow for high-volume screening of patients upon hospital admission, transfer to the ICU, or prior to high-risk procedures.
Rapid Isolation and Containment: The rapid nature of RMD allows for the immediate placement of high-risk patients into contact isolation or cohorting, minimizing the window during which an infected or colonized patient might transmit the organism to susceptible individuals. This is a critical component of preventing the establishment of Healthcare-Associated Infections (HAIs) and subsequent outbreaks.
Outbreak Management: During suspected outbreaks, RMD provides the speed and precision necessary to perform rapid case finding and contact tracing, using molecular typing to determine if cases are epidemiologically linked, thus guiding targeted cleaning and sterilization efforts.
Detection of Emerging and Highly Resistant Organisms
RMD is an essential early-warning system for the clinical microbiology laboratory, ensuring preparedness against emerging threats.
Carbapenem-Resistant Organisms (CROs): The ability of RMD to directly detect genes encoding carbapenemase enzymes from rectal swabs or clinical cultures is vital. Rapid CRO detection enables immediate, strict isolation protocols and informs the selection of highly restricted, last-resort antibiotics, mitigating the catastrophic potential of these "last-line" resistance threats.
Pandemic Preparedness: The swift development and deployment of RMD assays for novel pathogens, exemplified by the response to the SARS-CoV-2 pandemic, underscores their importance. RMD provides the rapid diagnostic capacity necessary for widespread screening, surveillance, and containment of new viral or bacterial threats before they overwhelm healthcare infrastructure. [19-22]
Technology Deep Dive: State-of-the-Art RMD Platforms
The success of Rapid Molecular Diagnostics (RMD) in clinical trials and hospital management is fundamentally underpinned by continuous technological innovation. The current landscape is dominated by sophisticated platforms that offer a range of capabilities, from high-throughput laboratory analysis to low-cost, field-deployable solutions.
Multiplex PCR and Array-Based Technologies
The foundational technology of real-time Polymerase Chain Reaction (PCR) has evolved into highly automated, integrated multiplex systems, which constitute the current standard for rapid, high-sensitivity diagnostics in centralized laboratories and increasingly in near-patient settings.
Mechanism and Capability: Multiplex PCR utilizes multiple primer sets simultaneously within a single reaction tube, enabling the exponential amplification and detection of numerous distinct targets—including multiple pathogen species (bacteria, viruses, fungi) and key Antimicrobial Resistance (AMR) genes (e.g., blaKPC?, mecA)—from a single clinical specimen. This "syndromic" approach addresses the complexity of infectious diseases where symptoms often overlap, providing a comprehensive etiological profile.
Array Integration: These assays are typically executed on fully automated platforms (e.g., cartridge- or pouch-based systems) that integrate sample processing, nucleic acid extraction, amplification (often nested or two-stage PCR), and detection. The final detection often employs array-based technologies, where amplicons bind to specific probes immobilized on a solid support (e.g., a chip or bead), allowing for the distinct readout of dozens of targets within a fast Turnaround Time (TAT), often less than 1.5 hours.
Clinical Relevance: These platforms are critical in high-acuity settings (ICU/ED) due to their sensitivity, high specificity, and minimal hands-on time, providing actionable results that guide immediate therapeutic decisions.
Isothermal Amplification Methods (e.g., LAMP)
While conventional PCR requires a thermal cycler to alternate temperatures for denaturation, annealing, and extension, Isothermal Amplification Methods represent a revolutionary advancement by maintaining a constant reaction temperature.
Loop-Mediated Isothermal Amplification (LAMP): LAMP is the most prominent isothermal technique, utilizing a unique set of four to six primers that recognize eight distinct regions of the target DNA. A DNA polymerase with strong strand displacement activity (e.g., Bst polymerase) generates characteristic stem-loop DNA structures, resulting in rapid and massive amplification.
Point-of-Care (POC) Potential: The central advantage is the elimination of the complex and costly thermal cycling instrument. The reaction can be executed using only a simple water bath or block heater, making it ideal for low-cost, Point-of-Care (POC) deployment in resource-limited settings or decentralized clinical locations.
Detection and Advantages: LAMP offers comparable sensitivity to PCR and is more resistant to inhibitors commonly found in crude clinical samples. Detection is often simplified, sometimes relying on a visually discernible readout (e.g., turbidity due to magnesium pyrophosphate precipitate, or a color change from an indicator dye), further enhancing its utility outside of central laboratories. The primary technical challenge remains the complex design of the multiple primer sets and the difficulty in efficiently multiplexing many targets simultaneously.
Next-Generation Sequencing (NGS) and Metagenomics
Next-Generation Sequencing (NGS), specifically when applied to the total nucleic acid content of a sample (known as Metagenomic Next-Generation Sequencing, or mNGS), represents the cutting edge of RMD, offering an unparalleled level of diagnostic depth.
Unbiased Pathogen Detection (mNGS): Unlike PCR-based assays, which are limited to pre-selected targets, mNGS performs a shotgun sequencing of all DNA and RNA present in a clinical sample (host, pathogen, and commensal organisms). Sophisticated bioinformatics pipelines then filter out human sequences and align the remaining microbial reads to vast genetic databases, providing a truly unbiased pathogen detection. This is invaluable for identifying rare, novel, fastidious (difficult-to-culture), or unexpected co-infecting pathogens missed by conventional or targeted RMD.
Comprehensive AMR Gene Profiling: When applied to cultured isolates (Whole-Genome Sequencing, or WGS) or directly to a clinical sample, NGS provides the most comprehensive data for AMR gene profiling. By sequencing the entire genome or the collective metagenome, researchers can simultaneously detect all known and potentially novel genetic determinants of resistance and virulence factors, offering predictive resistance information essential for guiding therapy.
Current Limitations: While providing maximum information, the major limitations for routine acute care application remain the relatively high cost, long TAT (typically 24–72 hours from sample to final report), and the demanding bioinformatic expertise required for data interpretation. Its current utility is greatest in complex, subacute, or chronic infections where the causative agent remains elusive after conventional testing. [23-28]
Challenges and Future Perspectives
Despite the profound benefits demonstrated in clinical trials and hospital management, the widespread and uniform adoption of RMD faces significant technical, economic, and operational challenges. Addressing these hurdles will define the trajectory of molecular diagnostics in infectious disease management over the next decade.
Cost-Effectiveness and Reimbursement
The primary barrier to broader RMD implementation in many healthcare settings is the complex economic calculation necessary to justify the technology.
High Initial Capital Cost: RMD platforms, particularly those utilizing sophisticated multiplex PCR or Next-Generation Sequencing (NGS), require a substantial initial capital investment for instrumentation and associated infrastructure. This financial commitment can be prohibitive for smaller hospitals or resource-limited regions.
Demonstrating Long-Term Value: The economic value proposition of RMD is often indirect. While the cost per test may be higher than traditional culture, RMD systems achieve cost-effectiveness by generating downstream savings that are difficult to model precisely. These savings include:
Lower Treatment Costs: Prompt de-escalation from expensive, broad-spectrum antibiotics to narrower, less costly agents.
Improved Survival and Reduced Morbidity: Preventing costly complications associated with delayed or inappropriate therapy.
Reimbursement Complexity: Complicating matters is the fragmented nature of reimbursement models. Payers often focus on the immediate cost of the diagnostic test rather than the overall economic benefit to the patient's course of care. Advocacy for revised reimbursement structures that recognize the comprehensive value of RMD is crucial for sustained adoption.
Translating Results into Clinical Action (The "Last Mile" Problem)
The speed of RMD is irrelevant if the resulting information is not immediately and correctly applied to patient care—a phenomenon known as the "last mile" problem.
Need for Immediate Interpretation: A rapid result from an RMD test, such as the detection of a specific resistance gene, often requires immediate adjustments to the patient's therapy. However, front-line clinicians, particularly those outside infectious disease specialties, may lack the specialized knowledge required to interpret complex molecular results (e.g., distinguishing between colonization and true infection, or understanding the phenotypic expression of a detected resistance gene).
Clinical Decision Support (CDS) Systems: The solution lies in integrating RMD results directly with Clinical Decision Support (CDS) systems embedded within the Electronic Health Record (EHR). These systems must be engineered to provide automated, patient-specific alerts and actionable therapeutic recommendations (e.g., "Change Vancomycin to Cefazolin for S. aureus positive, mecA negative").
Antimicrobial Stewardship (AMS) Integration: Robust Antimicrobial Stewardship teams are essential to close the "last mile." They serve as the critical human bridge, utilizing RMD data to proactively intervene, educate clinicians, and enforce local antibiotic guidelines, ensuring that diagnostic speed translates into appropriate therapeutic action.
Standardization, Validation, and Regulatory Hurdles
The proliferation of RMD platforms requires a concerted effort to ensure diagnostic quality and consistency across manufacturers and laboratories.
Standardization Challenges: Currently, significant heterogeneity exists in RMD platforms regarding target selection, assay design, performance metrics (sensitivity/specificity), and reporting formats. Achieving standardization in assay components, protocols, and data interpretation is necessary to ensure equivalent results across different healthcare networks and to facilitate multi-center clinical trials.
Regulatory Framework Evolution: Regulatory agencies (such as the FDA) face the challenge of evaluating and approving increasingly complex multiplex and metagenomic assays. These novel technologies often test for organisms and resistance markers simultaneously, requiring new validation standards that account for the clinical context and the simultaneous testing of dozens of targets. The regulatory pathway for laboratory-developed tests (LDTs) also remains an area of ongoing discussion and reform.
Bioinformatics Validation: For high-complexity systems like mNGS, the "wet lab" procedure is only half the battle. Bioinformatics pipelines, which interpret the raw genetic data, must be rigorously validated and continually updated to maintain accuracy, a challenge that requires specialized expertise not traditionally found in clinical microbiology labs.
The Future of POC and Microfluidics
The future of RMD is trending towards decentralization, focusing on systems that minimize hands-on time and maximize clinical accessibility.
Fully Automated, Sample-to-Answer Systems: Next-generation RMD platforms will increasingly be fully automated, sample-to-answer systems that require minimal technical skill. These systems integrate all procedural steps—from automated sample preparation (lysis and nucleic acid extraction) to amplification and final result reporting—into a sealed, disposable cartridge. This eliminates contamination risk and reduces the need for highly trained molecular staff, making the technology viable in remote clinics, ambulances, or non-laboratory hospital units.
Microfluidics and Nanopore Technology: Microfluidic chips will shrink laboratory processes to the microscale, enabling ultra-fast, high-density testing while conserving reagent volume. Furthermore, emerging technologies like Nanopore sequencing promise real-time, ultra-portable sequencing at the point of care. These devices could potentially allow for sequencing-based pathogen identification and resistance profiling directly at the bedside, representing the ultimate realization of rapid, comprehensive diagnostics for personalized infectious disease management. [29-31]
CONCLUSION
The evidence presented underscores the role of Rapid Molecular Diagnostics (RMD) not merely as an incremental laboratory improvement, but as an essential, transformative technology reshaping the trajectory of infectious disease management across the clinical and pharmaceutical continuum.
Synthesis of Dual Impact
RMD has achieved a dual and synergistic impact: accelerating the supply of novel anti-infectives while simultaneously enhancing the efficiency of their deployment within healthcare settings.
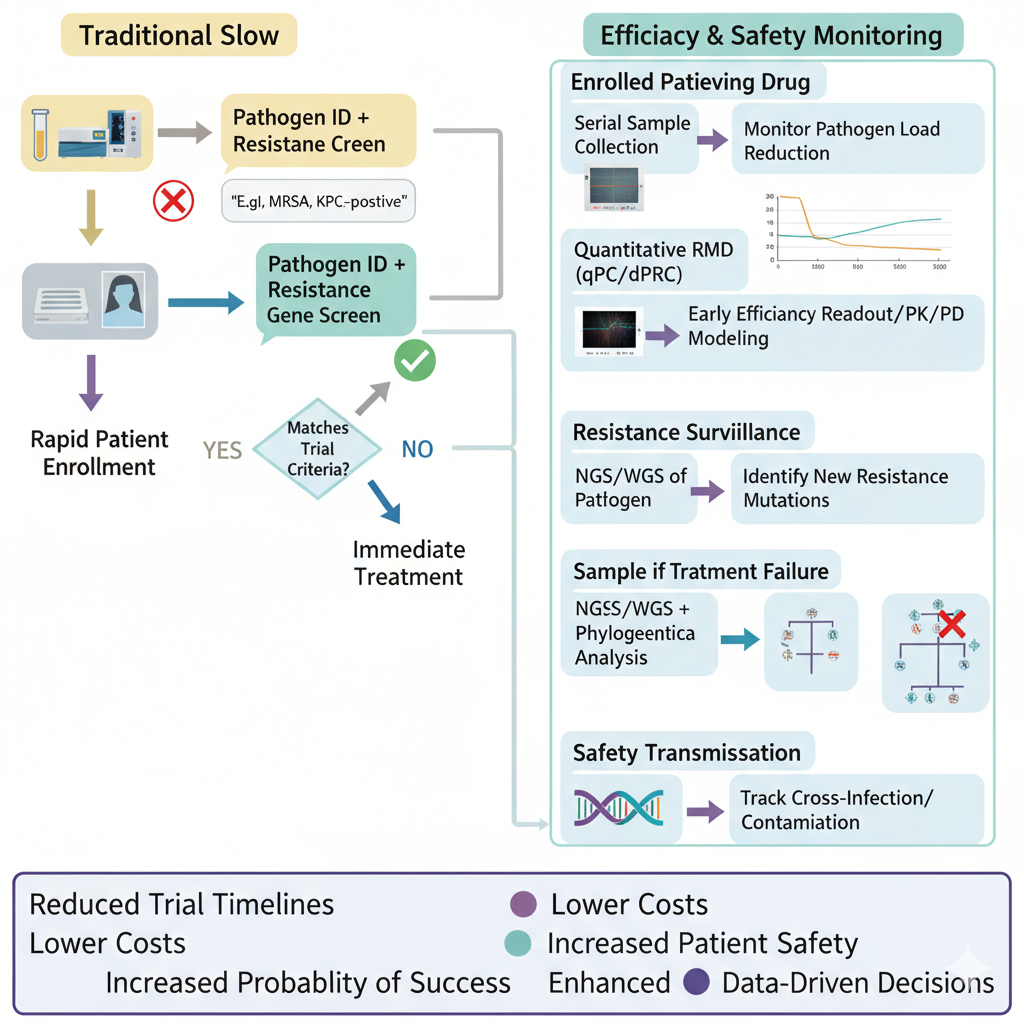
In the sphere of Pharmaceutical Clinical Trials, RMD platforms have fundamentally optimized the development process. By enabling real-time pathogen identification and resistance gene screening, RMD facilitates the swift and precise stratification of patient cohorts, drastically reducing enrollment times and ensuring that the right drugs are tested on the right infections. Furthermore, quantitative RMD methods (qPCR, dPCR) provide objective, early surrogate endpoints, offering faster efficacy readouts that accelerate decision-making regarding dose selection and overall trial progression. The integration of Next-Generation Sequencing (NGS) provides critical quality control, enabling high-resolution phylogenetic tracking to prevent and monitor trial-related contamination, thereby securing the integrity of high-stakes pharmaceutical research.
In the clinical domain of Hospital Infection Management (HIM), RMD has proven indispensable for safeguarding patient safety and optimizing antibiotic use. The deployment of syndromic panels in critical care settings allows for the rapid de-escalation of empirical, broad-spectrum antibiotics to targeted, pathogen-specific agents, a cornerstone of effective Antimicrobial Stewardship (AMS). Concurrently, RMD-based Active Surveillance Testing (AST) for high-threat organisms (e.g., MRSA, CROs) allows for immediate patient isolation and rigorous infection control measures, directly reducing the incidence of costly and deadly Healthcare-Associated Infections (HAIs).
Collectively, this dual impact confirms RMD as a core strategy in the global fight against Antimicrobial Resistance (AMR), providing the diagnostic clarity and speed necessary to outpace the evolution of drug-resistant pathogens.
Call to Action and Future Directives
To fully capitalize on the potential of RMD and to translate technological capability into universal public health benefit, a concerted call to action is necessary:
Sustained Investment in Research and Development: Continued public and private funding must be channeled into developing simpler, faster, and more robust RMD technologies. This includes miniaturization toward Point-of-Care (POC) microfluidic platforms and refining the speed and cost-effectiveness of Metagenomic NGS (mNGS) to bring its unbiased detection capabilities closer to routine clinical use.
Platform Integration and Standardization: Efforts must be intensified to standardize diagnostic performance metrics across diverse RMD platforms and to create unified regulatory pathways. Critically, investment is needed in Clinical Decision Support (CDS) systems that seamlessly integrate RMD results into Electronic Health Records (EHRs), overcoming the "last mile" challenge by providing automated, actionable therapeutic guidance to front-line clinicians.
Interdisciplinary Collaboration: Effective infectious disease management requires a tight partnership between pharmaceutical research (utilizing RMD for biomarker and companion diagnostic development), diagnostics companies (innovating new platforms), clinical microbiologists (implementing and validating tests), and Antimicrobial Stewardship programs (interpreting and enforcing appropriate use). Only through this collaborative ecosystem can the full life-cycle benefits of RMD—from the discovery of a new drug to its appropriate use at the patient bedside—be realized.
In summary, RMD is not merely a diagnostic tool; it is a strategic asset that enhances the scientific rigor of drug development and strengthens the resilience of the healthcare system against infectious threats. Its continued advancement and systematic integration are non-negotiable imperatives for modern medicine
Conflict of Interest
The author declares that there are no conflicts of interest regarding the publication of this article.
REFERENCES
MMojebi A, Wu P, Keeping S, Hale B, Chase JG, Beaubrun A. Clinical impact of rapid molecular diagnostic tests in patients presenting with viral respiratory symptoms: A systematic literature review. PLoS One. 2024;19(6):e0303560.
Coleman WB, Tsongalis GJ. Molecular diagnostics: for the clinical laboratorian. Springer Science & Business Media; 2007.
Tenover FC. The role for rapid molecular diagnostic tests for infectious diseases in precision medicine. Expert Review of Precision Medicine and Drug Development. 2018;3(1):69–77.
Schmitz JE, Stratton CW, Persing DH, Tang YW. Forty years of molecular diagnostics for infectious diseases. Journal of clinical microbiology. 2022;60(10):e02446-21.
Chiu RWK, Lo YMD, Wittwer CT. Molecular diagnostics: a revolution in progress. Oxford University Press; 2015.
Vos LM, Bruning AHL, Reitsma JB, Schuurman R, Riezebos-Brilman A, Hoepelman AIM, et al. Rapid molecular tests for influenza, respiratory syncytial virus, and other respiratory viruses: a systematic review of diagnostic accuracy and clinical impact studies. Clinical Infectious Diseases. 2019;69(7):1243–53.
Debnath M, Prasad GBKS, Bisen PS. Molecular diagnostics: promises and possibilities. Springer Science & Business Media; 2010.
Greub G, Sahli R, Brouillet R, Jaton K. Ten years of R&D and full automation in molecular diagnosis. Future microbiology. 2016;11(3):403–25.
Ito RK, Demers LM. Pharmacogenomics and pharmacogenetics: future role of molecular diagnostics in the clinical diagnostic laboratory. Clinical chemistry. 2004;50(9):1526–7.
Schachter SC, Dunlap DR, Lam WA, Manabe YC, Martin GS, McFall SM. Future potential of Rapid Acceleration of Diagnostics (RADx Tech) in molecular diagnostics. Expert review of molecular diagnostics. 2021;21(3):251–3.
Mojebi A, Wu P, Keeping S, Hale B, Chase JG, Beaubrun A. Clinical impact of rapid molecular diagnostic tests in patients presenting with viral respiratory symptoms: A systematic literature review. PLoS One. 2024;19(6):e0303560.
Kaushik R, Mahajan S, Dass G, Chatli MK. Introduction to Molecular Diagnostics. Molecular Diagnostics for Viral Diseases: Challenges and Emerging Concepts. :1.
Amos J, Patnaik M. Commercial molecular diagnostics in the US: The Human Genome Project to the clinical laboratory. Human mutation. 2002;19(4):324–33.
Tenover FC. The role for rapid molecular diagnostic tests for infectious diseases in precision medicine. Expert Review of Precision Medicine and Drug Development. 2018;3(1):69–77.
Chiu RWK, Lo YMD, Wittwer CT. Molecular diagnostics: a revolution in progress. Oxford University Press; 2015.
Liborio MP, Harris PNA, Ravi C, Irwin AD. Getting up to speed: rapid pathogen and antimicrobial resistance diagnostics in sepsis. Microorganisms. 2024;12(9):1824.
Luepke KH, Mohr III JF. The antibiotic pipeline: reviving research and development and speeding drugs to market. Expert review of anti-infective therapy. 2017;15(5):425–33.
Bradley JS, Guidos R, Baragona S, Bartlett JG, Rubinstein E, Zhanel GG, et al. Anti-infective research and development—problems, challenges, and solutions. The Lancet infectious diseases. 2007;7(1):68–78.
Singh A, Goering R v, Simjee S, Foley SL, Zervos MJ. Application of molecular techniques to the study of hospital infection. Clinical microbiology reviews. 2006;19(3):512–30.
Krishna NK, Cunnion KM. Role of molecular diagnostics in the management of infectious disease emergencies. Medical Clinics. 2012;96(6):1067–78.
Mouliou DS. Managing viral emerging infectious diseases via current molecular diagnostics in the emergency department: the tricky cases. Expert Review of Anti-infective Therapy. 2022;20(9):1163–9.
Burillo A, Bouza E. Faster infection diagnostics for intensive care unit (ICU) patients. Expert Review of Molecular Diagnostics. 2022;22(3):347–60.
Trinh KTL, Do HDK, Lee NY. Recent advances in molecular and immunological diagnostic platform for virus detection: A review. Biosensors. 2023;13(4):490.
Emperador DM, Mazzola LT, Kelly-Cirino C. An open-source molecular diagnostic platform approach for outbreak and epidemic preparedness. African Journal of Laboratory Medicine. 2020;9(2):1017.
MacLean E, Kohli M, Weber SF, Suresh A, Schumacher SG, Denkinger CM, et al. Advances in molecular diagnosis of tuberculosis. Journal of clinical microbiology. 2020;58(10):10–1128.
Zarei M. Advances in point-of-care technologies for molecular diagnostics. Biosensors and Bioelectronics. 2017;98:494–506.
Choi JR, Tang R, Wang S, Abas WABW, Pingguan-Murphy B, Xu F. based sample-to-answer molecular diagnostic platform for point-of-care diagnostics. Biosensors and Bioelectronics. 2015;74:427–39.
Tiveljung?Lindell A, Rotzén?Östlund M, Gupta S, Ullstrand R, Grillner L, Zweygberg?Wirgart B, et al. Development and implementation of a molecular diagnostic platform for daily rapid detection of 15 respiratory viruses. Journal of medical virology. 2009;81(1):167–75.
Padmanabhan S, McLaughlin R, Dominiczak AF. The living laboratory for precision medicine—Solutions for the last-mile of implementation of precision medicine. In: The Living Laboratory for Precision Medicine. Elsevier; 2025. p. 17–31.
Nichols BE, Girdwood SJ, Crompton T, Stewart?Isherwood L, Berrie L, Chimhamhiwa D, et al. Monitoring viral load for the last mile: what will it cost? Journal of the International AIDS Society. 2019;22(9):e25337.
Sodickson AD. Driving CT developments the last mile: case examples of successful and somewhat less successful translations into clinical practice. In: Medical Imaging 2017: Physics of Medical Imaging. SPIE; 2017. p. 188–94.
Reference
MMojebi A, Wu P, Keeping S, Hale B, Chase JG, Beaubrun A. Clinical impact of rapid molecular diagnostic tests in patients presenting with viral respiratory symptoms: A systematic literature review. PLoS One. 2024;19(6):e0303560.
Coleman WB, Tsongalis GJ. Molecular diagnostics: for the clinical laboratorian. Springer Science & Business Media; 2007.
Tenover FC. The role for rapid molecular diagnostic tests for infectious diseases in precision medicine. Expert Review of Precision Medicine and Drug Development. 2018;3(1):69–77.
Schmitz JE, Stratton CW, Persing DH, Tang YW. Forty years of molecular diagnostics for infectious diseases. Journal of clinical microbiology. 2022;60(10):e02446-21.
Chiu RWK, Lo YMD, Wittwer CT. Molecular diagnostics: a revolution in progress. Oxford University Press; 2015.
Vos LM, Bruning AHL, Reitsma JB, Schuurman R, Riezebos-Brilman A, Hoepelman AIM, et al. Rapid molecular tests for influenza, respiratory syncytial virus, and other respiratory viruses: a systematic review of diagnostic accuracy and clinical impact studies. Clinical Infectious Diseases. 2019;69(7):1243–53.
Debnath M, Prasad GBKS, Bisen PS. Molecular diagnostics: promises and possibilities. Springer Science & Business Media; 2010.
Greub G, Sahli R, Brouillet R, Jaton K. Ten years of R&D and full automation in molecular diagnosis. Future microbiology. 2016;11(3):403–25.
Ito RK, Demers LM. Pharmacogenomics and pharmacogenetics: future role of molecular diagnostics in the clinical diagnostic laboratory. Clinical chemistry. 2004;50(9):1526–7.
Schachter SC, Dunlap DR, Lam WA, Manabe YC, Martin GS, McFall SM. Future potential of Rapid Acceleration of Diagnostics (RADx Tech) in molecular diagnostics. Expert review of molecular diagnostics. 2021;21(3):251–3.
Mojebi A, Wu P, Keeping S, Hale B, Chase JG, Beaubrun A. Clinical impact of rapid molecular diagnostic tests in patients presenting with viral respiratory symptoms: A systematic literature review. PLoS One. 2024;19(6):e0303560.
Kaushik R, Mahajan S, Dass G, Chatli MK. Introduction to Molecular Diagnostics. Molecular Diagnostics for Viral Diseases: Challenges and Emerging Concepts. :1.
Amos J, Patnaik M. Commercial molecular diagnostics in the US: The Human Genome Project to the clinical laboratory. Human mutation. 2002;19(4):324–33.
Tenover FC. The role for rapid molecular diagnostic tests for infectious diseases in precision medicine. Expert Review of Precision Medicine and Drug Development. 2018;3(1):69–77.
Chiu RWK, Lo YMD, Wittwer CT. Molecular diagnostics: a revolution in progress. Oxford University Press; 2015.
Liborio MP, Harris PNA, Ravi C, Irwin AD. Getting up to speed: rapid pathogen and antimicrobial resistance diagnostics in sepsis. Microorganisms. 2024;12(9):1824.
Luepke KH, Mohr III JF. The antibiotic pipeline: reviving research and development and speeding drugs to market. Expert review of anti-infective therapy. 2017;15(5):425–33.
Bradley JS, Guidos R, Baragona S, Bartlett JG, Rubinstein E, Zhanel GG, et al. Anti-infective research and development—problems, challenges, and solutions. The Lancet infectious diseases. 2007;7(1):68–78.
Singh A, Goering R v, Simjee S, Foley SL, Zervos MJ. Application of molecular techniques to the study of hospital infection. Clinical microbiology reviews. 2006;19(3):512–30.
Krishna NK, Cunnion KM. Role of molecular diagnostics in the management of infectious disease emergencies. Medical Clinics. 2012;96(6):1067–78.
Mouliou DS. Managing viral emerging infectious diseases via current molecular diagnostics in the emergency department: the tricky cases. Expert Review of Anti-infective Therapy. 2022;20(9):1163–9.
Burillo A, Bouza E. Faster infection diagnostics for intensive care unit (ICU) patients. Expert Review of Molecular Diagnostics. 2022;22(3):347–60.
Trinh KTL, Do HDK, Lee NY. Recent advances in molecular and immunological diagnostic platform for virus detection: A review. Biosensors. 2023;13(4):490.
Emperador DM, Mazzola LT, Kelly-Cirino C. An open-source molecular diagnostic platform approach for outbreak and epidemic preparedness. African Journal of Laboratory Medicine. 2020;9(2):1017.
MacLean E, Kohli M, Weber SF, Suresh A, Schumacher SG, Denkinger CM, et al. Advances in molecular diagnosis of tuberculosis. Journal of clinical microbiology. 2020;58(10):10–1128.
Zarei M. Advances in point-of-care technologies for molecular diagnostics. Biosensors and Bioelectronics. 2017;98:494–506.
Choi JR, Tang R, Wang S, Abas WABW, Pingguan-Murphy B, Xu F. based sample-to-answer molecular diagnostic platform for point-of-care diagnostics. Biosensors and Bioelectronics. 2015;74:427–39.
Tiveljung?Lindell A, Rotzén?Östlund M, Gupta S, Ullstrand R, Grillner L, Zweygberg?Wirgart B, et al. Development and implementation of a molecular diagnostic platform for daily rapid detection of 15 respiratory viruses. Journal of medical virology. 2009;81(1):167–75.
Padmanabhan S, McLaughlin R, Dominiczak AF. The living laboratory for precision medicine—Solutions for the last-mile of implementation of precision medicine. In: The Living Laboratory for Precision Medicine. Elsevier; 2025. p. 17–31.
Nichols BE, Girdwood SJ, Crompton T, Stewart?Isherwood L, Berrie L, Chimhamhiwa D, et al. Monitoring viral load for the last mile: what will it cost? Journal of the International AIDS Society. 2019;22(9):e25337.
Sodickson AD. Driving CT developments the last mile: case examples of successful and somewhat less successful translations into clinical practice. In: Medical Imaging 2017: Physics of Medical Imaging. SPIE; 2017. p. 188–94.
Dhavalkumar Gohel
Corresponding author
Medical laboratory Scientist- Thomas Jefferson University Hospital, Philadelphia, PA, USA 19107


 10.5281/zenodo.18186549
10.5281/zenodo.18186549